-
8/6/2019 Sumit Bhutani
1/46
Sumit Bhutani
Neutropenic Fever
-
8/6/2019 Sumit Bhutani
2/46
-
8/6/2019 Sumit Bhutani
3/46
Fever
Fever is defined as a single oral
temperature measurement of >38.3C
(101F) or a temperature of >38.0C(100.4F) sustained over a
1-h period
-
8/6/2019 Sumit Bhutani
4/46
Neutropenia
Neutropenia is defined as an ANC of ,500
cells/mm3 or an ANC that is expected to
decrease to ,500 cells/mm3 during thenext 48h
Profound neutropenia
Functional neutropenia
-
8/6/2019 Sumit Bhutani
5/46
Primary aim of the practice guideline is to
assist practitioners in making decisions about
appropriate care for neutropenic patients
No specific drug or duration can be
unequivocally recommended for all patients
Recommendations are derived from well-
tested patterns of clinical practice that haveemerged from
cancer therapy clinical trials
-
8/6/2019 Sumit Bhutani
6/46
-
8/6/2019 Sumit Bhutani
7/46
History
The role played by the rapid institution of
empirical, broad-spectrum antibacterial therapy
for fever and neutropenia in reducing mortality is
now unquestioned, following the report bySchimpff et al and
Klastersky et al.
Observed a 53% success rate and 67%
respectively
1. Schimpff S, Satterlee W, Young VM, Serpick A Empiric therapy
with carbenicillin and
gentamicin for febrile patients with cancer and
granulocytopenia. N Engl J Med
1971;284:1061-5
2. Klastersky J, Cappel R, Debusscher L Evaluation of gentamicin
with carbenicillin in
infections due to Gram-negative bacilli. Curr Ther Res
1971;13:174-233.
-
8/6/2019 Sumit Bhutani
8/46
-
8/6/2019 Sumit Bhutani
9/46
NEW GRAM-POSITIVE
PATHOGENS
Viridans streptococci
Leuconostocspecies
Enterococcus species,esp. vancomycin-
resistant
Corynebacterium
jeikeium, C.urealyticum
Rhodococcus equi
Bacillus cereus
Stomatococcus
mucilaginosus Lactobacillus
rhamnosus
Clostridium septicum,
C. tertium
Zinner S. CID 1999:29;490
-
8/6/2019 Sumit Bhutani
10/46
NEW GRAM-NEGATIVE
PATHOGENS
Stenotrophomonousmaltophilia
Alteromonas
putrefaciens Legionella
pneumophilia, L.micdadei
Vibrio parahemolyticus
Capnocytophagaspecies
Alcaligenesxylosoxidans
Chrysebacteriummeningosepticum
Burkholderia cepacia
Fusobacteriumnucleatum Leptotrichia buccalis
Methylobacterium
species Moraxella-like
organisms
Zinner S. CID 1999:29;490
-
8/6/2019 Sumit Bhutani
11/46
2010 guidelines
Major change in the current guideline is a morestructured
consideration of the level of risk forserious infectious
complications that a given
patient with fever and neutropenia might face. Prevention of
infection in neutropenic patients isalso an important focus of this
guideline
Bacterial, viral, and fungal prophylaxisrecommendations
new sections on the management of indwellingCVCs and
environmental precautions forneutropenic patients
-
8/6/2019 Sumit Bhutani
12/46
I. What Is the Role of Risk Assessment and What
Distinguishes
High-risk and Low-risk Patients with Fever and Neutropenia?
Risk for complications of severe infection
should be undertaken at presentation of
fever
1. Type of empirical antibiotic therapy (oral
vs intravenous [IV])
2. Venue of treatment (inpatient vs
outpatient)
3. Duration of antibiotic therapy
-
8/6/2019 Sumit Bhutani
13/46
High-risk patients
Anticipated prolonged (>7 days duration)
Profound neutropenia (absolute neutrophil
count [ANC] 100 cells/mm3 followingcytotoxic chemotherapy)
Significant medical co-morbid conditions,
including hypotension, pneumonia, new-
onset abdominal pain, or neurologic
changes.
-
8/6/2019 Sumit Bhutani
14/46
Low-risk patients, including those with
anticipated brief (7 days duration)
neutropenic periods or no or few co-
morbidities, are candidates for oral
empirical therapy
-
8/6/2019 Sumit Bhutani
15/46
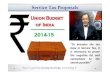
Formal risk classification may be performed
using the
MASCC scoring system High-risk patients have a MASCC score
21
-
8/6/2019 Sumit Bhutani
16/46
-
8/6/2019 Sumit Bhutani
17/46
High-risk patients have a MASCC score
-
8/6/2019 Sumit Bhutani
18/46
II What Specific Tests and Cultures Should
be Performed during the Initial Assessment?
CBC count with differential leukocyte count and
platelet count; BMP and LFTs
At least 2 sets of blood cultures are
recommended, with a set collectedsimultaneously from each lumen
of an existing
CVC, if present, and from a peripheral vein site;
2 blood culture sets from separate
venipunctures should be sent if no central
catheter is present
chest radiograph is indicated for patients with
respiratory signs or symptoms
-
8/6/2019 Sumit Bhutani
19/46
III In Febrile Patients With Neutropenia, What
Empiric
Antibiotic Therapy Is Appropriate and in What
Venue? Monotherapy with an anti-pseudomonal -
lactam agent, such as cefepime, acarbapenem (meropenem or
imipenem-cilastatin), or piperacillin-tazobactam, isrecommended
Other antimicrobials (aminoglycosides,fluoroquinolones, and/or
vancomycin) may beadded to the initial regimen for managementof
complications (eg, hypotension andpneumonia) or if antimicrobial
resistance issuspected or proven
-
8/6/2019 Sumit Bhutani
20/46
Vancomycin (or other agents active against
aerobic gram-positive cocci) is not
recommended as a standard part of the initial
antibiotic regimen for fever and neutropenia(A-I).
These agents should be considered for
specific clinical indications, includingsuspected
catheter-related infection, skin or
soft-tissue infection, pneumonia, or
hemodynamic instability.
-
8/6/2019 Sumit Bhutani
21/46
-
8/6/2019 Sumit Bhutani
22/46
MRSA: Consider early addition of
vancomycin, linezolid, or daptomycin.
VRE: Consider early addition of linezolidor daptomycin.
ESBLs: Consider early use of a
carbapenem.
KPCs: Consider early use of polymyxin-
colistin or tigecycline.
-
8/6/2019 Sumit Bhutani
23/46
Allergy issues
Most penicillin-allergic patients tolerate
cephalosporins, but those with a history of
an immediate-type hypersensitivity
reaction (eg, hives and bronchospasm)
should be treated with a combination that
avoids -lactams and carbapenems, such
as ciprofloxacin plus clindamycin oraztreonam plus
vancomycin
-
8/6/2019 Sumit Bhutani
24/46
Low risk patients
Low-risk patients who have initiated IV or oral antibiotics in
thehospital may have their treatment approach simplified if they
areclinically stable (A-I).
An IV-to-oral switch in antibiotic regimen may be made if
patients
are clinically stable and gastrointestinal absorption is felt to
beadequate (A-I).
Selected hospitalized patients who meet criteria for being at
low riskmay be transitioned to the outpatient setting to receive
either IV ororal antibiotics, as long as adequate daily follow-up
is ensured (B-III).
If fever persists or recurs within 48 h in outpatients, hospital
re-admission is recommended, with management as for
high-riskpatients (A-III).
-
8/6/2019 Sumit Bhutani
25/46
Oral Options
Ciprofloxacin plus amoxicillin-clavulanate incombination.
levofloxacin or ciprofloxacin monotherapy
ciprofloxacin plus clindamycin
(Patients receiving fluoroquinolone prophylaxisshould not
receive oral empirical therapy with afluoroquinolone)
-
8/6/2019 Sumit Bhutani
26/46
When to stop antibiotics?
Once blood culture results and organismsusceptibilities are
availableusually withinseveral days after blood samples are
drawnthey may direct a more specificchoice of antibiotics.
In a majority of cases, however, blood cultureresults are
negative. In these cases,
empirical antibiotics are generally continueduntil ANC recovery
is imminent or until aninfection requiring alternative
antimicrobialcoverage is identified.
-
8/6/2019 Sumit Bhutani
27/46
-
8/6/2019 Sumit Bhutani
28/46
Certain facts!
Only 23% of febrile neutropenic episodes
are associated with bacteremia
Frequencies of gram-positive, gram-negative, and polymicrobial
bacteremia
were approx 57%, 34%, and 9%,
respectively
greater mortality (5% vs 18%) with gram
negativesKlastersky J, Ameye L, Maertens J, et al. Bacteraemia
in febrile neutropenic
cancer patients. Int J Antimicrob Agents 2007
-
8/6/2019 Sumit Bhutani
29/46
Vancomycin is not a standard part of empiricalantibiotic therapy
for fever and neutropenia.
Despite the predominance of gram-positive
organisms as the cause of bacteremia during
fever and neutropenia, randomized studiescomparing empirical
regimens with and without
vancomycin as part of the initial empirical
regimen have shown no significant reductions in
either the duration of fever or overall mortalityVancomycin
added to empirical combination antibiotic therapy for fever in
granulocytopenic cancer patients.
European Organization for Research and Treatment of Cancer
(EORTC) International Antimicrobial Therapy
Cooperative Group and the National Cancer Institute of
Canada-Clinical Trials Group. J Infect Dis 1991; 163:951
8.
Paul M, Borok S, Fraser A, et al. Empirical antibiotics against
gram-positive infections for febrile neutropenia:
systematic review and meta-zanalysis of randomized controlled
trials. J Antimicrob
Chemother 2005; 55:43644.
-
8/6/2019 Sumit Bhutani
30/46
-
8/6/2019 Sumit Bhutani
31/46
If vancomycin or another gram-positive activeagent is added to
the initial regimen forclinical reasons, it should be discontinued
2
or 3 days later if susceptible bacteria are notrecovered from
the patient
The primary reason for the judicious use ofvancomycin has been
the epidemiological
link between its overuse and thedevelopment of drug resistance
inEnterococcus species and S. aureus
-
8/6/2019 Sumit Bhutani
32/46
VRE bloodstream infection is difficult to treatin the setting of
fever and neutropenia,particularly in leukaemic patients and/or
HSCT recipients, and it is an independentrisk factor for
death
Local and even individual patient patterns of
bacterial colonization and resistance must betaken into account
when choosing an initialempirical regimen for neutropenic patients
ata given institution
-
8/6/2019 Sumit Bhutani
33/46
IV. When and How Should Antimicrobials be
Modified During the Course of Fever and
Neutropenia? Modifications to the initial antibiotic regimen
should be guided by clinical andmicrobiologic data
Patients who remain hemodynamicallyunstable after initial doses
with standardagents for neutropenic fever should have
their antimicrobial regimen broadened toinclude coverage for
resistant gram-negative,gram-positive, and anaerobic bacteria
andfungi
-
8/6/2019 Sumit Bhutani
34/46
Empirical antifungal coverage should be
considered in high-risk patients who have
persistent fever after 47 days of a broad-
spectrum antibacterial regimen and no
identified fever source (A-II)
-
8/6/2019 Sumit Bhutani
35/46
-
8/6/2019 Sumit Bhutani
36/46
Recurrent or persistent fever > 3 days in durationdespite
empirical antibiotic therapy should prompt athorough search for a
source of infection, including anew set of blood cultures and
symptom-direction
collection of other diagnostic tests
recurrent or persistent fever, consideration should alsobe given
to noninfectious sources, such as drugrelated fever,
thrombophlebitis, the underlying canceritself, or resorption of
blood from a large hematoma. Inmany cases, no source of persistent
fever is identifiedbut the patient defervesces nonetheless, when
theANC increases to .500 cells/mm3
-
8/6/2019 Sumit Bhutani
37/46
V. How Long Should Empirical
Antibiotic Therapy be Given? In patients with clinically or
microbiologically
documented infections, the duration of therapy isdictated by the
particular organism and site;appropriate antibiotics should
continue for at least
the duration of neutropenia (until ANC > 500cells/mm3) or
longer if clinically necessary (B-III).
In patients with unexplained fever, it isrecommended that the
initial regimen be continued
until there are clear signs of marrow recovery; thetraditional
endpoint is an increasing ANC thatexceeds 500 cells/mm3 (B-II).
-
8/6/2019 Sumit Bhutani
38/46
VI. When Should Antibiotic Prophylaxis be
Given, and With What Agents?
Fluoroquinolone prophylaxis should be
considered for high-risk patients with
expected durations of prolonged and
profound neutropenia (ANC 7 days)
Antibacterial prophylaxis is not routinely
recommended for low-risk patients whoare anticipated to remain
neutropenic for 72 h oftherapy with appropriate antibiotics
For documented CLABSI caused by
coagulase negative staphylococci, thecatheter may be retained
using systemictherapy with or without antibiotic lock therapy
-
8/6/2019 Sumit Bhutani
46/46
XII. What Environmental Precautions Should be
Taken When Managing Febrile Neutropenic
Patients?
Hand hygiene is the most effective means of
preventingtransmission of infection in the hospital (A-II).
Standard barrier precautions should be followed for all
patients, andinfection-specific isolation should be used for
patients with certain
signs or symptoms (A-III).
HSCT recipients should be placed in private (ie,
singlepatient)rooms (B-III). Allogeneic HSCT recipients should be
placed in roomswith .12 air exchanges/h and HEPA filtration
(A-III).
Plants and dried or fresh flowers should not be allowed in the
roomsof hospitalized neutropenic patients
Hospital work exclusion policies should be designed to
encourageHCWs to report their illnesses or exposures