-
Sukumbis Review of Endocrine
1
Slide 1
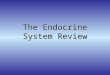
Shows 2 pictures of the same lady taken at different times. Her
complaint included new onset hypertension, diabetes mellitus &
onset of gaps.
Which of the following will you be interested in checking? Basal
level of growth hormone, blood glucose level, blood level of
insulin, blood level of insulin-like growth factor
Insulin-like growth factor that is produced by the liver. This
woman has acromegaly, do not pick growth hormone, b/c this is
released in a pulsatile manner, would not indicate properly
The MC cause of death in patients with acromegaly is which of
the following? Chronic renal failure, MI, congestive heart failure,
stroke, natural death
**congestive heart failure** The MC cause of such a change is in
which of the following? Carcinoma of the pituitary gland,
adenoma of prolactin secreting cells, adenoma of somatotrophs,
adenoma of corticotrophs Adenoma of somatotrophs, it is usually a
benign growth. Acromegaly occurs in patients who
already have fusion of the epiphysis, so bones can get fatter,
but not longer Look at the R slide, the face contour if very coarse
and the jaw is widened. You might see
some elongation of the jaw, called prognathism. Her fingers are
broad & described as sausage-shaped. Also on the inside the
woman has organomegaly enlarged organs
Prolactinoma is the MC pituitary growth. Remember that GH is an
antagonist to insulin & that it is a metabolic hormone that
affects all organ systems. This patient could possibly have
hypertension.
Sometimes the location of the tumor rises above the sella
turcica & can compress the optic chiasma affecting CN II
bitemporal hemianopsia
EXTRA
34 y/o lady with a history of infertility was accompanied to the
hospital by her husband. She has amenorrhea, lost libido, & the
husband noticed she had a lot of milk in her breasts (shes
lactating). She is not on any medication and further tests revealed
the fact that she is not pregnant.
Which of the following will be your best approach in managing
your patient? Irradiation, surgery, antibiotics, bromocriptin
Bromocriptin, this woman has prolactinoma, a tumor of the
pituitary. The MC presentation of this is described in the
question.
Note that sometimes, medication can cause this kind of
condition. Will have no ovulation, no libido, will be infertile.
Patients usually will come to the hospital
before it becomes a macroadenoma (tumor of pituitary that is
> 10mm), otherwise it is a microadenoma. You would not use
radiation for a microadenoma. Bromocriptin is like dopamine, it is
an antagonist, it will inhibit the proliferation of the glands
tissues.
-
Sukumbis Review of Endocrine
2
Slide 2
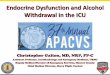
Related to slide above, another picture of acromegaly. Blood
glucose, GH, **insulin-like growth factor is elevated** Look at
slide thickened supraorbital ridge Slide 3
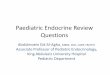
39 y/o lady shown here before & after treatment for Dx of
Cushings disease.
This implies what? She has been taking excess cortisol orally,
she has adrenal gland adenoma, she has oat cell carcinoma of the
lung that is producing ACTH, has a pituitary adenoma that is
producing ACTH
Pituitary hypothalamic problem, the other things listed as
answer choices can deal with Cushings SYNDROME, we are talking
about Cushings DISEASE.
They will also have DM xs glucose in the blood. This patient
would have osteoporosis. Would have a problem climbing stairs b/c
it affects the proximal muscles the hamstrings & quadriceps
will atrophy proximal myopathy of Cushings
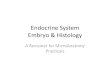
Slide 4
This is Cushings syndrome. Striae breaking down the collagen .:
the skin is
breaking down. She has weight gain, **truncal obesity**,
proximal
myopathy, features of DM, moonfaced, & you think she has
Cushings syndrome.
What is the first thing you do? Ask her about medication,
because the MC cause of Cushings is the administration of
exogenous cortisol. She could be taking steroids for asthma,
lupus, etc. If no medication 24 hour urine estimation for cortisol
& its metabolites. If it is , then there
is xs cortisol & you must do a low-dose dexamethasone
administration test. Give this woman a low-dose, after 24 hours get
a urine sample again & estimate the cortisol. If the cortisol
this woman does NOT have a pituitary adenoma b/c adenomas do not
respond to low-dose dexamethasone.
If on the other hand, you do the same thing & there is no
change in the urine cortisol urine level do a high-dose
dexamethasone if there is a change in the 24 hour cortisol urine
level, then the woman has a problem in the pituitary causing excess
cortisol.
Now what if you give both low-dose & high-doses & there
is still no change? Then may have an ectopic source or an adenoma
of the adrenal gland itself.
-
Sukumbis Review of Endocrine
3
Now measure the ACTH in the blood & see if there is an
ectopic source of this like oat cell carcinoma. Sometimes it is an
adenoma of the adrenal gland do imaging to Dx the adrenal gland
Remember that high stress will cause an extensive release of
cortisol into the body. Cushing syndrome glucose, water, & Na,
BUT prolactin is not in any type of Cushing
syndrome. *They can ask you a question just as simple as: What
cancer of the lung does this patient have?
Small cell carcinoma of the lung Upon examination of a Cushings
syndrome patient, you find hyperpigmentation of her skin
most likely to be from pituitary b/c high stimulation of
pituitary will also release MSH, causing darkened skin. Remember,
MSH is synthesized from the same precursor molecule that produces
ACTH. They sometimes use the slides from the lab video, picture of
2 hands, 1 normal and 1 pigmented.
If the source in this patient is exogenous cortisol then the
adrenal gland will atrophy, b/c its the release of ACTH that keeps
the gland level at normal
Slide 5
42 y/o man has just been diagnosed w/ HTN. His blood pressure
was 170/105 mm Hg. He was started on thiazide diuretics, and on the
3rd day he became very weak, lethargic & severely constipated.
His serum Na was normal, serum K lower than normal, serum renin
activity was on the lower side. An image study was done & shown
on the slide.
Which does he most likely have? Pheocytochroma, neofibroma,
Addisons disease, Conns syndrome, hypertension
Conns/1 hyperaldosteronism overproduction of aldosterone renin
b/c the aldosterone suppresses the RAS
HTN, losing hydrogen & K metabolic alkalosis. Must remove
the tumor for these patients. Most of the time it is an adenoma of
zona glomerulosa.
This picture can also be used with a pheochromocytoma question.
Slide 6
Gross specimen of the adrenal gland w/ a well-circumscribed mass
in the middle. Cortical part of adrenal gland.
How do you determine if it is benign or malignant? Absence of
capsule, it is always benign, presence of metastasis
Metastasis is the best predictor of malignancy Slide 7
Specimen removed from a 42 y/o lady who was diagnosed w/ HTN. In
addition, she has palpitations, occasional chest pain, &
sweating. This was removed from her abdomen.
-
Sukumbis Review of Endocrine
4
What do you expect to find in the urine of this patient?
C-peptide, glucagons, VMA, IGF VMA (Vanillomendallic acid). This is
pheochromocytoma overproduction of catecholamines
.: find catecholamines & their metabolites VMA &
metanephrines. Know the 10% rule 10% bilateral, 10% malignant
(presence of metastasis), 10% Familial, 10% Extra-adrenal. Neural
crest cells are the cell of origin for this kind of tumor.
Slide 8
Woman w/ a staring appearance. *Take note of the visible sclera
above the iris of the eyes.
What is responsible for her staring look? Accumulation of
mucopolysaccharides in the upper eyelids, in the retroorbital
space, or excess sympathetic activity
Excess of sympathetic activity keeps their eyelid in an excited
state lid lag. If you are talking about exophthalmos, then the
problem deposition of GAGs, swelling of extra-ocular muscles, LC
infiltration, & edema pushing the eyeball from the back. You
have to look from the top or side to check for exophthalmos.
If this patient has Graves, what is true about the thyroid
gland? She is likely going to have a hot spot on her radioiodine
scanning, a diffusely cold picture, one lobe hot and other lobe
cold, have a diffusely hot picture
**it will be diffusely hot** the thyroid follicles are taking up
the iodine & functioning. If one side is hot & one side is
cold, it is NOT Graves disease. If you get all cold spots, it is
NOT Graves. You will find **TSI antibodies** in this patient
stimulates the thyroid follicles to convert the colloid into
thyroxin thyrotoxicosis d/t hyperthyroidism. It will be a T2HS.
Other symptoms of hyperthyroidism tremors, sweating, flushed
warm skin, diarrhea, weight loss, excess eating & heat
intolerance
Apart from Graves, what are other causes of hyperthyroidism?
People who are trying to lose weight will take thyroxin called
factitious hyperthyroidism
Slide 9
Related to slide above. This shows pretibial myxedema, the
dermopathy
assoc w/ Graves local accum of GAGs localized thickening &
hyperpigmentation of the skin on the anterior feet & lower
legs.
Caused by stimulation of Ab. Generalized myxedema is seen in
hypothyroidism & is an accum of MPS face of this patient will
be edematous.
Slide 10
Remember that a patient who is diabetic, the MC cause of
fainting & going into coma is hypoglycemia. .: put sugar under
the patients tongue
If a patient is breathing very deeply/hyperventilating, has a
very ketoacidic smell DKA w/ Kussmaul breathing
Hyperglycemic hyperosmolarity can cause a coma
-
Sukumbis Review of Endocrine
5
MC cause of death in DM patients? MI after many years, followed
by chronic renal failure
43 y/o lady w/ DM who has not been compliant w/ her medication.
Each time she comes to the hospital her blood sugar has been in the
normal range.
What will you use to test? Fasting blood sugar, random blood
sugar, urinary glucose, glycated hemoglobin test
Glycated hemoglobin test(HbA1c) tells how much sugar flowing in
the body for the last 3 months, normal value should be
-
Sukumbis Review of Endocrine
6
glucose, C-peptide, insulin glucose, insulin secretion b/c
insulin secretion is stimulated by glucose; b/c it is exogenous
insulin, C-peptide levels b/c endogenous insulin production
**You must know that C-peptide rises w/ the bodys insulin
production for exam & Step 1**
**Know about AGEs, or advanced glycosylation end products d/t
non-enzymatic glycosylation of proteins
AGE on collagen causes cross-links between polypeptides, which
can trap plasma & other interstitial proteins can trap LDLs in
the blood vessels deposition of cholesterol accelerated
atherosclerosis that is seen in DM patients
AGE can also affect the structure of capillaries in the kidney
can develop leaky basement membranes
Slide 14
Shows the face of a middle-aged woman who has been diagnosed w/
depression & in addition she has cold intolerance, gaining
weight, constipated, sleeps most of the time, has menorrhagia and
her tongue is getting big. Her children also noticed that her voice
is becoming like a frogs sound.
No thyroxin everything concerning metabolism will be slower.
Mucopolysaccharides are accumulating in their vocal cords leading
to a croak voice.
What test do you do first? TSH if TSH, problem is w/ thyroid
gland 1 hypothyroidism.
Next, estimate the amount of thyroxin in the blood, T3 & T4
should be .
What tells you she might have Hashimotos? Anti-microsomal Ab
would be found, destroys the follicles no production of
thyroxin.
29 y/o lady has just recovered from a viral URT infection when
she developed pain & tenderness of her thyroid gland. In
addition, she had sweatiness, palpitations. A Bx from the neck
reveals granulomas, WBC count & ESR.
What is your Dx? Postpartum thyroiditis, Hashimotos, Graves, de
Quervain thyroiditis de Quervain thyroiditis subacute or
granulomatous thyroiditis **this is often associated
with a URT infection, maybe be viral** If a story is given about
a woman who has just given birth to a baby, then think of
postpartum
thyroiditis something happens with the thyroid gland & that
can lead to hypothyroidism lymphocytic infiltration &
hyperplastic germinal centers w/in thyroid parenchyma.
Slide 15
Bx specimen from the neck of a 57 y/o lady who had a goiter
affecting her thyroid gland. Histology showed normal looking
follicles with no stromal invasion & no pleomorphism.
-
Sukumbis Review of Endocrine
7
Follicular adenoma, it is a well circumscribed finding.
Papillary carcinoma is the MC of the thyroid gland. It shows
Psammoma bodies. Papillary
carcinoma also has the best prognosis, spreads through local LN,
not through the blood stream.
Follicular carcinoma spreads through the blood & can spread
to the lungs & other organs. The prognosis is poor & have
stromal invasion.
Medullary carcinoma affects C-cells which produce calcitonin.
Can use calcitonin to monitor this type of cancer. C-cells are from
neural crest cells.
Anaplastic cancer carries the worst prognosis. It metastasizes
very early, in elderly. Patients who has been exposed to excessive
radiation or genetic mutations are at risk for
these kinds of cancers. Plummer syndrome develop cancer from one
of the nodules in a multinodular goiter
combo of hyperparathyroidism & goiter, NO exophthalmos Slide
16
Related to above slides. Shows the thyroid gland & tumor on
one side.