Embed Size (px)
Citation preview

N
KEYWORDS
moleculargeneticchromosomekaryotypemosaicismuniparental disomycell-free fetal DNAamniocentesischorionic villus samplingcarrier screeninggenotypesequencingPCRnext-generation sequencingnoninvasive prenatal screeningvariantsingle nucleotide polymorphismcopy number variantmicroarraycomparative genomic hybridizationoligonucleotidepreimplantation genetic screeningpreimplantation genetic diagnosisembryo
AbstractThe collection of single nucleotide variations and copy number vari-ants within an individual forms a genetic backdrop that influences how a person looks, grows, and physiologically responds to stressors such as a disease or medication. High-frequency sequence variants in the population are part of the normal backdrop of the human genome, and for the most part are not thought to have functional consequences. Overt genetic pathology, in contrast, usually arises from genetic vari-ants that disrupt the normal expression or function of one or more genes. The old term mutation has been replaced by variant, which can be benign, likely benign, of unknown significance, likely pathogenic, or pathogenic. This chapter reviews the molecular (DNA-based) tech-niques available to detect, identify, or diagnose disease-associated as well as inconsequential genetic variants, specifically pertaining to screening and diagnostic needs during pregnancy. The extent and specificity of the resulting information depends on the source of genetic material, as well as the testing platform employed. General benefits of genetic testing include identification of disorders for which in utero treatment may provide benefit, optimization of neonatal out-comes by planning appropriate delivery staffing and location, provid-ing family preparation for caring for a child with a genetic disorder, the option of pregnancy termination, and providing reassurance when results are normal. With rapidly developing technologies at our dis-posal, reproductive and obstetric professionals have a responsibility to connect patients with resources to ensure full understanding of the benefits and limitations of various screening and diagnostic options. Exciting new technologies are in development, and should continue to be held to high standards of scientific rigor and clinical validation before entering mainstream practice.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
abs0010
Resnik_9103_Chapter 2_main.indd 99 3/21/2018 4:09:51 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
15
Molecular Genetic TechnologyJENNIFER GILNER, MD, PhD | ALEKSANDAR RAJKOVIC, MD, PhD | JEFFREY A. KULLER, MD
2
Detecting the Genetic Basis of DiseaseGENETIC VARIATION
Each human being’s complete genetic sequence reveals a sig-nificant amount of genetic variation. The collection of single nucleotide variations and copy number variations within an indi-vidual forms a genetic backdrop that influences how a person looks, grows, and physiologically responds to stressors such as a disease or medication. The allelic options at any given genetic locus derive from single nucleotide substitutions within the DNA sequence. Population sampling has demonstrated that, among healthy individuals, the genetic sequence differs at around 10 million sites (out of 3.2 billion total DNA base pairs [bp]). These naturally occurring differences are called single nucleo-tide polymorphisms (SNPs). To be classified as an SNP, two or more versions of the nucleotide sequence must be present in at least 1% of the general population. Disease-causing nucleotide changes are relatively rare, thus the term single nucleotide poly-morphism describes genetic variation of healthy individuals. Spe-cific SNP-associated phenotypes are relatively inconsequential, such as SNPs in the trichohyalin gene (TCHH) that cause straight versus curly hair.1 Conversely, SNPs within the cytochrome P-450 isozyme 2D6 gene (CYP2D6) produce phenotypes with drastic modifications in an individual’s rate of opioid or antidepressant metabolism, greatly altering drug side effect profiles.2,3 Identifica-tion of SNPs, their location, and their impact on gene function has the potential to predict the future health of the individual, even though an SNP does not directly cause disease.
In addition to individual sequence variation through SNPs, comparative genome studies between individual sequences have revealed a far more pervasive form of genetic variation, termed copy number variations (CNVs).4,5 These are structural variants made up of relatively large DNA segments (ranging in size from 1000 to 500,000 bp or more) that can be duplicated or deleted at a given genetic locus, and cumulatively affect 360 million nucleotides, or about 12% of the human genome.6 A CNV can be benign (no known effect on the phenotype) or pathogenic (well-documented effect on the phenotype), and a significant proportion of identified CNVs have as-yet unknown significance (may be changed to benign or pathogenic based on future data).
Thus, whereas SNPs introduce genetic variation at the level of individual base substitutions, CNVs represent variation in the “dose” of a relatively large DNA segment. The collection of SNPs and CNVs influences how an individual responds to a
challenge, such as an invading pathogen or ultraviolet ray expo-sure from the sun. Understanding genetic variation in the form of SNPs and CNVs and their biological influence can reveal predisposition toward disease, variable susceptibility to infec-tions, and diverse responses to pharmacotherapy.
GENETIC PATHOLOGY
High-frequency sequence variants in the population are part of the normal backdrop of the human genome, and for the most part are not thought to have functional consequences. Overt genetic pathology, in contrast, usually arises from genetic vari-ants that disrupt the normal expression or function of one or more genes (Table 2.1). Gene expression and function may be disrupted by less frequent gene variants in the coding portion of a gene, increases or decreases in the relative dose of a DNA segment (CNV), changes in the normal amount of a gene product, or sequence changes in regulatory regions that prevent the cell from normally expressing the intended gene product. The old term mutation has been replaced by variant, which can be benign, likely benign, of unknown significance, likely patho-genic, or pathogenic.7 Pathogenic and likely pathogenic variant designations are reserved for changes in the genetic code that lead to altered function and clinical consequences, based on several pieces of supporting information, including consistent human case reports, identification of the type of variant, and verification by functional studies, animal models, or both. A variant may involve changing a single nucleotide base or a larger segment, in which bases are removed, duplicated, or inserted. For example, in sickle cell anemia there is one identified disease-associated variant in the hemoglobin gene; alternatively, in cystic fibrosis (CF) more than 1000 disease-associated variants or alleles have been described to date in the CF transmembrane conductance regulator gene (CFTR). Both sickle cell anemia and CF are examples of single-gene disorders (also called men-delian disorders) in which the complete disease phenotype can be accounted for by the abnormal function of a single gene. Other human diseases or syndromes, such as autism, have a genetic basis, but the genotype-phenotype correlation is far more complex and may involve multiple genes in addition to environmental influences.8
Larger genetic alterations, which risk disruption or loss of multiple genes and their function, most commonly occur during cell division by mitosis or meiosis. A variety of chromosomal abnormalities may occur during chromosome alignment and segregation (see Chapter 1), leading to chromosome breaks or rearrangements or uneven distribution of chromosomes into
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
c00002
s0010
s0015
p0010
p0015
p0020
s0020
p0025
p0030
Resnik_9103_Chapter 2_main.indd 15 3/21/2018 4:09:52 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
16 PART 1 Scientific Basis of Perinatal Biology
daughter cells. Chromosome breaks and rearrangements may be genetically balanced (normal phenotype) or genetically imbal-anced (producing abnormalities resulting from gain or loss of one or more genes), or may completely disrupt a critical gene at the breakpoint site on the chromosome, leading to loss of function-ally relevant gene products. The molecular resolution of a regular karyotype (a technique for counting the chromosomal content of a cell under light microscopy) is above 5 megabases (Mb), which allows for detection of chromosome number changes and relatively large structural chromosome rearrangements. In the past decade, advances in molecular cytogenetic technology, such as array comparative hybridization (also termed chromosomal microarrays), have improved resolution for assessing cellular DNA content below 5 Mb, down to as low as 1 kilobase (kb), and revealed a new class of chromosomal syndromes caused by microdeletions and microduplications. These syndromes involve two or more contiguous genes (genes in adjacent locations on the chromosome). Table 2.2 lists some of the more commonly recognized syndromes caused by microdeletions and microdu-plications. The phenotypes of these conditions are the result of the absence (or duplication) of multiple contiguous (adjacent) genes within the involved region.
PRECONCEPTIONAL AND PRENATAL DIAGNOSIS OF GENETIC PATHOLOGY
The focus of this chapter is to review the molecular (DNA-based) techniques available to detect, identify, or diagnose
Location Genomic Disorder Associated With DeletionsGenomic Disorder Associated With Duplications Size (Mb)
1q21.1 Thrombocytopenia–absent radius syndrome (TAR) region (OMIM 274000)
Not known 0.347–0.357
1q21.1 1q21.1 microdeletion (OMIM 612474) 1q21.1 microduplication (OMIM 612475) 1.192q13 Carrier juvenile nephronophthisis Benign copy number variation 0.1503q29 3q29 microdeletion syndrome (OMIM 609425) 3q29 microduplication syndrome (OMIM
611936)1.6
7q11.23 Williams-Beuren syndrome (WBS) (OMIM 194050) WBS duplication syndrome (OMIM 609757) 1.5–1.815q11-q13 Angelman syndrome (OMIM 105830)/Prader-Willi
syndrome (OMIM 176270)15q11-q13 duplication syndrome (OMIM
608636)0.50 to ~6.0
15q13 15q11-q13 deletion syndrome (CHRNA7) (OMIM 612001)
Unclear (CHRNA7) (OMIM 612001) 0.4001.5–1.8
16p11.2 16p11.2 deletion syndrome (OMIM 611913) 16p11.2 duplication syndrome (OMIM 611913)
0.593–0.706
16p11.2-p12 16p11.2 deletion syndrome (OMIM 613604) Pathogenic—Genoglyphix Chromosome Aberration Database (GCAD) (OMIM 23196)
8.7
16p13.1 16p13.1 microdeletion predisposing to autism and/or mental retardation
16p13.1 microduplication 1.3
17p11.2 Smith-Magenis syndrome (OMIM 182290) Potocki-Lupski syndrome (OMIM 610883) 3.717p12 Neuropathy, hereditary, with liability to pressure
palsies (HNPP) (OMIM 162500)Charcot-Marie-Tooth disease CMT1A (OMIM
118220)1.4
17q11.2 Neurofibromatosis type I (OMIM 613675) NF1 critical region microduplication syndrome
1.2–1.4
17q12 17q12 deletion syndrome (OMIM 614527) 17q12 duplication syndrome (OMIM 614526) 1.517q23 17q23.1-q23.2 deletion syndrome (OMIM 613355) 17q23.1-q23.2 duplication syndrome (OMIM
613618)2.1
22q11.21 DiGeorge syndrome/velocardiofacial syndrome (OMIM 188400/192430)
22q11.2 microduplication (OMIM 608363) 1.5–3.0
22q11.23 22q11.2 distal microdeletion (OMIM 611867) Unclear ~2.5
Microdeletion or microduplication syndromes are caused by an aberrant copy number (gain or loss) of a specific subchromosomal region. The common use of array comparative genomic hybridization has resulted in rapid increase in identification of benign as well as disease-associated copy number variations.
TABLE
2.2 Microdeletion or Microduplication Syndromes
Disorder Risk AgePrevalence of Disorder
Trisomy 21, 13, 18 > 35 years 1/500 (0.2%)Sex chromosome
aneuploidiesAny 1/1000 (0.1%)
Balanced chromosomal abnormalities
Any 1/500 (0.2%)
Pathogenic (unbalanced) chromosomal abnormalities
Any 1/10,000 (0.01%)
Mendelian disorders
Any 1/280 (0.4%)
De novo variants Any ?Pathogenic
microdeletions/duplications
Any 1/90 (1.2%)
PHENOTYPIC INCIDENCEStructural/functional birth defects in
newborns1/33 (3%)
Autism 1/88 (1.2%)Total prevalence of genetic pathology 1/10 (10%) (30
million people in United States)
Genetic pathology may arise from variation in a single gene, multiple genes, segments of chromosomes, or total number of chromosomes in a cell.
TABLE
2.1 Genetic Pathology
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
t0010
t0015
s0025
p0035
Resnik_9103_Chapter 2_main.indd 16 3/21/2018 4:09:53 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 17
approach to maximize identification of couples at increased risk for having a pregnancy affected by a mendelian disorder. First, patients may not have accurate awareness of their ethnic ances-try. Second, although the carrier frequency for disorders on ethnicity-based panels is individually high, these disorders account for only a small percentage of known mendelian dis-orders. For example, ACOG recommends at a minimum pan-ethnic screening for SMA and CF, while currently over 3000 genes are known to cause mendelian disorders. Third, so-called next-generation sequencing technologies have enabled assaying hundreds or thousands of genes simultaneously in a cost-effective manner. These technological breakthroughs have led to widespread availability of expanded carrier screening, in which a large number of both common and rare disorders are screened for simultaneously in the general population.
Expanded carrier screening uses a highly customized, mul-tiple molecular inversion probe assay13–15 to convert the infor-mation content of a genetic variant into fluorescently labeled tag sequences.13 This approach identifies both the disease-associated and the wild-type alleles of each variant. At least 100 conditions have available screening, and that number is rapidly increasing.16 With such extensive availability of screen-ing options, ACOG has provided consensus recommendations for the design of expanded carrier screening panels in order to maintain focus on the ultimate goal of providing patients with meaningful information to guide pregnancy planning. Expanded carrier panels should only include disorders that meet at least several of the following criteria11:
• Have a carrier frequency of 1 in 100 or greater• Have a well-defined phenotype• Have a detrimental effect on quality of life• Cause cognitive or physical impairment• Require surgical or medical intervention• Have onset early in life• Have the ability to be diagnosed prenatallyAs with all screening tests, expanded carrier screening is risk
reducing rather than risk eliminating, because not all variants for any disorder can be identified. A common example of this is CF, in which a negative pan-ethnic variant panel significantly reduces the risk of a patient being a carrier but does not elimi-nate it given the large total number of variants in the gene. Furthermore, positive finding rates are high in expanded carrier screening panels, and some positive findings are inconclusive because many rare variants remain uncharacterized. Srinivasan and colleagues have recently reported an expanded carrier panel for more than 100 mendelian disorders, with multiple variants tested per allele, in which 35% of individuals were found to be a carrier for at least one variant, and the rate of carrier couples was approximately 0.6% to 0.8%.16 Although this carrier rate appears high, it should be considered that every individual is suspected to carry a dozen or more deleterious variants.
The appropriate extent of screening must be individualized for each patient, and take into account both identified genetic risks and personal values after counseling by a qualified profes-sional. Informed patient consent is required prior to offering expanded carrier screening, and should meet the following ACOG guidelines11,17:
1. Carrier screening of any nature is voluntary, and it is reasonable to accept or decline.
2. Results of genetic testing are confidential and protected in health insurance and employment by the Genetic Information Non-Discrimination Act of 2008.
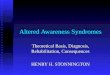
disease-associated as well as inconsequential genetic variants, specifically pertaining to screening and diagnostic needs when planning pregnancy or during pregnancy. The extent and speci-ficity of the resulting information depends on the source of genetic material, as well as the testing platform employed. Fig. 2.1 summarizes the potential sources of genetic material (DNA) for evaluation (Fig. 2.1A) and the currently available genetic assessments for preconceptional or prenatal screening or diag-nosis (Fig. 2.1B).
Genetic risk assessment begins with the evaluation of the biological parents. Family history and prior obstetric history may reveal indications for targeted testing, such as DNA sequencing or biochemical analysis for single-gene disorders, or parental karyotyping in the setting of recurrent pregnancy loss. Alternatively, indications to pursue screening or diagnostic testing may include increased risk of aneuploidy related to maternal age; racial or ethnic background, with increased carrier frequency of certain diseases; or simply population-based screening risk. In addition, it is acceptable for any patient, regardless of risk, to choose diagnostic prenatal testing after informed consent. Prenatal diagnosis may allow reproductive options, or interventions before disease is clinically detected in a child. In some rare cases, diagnosis in utero may allow the opportunity to prevent irreversible changes in early development.
Parental Carrier ScreeningCertain populations have an increased frequency of specific, identifiable, disease-associated genetic variants. This may occur because the population has remained relatively isolated, because many individuals in the population are descended from a few common relatives having a specific variant (founder effect), or because the carrier state has a beneficial effect on survival in a particular environment (sickle cell carrier state granting protec-tion from malaria). Carrier screening refers to genetic testing of asymptomatic individuals to determine if they carry one or more such genetic variants. Traditionally, carrier screening has been targeted to specific ethnic populations known to be at increased risk for particular disorders (ethnic-based screening). However, as the population becomes more racially and ethni-cally diverse, pan-ethnic screening for a panel of disorders offered to all individuals regardless of ethnicity has also been made available. Patients can undergo genetic carrier screening prior to conception or during pregnancy.9
The goal of carrier screening is to provide individuals with information that will permit them to make informed reproduc-tive decisions.10 Table 2.3 lists the currently recommended ethnic-based or pan-ethnic carrier screening tests that should be discussed with patients considering pregnancy or who are currently pregnant, according to the American College of Obstetricians and Gynecologists (ACOG).10,11 Screening for spinal muscular atrophy (SMA) and CF carrier status is recom-mended for all patients. Additional screening may be tailored by family history or ethnicity. Such testing is of maximal benefit when it is part of a comprehensive screening program including patient education, genetic counseling, timely disclosure of test results to patients, and availability of invasive diagnostic testing when needed.12
Expanded Carrier ScreeningAlthough ethnic-based carrier screening has been accepted practice for years, there are limitations to the ability of this
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0040
s0030
p0045
p0050
s0035
p0055
p0060
u0010
u0015
u0020
u0025
u0030
u0035
u0040
p0100
p0105
o0045
o0050
Resnik_9103_Chapter 2_main.indd 17 3/21/2018 4:09:53 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
18 PART 1 Scientific Basis of Perinatal Biology
SCREENING OPTIONS DIAGNOSTIC OPTIONS
Parental DNA
Embryo biopsy
Cell-free fetal DNA
Carrier screening
NIPS
PGS
Karyotype
MicroarrayCGHSNP array
FISH
PCR
Southern blot
PGD
Sequencing Next-generation sequencing
Resolution
MACRO(chromosome)
MICRO(subchromosome)
SEQUENCEVARIANTS
Increasing genomic “coverage”B
Pregnancy failure
Preconception
Prenatal/ Embryonic
Antenatal
Postnatal AdulthoodSources: Any
nucleated cells (cheek swab, blood
sample, etc.)
Sources: Gametes
Sources: Embryo biopsy
Sources: Products of conception
Sources: Genomic DNA from nucleated cells
(blood, skin, hair, cheek swab, saliva, etc.)
Sources
NONINVASIVE: Cell-free DNA
INVASIVE: Chorionic villiAmniocytesFetal biopsy
A
Figure 2.1 Schematic of preconceptional and prenatal molecular genetic screening and testing options. (A) Genomic DNA is the essential substrate needed for risk assessment or diagnosis of diseases that have a genetic basis. The range of options available for genetic testing throughout the reproductive process are shown. (B) Summary of the various molecular genetic technologies in use for reproductive genetic assessment. The techniques on the left side of the panel represent screening options, which will identify a level of risk that a pregnancy may be affected by a genetic disorder. The techniques on the right side of the panel are designed for diagnosis of genetic variants that may be associated with clinical pheno-types. Diagnostic tests require genomic DNA substrate from the embryo or fetus, and can be used to validate positive findings on a screening test. Each of the listed techniques is described in detail in this chapter. CGH, Comparative genomic hybridization; FISH, fluorescence in situ hybridization; NIPS, noninvasive prenatal screening; PCR, polymerase chain reaction; PGD, preimplantation genetic diagnosis; PGS, preimplantation genetic screening; SNP, single nucleotide polymorphism.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0010
Resnik_9103_Chapter 2_main.indd 18 3/21/2018 4:09:55 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 19
Group Genetic Disorder Carrier FrequencyScreening Test Available Detection Rate (%)
ALL WOMEN considering pregnancy or currently pregnant
Spinal muscular atrophy Caucasian, 1 : 35Hispanic, 1 : 117Ashkenazi Jew, 1 : 41Asian, 1 : 53African-American,
1 : 66
DNA variants(carrier screening
requires quantitative PCR)
Caucasian: 95%Hispanic: 91%Ashkenazi Jew: 90%Asian: 93%African-American:
71%Cystic fibrosis Caucasian, 1 : 25
Hispanic, 1 : 58Ashkenazi Jew, 1 : 24Asian, 1 : 94African-American,
1 : 61
DNA variants (>1300 disease-associated alleles identified)
Most common screen is panel of 23 pan-ethnic variants
Caucasian: 88%Hispanic: 72%Ashkenazi Jew: 94%Asian: 49%African-American:
65%Hemoglobinopathy(includes sickle cell disease [Hgb S], α-thalassemia, and β-thalassemia)
Hgb SAfrican-American,
1 : 10Also in high frequency:
Mediterranean, Middle Eastern, Southeast Asian, or West Indian descent
α-ThalassemiaAfrican, 1 : 3Mediterranean, 1 : 30Southeast Asian,
Middle Eastern, 1 : 20
β-ThalassemiaAfrican-American, <1 : 8
Asian, 1 : 20Mediterranean, 1 : 7
CBC with RBC indices for all women
Hemoglobin electrophoresis if ethnicity-based risk or abnormal RBC indices
Family history of fragile X–related disorders or intellectual disability suggestive of fragile X syndrome
Fragile X syndrome(related disorders include premature
ovarian insufficiency and fragile X–associated tremor/ataxia syndrome)
1 : 259 in general population
DNA-based molecular analysis (Southern blot and PCR) for triplet repeat
Ashkenazi Jewish (Eastern and Central European descent; should include Jews of unknown descent)
Tay-Sachs disease(Note: screening also recommended if
patient is French Canadian or Cajun descent)
Ashkenazi Jew, 1 : 30French Canadian,
Cajun, 1 : 30 to 1 : 50Non-Jewish groups,
1 : 300
Biochemical: hexosaminidase A level
98%
Canavan disease 1 : 41 DNA variants 97%Familial dysautonomia 1 : 31 DNA variants 99%Additional
autosomal recessive conditions for which screening should be considered in patients of Ashkenazi Jewish descent
Fanconi anemia group C
1 : 89 DNA variants 99%
Bloom syndrome 1 : 100 DNA variants 95%–97%Niemann-Pick
disease type A1 : 90 DNA variants 95%
Mucolipidosis type IV
1 : 127 DNA variants 95%
Gaucher disease 1 : 15 DNA variants 95%Familial
hyperinsulinism1 : 52 DNA variants
Glycogen storage disease type IA
1 : 71 DNA variants
Joubert syndrome 1 : 92 DNA variantsMaple syrup urine
disease type 1B1 : 81 DNA variants
Usher syndrome 1 : 95 (type III) DNA variants
ACOG, American College of Obstetricians and Gynecologists; CBC, complete blood count; PCR, polymerase chain reaction; RBC, red blood cell count.
TABLE
2.3 Disorders Recommended for Ethnic-Based or Pan-ethnic Carrier Screening by ACOG
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
t0020
Resnik_9103_Chapter 2_main.indd 19 3/21/2018 4:09:55 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
20 PART 1 Scientific Basis of Perinatal Biology
which are laboratory-based techniques for evaluating DNA sequence variation in an embryo or fetus. The benefits and limitations of the various types of genetic assessment are dis-cussed for each technique. General benefits of genetic testing include identification of disorders for which in utero treatment may provide benefit, optimization of neonatal outcomes by planning appropriate delivery staffing and location, providing family preparation for caring for a child with a genetic disorder, the option of pregnancy termination, and providing reassur-ance when results are normal.
Sources of Parental Genetic MaterialGenomic DNA is relatively stable; therefore it can be obtained from any cell with a nucleus, even if the cells are no longer viable. Samples for molecular testing can include blood lym-phocytes, skin scrapings, hair, cheek cells or saliva, semen, urine, and paraffin tissue blocks. At the individual gene level, disease-specific testing for families that carry known genetic variants may be performed using standard polymerase chain reaction (PCR) amplification and Sanger DNA sequencing methods (see Hybridization Techniques: Southern Blot, Polymerase Chain Reaction, later). An updated list of relatively common genetic conditions for which DNA-based prenatal diagnosis is available is kept on the Genetic Testing Registry website (www.ncbi.nlm.nih.gov/gtr).
Sources of Fetal Genetic MaterialEMBRYO BIOPSY
Advancement of in vitro fertilization techniques has allowed optimization of methods to remove or biopsy small numbers of cells from an in vitro fertilized embryo for genetic assessment prior to implantation. The techniques available to retrieve pre-implantation cells include polar body biopsy of prefertilized oocytes, biopsy of one or two cells (termed blastomeres) from the six- to eight-cell early-cleavage-stage embryo on day 3, or removal of 5 to 12 cells from the trophectoderm of the 5- to 7-day blastocyst.20 In all cases, removal of the cells does not appear to cause any cellular damage, with continued develop-ment of the embryo and no increased risk for congenital anomalies.21
NONINVASIVE APPROACH: CELL-FREE FETAL DNA IN THE MATERNAL CIRCULATION
Early attempts at noninvasive genetically based prenatal screen-ing were focused on isolation of intact fetal cells within the maternal circulation. To date, this technology has proven unsuitable for clinical application due to multiple technological obstacles such as limited numbers of fetal cells, unreliable recovery of fetal cells, and evidence that these cells persist long after pregnancy, thus complicating specificity in the setting of subsequent pregnancies.22
In contrast, identification of fetal-derived cell-free small DNA fragments (<200 bp) in maternal plasma has been highly successful. In 1997, Dr. Dennis Lo and colleagues published the first report of identifiable cell-free fetus-derived Y chromosome sequences in the plasma of pregnant women carrying male fetuses.23 Subsequent work has established that approximately 5% to 20% of the cell-free DNA circulating in maternal plasma
3. Conditions included on expanded carrier screening panels vary in severity. Many are associated with signifi-cant adverse outcomes such as cognitive impairment, decreased life expectancy, and need for medical or surgi-cal intervention.
4. Pregnancy risk assessment depends on accurate knowl-edge of paternity. If the biological father is not available for carrier screening, accurate risk assessment for reces-sive conditions is not possible.
5. A negative screen reduces but does not eliminate risk to offspring.
6. Because expanded carrier screening includes a large number of disorders, it is common to identify carriers for one or more conditions. In most cases, being a carrier of an autosomal recessive condition has no clinical conse-quences for the individual carrier. If each partner is iden-tified as a carrier of a different autosomal recessive condition, offspring are not likely to be affected.
7. In some instances, an individual may learn that he/she has two pathogenic variants for a condition (homozygous or compound heterozygous) and thus learn through carrier screening that he/she has an autosomal recessive condi-tion that could affect his/her personal health. Some expanded screening panels screen for selected autosomal dominant and X-linked conditions, and likewise an indi-vidual may learn that he/she has one of these conditions that might affect his/her health. Referral to an appropriate specialist for medical management and genetic counsel-ing is indicated in such circumstances to review the inher-itance patterns, recurrence risks, and clinical features.
8. It is important for parents to understand that over 30% of genetic disorders are the result of de novo genetic vari-ants. De novo variants arise in the germline or due to an error of somatic cell division. Therefore these variants will not be detected on parental carrier screens.
9. Downstream prenatal genetic testing on the offspring of carrier-positive parents is not available for all of the genes offered on expanded carrier screening panels. Therefore careful research on which laboratory can perform prenatal testing for a given condition is necessary prior to perform-ing chorionic villus sampling (CVS) or amniocentesis.
Fetal Genetic Screening and TestingACOG and the Society for Maternal-Fetal Medicine (SMFM) recommend that all pregnant women be counseled, as early as possible in their prenatal care, about the opportunities for pre-natal genetic assessment consisting of either aneuploidy screen-ing or diagnostic testing. This recommendation is not dependent on maternal age or other risk factors.9 Furthermore, the same professional societies, in addition to the American College of Radiology, all recommend prenatal ultrasound for multiple reasons, including accurate determination of gestational age, fetal number, cardiac activity, and placental localization and diagnosis of major fetal anomalies.18 The identification of fetal structural anomalies or minor sonographic markers on ultra-sound increases the likelihood of aneuploidy, DNA microdele-tions, or other genetic syndromes.19 Prenatal genetic testing should be offered to further evaluate abnormal findings on prenatal ultrasound.
Comprehensive discussion of screening modalities and screening or testing indications for pregnancy is presented in Chapter 32. Here we focus on molecular genetic technologies,
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
o0055
o0060
o0065
o0070
o0075
o0080
o0085
s0040
p0155
p0160
s0045
p0165
s0050
s0055
p0170
s0060
p0175
p0180
Resnik_9103_Chapter 2_main.indd 20 3/21/2018 4:09:56 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 21
single sample. In development the mosaicism becomes general-ized (present in the entire organism) or confined to a specific compartment (placenta, fetus, specific fetal organ system), depending on whether the improper chromosome segregation occurs in meiosis, early postzygotic mitosis, or late postzygotic mitosis (also refer to Chapter 1 for review of mechanisms of chromosome segregation). The most commonly encountered aneuploidy in prenatal diagnostic testing is trisomy. Note that, if trisomy originates in the zygote, the organism becomes mosaic by way of trisomy rescue, or elimination of the extrane-ous chromosome copy. Generally speaking, the earlier in devel-opment that an abnormal chromosome segregation event such as nondisjunction or trisomy rescue occurs, the more wide-spread the mosaicism may be in the differentiated organism (i.e., more likely to affect both the chorion/placenta and the fetus). Later chromosome segregation events are more likely to be confined to specific cell types, giving rise to clinical findings such as confined placental mosaicism, which leads to discordant karyotypes found with CVS versus amniocentesis. By under-standing the developmental origin of the cells biopsied via CVS, amniocentesis, or postnatal karyotyping, the clinician can use appropriate testing methods to distinguish between placental mosaicism and generalized mosaicism.
Laboratory Considerations for AmniocentesisThe cells in the amniotic fluid derive from extraembryonic ectoderm, and include cells from the fetal skin, respiratory tract, urinary tract, gastrointestinal tract, and amnion. Amniotic fluid after 16 weeks’ gestation may be analyzed directly by extraction of DNA from the amniocytes for hybridization-based methods of DNA analysis such as microarray or PCR. Alternatively or in parallel, the amniocytes may be cultured for cytology-based methods of chromosomal analysis, such as karyotyping. Cytology-based methods require the cells to proliferate in tissue culture. After 3 to 7 days of growth, sufficient mitoses are present for staining and karyotype analysis. Cells grown in flasks are harvested and analyzed together; those grown on cov-erslips are analyzed in situ as individual colonies.35,36 Amniocyte culture is quite reliable, with failure occurring in less than 1% of cases.37 Of note, hybridization-based analysis (microarray, PCR) can also be performed on DNA from cultured amnio-cytes, and is customarily done to confirm any results from direct analysis.
Amniocentesis: Mosaic ResultsChromosomal mosaicism occurs in approximately 0.1% to 0.3% of amniocentesis cases. The most common etiology is pseudomosaicism,38 where the abnormality is evident in only one of several flasks or confined to a single colony on a cover-slip. In this case the abnormal cells have arisen in vitro, are not present in the fetus, and are not clinically important. Even the observation of multiple cell lines on more than one coverslip or in more than one flask in a sample does not necessarily mean that the fetus is mosaic, because the results are confirmed by repeat karyotyping at birth or pregnancy termination in only 70% of cases.39 Some mosaic results (e.g., trisomy 20) occur in the amniotic fluid relatively frequently, but are rarely confirmed in the fetus.40
True fetal mosaicism is rare, occurring in 0.25% of amnio-centeses, but it can be clinically important, leading to pheno-typic or developmental abnormalities.38 This most frequently results from postzygotic nondisjunction,38 but it can also occur
originates from the fetus (derived from the trophoblast) and provides 25 times more fetal DNA present in a pregnant woman’s plasma than could be extracted from intact circulating fetal cells.24 Massive parallel sequencing of cell-free DNA derived from maternal plasma has led to the development of algorithms to determine fetal ploidy (chromosome count) in noninvasive prenatal screening (see details later).
Circulating fetal DNA is predominantly a product of placen-tal apoptosis.25–27 This cell-free DNA consists of small fragments (fewer than 200 bp), undergoes a rapid turnover, and may appear in apoptotic bodies or nucleosomes.28 Fetal SRY gene sequences are present in the circulation as early as 18 days after embryo transfer, before the definitive fetoplacental circulation, which is not established until 28 days after conception.29 Fetal DNA is continuously liberated into the maternal circulation, with a mean half-life estimated to be 16 minutes at term. Levels increase until approximately 10 weeks’ gestation, remain stable between 10 and 21 weeks, and then continue to increase until the third trimester.30 Fetal DNA levels are undetectable about 2 hours after birth.31
INVASIVE PRENATAL GENETIC SAMPLES
For the goal of prenatal diagnosis (not screening), the most commonly employed forms of genetic testing are CVS and amniocentesis to obtain cellular samples from the placenta and fetus, respectively, for cytogenetic analysis and molecular genetic testing (see also Chapter 32 for full discussion of indications and techniques). ACOG recommends that all women, regard-less of age or risk, be offered biochemical and/or ultrasound screening and invasive testing.32 The decision to pursue invasive testing needs to incorporate considerations of level of risk that the fetus is affected, level of risk associated with the procedure, and the patient’s impression of the impact of having an affected child.
Of note, the risks involved with invasive testing may be much lower than estimates that have been previously quoted since the advent of invasive testing in the 1970s. Results of a recent meta-analysis, which included only contemporary large studies (pub-lished after the year 2000, reporting greater than 1000 total procedures), demonstrated no significant difference in the risk of miscarriage prior to 24 weeks’ gestation for women undergo-ing amniocentesis or CVS compared to those who do not have invasive testing.33 Procedure-related risk of miscarriage for amniocentesis was 0.1% and for CVS was 0.2%. Nevertheless, rates of performance of these invasive procedures are signifi-cantly declining as screening tests with higher detection rates and lower false-positive rates have become available (see Non-invasive Prenatal Screening, later). Thus it will be more difficult in coming years for practitioners to be adequately trained in these invasive techniques. It is important to note that the range of abnormalities that can be detected is far greater with invasive testing than with any available noninvasive screening tests.
Ontogenesis of Fetal Samples: Origins of MosaicismTo understand the clinical implications of abnormal chromo-somal content in some or all of the cells obtained from prenatal sampling (CVS or amniocentesis), it is important to review the different cellular origins and early development of the fetus and placenta (Fig. 2.2).34 Chromosomal mosaicism refers to the presence of two or more cell lines with different karyotypes in a
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0185
s0065
p0190
p0195
s0070
p0200
s0075
p0205
s0080
p0210
p0215
Resnik_9103_Chapter 2_main.indd 21 3/21/2018 4:09:56 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
22 PART 1 Scientific Basis of Perinatal Biology
phenomenon in which certain genes are modified during game-togenesis or prior to fertilization such that they function differ-ently based on maternal or paternal inheritance. Uniparental inheritance of imprinted genes causes significant clinical syn-dromes, such as Prader-Willi syndrome caused by maternal UPD of chromosome 15, and the converse, Angelman syn-drome caused by paternal UPD of chromosome 15. Table 2.4 lists known imprinting disorders reported in the setting of UPD.
In many cases the question of whether amniotic fluid mosa-icism involves the fetus can be resolved by karyotyping fetal
from meiotic errors with trisomy rescue. An important consid-eration for any prenatal mosaic results is to investigate the pos-sibility of uniparental disomy (UPD) among euploid cells, or the presence of two homologous chromosomes derived from the same parent. If the mechanism of mosaicism is trisomy rescue, theoretically one-third of the time the resulting diploid cell line will have UPD.41 Clinical consequences of UPD depend on the chromosome involved and include loss of heterozygosity and genomic imprinting. Loss of heterozygosity may result in expression of a recessively inherited variant when only one parent is a carrier. Genomic imprinting is an epigenetic
ZygoteCleavage embryo
Blastocyst
Trophoblast
Inner cell mass
Cytotrophoblast
Extraembryonic mesoderm (villus core)
Fetus
Extraembryonic ectoderm
(amniocytes)
Placenta
CHORIONIC VILLI(CVS)
AMNIOCENTESIS
47 Potential origins of aneuploid cell lineage
47
47
47
47
Figure 2.2 Ontogenesis of fetal and placental tissues for prenatal testing: origins of mosaicism. Discrepancies in karyotype between the placenta and the fetus can occur because the cells contributing to the chorionic villi differentiate separately and distinctly from those forming the embryo in early development. Lineage differentiation that occurs at the blastocyst stage gives rise to the trophoblast cell line and the inner cell mass. The trophoblast becomes the cytotrophoblast and syncytiotrophoblast of the developing placenta. Cell subsets within the inner cell mass develop into the extraembryonic mesoderm (which makes up the core of the chorionic villi), the extraembryonic ectoderm, and the fetus proper. Mosaicism can occur through meiotic nondisjunction with subsequent trisomy rescue, or as a result of postzygotic mitotic nondisjunction. To under-stand the implications of abnormal karyotype analysis found on chorionic villus sampling (CVS) or amniocentesis, it is critical to understand the developmental origins of the cell populations sampled in each technique.
Chromosome UPD Syndrome OMIMa
6 UPD(6)pat Transient neonatal diabetes #6014107 UPD(7)mat Silver-Russell syndrome #180860
11 UPD(11)pat Beckwith-Wiedemann syndrome #13065011 UPD(11)mat Silver-Russell syndrome #18086014 UPD(14)pat Kagami-Ogata syndrome (uniparental disomy, paternal, chromosome 14) #60814914 UPD(14)mat Temple syndrome #61622215 UPD(15)pat Angelman syndrome #10583015 UPD(15)mat Prader-Willi syndrome #17627020 UPD(20)pat Pseudohypoparathyroidism type Ib #603233
aOn the OMIM website, # indicates “Phenotype description, molecular basis known.”mat, Maternal; OMIM, Online Mendelian Inheritance in Man; pat, paternal.
TABLE
2.4 Genomic Imprinting Disorders Associated With Uniparental Disomy (UPD)
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0015
t0025
p0220
Resnik_9103_Chapter 2_main.indd 22 3/21/2018 4:09:57 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 23
Direct cell analysis also minimizes the likelihood of maternal cell contamination because the maternal decidua has a low mitotic index. However, long-term tissue culture is better for generating a larger amount of material, if a small tissue sample was recovered. Additionally, large series comparing CVS direct and long-term culture method results to fetal karyotyping have demonstrated a higher rate of inaccurate diagnosis by the direct method than by the long-term culture method.47,48 The false-positive rate for the direct method is estimated at 1 in 125, compared to 1 in 350 for the long-term culture method; and the false-negative rate is estimated at 1 in 1000 for the direct method, compared to less than 1 in 5000 for the culture method. Given this low rate of false negatives overall, if a long-term culture fails, a nonmosaic normal direct preparation result can be considered conclusive, although rare cases of false-negative rates for trisomy 21 and 18 have been reported.49,50 Ideally, both the direct and culture methods should be used to maximize diagnostic accuracy because each evaluates slightly different tissue sources, namely cytotrophoblasts in the direct method and mesenchymal cells following long-term culture. If perfor-mance of both methods of analysis is not feasible or cost-effective, the long-term culture method is more likely to accurately represent fetal karyotype.
Most biochemical diagnoses that can be made from amniotic fluid or cultured amniocytes can be made from chorionic villi as well.51 In many cases the results are available more rapidly and efficiently when villi are used rather than amniocytes, because sufficient enzyme is present to allow for direct analysis, rather than requiring products of tissue culture. However, for certain rare biochemical diagnoses, such as metachromatic leu-kodystrophy, villi are not an appropriate or reliable diagnostic source.51 The affected enzyme in metachromatic leukodystro-phy, arylsulfatase A, is expressed at very low levels in chorionic villi even in unaffected individuals. To ensure that appropriate testing is possible for a specific diagnosis or condition, the labo-ratory should be consulted before CVS is performed.
Chorionic Villus Sampling: Maternal Contamination and MosaicismGenetic evaluation of chorionic villi provides a high degree of success and accuracy, particularly with regard to the diagnosis of common trisomies.52 The US Collaborative Study revealed a 99.7% rate of successful cytogenetic diagnosis, with only 1.1% of the patients requiring a second diagnostic test such as amnio-centesis or fetal blood analysis to further interpret the results.52 In most cases the additional testing was required to delineate the clinical significance of mosaic or other ambiguous results (76%), although laboratory failure (21%) and maternal cell contamination (3%) also required follow-up testing.
Chorionic villus samples typically contain a mixture of pla-cental villi and maternally derived decidua. Although specimens are thoroughly washed and inspected under a microscope after collection, some maternal cells may remain and grow in the culture. As a result, two cell lines, one fetal and the other mater-nal, may be identified. In other cases the maternal cell line may completely overgrow the culture, thereby leading to diagnostic errors, including incorrect sex determination53–55 and poten-tially false-negative diagnoses. For this reason, a maternal blood sample should be provided along with the chorionic villus sample so that, if indicated, the level of maternal cell contami-nation can be quantitated by genotyping informative microsat-ellite markers in maternal and chorionic villus samples.56 Direct
lymphocytes obtained by percutaneous umbilical blood sam-pling or cordocentesis.42 However, this approach may not be valid in all cases, because the mosaic cell line may involve other fetal tissues but be excluded from the fetal hematopoietic com-partment, and therefore not present in a fetal blood sample.40 Certain chromosomes, such as 22, are notorious for exclusion from fetal blood and may require testing of additional fetal tissues, such as the skin, or postnatal biopsy.43
Evaluation of mosaic results should include detailed ultra-sound assessment to exclude structural anomalies. If both ultra-sound and fetal percutaneous umbilical blood sampling are normal, the parents can be generally reassured that in most cases the fetus is unaffected.42 However, a small chance of fetal involvement still exists, because the presence of an undetectable but clinically significant abnormal cell line can never be abso-lutely excluded. Follow-up ultrasound examinations are usually performed due to a higher chance of fetal growth restriction associated with some mosaic results. Because of the complexity of interpreting mosaic amniotic fluid results, consultation with a cytogenetics laboratory and a clinical geneticist or genetic counselor is generally recommended.
Laboratory Considerations for Chorionic Villus SamplingChorionic villi have three major components: an outer layer of hormonally active and invasive syncytiotrophoblast, a middle layer of cytotrophoblast from which syncytiotrophoblast cells are derived, and an inner mesodermal core containing blood capillaries and mesenchymal stroma. The cytotrophoblasts and syncytiotrophoblasts derive from the trophoblast layer, which differentiates at the blastocyst stage. The villus core derives from the extraembryonic mesoderm of the inner cell mass (see Fig. 2.2).
The average sample from a CVS procedure contains 15 to 30 mg of villous material. The villi collected in the syringe are carefully and aseptically transferred for inspection and dissec-tion under a microscope to eliminate adherent decidua. The villi are then exposed to trypsin to digest and separate the cytotrophoblast from the underlying mesodermal core. As with amniocytes, DNA can be extracted from both cell types in the villi for direct analysis (without the need for culture) by hybrid-ization methods such as microarray or PCR. One notable advantage of chorionic villi over amniocytes is that the cytotro-phoblast has a high mitotic index, with many spontaneous mitoses available for immediate cytology-based chromosomal analysis. This direct chromosome preparation can give prelimi-nary karyotype results within 2 to 3 hours.44,45 However, most laboratories now use a short-term culture to improve karyotype quality and thus report results within 2 to 4 days. Direct analysis results are generally confirmed with long-term culture-based testing. The remaining villi are placed in tissue culture to allow proliferation of cytotrophoblasts as well as mesenchymal cells from the mesodermal core. Cultured mesenchymal cells are typically ready for harvest and cytology-based chromosomal analysis within 1 week.46 As with amniocyte culture, DNA may be extracted from cultured cytotrophoblasts or villous mesen-chymal cells as well, allowing for later application of hybridization-based DNA analysis (microarray, PCR).
The direct method of sample analysis has the advantage of providing a rapid result and avoids cultural artifacts such as culture-induced aneuploidy and overgrowth with cells of certain genotypes that may have culture growth advantage.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0225
s0085
p0230
p0235
p0240
p0245
s0090
p0250
p0255
Resnik_9103_Chapter 2_main.indd 23 3/21/2018 4:09:57 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
24 PART 1 Scientific Basis of Perinatal Biology
in a culture than in a direct preparation. The specific chromo-some involved also predicts the likelihood of fetal involve-ment.62 Phillips and coworkers70 demonstrated that autosomal mosaicism involving common trisomies (i.e., 21, 18, and 13) was confirmed in the fetus in 19% of cases, whereas uncommon trisomies involved the fetus in only 3%. When sex chromosome mosaicism was found in the placenta, the abnormal cell line was confirmed in the fetus in 16% of cases.
When placental mosaicism is discovered, amniocentesis can be performed to elucidate the extent of fetal involvement. When mosaicism is limited to the direct preparation of CVS, subse-quent amniocentesis correlates with fetal genotype in 100% of cases.70 When mosaicism is observed in long-term culture prep-aration of CVS, the CVS result correctly predicts the true fetal karyotype in approximately 94% of cases, with both false-positive and false-negative results seen.70 Two cases were reported of mosaic trisomy 21 on villus culture, and despite a normal amniotic fluid analysis, a fetus or newborn was seen with mosaic aneuploidy.52 Therefore in cases of mosaicism present in long-term culture preparations of CVS, particularly involving common trisomies (21, 18, 13), amniocentesis should be offered, but the patient should be advised of the rare possibil-ity of false-negative amniocentesis results. If amniocentesis is normal after a mosaic long-term culture CVS result, follow-up may include detailed ultrasonography, fetal blood sampling, or fetal skin biopsy to fully assess the risk of fetal mosaicism. At present, the predictive accuracy of these additional tests is uncertain and fetal skin biopsy is rarely performed.
For CVS mosaicism involving sex chromosome abnor-malities, polyploidy, marker chromosomes, structural rear-rangements, and most uncommon trisomies, the patient can generally be reassured that, if amniocentesis results are euploid and detailed ultrasonographic examination is normal, the mosaicism is unlikely to be present in the fetus. As described previously, in certain cases testing for UPD is indicated (see Table 2.4).
OTHER INVASIVE FETAL BIOPSY/DIAGNOSTIC PROCEDURES
On infrequent occasions analysis of other fetal tissues may be required. Fetal skin biopsy can be helpful in the evaluation of fetal mosaicism for chromosomes (such as 22) known not to be manifested in fetal blood.43 Historically, fetal skin biopsy was also used to aid in the diagnosis of severe genetic skin blistering disorders (ichthyosis) to allow for electron microscopy and immunohistochemistry of cell junction structures; however, the availability of genetic testing for these disorders has since elimi-nated the need for fetal biopsy.73 Fetal muscle biopsy for dys-trophin analysis has been used to diagnose Duchenne muscular dystrophy in a male fetus if DNA testing was not informa-tive.74,75 Fetal kidney biopsy has diagnosed congenital nephrosis in utero,76 and aspiration and analysis of fetal urine is impera-tive in the pre-shunt evaluation of fetal renal function in cases of bladder outlet obstructions.77 Fluid from a cystic hygroma can be aspirated and accurately analyzed in lieu of amniocen-tesis or CVS. Each of these fetal biopsy techniques is performed under ultrasound guidance. These procedures are only rarely required, so their use is usually confined to only a few regional referral centers (with the exception of cystic hygroma aspira-tion, which is similar to amniocentesis) in hopes of limiting procedural risk.
preparations of chorionic villi are generally thought to prevent maternal cell contamination,44,53 whereas long-term culture has a rate varying from 1.8% to 4%.54 Maternal cell contamination is much less likely to occur in cytogenetic laboratories that process large numbers of prenatal samples and have experi-enced technicians who can separate the two cell populations. Interestingly, for reasons still uncertain, maternal cell contami-nation occurs more frequently in specimens retrieved by the transcervical route than by the transabdominal route.54
The second major source of potential diagnostic error asso-ciated with CVS is confined placental mosaicism. Due to dispa-rate ontogenesis, or developmental origin, of fetal and chorionic cells, chorionic villus tissue does not always reflect the fetal genotype (see Fig. 2.2). There are two basic mechanisms by which an aneuploid cell line would be confined to the placenta. The first possibility is a trisomy rescue early in the cleavage-stage embryo, in which the aneuploid cell line becomes isolated to the trophoblast while the euploid (“rescued”) cell line is isolated to the inner cell mass. The other potential mechanism is a mitotic error at the late cleavage or blastocyst stage that is isolated to the trophoblast or the portion of the inner cell mass that gives rise to the extraembryonic mesoderm.34 Mosaic aneu-ploid results on CVS must therefore be interpreted with caution, and follow-up testing is necessary to determine the full extent of cells that share the abnormal chromosome complement.
Although initially there was concern that this phenomenon of confined placental mosaicism might invalidate CVS as a pre-natal diagnostic tool, subsequent investigations have led to a clearer understanding of villus biology, so that accurate clinical interpretation is now possible. This understanding has also revealed new information about the etiology of pregnancy loss, discovered a new cause of fetal growth restriction, and clarified the basic mechanism of UPD.41,57–59 Importantly, a CVS diagno-sis of confined placental mosaicism for trisomy 15 may be the initial clue that UPD could be present and lead to an affected child.60,61 Therefore all cases in which trisomy 15 (either com-plete or mosaic) is diagnosed in the placenta should be evalu-ated for UPD by amniotic fluid analysis. In addition to chromosome 15, chromosomes 6, 7, 11, 14, and 20 contain known imprinted regions and require similar follow-up (see Table 2.4).34,62
Confined placental mosaicism (unassociated with UPD) can alter placental function and lead to fetal growth restriction or perinatal death.57,59,63–67 This aneuploidy effect on placental function is generally limited to specific chromosomes. For example, confined placental mosaicism for chromosome 16 leads to severe fetal growth restriction, prematurity, or perinatal death, with less than 30% of pregnancies resulting in normal, appropriate-for-gestational-age, full-term infants.64,68–71 Con-fined placental mosaicism involving chromosomes 2, 7 to 10, 13 to 18, 21, and 22 have also been associated with poor peri-natal outcomes; however, the exact mechanism by which abnor-mal cells in the placenta affect fetal growth or placental function is poorly understood.41
Mosaicism occurs in about 1% of all CVS samples54,68,72 but is confirmed in the fetus in 10% to 40% of these cases. In most cases, if the mosaic results are confined to the placenta, fetal development will be normal. If the mosaic cell line involves the fetus, significant phenotypic consequences are possible. The probability of fetal involvement appears to be related to the tissue source in which the aneuploid cells were detected; an abnormal result is more likely to reflect a true fetal mosaicism
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0260
p0265
p0270
p0275
p0280
p0285
s0095
p0290
Resnik_9103_Chapter 2_main.indd 24 3/21/2018 4:09:57 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 25
FISH probes are relatively short, fluorescence-labeled DNA sequences that are hybridized to a known location on a specific chromosome, allowing the number and location of specific DNA sequences to be determined. Metaphase or interphase cells are evaluated by counting the number of discrete fluorescent signals from each probe. A normal diploid cell queried with a probe for chromosome region in the long arm of chromosome 21 would have two signals, whereas a trisomy 21 cell would have three (see Fig. 2.4D).
Prenatal interphase evaluation of uncultured amniotic fluid can detect aneuploidies caused by monosomies, complete tri-somies, trisomies associated with robertsonian translocations, triploidy, and other numerical chromosomal abnormalities. In standard practice, probes involving chromosomes 13, 18, 21, X, and Y are used. This technology does not routinely detect cyto-genetic abnormalities such as mosaics, translocations, and rare aneuploidies.78,79 Since 1993 the position of the American College of Medical Genetics and Genomics (ACMG) has been that prenatal FISH is investigational. In 1997 the US Food and Drug Administration cleared the specific FISH probes to enu-merate chromosomes 13, 18, 21, X, and Y for prenatal diagnosis. Subsequent studies have demonstrated an extremely high con-cordance rate between FISH and standard cytogenetics (99.8%) for the specific abnormalities that the assay is designed to detect.80–83 These performance characteristics support the use of FISH for prenatal testing when a diagnosis of aneuploidy of chromosome 13, 18, 21, X, or Y is highly suspected by virtue of maternal age, positive maternal serum screening, or abnormal ultrasound findings, although confirmation with amniocyte culture results is still recommended.84
At present, it is suggested that FISH analysis not be used as a primary screening test on all genetic amniocenteses because
Cytogenetic Testing: Detection of Chromosomal or Subchromosomal AbnormalitiesKARYOTYPE
The predominant use for fetal cells obtained by amniocentesis or CVS has traditionally been cytogenetic analysis. Cells can be analyzed directly or after cell culture for approximately a week to synchronize cells in metaphase for chromosomal Giemsa staining (G-banding) to determine karyotype. With this type of staining, each chromosome has a unique pattern (Fig. 2.3). The stained chromosomes are visualized under light microscopy, and large deletions or rearrangements can be detected (resolu-tion on the order of 5 to 10 Mb). Higher resolution or more specific testing for known disease-causing chromosome regions, such as 22q11, requires molecular cytogenetic technology such as fluorescence in situ hybridization (FISH) and chromosomal microarray analysis (CMA).
FLUORESCENCE IN SITU HYBRIDIZATION
FISH, the most widely used molecular cytogenetic technology, takes advantage of the complementary nature of DNA. In this approach, denatured DNA sequences labeled with a fluorescent dye are hybridized (matched by complementary nucleotide sequence) onto denatured chromosomes that have been immo-bilized onto a slide. The chromosomes are then viewed with a wavelength of light that excites the fluorescent dye (Fig. 2.4). FISH is a powerful tool to confirm or diagnose syndromes that are caused by microdeletions of segments of chromosomal material (see Table 2.2).
1 2 3 4 5
6 7 8 9 10 11 12
13 14 15 16 17 18
19 20 21 22 X Y
Figure 2.3 A standard G-banded karyogram. There are approximately 550 bands in one haploid set of chromosomes in this karyogram. The sex karyotype is X,Y (male). A female karyogram would show two X chromosomes.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0020
s0100
s0105
p0295
s0110
p0300
p0305
p0310
p0315
Resnik_9103_Chapter 2_main.indd 25 3/21/2018 4:09:57 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
26 PART 1 Scientific Basis of Perinatal Biology
diagnosis of 22q11.2 deletion syndrome, a phenotypically vari-able autosomal dominant deletion syndrome that commonly includes congenital heart defects, palate abnormalities, charac-teristic facial features, immunodeficiency, learning disabilities, and other abnormalities requiring specialized medical care. Specialized FISH probes to the TUP1-like enhancer of split protein 1 (TUPLE) region of chromosome 22 hybridize within the deleted region. FISH results with only one hybridized probe can diagnose a subchromosomal deletion that could not be detected by conventional karyotype.87
CHROMOSOMAL MICROARRAY ANALYSIS
CMA is a powerful technology with the ability to survey the entire genome and to identify not only chromosomal abnor-malities detected by conventional cytogenetic techniques but also submicroscopic deletions and duplications (CNVs).88 This
of its inability to detect structural rearrangements, mosaicism, marker chromosomes, and uncommon trisomies. Evans and colleagues85 surveyed the results of almost 73,000 prenatal cases from seven centers and reported that only 67% of chromosomal abnormalities would have been detected by routine FISH. This interpretation may be misleading in that some of the missed abnormalities would not have had an impact on fetal develop-ment. Because all abnormalities would be detectable by tissue culture, FISH analysis is not cost-effective. Most practitioners order FISH to offer more rapid reassurance to patients with an unusually high degree of anxiety, or to test fetuses at the highest risk, such as those with ultrasound anomalies. It is also beneficial when rapid results are crucial to subsequent manage-ment, such as with advanced gestational age. FISH on meta-phase chromosomes using probes for unique sequences has greatly expanded the resolution of conventional chromosomal analysis.86 One of the most commonly utilized examples is for
A
C D E
B
Figure 2.4 Chromosomal aberrations detected by fluorescence in situ hybridization (FISH) analysis. (A) Two-color metaphase analysis reveal-ing an unbalanced chromosome rearrangement in a patient with normal karyotype. FISH analysis using probes mapped to the terminal 6p region (red signal) and a control probe, located at the long arm of chromosome 6 (green signal), detected an additional red signal on the short arm of chromosome 2 (arrow). (B) FISH analysis with the chromosome 2 locus-specific probes showing the red and green signals on the normal chromo-some 2. Red signal is absent on the second chromosome 2 (arrow), indicating a deletion on the terminal short arm. (C) A duplication involving the 17p11.2 region (red signal) is detected on interphase cells from a patient with Charcot-Marie-Tooth 1A disease. (D) FISH analysis of interphase amniotic fluid cells detecting three signals for chromosome 21 (red signal) and two signals for chromosome 13 (green signal), indicating a fetus with trisomy 21. (E) Multicolor FISH analysis on paraffin-embedded tissue sections from a missed abortion showing three copies of chromosome 18 (green signal) and a total of three sex chromosomes: two copies of the X chromosome (aqua signal) and one copy of the Y chromosome (red signal), indicating a fetus with triploidy.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0025
s0115
p0320
Resnik_9103_Chapter 2_main.indd 26 3/21/2018 4:10:00 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 27
hybridized sequence can be quantitated (Fig. 2.5). Using this platform, a patient’s genome is compared to a normal control, and readout is expressed by comparative intensity between the patient and the control.89 The advantage of an oligonucleotide array is less noise (variation generated by the experimental method that does not represent true biological variation), and coverage of regions of the genome that do not contain SNPs.
The second popular platform for prenatal diagnosis is a pure SNP array. In an SNP array, probes are chosen from DNA loca-tions known to vary by a single base pair. A patient’s DNA is hybridized to the array, and readout is by absolute intensity of signal from bound DNA fragments (Fig. 2.6). This platform does not require a normal standard because the assay is designed to demonstrate the number of alleles the patient has at each represented locus. Greater than or less than two alleles at any tested locus represents gain or loss of genetic material in that region. This method can detect more abnormalities than just
is a high-throughput technique to detect the relative “dose” of genetic material at thousands of points across the genome. A microarray generally consists of a thin slice of glass or silicon about the size of a postage stamp on which threads of syn-thetic nucleic acids are arrayed. Sample probes are added to the chip, and matches are read by an electronic scanner. The resolution of CMA is on the order of 10 to 400 kb, or more than 100-fold greater resolution than traditional G-banding karyotyping.
Three general microarray platforms are in common use for genome assessment: array comparative genomic hybridization (CGH), pure SNP array, and a combination platform that uses both oligonucleotides and SNPs. The array CGH platform is used to measure differences in copy number or dosage of a particular chromosomal segment. In brief, two genomic librar-ies are mixed and hybridized to a panel of reference oligonucle-otides from across the genome such that relative “doses” of a
A
D E
B C
1
Test
p q p q
2.0
1.0
–1.0
–2.02 copies 2 copies 3 copies
DuplicationTriplication
4 copies1 copy
Deletion
Position, Mb 26.0 27.0 28.0 29.0 36.0 38.0 40.0 42.0 44.0log2
0.0
1.0
–1.0
–2.0
log2
0.0
Control
2
3
Figure 2.5 Array comparative genomic hybridization (CGH). (A) A DNA microarray is usually a microscope slide with a set of short DNA frag-ments from selected regions of the genome spotted onto a surface. (B) A magnified view of the microarray surface after hybridization. (C) Genomic DNAs from the test (patient) and control (normal individual of the same gender) samples are differentially labeled using Cy3 and Cy5 cyanine dyes, mixed, and hybridized onto the array. Spots with an equal amount of Cy3 and Cy5 (spot 1) appear yellow, whereas spots with an extra amount of test DNA look green (spot 2) and spots where the amount of test DNA is decreased appear red (spot 3). (D) Array CGH plot showing a deletion. Probes (black and red dots) are aligned along the X axis according to the physical position on the chromosome (from the short to the long arm). The ratio between the intensity of Cy3 and Cy5 for each probe is calculated and values are placed onto a log2 scale (Y axis). Probes with an equal amount of the test and control DNA (black dots, ratio = 2/2, log2(2/2) = 0) are clustered around a “0” score on the log2 scale. A negative log2 score indicates deletion (red dots; ratio = 1/2, log2(1/2) = −1.0). (E) Array CGH plot showing a complex duplication/triplication rearrangement. Gain in DNA copy number is seen as positive log2 scores. Blue dots represent duplication (ratio = 3/2, log2(3/2) = 0.58). Green dots (ratio = 4/2, log2(4/2) = 1.0) depict a triplication (total four copies of DNA).
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0030
p0325
p0330
Resnik_9103_Chapter 2_main.indd 27 3/21/2018 4:10:02 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
28 PART 1 Scientific Basis of Perinatal Biology
fetal ultrasound. Several studies have demonstrated the incre-mental diagnostic utility of CMA in the setting of a fetus with one or more anomalies on ultrasound but a normal karyotype. A prospective study funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development identified clinically relevant CNVs by microarray in 6% of anomalous fetuses with a normal karyotype.93 Furthermore, the likelihood of identifying either pathogenic CNVs or CNVs of uncertain significance was more likely in fetuses with multiple anomalies, whereas for isolated findings the greatest yield was in fetuses with cardiac and renal anomalies.94 Even in the absence of identified anomalies, CMA should be offered for any patient undergoing invasive sampling, because CMA has been demonstrated to detect a pathogenic or likely pathogenic CNV in approximately 1% of patients with a normal ultrasound and a normal karyotype.95
Clinicians and genetic counselors must continue to exercise reasonable caution when offering microarray analysis and when
copy number (e.g., UPD), and can determine zygosity, pater-nity, degree of consanguinity, parent of origin for a given variant, and maternal cell contamination.90 A third type of plat-form combines both oligonucleotides and SNPs and provides the advantages of diminished noise and SNP information. Table 2.5 summarizes the relative benefits and drawbacks of the most commonly employed microarray platforms.
In neonatal and pediatric studies, microarray results have revealed underlying genetic etiologies for 15% to 20% of cases with previously unexplained developmental delay, intellectual disability, or congenital anomalies. Only about 3% of these cases would have been diagnosed by traditional karyotyping.91 CMA is considered the first-line test of an individual with unex-plained birth defects or mental retardation, or in unexplained stillbirth.92 In contrast to neonatal studies, which have the advantage of correlating genomic findings with complete phys-ical examination and behavioral phenotype, prenatal applica-tions are limited to phenotypic findings that can be detected by
Spot
AA
A-
AAA
AAB
ABB
BBB
AB
BB
B-
--
Genotype Allele A Allele B
2 copies
2 copies
PatientGreen label
Hybridise
Computer analysisand comparison toreference datafile
0 copies
3 copies
3 co
pies
Flu
ores
cenc
eIn
tens
ity
B A
llele
Fre
quen
cy
BB
B–
– –
1 copy
1 co
py
Figure 2.6 Single nucleotide polymorphism (SNP) array. In an SNP array, a patient’s DNA is hybridized to the array and does not require a reference sequence, and readout is by absolute intensity of signal from bound DNA fragments. Resolution will depend on the probe density and may be limited by the nonrandom distribu-tion of SNPs in the genome. A major advantage of SNP arrays over other platforms is the ability to detect trip-loidy, mosaicism, maternal cell contamination, and loss of heterozygosity. (From Karampetsou E, Morrogh D, Chitty L. Microarray technology for the diagnosis of fetal chromosomal aberrations: which platform should we use? J Clin Med. 2014;3:663–678. https://creativecommons.org/licenses/by-nc-sa/3.0/legalcode.)
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0035
p0335
p0340
Resnik_9103_Chapter 2_main.indd 28 3/21/2018 4:10:04 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 29
Although the full clinical effect of the patient’s CNV is not known, the pathogenic nature of the CNV is not in ques-tion. The laboratory should provide an explanation of why the alteration is considered pathogenic, including a list of genes known to be dosage-sensitive that occur in the altered region.
Uncertain clinical significance: This designation represents a fairly broad category, including CNV findings that are later demonstrated to be either clearly pathogenic or clearly benign. Fortunately, additional information on the classification of CNVs is accumulating rapidly, which will reduce the number of findings with uncertain significance in the future, and the current rate of uncertain significance classification is less than 5%. However, if, at the time of reporting, insufficient evidence is available for unequivo-cal determination of clinical significance and the CNV meets the reporting criteria established by the laboratory, the CNV should be reported as a CNV of uncertain clinical significance. This uncertainty should be clear in the report. Laboratories are encouraged to include available evidence for the likelihood that the CNV is pathogenic or benign. Clinicians are encouraged to discuss uncertain variants with the reporting laboratory and to share clinical infor-mation that might affect the interpretation. Referral for genetic counseling in these situations is encouraged.
These categories do not cover all scenarios because each CNV has unique considerations requiring clinical judgment and cor-roboration with phenotypic findings.
Limitations of Chromosomal Microarray AnalysisAlthough CMA is designed to assess genetic imbalance, it does not reach the resolution of single nucleotide variants or very small CNVs below the level of detection. Likewise, balanced rearrangements, such as inversions and reciprocal or insertional translocations, are not detected by CMA. Overall, these occur in approximately 0.6% of individuals.98 One in 2000 prenatal cases has an apparently balanced translocation (0.05%).99 In most cases this does not lead to an altered fetal phenotype, but the information will not be available for reproductive counsel-ing. Notably, CMA can detect some copy number changes near the chromosome breakpoint sites in rearrangements that appear to be balanced on a conventional karyotype.
CMA fails to detect pathogenic copy number changes in areas not represented on the specific array platform. Commercially available arrays include probes that span the entire genome, with denser probe coverage in sequence regions known to have clinical relevance. Denser probe coverage allows for a larger volume of output information, but is more prone to VUS. Less dense probe
interpreting results of microarray findings. Patients are entitled to professional genetic counseling before microarray testing to appropriately discuss the risks of testing, including the possibil-ity of detecting consanguinity, nonpaternity, or genetic variants of uncertain significance (VUS). An excellent CNV database exists through the International Standards for Cytogenomic Arrays Consortium.91 Many CNVs may have dose-dependent phenotypic effects, or may be modified by the presence of other genetic elements such as SNPs.
Traditionally, prenatal screening and testing modalities focused on diseases that significantly affect quality of life and have a fetal, neonatal, or early childhood onset and well-defined phenotypes. With microarray technology, genetic variant rec-ognition may outstrip our current ability to interpret some of these alterations.96 Previously unreported and relatively rare variants with unknown phenotypes may be identified, which requires skilled genetic counseling and interpretation to help patients decide what to do with this information. Informing patients of VUS may generate significant anxiety and negative anticipation. Learning that one’s fetus has a possible abnormal-ity with unquantifiable risks of mysterious consequences natu-rally causes worry, may result in ambivalence about continuing the pregnancy, and has the potential to weigh on the parents’ minds with any perceived “abnormal” phenotype their child may exhibit.
Interpretation of Copy Number VariationAll practitioners offering prenatal CMA should be aware of the reporting criteria of the laboratory analyzing the sample. Guidelines recently provided by ACMG for postnatal CMA interpretation are available and have been adapted for prenatal use.97 These guidelines recommend that the interpreting labora-tory geneticist assign a CNV to one of four main categories of significance to facilitate unambiguous communication of clini-cal significance:
Normal: No copy number changes of clinical significance were identified. Normal results may or may not include mention of copy number changes that were identified and believed to be benign.
Benign: A CNV should be considered benign if it has been reported in multiple peer-reviewed publications or curated databases as a benign variant, particularly if the nature of the CNV has been well characterized, or if the CNV represents a common polymorphism documented in greater than 1% of the population.
Pathogenic: The CNV is documented as clinically significant in multiple peer-reviewed publications, even if penetrance and expressivity of the CNV are known to be variable.
Technique Aneuploidy
Balanced Translocations and Inversions
Unbalanced Translocations Triploidy
AOH/Consanguinity CNVs
Conventional karyotype + + + + − −CGH array + − + − − +SNP array + − + + + +
AOH, Absence of heterozygosity; CGH, comparative genomic hybridization; CNVs, copy number variations; SNP, single nucleotide polymorphism.
From Society for Maternal-Fetal Medicine (SMFM), Dugoff L, Norton ME, Kuller JA. The use of chromosomal microarray for prenatal diagnosis. Am J Obstet Gynecol. 2016;215(4):B2–B9.
TABLE
2.5 Abnormalities Detected With Conventional Karyotype, CGH, and SNP Arrays
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
t0030
p0345
s0120
p0350
u0090
u0095
u0100
u0105
s0125
p0375
p0380
Resnik_9103_Chapter 2_main.indd 29 3/21/2018 4:10:04 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
30 PART 1 Scientific Basis of Perinatal Biology
for genes in which a high proportion of patients may have de novo variants.
HYBRIDIZATION TECHNIQUES: SOUTHERN BLOT, POLYMERASE CHAIN REACTION
The initial molecular diagnostic techniques to make use of the recombinant DNA revolution were based on restriction frag-ment length polymorphisms, generated by cutting amplified DNA sequences using specialized bacterial enzymes called restriction endonucleases. These highly specific enzymes rec-ognize and cut a unique sequence of nucleotides, usually a palindrome of 4 to 8 bp in length. In a palindrome of double-stranded DNA, complementary strands at the cut site will read the same when moving from the 5′ to the 3′ direction, such as GAATTC. Because of this sequence specificity, the pattern of DNA fragments resulting from restriction endonuclease digestion is unique to each gene sequence. The resulting frag-ments are separated by gel electrophoresis, transferred (blotted) onto a membrane, and hybridized with a radioactively labeled probe with known sequence. This technique is called Southern blotting,101 which requires substantial amounts of DNA and is relatively labor intensive and difficult to automate, making it expensive (Fig. 2.7). This approach is still used to identify large repeat expansions for genes subject to dynamic variants, such as in fragile X,102 or to identify large deletions within the dys-trophin gene responsible for Duchenne and Becker muscular dystrophies.103
The development of PCR by Mullis and coworkers in the mid-1980s allowed selective amplification of any desired sequence of DNA, and radically changed the power of DNA diagnostics in terms of sample requirements and assay options.104,105 Synthetic oligonucleotides are used to prime DNA synthesis so that the single-stranded product generated from each primer includes the sequence complementary to the other primer (Fig. 2.8). Multiple temperature-dependent cycles of DNA denaturation, primer annealing, and elongation of DNA synthesis create an exponential increase in copy number or amplification of the DNA sequence between the two primers.
The power of PCR lies in its ability to rapidly replicate any genomic sequence starting from minimal amounts of biological sample. This is useful for tracking known genetic variants, such as genotyping SNPs or identifying disease-associated alleles for single-gene disorders. Alternatively, PCR can identify previously unknown sequence variants that give rise to a clinical pheno-type. As an example, for genes in which no single variant is common among patients, such as the hereditary hearing loss gene GJB2, novel sequence variations can be identified by PCR amplification of an affected patient’s DNA using flanking probes at the gene locus. The PCR reaction generates large amounts of identical DNA copies of the locus in question, and the gene sequence for the affected patient can be analyzed.
When PCR is used to amplify specific DNA fragments, mul-tiple diagnostic tests can be performed on minimal amounts of starting material. Variations in length, such as found in dynamic variants in genes with expandable trinucleotide repeat sequences (e.g., Huntington disease106), can be assayed directly by PCR amplification followed by gel electrophoresis to determine the size of the PCR product. Anonymous marker loci (e.g., SNPs or simple sequence length polymorphisms) can be assayed in the same way for gene mapping and forensic studies. SNPs are amplified singly or in a multiplex combination of loci and
coverage can minimize the chance of a VUS, but it also may fail to detect a rare or novel genomic imbalance. CMA used for pre-natal diagnosis tends to have less dense probe coverage to focus results on areas of known genotype-phenotype correlation.88
CMA arrays that rely solely on oligonucleotide probes do not routinely detect polyploidy, because there are no relative genomic imbalances. SNP arrays, however, can detect trip-loidy.100 Importantly, neither CMA platform can provide infor-mation about the chromosomal mechanism of a genetic imbalance. For example, CMA does not differentiate between nondisjunction and translocation, which may have important implications for recurrence risk counseling.88 So, if a fetus is identified to have trisomy 21 by CMA, conventional karyotyp-ing is then needed as a follow-up to differentiate a full trisomy from an unbalanced translocation; if the latter is found, parents should be karyotyped to identify the balanced carrier.
Ethical Considerations of Genetic Diagnosis in a FetusCommonly identified “pitfalls” of identifying genetic anoma-lies, which lead to formidable counseling challenges, include VUS, identification of adult-onset disease or parental presymp-tomatic disorders, revelation of nonpaternity, unsuspected con-sanguinity, incest, findings linked to diseases with variable expressivity and penetrance, or microdeletions involving a gene linked to cancer development or progression.96 These restraints are amplified in the prenatal setting, where correlation of phe-notypic data is significantly limited. The widespread use of CMA for genetic diagnosis in the pediatric population is strongly informed by evaluation of a patient expressing a defi-nite abnormal phenotype. However, for a fetus, genetic variants identified on CMA may have unclear penetrance or expressivity, which complicates counseling and prognostication.
The weight of the evidence for the reported finding must be carefully considered before irrevocable action is pursued, such as pregnancy termination. The potential impact even goes beyond the tested pregnancy. Incidental findings such as men-delian diseases with adult-onset symptoms or inherited variants in cancer-associated genes raise the risk of labeling the unborn child as well as the parents or extended family with predestined illness. Furthermore, these findings may cause considerable unfounded anxiety throughout pregnancy and into childhood, depending on the strength of disease association. In light of these numerous important issues, pre- and posttest counseling is imperative for the parents to understand the scope and limi-tations of the available genetic technologies.
Genotyping/SequencingThis section provides an overview of many methods to evaluate genetic sequence variation and disease-causing gene character-ization. These techniques can be applied to the gamete, embryo, fetal, or adult genomic DNA to decipher the individual DNA sequence and compare it to known reference standards. DNA diagnostics in medicine can use either direct assays for a spe-cific variant or linkage analysis with polymorphisms linked to a disease locus. Direct assays for specific variants are most useful when relatively few distinct variants account for most patients with a particular form of disease. As analysis methods have become faster, cheaper, and more highly automated, perform-ing direct sequencing of a disease gene without knowing the precise variant has become increasingly practical, particularly
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0385
s0130
p0390
p0395
s0135
p0400
s0140
p0405
p0410
p0415
p0420
Resnik_9103_Chapter 2_main.indd 30 3/21/2018 4:10:04 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 31
full karyotype result within about 4 hours! Rapid karyotyping may be applied in situations with fetal anomalies identified on ultrasound, as a deciding factor as to whether to proceed with chromosomal microarray or if routine karyotype may be suf-ficient for diagnosis.
DNA SEQUENCING
Sequencing determines the complete nucleotide sequence, or specific order of nucleotides in a gene. By listing the full genetic code, variations from an accepted “normal” (reference or con-sensus sequence) may be discovered. This has the potential to uncover pathogenic variants as well as benign variants, and given our limited understanding of how the genome is trans-lated, will potentially identify what are now VUS into a defined clinical phenotype.
The original technique of sequencing, called Sanger sequenc-ing, involves synthesizing multiple copies of DNA that is com-plementary to a single-stranded template of interest using nucleotide-specific chain terminators, or dideoxynucleotide triphosphates (ddATP, ddGTP, ddCTP, ddTTP). This generates synthesized fragments of varying length that can be arranged by size, and the reactions containing each terminating base (A, G, C, or T) are kept separated. Then, by “reading” the terminat-ing base of the synthesized copies from smallest to largest, the sequence of the original single-stranded template is revealed. This molecular method was revolutionary but very time con-suming, labor intensive, and limited to relatively short DNA sequences.
detected by electrophoretic, hybridization, or spectroscopic methods. Multiplex PCR amplifications can allow rapid and parallel analysis of many genetic loci simultaneously.
Perhaps one of the most useful examples of rapid multiplex PCR in prenatal applications is real-time quantitative PCR for rapid karyotype analysis.107 Appropriately selected primers amplify representative genes from each chromosome. Assay parameters are carefully optimized in order to multiplex (simul-taneously run) the full panel of PCR reactions. Moreover, “real-time” technology incorporates fluorescent markers at each round of replication such that tracking the exponential rate of fluorescence increase serves to measure the dose of starting material that was in the reaction.108 The end result is a rapid measurement of the amount of each chromosome from as little starting material as a single cell—that translates to an estimated
Restrictionenzyme
site
GenomicDNA
Restriction enzymecleavage
Electrophoresis
Transfer tonylon filter
Hybridization with32P-labeled probe
X-ray film
Figure 2.7 Southern blotting. DNA is cleaved by a restriction enzyme, separated according to size by agarose gel electrophoresis, and transferred to a filter. After hybridization of the DNA to a labeled probe and exposure of the filter to x-ray film, complementary sequences can be identified.
Target DNAsequence
Denature, anneal, extend
Denature, anneal, extend
25 cycles
106 - 107 copiesof target sequence
Figure 2.8 Polymerase chain reaction (PCR). Repeated synthesis of a specific target DNA sequence (upward arrows) results in exponential amplification. The reaction proceeds from the primers (blue squares, red squares) in the 3′ direction on each strand. The first two cycles of the PCR are shown.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0040
f0045
p0425
s0145
p0430
p0435
Resnik_9103_Chapter 2_main.indd 31 3/21/2018 4:10:05 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
32 PART 1 Scientific Basis of Perinatal Biology
molecular genetic diagnosis rate among all patients referred, and among patients in the study with an abnormal neurologic phenotype, molecular diagnosis was abnormal in as high as 33% of cases.110 Among the 62 patients with likely causative diagnosis, 26% were autosomal recessive, 16% were X-linked, 53% were autosomal dominant, and 50% were de novo variants.
At present, the practical clinical application of sequencing is to search one or many genes (or the whole genome) for a caus-ative variant in the setting of a recognized abnormal phenotype. Small case series in the prenatal setting are accumulating, describing results of WES performed on prenatal samples from fetuses with congenital anomalies. These early data suggest that WES has the potential to significantly increase the proportion of cases for which a genetic etiology can be identified.111 However, larger studies are needed for validation, and wide-spread use of this technology is currently limited by very long turnaround times, prohibitive cost, and generation of high numbers of VUS. Moreover, prenatal genotyping by WES or WGS is not easy to interpret in the setting of limited phenotyp-ing offered by ultrasound. It is therefore prudent to postpone such testing to the postnatal period, when more phenotyping is available to make the interpretation.
Special ApplicationsNONINVASIVE PRENATAL SCREENING
Noninvasive prenatal screening (NIPS) refers to a class of genetic tests designed to detect fetal aneuploidy by quantitation of small fragments of cell-free fetal DNA (cffDNA) circulating in the maternal plasma. The advent of NGS technologies rapidly expanded the amount of data that can be gathered from fetal DNA in maternal plasma in a time frame amenable to prenatal screening applications. As a result, cell-free DNA tests to screen for fetal aneuploidy moved quickly through development and into clinical use by 2011 in the US and Asia, followed by Canada and Europe in 2012.112 NIPS represents the first widespread application of genomic testing in medicine.
In 2008 two groups identified Down syndrome pregnan-cies113,114 by analyzing the cffDNA in the maternal plasma. Using massively parallel shotgun sequencing, the beginning portions of all circulating DNA fragments (both maternal and fetal) were sequenced and identified to determine their specific chromo-somal origin. If the fetus has a third chromosome 21, the per-centage of chromosome 21 fragments compared to disomic chromosomes will be slightly higher than expected. In a preg-nancy in which 10% of the cell-free DNA is fetal, a woman carrying a trisomy 21 fetus should have about 1.05 times more DNA from chromosome 21 fragments than a woman carrying a disomic 21 fetus. Trisomy 21 prediction is based on the ability to distinguish this difference by sequencing millions of frag-ments, identifying their chromosomal origin, and then quanti-fying their relative proportion.
Following the initial success in aneuploidy detection and widespread clinical application of NIPS technology, several dif-ferent platforms are now available to generate sequencing reads of the cffDNA material; platform type determines the speed, cost, and resolution of the commercially available NIPS options. Fig. 2.9 diagrams the key features of the different sequencing and tabulation platforms.115,116 Each of the commercially avail-able NIPS methods uses the same fundamental approach to detecting abnormal fetal DNA complement: (1) an NGS method
Next-generation sequencing (NGS) has revolutionized genetic sequencing capabilities, and moved the fields of science and medicine into the “post-genome” era. NGS involves prepa-ration of a full DNA library (no longer one small segment at a time) by amplifying (making many copies) and fragmenting the DNA source of interest (genomic DNA, coding DNA). After amplification and fragmenting, the DNA library consists of thousands or even millions of small overlapping DNA copy fragments, which are physically bound to a solid surface (plat-form specific, often beads or glass slides). The fragments are loaded into specialized multiplex machines for parallel sequenc-ing; in other words, the sequence of every fragment on the surface can be assayed simultaneously. Individual sequence reads are subsequently aligned (recall the expected overlap due to random fragmentation of many identical copies of DNA) using various bioinformatics platforms for comparison to a reference sequence. The full set of aligned reads reveals the entire sequence of the starting DNA product. Thus, NGS applies the concept of Sanger sequencing to an entire genome with results produced in matter of hours. NGS is a very thorough and powerful method of generating genetic sequence informa-tion. Whereas CMA can simultaneously assess many snippets of DNA sequence from representative regions across the genome, NGS can provide the entire sequence of the substrate DNA, in a matter of hours. This could be likened to quickly finishing a book by reading only the first and last page of every chapter (microarray) versus developing true speed-reading capability to read every single word within a matter of hours.
Whole exome sequencing (WES), which includes only the protein-coding region of DNA, and whole genome sequencing (WGS) are currently in use mostly in the pediatric setting, and are considered the “next frontier” in prenatal genetic diagnostic techniques. WES is designed to determine the DNA sequence of the 20,000 to 25,000 genes that code for known proteins (about 1.5% of the full genome). This coding portion, or exome, is said to contain up to 85% of the variants that have been demonstrated to cause genetic disorders19; however, it is likely that many of the variants in noncoding portions of the genome also play a significant role in human disease. By comparison, WGS requires sequencing of the full genome, including non-coding regions and introns. Data generated from sequencing methods are vast. The primary limitation of both WES and WGS is that accurate clinical interpretation lags behind the ability to generate sequence data. This is because sequencing is high throughput and there are currently no similar high-throughput assays of function to assess putative pathologic sequence findings. This technology generates thousands of vari-ants, and new databases, such as ClinVar and ClinGen as well as the Human Gene Mutation Database, allow for evolving interpretation as more sequence data become available. Cura-tion of variants remains a problem and will be a challenge for years to come. There is enough natural variation in the human genome that any putative finding requires rigorous validation at the level of sequence, molecular function, and interaction within the full biological system. Current recommendations from ACOG and SMFM specify that the use of WES or WGS for prenatal diagnosis be limited to clinical trials until these techniques can be further validated in prenatal samples.109
The first published large clinical series presented WES analy-sis from 250 consecutive patients referred for phenotypes sug-gestive of as-yet unidentified genetic causes (no prenatal cases were included in this series). The study demonstrated a 25%
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0440
p0445
p0450
p0455
s0150
s0155
p0460
p0465
p0470
Resnik_9103_Chapter 2_main.indd 32 3/21/2018 4:10:05 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 33
proportion of the genome represented and the number of sequence reads per amplification round; (2) the reference tags used for alignment of the sequence reads; and (3) the counting statistics applied to generate a readout of relative fetal sequence representation. Fig. 2.9A models a platform commonly called massively parallel sequencing, which is the most resource
is used to produce millions of simultaneous sequencing reads; (2) generated sequences are hybridized to reference templates; and (3) bioinformatics tabulation methods “count” relative rep-resentation of fetal- versus maternal-derived genetic segments. The key differences between the platforms include (1) the breadth and “depth” of sequencing, also expressed as the
ATGGT
Rea
d co
unt
CTAGG
CCTGA
ATGTT
ATGTT
ATGTT
ATGTT
ATGTT
ATGTT
ATGTT
CCTGA
CCTGA
CCTGA
CCTGA
CTAGG
CTAGG
CTAGG
ATGGT
ATGGT
ATGGT
ATGGT
ATGGT
Chr1 ... ... ...Chr13
G+C% correction
Apply counting statistics tocalulate genome representation
Chr18 Chr21
Counting of aligned reads
CCTGA
CCTGA
CCTGA
ATGTT
ATGTT
across the genome
cfDNA in maternal plasma
Maternal DNA
Red blood cell
NGS of total DNA presentin maternal plasma foraneuploidy detection
Random sequencing
Tag-counting approach
Genome-wide shotgun sequencing
SNP-based approach
Targeted sequencing
Non–SNP-based approach
Plasma
Plasmafetal DNA
Ligation
Ligation
probe A
probe B
maternal DNA
Selection of targeted regions
Nontarget locus
Adding locus-specific oligonucleotides
Multiple
Coamplification of targetedregions and sequencing
Sequencing
Apply counting statistics tocalulate genome representation
regions
Target locus
C
Multiplex PCR targeting polymorphicSNPs on the chromosomes of interest
Fetal DNA
A B
SNP1
SNP1
SNP2SNP1
SNP2
Sequencing
CCTGA CCTGA
ATGTT
ATGTT
Calculation of the distributions offetal- and meternal-specific alleles
Mat Fetal
SNP1 2:11:0SNP2
Apply counting statistics tocalulate genome representation
CCTGA
:
Figure 2.9 Noninvasive prenatal screening (cell-free fetal DNA) aneuploidy screening methods. Two major strategies are widely implemented in routine cell-free fetal DNA (cfDNA) aneuploidy testing: random sequencing and targeted sequencing. (A) Random sequencing applies counting statistics on the reads that map to the human reference genome. (B) In targeted sequencing, selected loci with single nucleotide polymorphisms (SNPs) (red and blue stars) are analyzed. The maternal (mat) genotypes are used to model the allelic distributions for every ploidy scenario and based on the actual SNP distributions the likelihood for each hypothesis is calculated. (C) In an alternative targeted sequencing approach, selected fragments are enriched, sequenced, and mapped to the human genome. A chromosome proportion metric is calculated by applying counting statistics. PCR, Polymerase chain reaction. (From Vermeesch JR, Voet T, Devriendt K. Prenatal and pre-implantation genetic diagnosis. Nat Rev Genet. 2016;17:643–656.)
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0050
Resnik_9103_Chapter 2_main.indd 33 3/21/2018 4:10:08 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
34 PART 1 Scientific Basis of Perinatal Biology
intensive due to the depth and breadth of sequencing. Fig. 2.9B represents an SNP allelic ratio platform, and Fig. 2.9C represents a non-SNP allelic ratio platform.
The NIPS clinical performance statistics for detection of spe-cific aneuploidies (trisomy 21, 18, and 13) in a high-risk popu-lation are far better than any other standard screening methods, although NIPS is still not considered diagnostic. A 2016 system-atic review and meta-analysis found that the sensitivity of NIPS for detection of trisomy 21 was 97%, that for trisomy 18 was 93%, and that for trisomy 13 was 95% in a combined high-risk cohort representing 10,000 pregnancies. The positive predictive values in this high-risk group were 91%, 84%, and 87% for trisomy 21, 18, and 13, respectively. In the 100,000 tabulated low-risk pregnancies the positive predictive values of NIPS fell to 82%, 37%, and 49% for trisomy 21, 18, and 13, respectively.117 Although there are several different NIPS platforms, their diag-nostic accuracy, sensitivity, specificity, and positive predictive value are very similar.
There are several important caveats to the use of NIPS, which are critical for the provider to communicate to any patient considering this form of screening. As mentioned previously, while NIPS performs well clinically from the standpoint of a screening test, false negatives do occur. Furthermore, for all screen-positive cases, invasive diagnostic testing is recom-mended. Most commercial platforms offer standard screening for trisomy 21, trisomy 18, and trisomy 13. Noninvasive screen-ing for sex chromosome abnormalities has also become more commonly offered, but with a lower reported sensitivity and specificity than for trisomy 21.118–122 This reduced performance is related to the differing guanine-cytosine content of the chro-mosomes, making sequencing less efficient. Furthermore, there is active debate over how to interpret tests that either do not produce a result, or produce results discrepant from diagnostic testing. About 5% of samples may initially be unacceptable for analysis for a number of reasons, including a low percentage of fetal DNA (low fetal fraction). This rate is higher in patients with a body mass index greater than 30, probably due to the increased apoptosis of maternal cells reducing the percentage of fetal DNA.113,119,123,124 Interestingly, the aneuploidy rate is much higher in samples with an inadequate fetal fraction com-pared to the general population (2.7% versus 0.4%, P < .001), suggesting that “no readout” results should be considered a form of positive screen.125,126 Other causes of inaccurate results include confined placental mosaicism, true fetal mosaicism, maternal sex chromosome abnormality, organ transplant, co-twin demise, maternal chromosomal deletion, maternal neoplasm, maternal fibroids, and laboratory error.111
Current guidelines from multiple US and international pro-fessional societies recommend that the use of cffDNA screening be limited to women with increased risk of fetal aneuploidy. This includes women of advanced maternal age (>35 years at delivery); women with soft markers or structural abnormalities associated with trisomy 21, 18, or 13; prior pregnancy history of a fetus with trisomy 21, 18, or 13; a biochemical screening result positive for increased risk of aneuploidy; or known parental balanced robertsonian translocation with increased risk of trisomy 21, 18, or 13. In a low-risk patient cohort the scope of genetic abnormalities represented will not be as heavily skewed toward Down syndrome, which argues the need for a screening tool with a broader scope such as traditional first-trimester screening. Nonetheless, cffDNA screening is an area of active research and development, and detection capabilities
for a wider range of microdeletion/duplication syndromes may be routine in the near future.127 Of note, ACOG, SMFM, and ACMG have also stated that, in the interest of patient autonomy, NIPS should still be made available to all patients who desire additional testing beyond current professional recommenda-tions. NIPS is superior to serum screening in detecting the common aneuploidies, and studies among all risk individuals indicate that it performs well in low-risk populations. NIPS can be used as a first-tier screening test for aneuploidy detection, followed by invasive testing where needed.
Expanded Applications of Cell-Free Fetal Nucleic Acid TestingApplications of NIPS are rapidly broadening, although these “frontier” applications of cffDNA and cell-free fetal RNA will require rigorous validation before transitioning to routine use. There are promising data on accurate detection of fetal microdeletion syndromes such as 22q11.2 (DiGeorge), 5p (cri du chat), and 1p36 (Noonan) using an SNP-based NIPS approach.128 However, SMFM does not recommend routine screening for microdeletions with cffDNA at this time because clinical validation with patient samples is currently lacking.112 Some commercial laboratories have marketed a cffDNA-based screening test designed to detect genome-wide gains or losses that include DNA regions of 7 Mb or more (similar to resolu-tion of a conventional karyotype).129 Early reports have been published to serve as proof of principle for the derivation of prenatal plasma methylomic and transcriptomic profiles.115 Researchers continue to expand the scope of fetal genetic testing by a noninvasive prenatal approach, promising to drastically enrich our capabilities of prenatal genetic surveillance.
PREIMPLANTATION GENETIC TESTING
Over the past two decades, methods of in vitro fertilization (IVF) and embryo culture and transfer have become routine clinical practice. Simultaneously, the introduction of increas-ingly sophisticated genetic diagnostic procedures now allows preimplantation diagnoses to be performed by testing a few cells of a developing preimplantation (usually day 5 or day 6) blastocyst embryo. This technique was developed initially to benefit patients at high risk for a fetal genetic disorder (parents with known variants). Preimplantation testing allows for selec-tion of unaffected embryos for implantation, and avoids the emotional stress of having to terminate an affected pregnancy. Most of these diagnoses were for relatively rare mendelian disorders.
In recent years, more widespread utilization of embryo testing began with screening preimplantation embryos for aneuploidies to presumably improve implantation rates and take-home pregnancy rates.130 Initial indications for preimplan-tation genetic testing (PGT) have been to improve singleton pregnancy rates by IVF, reduce twinning rates, improve out-comes for patients with repetitive miscarriages, and improve pregnancy rates for women of advanced maternal age. However, randomized controlled data supporting many of these indica-tions are lacking. PGT is now divided into two general catego-ries: high-risk PGT (also known as preimplantation genetic diagnosis [PGD]) and low-risk PGT (also known as preim-plantation genetic screening [PGS]). High-risk PGT (or PGD) refers to analysis carried out for patients at risk of transmit-ting a known genetic or chromosomal abnormality to their
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0475
p0480
p0485
s0160
p0490
s0165
p0495
p0500
Resnik_9103_Chapter 2_main.indd 34 3/21/2018 4:10:08 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 35
During the two-, four-, and eight-cell stages of early embryo development, mosaicism with normal and aneuploid cells may be common, but only the small minority of normal cells will endure and give rise to the embryo. Other drawbacks of these studies included examination of only a select number of chromosomes, errors resulting from single-cell analyses, and embryo biopsy at the cleavage stage, which is a developmental stage known to contain many aneuploid cells that are shed with further embryo growth. It is unlikely that molecular testing would be predictive at cleavage stage because naturally 50% of IVF blastomeres had chromosomal abnormalities and only 9% of embryos were normal diploid in all blastomeres.136
Negative results on this cleavage-stage randomized con-trolled trial did not deter various groups from applying new technologies to biopsy embryos at a later stage of develop-ment. The current “PGS version 2.0” usually refers to embryo biopsy at the blastocyst stage (day 5 or 6), followed by genome-wide aneuploidy detection via array CGH, quantitative PCR, or massive parallel sequencing, and then subsequent frozen elec-tive single embryo transfer. The advantages of trophectoderm biopsy at a blastocyst stage include: (1) the ability to harvest several cells for more DNA to analyze; (2) the blastocyst biopsy is less damaging to the embryo than blastomere biopsy; and (3) there is, in general, less overall aneuploid mosaicism at the blastocyst stage. Massive parallel sequencing (NGS tech-nology) relies on the same principle as WES/WGS sequencing (Fig. 2.10) and has only recently entered PGS.132 While array CGH is considered a gold standard, early claims are being made that massive parallel sequencing may detect clinically signifi-cant mosaicism. However, such claims need to be tempered against the facts that only a few cells are being analyzed, and the site of biopsy may significantly alter detection of mosa-icism; therefore further studies are necessary before massive parallel sequencing can become a standard assay for mosa-icism. A number of small randomized controlled studies have shown 15% to 20% increased implantation and delivery rates with PGS version 2.0.137–140 Other studies on PGS have shown decreased miscarriage rates in women older than 37 years of age who used PGS, and no effect on individuals younger than 35 years.140
offspring. This includes single-gene defects, translocations, and structural chromosomal aberrations. Low-risk PGT (or PGS) is reserved for infertility patients undergoing IVF, with the goal of increasing take-home pregnancy rates by screening for aneu-ploidy.131 PGT raises many ethical questions before conception, including whether to test for adult-onset disorders, whether to use PGS for sex selection outside of medical indications, and whether to transfer embryos with identified pathogenic variants due to family wishes. It is important to keep in mind that any form of genetic testing of the embryo or parents should involve genetic counseling by the health care provider. There is little controversy regarding detecting embryos at risk for heritable mendelian disorders. However, there is significant controversy regarding aneuploidy screening in embryos to improve implan-tation and take-home pregnancy rates, with expert opinions ranging from offering PGS to all women undergoing IVF to recommending that no PGS be offered until further clinical studies are completed to show its utility.132
Preimplantation Genetic Screening for AneuploidyAneuploidy screening by FISH for select chromosomes (1, 13, 16, 17, 18, 21, X, and Y) and preselection of euploid embryos, particularly in women of advanced maternal age, has been sug-gested to improve IVF implantation and pregnancy rates even if no genetic indication for testing is present. This reasoning is supported by the very high number of aneuploid embryos encountered in women over 35 years of age (>30%), a statistic that rises exponentially to 60% by age 40. However, early enthu-siasm for this approach has been tempered by several clinical trials.133,134 One large multicenter, randomized, double-blind, controlled trial conducted between 2003 and 2007 comparing IVF with PGS to standard IVF in 408 women (age range, 35 to 41 years) showed a decreased pregnancy success rate (25% versus 37%) in those receiving PGS compared to those who did not.133 Aneuploidy screening may have failed to improve outcomes because many of the embryos that were rejected on the basis of aneuploidy by PGD FISH results would have been ultimately normal embryos with successful pregnancy potential (perhaps indicating that biopsy of a single blastomere is not representative of the karyotype of the conceptus).135,136
A
0.5Deletion 9p, Trisomy 16 Male
Female
Trisomy 14
–0.5
–1.5
1 2 3 4 5 6 8 97 10 11 12 13 14 15 16 17 18 19 20 21 22 X Y
1 2 3 4 5 6 8 97 10 11 12 13 14 15 16 17 18 19 20 21 22 X Y
0.0
0.5
–0.5
–1.5
0.0
BFigure 2.10 Whole-genome profiling by oligonucleotide comparative genomic hybridization microarray performed on biopsy from a 6-day blastocyst and displayed by Agilent CytoGenomics software 4.0. Chromosomes are plotted in a horizontal orientation and are listed at the bottom of a plot. The Single Cell Recommended Analysis Method was used to detect aberrations with a minimum size of 5 Mb, and minimum log2 ratios of 0.35 for gains and −0.45 for losses. The moving average from an embryonic DNA was compared against the male reference sample (blue line) and the female reference sample (pink line). The gender of an embryo is determined by a copy number of sex chromosomes and by comparison to normal reference male and female DNA. (A) A loss in copy number for the short arm of chromosome 9 (9p deletion) and a gain of all chromo-some 16 probes (trisomy 16) were detected in a male embryo. (B) Chromosome 14 gain (trisomy 14) was observed in a female embryo. Arrows indicate location of abnormal loss and gain in copy numbers.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
f0055
s0170
p0505
p0510
p0515
Resnik_9103_Chapter 2_main.indd 35 3/21/2018 4:10:09 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
36 PART 1 Scientific Basis of Perinatal Biology
found not to have the genetic variant are transferred into the uterus. This is the method that has been most commonly used to date. Finally, PGD can be performed at the blastocyst stage by sampling a portion of the trophectoderm (early placenta). All three approaches appear to be safe, with studies showing no increased risk of birth defects or growth disorders in infants born after PGD when compared to infants born after other assisted reproductive technologies.
Each technique is associated with some limitations. Polar body testing can result in an erroneous diagnosis because of crossing over occurring during meiosis. This limitation has become rare as newer technologies of direct gene testing have been introduced, replacing earlier studies that used linkage markers. However, its major limitation for recessive disorders is that polar body biopsy only determines the maternal contribu-tions to the embryo. A finding that the embryo will have the maternal variant does not differentiate between a carrier and an affected embryo, thus decreasing the number of embryos that are “unaffected” to only those that receive the normal allele from the mother. Blastomere biopsy is subject to error relating to the requirement for DNA amplification from a single cell by PCR. Erroneous amplification of sperm DNA from the zona pellucida, allele dropout of one of the parental alleles during amplification, or both may lead to false-negative results. However, current molecular technologies using SNPs and short tandem repeats allow simultaneous variant detection and marker analysis, almost completely eliminating the risk of mis-diagnosis by sperm contamination. Similarly, SNP microarrays following whole genome amplification provide methods to overcome the allele dropout problem as well. Blastocyst biopsy has the benefit of providing more cells but requires a longer culture period. Because of the late stage when the biopsy is performed, any genetic testing must be done rapidly, within 24 hours, or the biopsied blastocysts must be cryopreserved for later use. With improved embryo cultured conditions, many groups are performing PGD on blastocyst embryos (embryo day 5 or 6), and in many centers, PGD is usually performed in conjunction with PGS so that euploid and pathogenic variant-free embryos are transferred.
In order for PGD to be performed, carrier status of the parents and the precise coordinates of the pathogenic variants are required. It is important to understand that currently PGD only detects inherited disorders, that is, pathogenic variants present in the parents and transmitted to the offspring. PGD will not detect de novo genetic disorders, variants that are not detectable in parental blood but present in the offspring. Impor-tantly, de novo variants contribute as much as 40% to clinically significant phenotypes. It is critical for couples to understand the scope and limitations of current PGD testing. The most common monogenetic disorders evaluated by PGD are CF, β-thalassemia, and SMA among the autosomal recessive disor-ders; myotonic dystrophy, Huntington disease, and Charcot-Marie-Tooth disease among the dominant disorders; and fragile X syndrome, Duchenne or Becker muscular dystrophy, and hemophilia among the X-linked disorders.
PGD for Carriers of Balanced Rearrangements. A parent who is the carrier of a balanced rearrangement typically has a high risk of producing unbalanced embryos, leading to recur-rent miscarriages or a child with an unbalanced rearrangement. PGD permits the transfer of only those embryos with a normal or balanced chromosome complement, and it has been
A number of indications have been proposed for PGS, including recurrent miscarriage, advanced maternal age, dimin-ished ovarian reserve, multiple failed IVF cycles, personal reasons (sex selection), improvement of singleton pregnancy IVF, reduction of twinning, and patient preference for transfer of a euploid embryo. Many couples at risk of carrying a child with a mendelian disorder undergo PGS in addition to PGD. Despite all of the reasons mentioned previously, there is signifi-cant controversy regarding the effectiveness of PGS due to lack of larger multicenter randomized controlled trials, practical problems of obtaining significant number of blastocysts in older patients, reports of euploid deliveries from aneuploidy embryos, and controversies regarding discrepant karyotype and mosaicism in inner cell mass versus trophectoderm.141 Claims of higher implantation rates after PGS are countered by the fact that performing PGS is also associated with a subsequent lower number of embryos for transfer and/or cryopreservation. The lack of consensus regarding the overall clinical utility of PGS will hopefully improve with outcomes of additional trials that are underway.132 Nonetheless, the attractiveness of assessing and only transferring seemingly euploid embryos has become com-monplace in the United States.
Careful counseling of couples regarding the pros and cons of embryo aneuploidy screening is very important. It is also critical to understand the limitations of PGS and to communi-cate these limitations to the couple considering this procedure. Errors in PGS can arise due to mislabeling of samples, contami-nation with extraneous DNA, technical problems (amplifica-tion failure, array noise), discrepancy between inner cell mass karyotype and trophectoderm karyotype, and mosaicism in the trophectoderm sample. Moreover, PGS is a screening test, and the detection rate is not 100%. Screening is limited to whole chromosome gain or loss and will not detect subchromosomal deletions/duplications. PGS also does not test for whole chro-mosome mosaicism, triploidy (three sets of each chromosome), or genetic conditions caused by single-gene variants (such as CF). The false-negative rate for microarray PGS is lower than 1%. Every couple, regardless of their ethnic background and family history, has a 3% to 5% risk for birth defects with each pregnancy, and even if the result of PGS is normal, the baby could still have one or more birth defects or intellectual dis-ability from causes not detected by PGS testing. PGS does not replace prenatal testing such as CVS or amniocentesis. Stan-dard prenatal screening or testing should still be made available to patients undergoing IVF, including patients who had PGS. Women who do not desire to undergo diagnostic procedures due to associated risk of loss can be offered cffDNA screening test with all the caveats associated with such testing.
Preimplantation Genetic DiagnosisPGD for Mendelian Disorders. PGD is used to describe genetic testing that occurs before an embryo implants in the uterus. Three approaches have been utilized for PGD to date. The first approach was based on polar body removal, and the genetic status of the oocyte was inferred from the results of the polar body assay. In the circumstance in which the polar body has the mutated gene, the oocyte is inferred to be “normal,” and therefore an embryo obtained by fertilization of this oocyte would be unaffected with the genetic condition of interest. A second method of PGD is blastomere biopsy, in which one or two blastomeres are removed from an eight-cell (day 3) embryo and analyzed for the genetic condition of interest. Only embryos
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
p0520
p0525
s0175
s0180
p0530
p0535
p0540
s0185
p0545
Resnik_9103_Chapter 2_main.indd 36 3/21/2018 4:10:09 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 37
nonhuman organ donor, or crops that carry variants to grow faster and be disease resistant. Routine application of genome editing to humans is unlikely to occur soon due to various problems, including generation of mosaic embryos, off-target effects (genetic editing at nonprescribed sites) with unintended consequences, and overall safety concerns inherent in new tech-nologies. Research in this arena should be allowed to proceed because there are significant benefits that genetically affected human embryos may derive in the future.
ConclusionThe past two decades have yielded revolutionary advances in reproductive genetic technology. Curation of human genome sequence information in the years since completion of the Human Genome Project and expanding applications of NGS have provided seemingly endless genotype data, and work is ongoing to translate that information to correlated phenotypes and reduce the burden of VUS. Access to genetic material has also burgeoned, with improved understanding of embryonic development, results of embryo biopsy, and ongoing explora-tion of data available from cell-free DNA. With rapidly devel-oping technologies at our disposal, reproductive and obstetrics professionals have a responsibility to connect patients with resources to ensure full understanding of the benefits and limi-tations of various screening and diagnostic options. Obtaining genetic information prior to conception or birth is fundamen-tal to making informed reproductive decisions, particularly for patients with a personal, family, or obstetric history signifying elevated risk for a genetic disorder. Often a combination of a long-standing diagnostic method (such as karyotyping) and a more recently developed technology (array CGH) will be the best approach to generate clinically useful information. Exciting new technologies are in development, and should continue to be held to high standards of scientific rigor and clinical valida-tion before entering mainstream practice.
Key Points• There is a significant amount of naturally occurring
genetic variation in the human genome. Single nucleotide polymorphisms (SNPs) introduce genetic variation at the level of individual base substitutions, while copy number variations (CNVs) represent variation in the “dose” of a relatively large DNA segment (1000 to 500,000 bp or more). The biological implications of genetic variants depend on the gene or genes affected by the change in DNA.
• The term mutation has been replaced by the term variant, which can be classified as benign, likely benign, of unknown significance, likely pathogenic, or pathogenic.
• Genetic disease ranges from abnormal numbers of whole chromosomes, to phenotypes caused by loss or gain of subchromosomal DNA segments containing several con-tiguous genes (called microdeletions and microduplica-tions), to single-gene disorders (also called mendelian disorders). Human disease may also have a genetic basis with a more complex genotype-phenotype correlation, such as autism, which may involve multiple genes in addi-tion to environmental influences.
• Genetic screening and testing should be accompanied by patient education, genetic counseling, timely disclosure of
demonstrated to significantly improve outcomes.142,143 An impressive report comes from Otani and colleagues,144 who assessed PGD in 33 couples with repetitive miscarriages and no liveborn children, in which one member of the couple is a translocation carrier. After PGD (an average of 1.24 cycles per patient), only 18% of the total embryos were either balanced or normal: 20 of 88 embryos from robertsonian translocation car-riers and 86 of 491 from reciprocal translocation carriers. Of the 19 subsequent pregnancies in which normal or balanced embryos were implanted, just one (5%) miscarried; the other 18 pregnancies proceeded into the second trimester or culmi-nated in a live birth.
Ethical Issues Surrounding Preimplantation Genetic DiagnosisPGD has raised numerous ethical issues. It allows individu-als with adult-onset disorders, such as carriers for the BRCA1 variant, to carry embryos free of the pathogenic variants. PGD for adult-onset conditions is ethically justified both in cases when the condition is serious and for adult-onset conditions of lesser severity or penetrance.145 Significant counseling regard-ing PGD in such cases should include detailed review of the adult condition from which the parent suffers, the degree of penetrance and expressivity of such condition, and medical interventions to manage the condition, as well as the overall residual risk of genetic disorders. Penetrance of many patho-genic variants for individual conditions is below 100%, and intrafamily variation is significant and should be understood by the patient. Publicly funded databases such as ClinGen are striving to curate all the pathogenic variants and provide clinicians with guidelines regarding phenotypes and medical interventions. Another set of ethical considerations arises when individuals want to transfer embryos with genetic anomalies.146 Such requests are rare, and may involve individuals who them-selves are affected with conditions such as hearing loss and achondroplasia and would like to rear children with a similar phenotype. Extensive and highly individualized counseling in such situations is important, as for any PGD procedure, and should involve discussion about the condition; the full spec-trum of the phenotype expressivity and penetrance as well as the potential lethality; and the emotional, physical, and finan-cial effects that such a condition may have on the family unit. If the provider is not willing to assist the patients with their requests, patients should be given the option to seek help else-where. Overwhelming numbers of individuals with genetic conditions are born to couples without infertility problems, and therefore individuals who seek assisted reproductive ser-vices should likewise have the same choices. Nonetheless, in circumstances in which a child is highly likely to be born with a severe condition that is associated with severe handicap and suffering, the physician can refuse to transfer such embryos.
Much controversy has also been generated surrounding the use of newly available genome editing technologies, such as clustered regularly-interspaced short palindromic repeats/CRISPR-associated protein 9 (CRISPR/Cas9), to edit embryo genomes. Genome editing theoretically can be used to revert a pathogenic variant in the embryo to a benign variant. Alterna-tively, it could be used to “enhance” the embryo, with variants that can, for example, prevent infection with human immuno-deficiency virus or provide other advantages. Genome editing is now widely used in animals and plants for various purposes, including pigs that carry variants that allow them to be a
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
s0190
p0550
p0555
s0195
p0560
s0200
p0565
u0115
u0120
u0125
Resnik_9103_Chapter 2_main.indd 37 3/21/2018 4:10:09 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
38 PART 1 Scientific Basis of Perinatal Biology
transfer of the fragments to a membrane where they can be probed for the DNA segment of interest. This technique is commonly used to identify large repeat expansions for genes subject to dynamic variations, such as in fragile X syndrome.
• When PCR is used to amplify specific DNA fragments, multiple diagnostic genetic tests can be performed on minimal amounts of starting material.
• Next-generation sequencing (NGS) is the revolutionary technology that changed the scale of genetic testing pos-sibilities. NGS, or massively parallel sequencing, is an automated technology that generates millions of simulta-neous sequencing reads. NGS can be used to sequence entire genomes or constrained to specific areas of interest, including all protein-coding genes (a whole exome) or small numbers of individual genes.
• Current recommendations from ACOG and SMFM specify that use of whole exome sequencing (WES) or whole genome sequencing (WGS) for prenatal diagnosis be limited to clinical trials until these techniques can be further validated in prenatal samples.
• The diagnostic accuracy of molecular genetic techniques depends on the source of DNA, the percentage of the total genome that is assessed in any given technique and, for sequencing technology, the depth of sequence assessment (the number of overlapping sequence reads for a given segment of DNA).
• Noninvasive prenatal screening (NIPS) uses NGS of cell-free DNA derived from maternal plasma coupled with bioinformatics algorithms to determine fetal ploidy (chro-mosome count). The available tests have a high sensitivity and specificity for common trisomies (21, 18, 13); however, the predictive value of the tests is significantly different depending on the prevalence of aneuploidy in the popula-tion being tested. NIPS is an excellent screening tool for common aneuploidies in high-risk populations; however, limitations in predictive value should be discussed with patients who desire additional testing beyond current pro-fessional recommendations.
• Women whose reports from NIPS are indeterminate or uninterpretable have an increased risk of aneuploidy and should undergo comprehensive ultrasound evaluation and genetic counseling with the option for diagnostic genetic testing.
• Low-risk preimplantation genetic testing (also known as preimplantation genetic screening [PGS]) is an option for infertility patients undergoing in vitro fertilization (IVF), with the goal of increasing take-home pregnancy rates by screening for aneuploidy. There is significant controversy regarding the effectiveness of PGS due to lack of larger multicenter randomized controlled trials.
• High-risk preimplantation genetic testing (also known as preimplantation genetic diagnosis [PGD]) involves genetic testing on embryos prior to implantation, from parents with identified risk of transmitting a known genetic or chromosomal abnormality to their offspring. PGD detects only inherited disorders, and will not detect de novo genetic variants, which contribute as much as 40% to clinically significant phenotypes.
A full reference list is available online at ExpertConsult.com.
test results to patients, and the availability of “next steps” (such as definitive prenatal genetic testing) in the event of positive results.
• Carrier screening refers to genetic testing of asymptomatic individuals to determine if they carry one or more disease-associated genetic variants. Ethnic-based carrier screening is targeted to specific ethnic populations known to be at increased risk for particular disorders. Pan-ethnic carrier screening tests for a select panel of disorders in all patients, regardless of ethnicity.
• Genetic risk assessment before or during pregnancy may be indicated based on family history, prior obstetric history, parental age, or ethnic background. Additionally, it is acceptable for any patient, regardless of risk, to choose diagnostic prenatal genetic testing after informed consent.
• Benefits of genetic testing include optimization of neona-tal outcomes by planning appropriate delivery staffing and location, identification of disorders for which in utero treatment may provide benefit, the option of pregnancy termination or preimplantation selection, and providing reassurance when results are normal.
• The fetus, amniocytes, and chorionic villi each develop from different cell lines in early embryo development. Thus it is possible for tissue samples from each of these sources to have disparate karyotypes resulting from abnor-mal chromosome segregation. The earlier in development that an abnormal chromosomal segregation event such as nondisjunction or trisomy rescue occurs, the more wide-spread the mosaicism may be in the differentiated organ-ism (i.e., more likely to affect both the chorion/placenta and the fetus). Later chromosomal segregation events are more likely to be confined to specific cell types, giving rise to clinical findings such as confined placental mosaicism, which leads to discordant karyotypes between chorionic villus sampling (CVS) and amniocentesis. Factors influ-encing the likelihood of fetal involvement for a mosaic aneuploidy result include the specific chromosome involved and the tissue source where the aneuploidy was detected.
• CVS and amniocentesis samples can be assessed by direct analysis and by analysis following long-term culture (approximately 1 week). There are benefits and draw-backs to each method, but diagnostic accuracy is maxi-mized when both direct and culture methods are used concurrently. For both CVS and amniocentesis, long-term culture gives more accurate diagnostic capability for fetal karyotype.
• The molecular resolution of a G-banded karyotype is 5 Mb, which allows detection of chromosome number changes and relatively large structural chromosome rearrangements.
• Chromosomal microarray analysis (CMA) is a technique that samples across the whole genome with resolution down to a 50- to 100-kb level. CMA allows for detection of CNVs, including microdeletions and microduplications that would not be diagnosed on karyotype. Microarray is recommended for genetic analysis in cases with sonographic fetal anomalies, and can be considered in any patient who chooses to undergo diagnostic prenatal testing.
• Southern blotting involves enzymatic digestion of DNA at unique cut sites, separation of fragment sizes on a gel, and
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
u0130
u0135
u0140
u0145
u0150
u0155
u0160
u0165
u0170
u0175
u0180
u0185
u0190
u0195
u0200
u0205
p0670
Resnik_9103_Chapter 2_main.indd 38 3/21/2018 4:10:10 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 38.e1
REFERENCES
1. Medland SE, Nyholt DR, Painter JN, et al. Common variants in the trichohyalin gene are associated with straight hair in Europeans. Am J Hum Genet. 2009;85:750.
2. Gasche Y, Daali Y, Fathi M, et al. Codeine intox-ication associated with ultrarapid CYP2D6 metabolism. N Engl J Med. 2004;351:2827.
3. Bijl MJ, Visser LE, Hofman A, et al. Influence of the CYP2D6*4 polymorphism on dose, switching and discontinuation of antidepres-sants. Br J Clin Pharmacol. 2008;65:558.
4. Iafrate AJ, Feuk L, Rivera MN, et al. Detec-tion of large-scale variation in the human genome. Nat Genet. 2004;36:949.
5. Sebat J, Lakshmi B, Troge J, et al. Large-scale copy number polymorphism in the human genome. Science. 2004;305:525.
6. Redon R, Ishikawa S, Fitch KR, et al. Global variation in copy number in the human genome. Nature. 2006;444:444.
7. den Dunnen JT, Dalgleish R, Maglott DR, et al. HGVS recommendations for the description of sequence variants: 2016 update. Hum Mutat. 2016;37:564.
8. Veltman JA, Brunner HG. De novo mutations in human genetic disease. Nat Rev Genet. 2012;13:565.
9. American College of Obstetricians and Gyne-cologists. Practice bulletin no. 162: prenatal diagnostic testing for genetic disorders. Obstet Gynecol. 2016;127:e108.
10. Committee on Genetics. Committee opinion no. 691: carrier screening for genetic condi-tions. Obstet Gynecol. 2017;129:e41.
11. Committee on Genetics. Committee opinion no. 690: carrier screening in the age of genomic medicine. Obstet Gynecol. 2017;129:e35.
12. Committee on Genetics. Committee opinion no. 693: counseling about genetic testing and communication of genetic test results. Obstet Gynecol. 2017;129:e96.
13. Absalan F, Ronaghi M. Molecular inversion probe assay. Methods Mol Biol. 2007;396:315.
14. Daly TM, Dumaual CM, Miao X, et al. Mul-tiplex assay for comprehensive genotyping of genes involved in drug metabolism, excretion, and transport. Clin Chem. 2007;53:1222.
15. Wang Y, Moorhead M, Karlin-Neumann G, et al. Analysis of molecular inversion probe performance for allele copy number determi-nation. Genome Biol. 2007;8:R246.
16. Srinivasan BS, Evans EA, Flannick J, et al. A universal carrier test for the long tail of mendelian disease. Reprod Biomed Online. 2010;21:537.
17. Edwards JG, Feldman G, Goldberg J, et al. Expanded carrier screening in reproductive medicine-points to consider: a joint statement of the American College of Medical Genetics and Genomics, American College of Obstetri-cians and Gynecologists, National Society of Genetic Counselors, Perinatal Quality Founda-tion, and Society for Maternal-Fetal Medicine. Obstet Gynecol. 2015;125:653.
18. American College of Obstetricians and Gyne-cologists. Practice bulletin no. 175: ultra-sound in pregnancy. Obstet Gynecol. 2016;128: e241.
19. Norton ME, Rink BD. Changing indications for invasive testing in an era of improved screening. Semin Perinatol. 2016;40:56.
20. Harper JC, Delhanty JD. Preimplantation genetic diagnosis. Curr Opin Obstet Gynecol. 2000;12:67.
21. Hardy K, Martin KL, Leese HJ, et al. Human preimplantation development in vitro is not adversely affected by biopsy at the 8-cell stage. Hum Reprod. 1990;5:708.
22. Bianchi DW, Simpson JL, Jackson LG, et al. Fetal gender and aneuploidy detection using fetal cells in maternal blood: analysis of NIFTY I data. National institute of child health and development fetal cell isolation study. Prenat Diagn. 2002;22:609.
23. Lo YM, Corbetta N, Chamberlain PF, et al. Presence of fetal DNA in maternal plasma and serum. Lancet. 1997;350:485.
24. Lo YM. Fetal DNA in maternal plasma: biology and diagnostic applications. Clin Chem. 1903;46:2000.
25. Angert RM, LeShane ES, Lo YM, et al. Fetal cell-free plasma DNA concentrations in mater-nal blood are stable 24 hours after collection: analysis of first- and third-trimester samples. Clin Chem. 2003;49:195.
26. Bianchi DW, Lo YM. Fetomaternal cellular and plasma DNA trafficking: the yin and the yang. Ann N Y Acad Sci. 2001;945:119.
27. Zhong XY, Holzgreve W, Hahn S. Cell-free fetal DNA in the maternal circulation does not stem from the transplacental passage of fetal eryth-roblasts. Mol Hum Reprod. 2002;8:864.
28. Halicka HD, Bedner E, Darzynkiewicz Z. Seg-regation of RNA and separate packaging of DNA and RNA in apoptotic bodies during apoptosis. Exp Cell Res. 2000;260:248.
29. Guibert J, Benachi A, Grebille AG, et al. Kinet-ics of SRY gene appearance in maternal serum: detection by real time PCR in early pregnancy after assisted reproductive technique. Hum Reprod. 1733;18:2003.
30. Norton ME, Brar H, Weiss J, et al. Non-invasive chromosomal evaluation (NICE) study: results of a multicenter prospective cohort study for detection of fetal trisomy 21 and trisomy 18. Am J Obstet Gynecol. 2012;207:137e1.
31. Lo YM, Zhang J, Leung TN, et al. Rapid clear-ance of fetal DNA from maternal plasma. Am J Hum Genet. 1999;64:218.
32. American College of Obstetricians and Gyne-cologists. Practice bulletin no. 163: screen-ing for fetal aneuploidy. Obstet Gynecol. 2016;127:e123.
33. Akolekar R, Beta J, Picciarelli G, et al. Pro-cedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: a systematic review and meta-analysis. Ultra-sound Obstet Gynecol. 2015;45:16.
34. Taylor TH, Gitlin SA, Patrick JL, et al. The origin, mechanisms, incidence and clinical consequences of chromosomal mosaicism in humans. Hum Reprod Update. 2014;20:571.
35. Hecht F, Peakman DC, Kaiser-McCaw B, et al. Amniocyte clones for prenatal cytogenetics. Am J Med Genet. 1981;10:51.
36. Kuller JA, Chescheir N, Cefalo RC. Prenatal Diagnosis & Reproductive Genetics. St. Louis, MO: Mosby; 1996.
37. Reid R, Sepulveda W, Kyle PM, et al. Amniotic fluid culture failure: clinical significance and association with aneuploidy. Obstet Gynecol. 1996;87:588.
38. Hsu LY, Perlis TE. United states survey on chro-mosome mosaicism and pseudomosaicism in prenatal diagnosis. Prenat Diagn. 1984;4(Spec No):97.
39. Bui TH, Iselius L, Lindsten J. European collab-orative study on prenatal diagnosis: mosaicism,
pseudomosaicism and single abnormal cells in amniotic fluid cell cultures. Prenat Diagn. 1984;4(Spec No):145.
40. Johnson A, Wapner RJ. Mosaicism: implica-tions for postnatal outcome. Curr Opin Obstet Gynecol. 1997;9:126.
41. Lestou VS, Kalousek DK. Confined placental mosaicism and intrauterine fetal growth. Arch Dis Child Fetal Neonatal Ed. 1998;79:F223.
42. Gosden C, Nicolaides KH, Rodeck CH. Fetal blood sampling in investigation of chromo-some mosaicism in amniotic fluid cell culture. Lancet. 1988;1:613.
43. Berghella V, Wapner RJ, Yang-Feng T, et al. Prenatal confirmation of true fetal trisomy 22 mosaicism by fetal skin biopsy following normal fetal blood sampling. Prenat Diagn. 1998;18:384.
44. Handling chorionic villi for direct chromo-some studies. Lancet. 1983;2:1491.
45. Simoni G, Brambati B, Danesino C, et al. Effi-cient direct chromosome analyses and enzyme determinations from chorionic villi samples in the first trimester of pregnancy. Hum Genet. 1983;63:349.
46. Chang HC, Jones OW, Masui H. Human amniotic fluid cells grown in a hormone-supplemented medium: suitability for pre-natal diagnosis. Proc Natl Acad Sci USA. 1982;79:4795.
47. Pittalis MC, Dalpra L, Torricelli F, et al. The predictive value of cytogenetic diagnosis after CVS based on 4860 cases with both direct and culture methods. Prenat Diagn. 1994;14:267.
48. Sachs ES, Jahoda MG, Los FJ, et al. Interpreta-tion of chromosome mosaicism and discrep-ancies in chorionic villi studies. Am J Med Genet. 1990;37:268.
49. Martin AO, Simpson JL, Rosinsky BJ, et al. Chorionic villus sampling in continuing preg-nancies. II. Cytogenetic reliability. Am J Obstet Gynecol. 1986;154:1353.
50. Bartels I, Hansmann I, Holland U, et al. Down syndrome at birth not detected by first-trimes-ter chorionic villus sampling. Am J Med Genet. 1989;34:606.
51. Poenaru L. First trimester prenatal diagnosis of metabolic diseases: a survey in countries from the european community. Prenat Diagn. 1987;7:333.
52. Ledbetter DH, Martin AO, Verlinsky Y, et al. Cytogenetic results of chorionic villus sam-pling: high success rate and diagnostic accu-racy in the United States Collaborative Study. Am J Obstet Gynecol. 1990;162:495.
53. Williams J 3rd, Medearis AL, Chu WH, et al. Maternal cell contamination in cultured chorionic villi: comparison of chromosome q-polymorphisms derived from villi, fetal skin, and maternal lymphocytes. Prenat Diagn. 1987;7:315.
54. Ledbetter DH, Zachary JM, Simpson JL, et al. Cytogenetic results from the U.S. Collaborative study on CVS. Prenat Diagn. 1992;12:317.
55. Boehm FH, Salyer SL, Dev VG, et al. Chorionic villus sampling: quality control–a continuous improvement model. Am J Obstet Gynecol. 1766;168:1993.
56. Winsor EJ, Akoury H, Chitayat D, et al. The role of molecular microsatellite identity testing to detect sampling errors in prenatal diagnosis. Prenat Diagn. 2010;30:746.
57. Kalousek DK, Howard-Peebles PN, Olson SB, et al. Confirmation of CVS mosaicism in
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
Resnik_9103_Chapter 2_main.indd 1 3/21/2018 4:10:10 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
38.e2 PART 1 Scientific Basis of Perinatal Biology
term placentae and high frequency of intra-uterine growth retardation association with confined placental mosaicism. Prenat Diagn. 1991;11:743.
58. Mardy A, Wapner RJ. Confined placental mosaicism and its impact on confirmation of NIPT results. Am J Med Genet C Semin Med Genet. 2016;172:118.
59. Wolstenholme J. Confined placental mosa-icism for trisomies 2, 3, 7, 8, 9, 16, and 22: their incidence, likely origins, and mechanisms for cell lineage compartmentalization. Prenat Diagn. 1996;16:511.
60. Cassidy SB, Lai LW, Erickson RP, et al. Trisomy 15 with loss of the paternal 15 as a cause of Prader-Willi syndrome due to maternal disomy. Am J Hum Genet. 1992;51:701.
61. Purvis-Smith SG, Saville T, Manass S, et al. Uniparental disomy 15 resulting from “correc-tion” of an initial trisomy 15. Am J Hum Genet. 1992;50:1348.
62. Ledbetter DH, Engel E. Uniparental disomy in humans: development of an imprinting map and its implications for prenatal diagnosis. Hum Mol Genet. 1757;4(Spec No):1995.
63. Worton RG, Stern R. A canadian collabora-tive study of mosaicism in amniotic fluid cell cultures. Prenat Diagn. 1984;4(Spec No):131.
64. Kalousek DK, Dill FJ, Pantzar T, et al. Con-fined chorionic mosaicism in prenatal diagno-sis. Hum Genet. 1987;77:163.
65. Goldberg JD, Porter AE, Golbus MS. Current assessment of fetal losses as a direct conse-quence of chorionic villus sampling. Am J Med Genet. 1990;35:174.
66. Johnson A, Wapner RJ, Davis GH, et al. Mosa-icism in chorionic villus sampling: an asso-ciation with poor perinatal outcome. Obstet Gynecol. 1990;75:573.
67. Wapner RJ, Simpson JL, Golbus MS, et al. Chorionic mosaicism: association with fetal loss but not with adverse perinatal outcome. Prenat Diagn. 1992;12:347.
68. Breed AS, Mantingh A, Vosters R, et al. Follow-up and pregnancy outcome after a diagnosis of mosaicism in CVS. Prenat Diagn. 1991;11:577.
69. Post JG, Nijhuis JG. Trisomy 16 confined to the placenta. Prenat Diagn. 1992;12:1001.
70. Phillips OP, Tharapel AT, Lerner JL, et al. Risk of fetal mosaicism when placental mosaicism is diagnosed by chorionic villus sampling. Am J Obstet Gynecol. 1996;174:850.
71. Benn P. Trisomy 16 and trisomy 16 mosaicism: a review. Am J Med Genet. 1998;79:121.
72. Vejerslev LO, Mikkelsen M. The european col-laborative study on mosaicism in chorionic villus sampling: data from 1986 to 1987. Prenat Diagn. 1989;9:575.
73. Fassihi H, McGrath JA. Prenatal diagno-sis of epidermolysis bullosa. Dermatol Clin. 2010;28:231.
74. Evans MI, Krivchenia EL, Johnson MP, et al. In utero fetal muscle biopsy alters diagnosis and carrier risks in Duchenne and Becker muscular dystrophy. Fetal Diagn Ther. 1995;10:71.
75. Kuller JA, Hoffman EP, Fries MH, et al. Pre-natal diagnosis of Duchenne muscular dystro-phy by fetal muscle biopsy. Hum Genet. 1992; 90:34.
76. Suren A, Grone HJ, Kallerhoff M, et al. Pre-natal diagnosis of congenital nephrosis of the Finnish type (CNF) in the second trimester. Int J Gynaecol Obstet. 1993;41:165.
77. Johnson MP, Bukowski TP, Reitleman C, et al. In utero surgical treatment of fetal obstructive uropathy: a new comprehensive approach to
identify appropriate candidates for vesicoam-niotic shunt therapy. Am J Obstet Gynecol. 1770;170:1994.
78. Klinger K, Landes G, Shook D, et al. Rapid detection of chromosome aneuploidies in uncultured amniocytes by using fluorescence in situ hybridization (FISH). Am J Hum Genet. 1992;51:55.
79. Ward BE, Gersen SL, Carelli MP, et al. Rapid prenatal diagnosis of chromosomal aneu-ploidies by fluorescence in situ hybridization: clinical experience with 4,500 specimens. Am J Hum Genet. 1993;52:854.
80. Cheong Leung W, Chitayat D, Seaward G, et al. Role of amniotic fluid interphase fluorescence in situ hybridization (FISH) analysis in patient management. Prenat Diagn. 2001;21:327.
81. Sawa R, Hayashi Z, Tanaka T, et al. Rapid detection of chromosome aneuploidies by prenatal interphase FISH (fluorescence in situ hybridization) and its clinical utility in japan. J Obstet Gynaecol Res. 2001;27:41.
82. Tepperberg J, Pettenati MJ, Rao PN, et al. Pre-natal diagnosis using interphase fluorescence in situ hybridization (FISH): 2-year multi-center retrospective study and review of the literature. Prenat Diagn. 2001;21:293.
83. Weremowicz S, Sandstrom DJ, Morton CC, et al. Fluorescence in situ hybridization (FISH) for rapid detection of aneuploidy: experience in 911 prenatal cases. Prenat Diagn. 2001;21:262.
84. Technology Transfer Committee, American College of Medical Genetics. Technical and clinical assessment of fluorescence in situ hybridization: an ACMG/ASHG position statement. I. Technical considerations. Test and technology transfer committee. Genet Med. 2000;2:356.
85. Evans MI, Goldberg JD, Horenstein J, et al. Selective termination for structural, chromo-somal, and Mendelian anomalies: international experience. Am J Obstet Gynecol. 1999;181:893.
86. Pergament E. The application of fluorescence in-situ hybridization to prenatal diagnosis. Curr Opin Obstet Gynecol. 2000;12:73.
87. McDonald-McGinn DM, Emanuel BS, Zackai EH. 22q11.2 Deletion Syndrome, in Genereviews(r). Seattle (WA): 1993.
88. Society for Maternal-Fetal Medicine. Elec-tronic address pso, Dugoff L, Norton ME, et al. The use of chromosomal microarray for prenatal diagnosis. Am J Obstet Gynecol. 2016;215:B2.
89. Snijders AM, Nowak N, Segraves R, et al. Assembly of microarrays for genome-wide measurement of DNA copy number. Nat Genet. 2001;29:263.
90. Beaudet AL, Belmont JW. Array-based DNA diagnostics: let the revolution begin. Annu Rev Med. 2008;59:113.
91. Miller DT, Adam MP, Aradhya S, et al. Consen-sus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. Am J Hum Genet. 2010;86:749.
92. Hillman SC, Willams D, Carss KJ, et al. Prena-tal exome sequencing for fetuses with struc-tural abnormalities: the next step. Ultrasound Obstet Gynecol. 2015;45:4.
93. Wapner RJ, Martin CL, Levy B, et al. Chromo-somal microarray versus karyotyping for pre-natal diagnosis. N Engl J Med. 2012;367:2175.
94. Donnelly JC, Platt LD, Rebarber A, et al. Asso-ciation of copy number variants with specific ultrasonographically detected fetal anomalies. Obstet Gynecol. 2014;124:83.
95. Reddy UM, Page GP, Saade GR, et al. Karyo-type versus microarray testing for genetic abnormalities after stillbirth. N Engl J Med. 2012;367:2185.
96. Yatsenko SA, Davis S, Hendrix NW, et al. Application of chromosomal microarray in the evaluation of abnormal prenatal findings. Clin Genet. 2013;84:47.
97. Kearney HM, Thorland EC, Brown KK, et al. American College of Medical Genetics stan-dards and guidelines for interpretation and reporting of postnatal constitutional copy number variants. Genet Med. 2011;13:680.
98. Giardino D, Corti C, Ballarati L, et al. De novo balanced chromosome rearrangements in pre-natal diagnosis. Prenat Diagn. 2009;29:257.
99. Warburton D. De novo balanced chromosome rearrangements and extra marker chromo-somes identified at prenatal diagnosis: clinical significance and distribution of breakpoints. Am J Hum Genet. 1991;49:995.
100. Conlin LK, Thiel BD, Bonnemann CG, et al. Mechanisms of mosaicism, chimerism and uniparental disomy identified by single nucle-otide polymorphism array analysis. Hum Mol Genet. 2010;19:1263.
101. Southern EM. Detection of specific sequences among DNA fragments separated by gel elec-trophoresis. J Mol Biol. 1975;98:503.
102. Sutherland GR, Gedeon A, Kornman L, et al. Prenatal diagnosis of fragile X syndrome by direct detection of the unstable DNA sequence. N Engl J Med. 1720;325:1991.
103. Prior TW, Bridgeman SJ. Experience and strat-egy for the molecular testing of Duchenne muscular dystrophy. J Mol Diagn. 2005;7:317.
104. Mullis K, Faloona F, Scharf S, et al. Specific enzymatic amplification of DNA in vitro: the polymerase chain reaction. Cold Spring Harb Symp Quant Biol. 1986;51(Pt 1):263.
105. Mullis KB, Faloona FA. Specific synthesis of DNA in vitro via a polymerase-catalyzed chain reaction. Methods Enzymol. 1987;155:335.
106. Jama M, Millson A, Miller CE, et al. Triplet repeat primed PCR simplifies testing for Hun-tington disease. J Mol Diagn. 2013;15:255.
107. Treff NR, Tao X, Ferry KM, et al. Development and validation of an accurate quantitative real-time polymerase chain reaction-based assay for human blastocyst comprehensive chro-mosomal aneuploidy screening. Fertil Steril. 2012;97:819.
108. Higuchi R, Fockler C, Dollinger G, et al. Kinetic PCR analysis: real-time monitoring of DNA amplification reactions. Biotechnology (N Y). 1993;11:1026.
109. Committee on Genetics and the Society for Maternal-Fetal Medicine. Committee opinion no.682: microarrays and next-generation sequencing technology: the use of advanced genetic diagnostic tools in obstetrics and gyne-cology. Obstet Gynecol. 2016;128:e262.
110. Yang Y, Muzny DM, Reid JG, et al. Clini-cal whole-exome sequencing for the diag-nosis of mendelian disorders. N Engl J Med. 1502;369:2013.
111. Van den Veyver IB. Recent advances in pre-natal genetic screening and testing. F1000Res. 2016;5:2591.
112. SMFM Consult Series #36. Prenatal aneu-ploidy screening using cell free DNA. Am J Obstet Gynecol. 2015;711.
113. Fan HC, Blumenfeld YJ, Chitkara U, et al. Noninvasive diagnosis of fetal aneuploidy by shotgun sequencing DNA from maternal blood. Proc Natl Acad Sci USA. 2008;105:16266.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
Resnik_9103_Chapter 2_main.indd 2 3/21/2018 4:10:10 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.

N
2 Molecular Genetic Technology 38.e3
114. Chiu RW, Chan KC, Gao Y, et al. Noninvasive prenatal diagnosis of fetal chromosomal aneu-ploidy by massively parallel genomic sequenc-ing of DNA in maternal plasma. Proc Natl Acad Sci USA. 2008;105:20458.
115. Wong FC, Lo YM. Prenatal diagnosis innova-tion: genome sequencing of maternal plasma. Annu Rev Med. 2016;67:419.
116. Vermeesch JR, Voet T, Devriendt K. Prenatal and pre-implantation genetic diagnosis. Nat Rev Genet. 2016;17:643.
117. Taylor-Phillips S, Freeman K, Geppert J, et al. Accuracy of non-invasive prenatal testing using cell-free DNA for detection of down, edwards and patau syndromes: a systematic review and meta-analysis. BMJ Open. 2016;6:e010002.
118. Zimmermann B, Hill M, Gemelos G, et al. Noninvasive prenatal aneuploidy testing of chromosomes 13, 18, 21, X, and Y, using tar-geted sequencing of polymorphic loci. Prenat Diagn. 2012;32:1233.
119. Palomaki GE, Kloza EM, Lambert- Messerlian GM, et al. DNA sequencing of maternal plasma to detect down syndrome: an international clinical validation study. Genet Med. 2011;13:913.
120. Bianchi DW, Platt LD, Goldberg JD, et al. Genome-wide fetal aneuploidy detection by maternal plasma DNA sequencing. Obstet Gynecol. 2012;119:890.
121. Palomaki GE, Deciu C, Kloza EM, et al. DNA sequencing of maternal plasma reliably iden-tifies trisomy 18 and trisomy 13 as well as down syndrome: an international collabora-tive study. Genet Med. 2012;14:296.
122. Mazloom AR, Dzakula Z, Oeth P, et al. Nonin-vasive prenatal detection of sex chromosomal aneuploidies by sequencing circulating cell-free DNA from maternal plasma. Prenat Diagn. 2013;33:591.
123. Poon LC, Musci T, Song K, et al. Maternal plasma cell-free fetal and maternal DNA at 11-13 weeks’ gestation: relation to fetal and maternal characteristics and pregnancy out-comes. Fetal Diagn Ther. 2013;33:215.
124. McCullough RM, Almasri EA, Guan X, et al. Non-invasive prenatal chromosomal aneu-ploidy testing–clinical experience: 100,000 clinical samples. PLoS ONE. 2014;9:e109173.
125. Norton ME, Jacobsson B, Swamy GK, et al. Cell-free DNA analysis for noninvasive exami-nation of trisomy. N Engl J Med. 2015;1.
126. Committee opinion no. 640: cell-free DNA screening for fetal aneuploidy. Obstet Gynecol. 2015;126:e31.
127. Wapner RJ, Levy B. The impact of new genomic technologies in reproductive medicine. Discov Med. 2014;17:313.
128. Wapner RJ, Babiarz JE, Levy B, et al. Expand-ing the scope of noninvasive prenatal testing: detection of fetal microdeletion syndromes. Am J Obstet Gynecol. 2015;212:332e1.
129. Society for Maternal-Fetal Medicine, Norton ME, Biggio JR, et al. The role of ultrasound in women who undergo cell-free DNA screening. Am J Obstet Gynecol. 2017;216:B2.
130. Forman EJ, Hong KH, Ferry KM, et al. In vitro fertilization with single euploid blastocyst transfer: a randomized controlled trial. Fertil Steril. 2013;100:100.
131. Thornhill AR, deDie-Smulders CE, Geraedts JP, et al. Eshre pgd consortium ‘Best practice guidelines for clinical preimplantation genetic diagnosis (PGD) and preimplantation genetic screening (PGS)’. Hum Reprod. 2005;20:35.
132. Sermon K, Capalbo A, Cohen J, et al. The why, the how and the when of PGS 2.0: current practices and expert opinions of fertility spe-cialists, molecular biologists, and embryolo-gists. Mol Hum Reprod. 2016;22:845.
133. Mastenbroek S, Twisk M, van Echten-Arends J, et al. In vitro fertilization with preimplanta-tion genetic screening. N Engl J Med. 2007; 357:9.
134. Twisk M, Mastenbroek S, Hoek A, et al. No beneficial effect of preimplantation genetic screening in women of advanced maternal age with a high risk for embryonic aneuploidy. Hum Reprod. 2008;23:2813.
135. Vanneste E, Voet T, Melotte C, et al. What next for preimplantation genetic screening? High mitotic chromosome instability rate provides the biological basis for the low success rate. Hum Reprod. 2009;24:2679.
136. Vanneste E, Voet T, Le Caignec C, et al. Chro-mosome instability is common in human cleavage-stage embryos. Nat Med. 2009;15: 577.
137. Forman EJ, Upham KM, Cheng M, et al. Com-prehensive chromosome screening alters tradi-tional morphology-based embryo selection: a prospective study of 100 consecutive cycles of planned fresh euploid blastocyst transfer. Fertil Steril. 2013;100:718.
138. Scott RT Jr, Upham KM, Forman EJ, et al. Blastocyst biopsy with comprehensive chro-mosome screening and fresh embryo transfer significantly increases in vitro fertilization implantation and delivery rates: a randomized controlled trial. Fertil Steril. 2013;100:697.
139. Fiorentino F, Biricik A, Bono S, et al. Development and validation of a next-generation sequencing-based protocol for 24- chromosome aneuploidy screening of embryos. Fertil Steril. 2014;101:1375.
140. Chang J, Boulet SL, Jeng G, et al. Outcomes of in vitro fertilization with preimplanta-tion genetic diagnosis: an analysis of the united states assisted reproductive technol-ogy surveillance data, 2011-2012. Fertil Steril. 2016;105:394.
141. Gleicher N, Vidali A, Braverman J, et al. Accu-racy of preimplantation genetic screening (PGS) is compromised by degree of mosaicism of human embryos. Reprod Biol Endocrinol. 2016;14:54.
142. Munne S, Velilla E, Colls P, et al. Self-correc-tion of chromosomally abnormal embryos in culture and implications for stem cell produc-tion. Fertil Steril. 2005;84:1328.
143. Keymolen K, Staessen C, Verpoest W, et al. A proposal for reproductive counselling in car-riers of robertsonian translocations: 10 years of experience with preimplantation genetic diagnosis. Hum Reprod. 2009;24:2365.
144. Otani T, Roche M, Mizuike M, et al. Preim-plantation genetic diagnosis significantly improves the pregnancy outcome of translo-cation carriers with a history of recurrent mis-carriage and unsuccessful pregnancies. Reprod Biomed Online. 2006;13:869.
145. Ethics Committee of the American Society for Reproductive Medicine. Use of preimplanta-tion genetic diagnosis for serious adult onset conditions: a committee opinion. Fertil Steril. 2013;100:54.
146. Ethics Committee of the American Society for Reproductive Medicine. Transferring embryos with genetic anomalies detected in preimplan-tation testing: an ethics committee opinion. Fertil Steril. 2017;107:1130.
ISBN: 978-0-323-47910-3; PII: B978-0-323-47910-3.00002-4; Author: Resnik; 00002
Resnik_9103_Chapter 2_main.indd 3 3/21/2018 4:10:11 PM
To protect the rights of the author(s) and publisher we inform you that this PDF is an uncorrected proof for internal business use only by the author(s), editor(s), reviewer(s), Elsevier and typesetter Toppan Best-set. It is not allowed to publish this proof online or in print. This proof copy is the copyright property of the publisher and is confidential until formal publication. These proofs may contain color(colour) figures. Those figures may print black and white in the final printed book if a color(colour) print product has not been planned. The color(colour) figures will appear in color(colour) in all electronic versions of this book.