Embed Size (px)
Citation preview
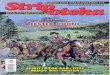
C-endo (a division of C-health)Suite 240, 1016 - 68 Avenue SW
Calgary, AB T2V 4J2PH: (403) 705-3636 FAX: (403) 705-2636
www.c-health.ca
C-ENDO-ACENTREOFEXCELLENCECOMMITTEDTOCOMPREHENSIVEDIABETESANDENDOCRINOLOGYCARE
DateofReferral:PATIENTINFORMATION(orattachpatientlabel)PatientName:ULI#:Phone:Address:
PostalCode:Gender: Male Female
City,Prov.:
DateofBirth:
RelevantHistory:
ReferringPhysicianSignature:
Fax:ReferringPhysician:Ph:PracticeID:AdditionalReportto:Fax:
PleaseNote:Wewill faxtheappointmentdateandtimetoyouroffice and notify the patient by phoneor letter. The patient may require labs to becompleted prior to this appointment and a labrequisition will also be sent to the patient. Werequire 48-hour notice for cancellation orreschedulingofappointment.
Fortriageofreferralspleasecheckoneofthefollowing:
DIABETESMANAGEMENT
ENDOCRINOLOGISTGENERALINTERNISTNOPREFERENCE,SHORTESTWAITTIME
GENERALENDOCRINOLOGY
THYROIDDISORDER FEMALEREPRODUCTIVEMALEREPRODUCTIVEOSTEOPOROSISCALCIUM/PARATHYROIDBARIATRICMATTERSPITUITARY/ADRENALOTHER
URGENT FIRSTAVAILABLE ROUTINE
Note:Pleaseensurepatientdemographicsarecurrent.