Embed Size (px)
Citation preview

86 (2006) 221–225www.elsevier.com/locate/schres
Schizophrenia Research
Suicidality in first episode psychosis
Mary Clarke a,⁎, Peter Whitty a, Stephen Browne a, Orfhlaith Mc Tigue a,Anthony Kinsella a,e, John L. Waddington d, Conall Larkin a, Eadbhard O'Callaghan a,b,c
a Stanley Research Unit, Department of Adult Psychiatry, Hospitaller Order of St John of God, Cluain Mhuire Service, Blackrock, Dublin, Irelandb Department of Psychiatry, University College Dublin, Ireland
c DELTA/DETECT Early Intervention Service, 1 Marine Tec., Dunlaoghaire, Co. Dublin, Irelandd Stanley Research Unit, Department of Clinical Pharmacology, Royal College of Surgeons in Ireland, Dublin, Ireland
e Department of Mathematics, Dublin Institute of Technology, Dublin 8, Ireland
Received 16 February 2006; received in revised form 23 May 2006; accepted 27 May 2006Available online 17 July 2006
Abstract
Many studies have confirmed that the risk of suicide is high in the period after first presentation. There is relatively littleinformation about the risk of suicide using illness onset as the starting point. We assessed suicidality in a cohort of 166 individualsfrom an urban catchment area during the period of untreated psychosis and at 4 year follow up. Nearly 10% of individualsattempted suicide prior to presentation. Four years later 18% had made a suicide attempt and 3% completed suicide. Suicideattempts prior to presentation were associated with a longer duration of untreated psychosis.© 2006 Elsevier B.V. All rights reserved.
Keywords: Psychosis; suicide; duration of untreated psychosis
1. Introduction
Much of the research on suicidality in psychosis hasfocused on schizophrenia and fewer studies havesystematically examined suicidal behaviour across abroad spectrum of patients with psychotic disorders(Radomsky et al., 1999). Studies involving mainlyindividuals with schizophrenia, have shown that the riskfor suicide is influenced by the stage of the illness. Riskis consistently highest during the early phases of the
⁎ Corresponding author. St John of God Hospital, Stillorgan, CoDublin, Ireland. Tel.: +353 1 2771400; fax: +353 12881034.
E-mail address: [email protected] (M. Clarke).
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.05.026
illness, with two thirds of suicides occurring during thefirst 5 years after diagnosis (Harris and Barraclough,1997; Copas and Robin, 1982). In examining the earlystages of the illness, most studies have focused onsuicidal behaviour from the time of presentation ratherthan the actual onset of illness. In this first episodepsychosis study we explore whether variables associatedwith suicidal behaviour are influenced by stage ofillness. We examine risk factors for suicidality at twoseparate time periods; during the period of untreatedpsychosis and after first presentation over a 4 yearfollow up. Furthermore, given the interest in earlyintervention in psychosis, we specifically ask whethersuicidal behaviour is associated with duration ofuntreated psychosis (DUP).

Table 1Baseline characteristics of the sample
Number (%)
Gender (male) 99 (58)Marital status (single) 146 (85)DiagnosisSchizophrenia or schizophreniform disorder 101 (59)Bipolar disorder with manic symptoms 11 (6.4)Depressive disorder, 25 (14.6)Substance induced psychosis 12 (7.0)Delusional disorder 13 (7.6)Psychosis NOS 4 (2.3)Organic psychosis. 5 (2.9)DSM-IV substance use 71 (41.5)History of alcohol abuse/ dependence 39 (23.5)History of drug abuse/ dependence 61 (36.8)Current alcohol use/dependence 38 (22.9)Current drug use or dependence 31 (18.7)Mean age at presentation 28.5 years (SD 11.1)Mean age at onset of psychosis 27.3 years (SD 10.9)Mean duration of untreated psychosis 17.8 months (SD 31.7)
222 M. Clarke et al. / Schizophrenia Research 86 (2006) 221–225
2. Methods
The study was approved by the institutional reviewboard and all patients gave verbal informed consent. Thesample consisted of 171 persons from an urbancatchment area of 165,000 who participated in the StJohn of God and Cluain Mhuire Family Centre firstepisode psychosis study (Browne et al., 2000). Atinception we measured symptomatology using thePositive and Negative Syndrome Scale (PANSS) (Kayet al., 1987) and global functioning using the GlobalAssessment of Functioning scale (GAF) (Spizter et al.,1995). We used the Structured Clinical Interview forDSM (SCID) to ascertain DSM-IV Axis I diagnoses(American Psychiatric Association, 1994). During thecourse of these interviews we asked patients aboutmood, suicidal thoughts and acts. We evaluated theemergence of different phases of a psychotic illnessduring a family interview using the Beiser Scale (Beiseret al., 1993), which contains specific checklists for bothsuicidal ideation and suicidal acts during the period ofuntreated psychosis. Drawing from the concept of apossible continuum of suicidal ideation and behaviour(Beck et al., 1974; Murphy et al., 1992), we categorizedpatients into three levels of suicidality: suicide attempts(SA) (acts of purposeful self harm with expressedsuicidal intent), suicidal ideation (SI), and not suicidal(NS). DUP was defined as the interval between firstnoted psychotic symptom(s) and presentation to thepsychiatric services for initiation of adequate treatmentof a psychotic illness, with first manic symptom(s) usedfor bipolar disorder. This figure was based onindependent parental/relative and patient interviews; ininstances where there was discrepancy between thesetwo figures, or where there was no information availablefrom a relative, we assigned a consensus duration usingall available sources of information.
Four years later a researcher who was blind to DUPand original symptom scores contacted all individuals inthe inception sample and invited them to come for afollow up interview where symptomatology, (PANSS)and global functioning (GAF) were reassessed andsuicidal behaviour was documented over the 4 yearssince presentation. Individuals were tracked usingoriginal contact information and information from theclinical teams however tracing methods did not extendto obtaining national death records.
2.1. Inter-rater reliabilities
We assessed inter-rater reliabilities for the PANSS bythe consecutive examination of ten patients with chronic
schizophrenia. We rated ten family interviews to assessinter-rater reliabilities the family's dating of the onset ofprominent psychotic symptoms. Intraclass CorrelationCoefficients (ICC's) were 0.73 for the negative syndromesubscale and in excess of 0.84 for the remaining subscalesand the total score for the PANSS. ICCs were 0.94 for thedating of the onset of prominent psychotic symptoms.
2.2. Statistics
We performed statistical analyses using the StatisticalPackage for the Social Sciences. In view of the skewednature of the DUP data we log transformed it, beforecomparing DUPs between the three suicidal groupsusing an analysis of variance procedure. We identifieddemographic (male gender, younger age, years in edu-cation, (Caldwell and Gottesman, 1990, Drake et al.,1985, Sletten et al., 1972)) and clinical variables(positive symptoms, negative symptoms, insight andsubstance misuse (McGirr et al., 2006; Schwartz andSmith, 2004; Verdoux et al., 1999)) in addition to DUP(Altamura et al., 2003) that have previously beenassociated with suicidal behaviour. We used a stepwiselogistic regression model with a stepwise forced entryprocedure to examine the clinical and demographicpredictors of suicide attempts at presentation and overthe 4 year follow up period.
3. Results
This sample consisted of 171 individuals. A minority(n=27, 15.8%) was treated as an outpatient. Table 1

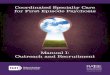
Fig. 1. Box plot of DUP by suicidality level at presentation.
223M. Clarke et al. / Schizophrenia Research 86 (2006) 221–225
shows the baseline characteristics of the sample. Weexcluded those with a diagnosis of organic psychosisthus reducing the N to 166. The mean DUP was17.8 months, (SD=31.7, median=5, interquartile range(IQR)=1,24). Sixteen patients (9.6%) made a suicideattempt during the period of untreated psychosis. Thirtysix (21.7%) individuals reported suicidal ideation priorto presentation and 114 (68.6%) had no history ofsuicidal ideation or intent. There were significantdifferences in DUP between the 3 suicidal groups. Thedownward trend in the mean DUP (log transformed) ofthe 3 suicidal groups (SA mean=1.1, SI mean=0.9, NSmean=0.5) was highly significant (p=0.004), Fig. 1.
We then tested the effect of DUP in predicting suicideattempts in a logistic regression model that included thefollowing variables, gender, DUP, age at onset ofpsychosis, years in education, lifetime history of alcoholabuse, lifetime history of substance misuse, diagnosis(subdivided into schizophrenia or not), positive symp-toms at presentation, negative symptoms at presentationand insight scores (measured on the PANSS). Theresults of the logistic regression model (Model ChiSquare=6.9, df=1, p=0.009) indicated that the onlysignificant predictor of suicide attempts was a longerDUP, (B=−0.98, S.E.=0.40, p=0.01, Exp B=0.4).Diagnosis was not associated with suicidality. This wasconfirmed when we repeated this analysis confining thesample to schizophrenia (n=101) and found that theresults did not remain significant (Residual ChiSquare=8.9, df=8, p=0.35).
One hundred and thirty-two of 166 patients (79.5%)consented to a second direct interview and assessment 4
years after presentation, while 30 (18.1%) refusedfollow-up assessment or were untraceable. Twenty-eight individuals attempted suicide over the 4 yearfollow up period of whom four completed suicide. Thisrepresents a 4 year prevalence of 3.0% when the sampleis restricted to those we followed up and is 2.4% of theoriginal sample. Of the remaining twenty four (18.2%)who attempted suicide, four (16.7%) had a previoushistory of suicide attempts and five (20.8%) a history ofsuicidal ideation. We tested the effects of the followingvariables in predicting suicide attempts over the 4 yearfollow up in a logistic regression model — previoussuicide attempts, gender, age at onset of psychosis, yearsin education, DUP, diagnosis, positive symptoms,negative symptoms, insight and global functioning (allmeasured at presentation). The model (Model ChiSquare=7.6, df=1, p=0.006) indicated that the onlysignificant predictor of suicide attempts at follow up wasa younger at onset of psychosis (B=0.08, S.E.= 0.03,p=0.01, Exp B=1.1). When we repeated this analysisconfining the sample to schizophrenia only, we foundthat the results did not remain significant (Residual ChiSquare=12.8, df=10, p=0.24).
4. Discussion
Our data demonstrate that almost one in tenindividuals attempted suicide during the period ofuntreated psychosis (Addington et al., 2004). Evenhigher rates have been reported in other studies(Johnstone et al., 1986; Cohen et al., 1994; Verdoux etal., 1999; Nordentoft et al., 2002). However our sampleincluded both in and outpatients; this may haveproduced a group with a broader range of illness.
This association between DUP and suicide attemptshas not been consistent in other studies. Altamura et al.(2003) demonstrated a significant association betweenDUPs greater than 1 year and suicide attempts in asample with chronic schizophrenia or schizoaffectivedisorder, whereas Nordentoft et al. (2002) found noassociation between DUP and suicide attempts in theirfirst episode sample. We found a significant relationshipbetween DUP and suicide attempts prior to presentation,with DUP increasing with each level of suicidality.From our data we cannot establish whether this effect isa reflection of added opportunity time or whether it is aresult of being exposed to a prolonged period ofpsychosis. Against the latter explanation is the factthat a longer DUP did not predict suicidal behaviourduring follow up. An alternative explanation is thatindividuals with a long DUP have a more malignantform of illness that is more likely to be associated with

224 M. Clarke et al. / Schizophrenia Research 86 (2006) 221–225
suicidal behaviour. However if this were the case onewould expect that DUP would also predict suicideattempts over the follow up period and in this study thiswas not the case. Another possibility is DUP may be aproxy factor for another variable that is associated withboth the DUP and the suicidal behaviour.
We can only speculate as to why the variablesassociated with suicidal behaviour were not constantbetween both time points in the study. One possibility isthat risk factors for suicidal behaviour may beinfluenced by the stage of the illness. With this inmind, it is noteworthy that there was a relatively smalloverlap between individuals who attempted suicide atboth time points in the study. This finding is consistentwith the study of Addington et al. (2004) who found nooverlap between those who attempted suicide before andafter entry to an early psychosis programme. Thisfinding highlights the practical difficulties faced byclinicians in identifying those at risk of suicidalbehaviour.
We found a 4 year prevalence of completed suicide ofonly 3%. It is possible that this is an underestimate giventhe loss to follow up, though our sample attrition wasrelatively modest. Two other first episode 1 year followup studies, both based in specialist treatment settingshave reported an even lower prevalence of completedsuicide, 0.4% and 0.3%, respectively (Addington et al.,2004; Nordentoft et al., 2002).
We wish to acknowledge a number of potentiallimitations to the study. Examination of suicidalbehaviour was not an ‘a priori’ aim of the study, andtherefore the possibility exists that the figures reportedhere may underestimate the frequency of suicideattempts in a first episode sample. However, we triedto minimize this possibility by collecting data usingmultiple sources of information. We have no informa-tion on patients who may have been referred to, andtreated in a general hospital following a suicide attempt.However in our clinical experience such patients areusually subsequently referred for specialist psychiatricevaluation. The strengths of the study include the factthat the sample was drawn from a defined catchmentarea, and consisted of consecutive presentations of inand outpatients to a ‘real life’ clinical services andtherefore is likely to be representative.
Many centres worldwide have developed earlyintervention programmes that educate the public andmental health professional about the warning signs andsymptoms of psychosis and offer early treatment (Melleet al., 2004). They are expensive to resource and therehas been much controversy over whether they have thepotential to improve outcome of the illness (Marshall et
al., 2005). But if they are shown to reduce suicidalbehaviour (Melle et al., 2006) then surely its money wellspent.
Acknowledgments
This study was supported by the Stanley Foundation.
References
Addington, J., Williams, J., Young, J., Addington, D., 2004. Suicidalbehaviour in early psychosis. Acta Psychiatr. Scand. 109 (2),116–120.
Altamura, A.C., Bassetti, R., Bignotti, S., Pioli, R., Mundo, E.,2003. Clinical variables related to suicide attempts in schizo-phrenic patients: a retrospective study. Schizophr. Res. 60 (1),47–55.
American Psychiatric Association, 1994. Diagnostic and StatisticalManual of Mental Disorders (4th edn) (DSM-IV). APA,Washington, DC.
Beck, A.T., Resnick, H.L.P., Lettieri, D.J. (Eds.), 1974. The Predictionof Suicide. In Charles Press, Bowie, MD.
Beiser, M., Erickson, D., Fleming, J., Iacono, W.G., 1993. Establishingthe onset of psychotic illness. Am. J. Psychiatry 159, 1349–1354.
Browne, S., Clarke, M., Gervin, M., Waddington, J.L., Larkin, C.,O'Callaghan, E., 2000. Determinants of quality of life at firstpresentation with schizophrenia. Br. J. Psychiatry 176, 173–176.
Caldwell, C.B., Gottesman I.I., 1990. Schizophrenics kill themselvestoo: a review of risk factors for suicide. Schizophr. Bull. 16,571–589.
Cohen, S., Lavelle, J., Rich, C.L., Bromet, E., 1994. Rates andcorrelates of suicide attempts in first-admission psychotic patients.Acta Psychiatr. Scand. 90, 167–171.
Copas, J.B., Robin, A., 1982. Suicide in psychiatric inpatients. Br. J.Psychiatry 141, 511–530.
Drake, R.E., Gates, C., Whitaker, A., Cotton, P.G., 1985. Suicideamong schizophrenics: a review. Compr. Psychiatry 26 (1),90–100.
Harris, E.C., Barraclough, B., 1997. Suicide as an outcome for mentaldisorders. A meta analysis. Br. J. Psychiatry 170, 205–228.
Johnstone, E.C., Crow, T.J., Johnson, A.L, MacMillan, J.F., 1986. TheNorthwick study of first episodes of schizophrenia: I. Presentationof the illness and problems relating to admission. Br. J. Psychiatry148, 115–120.
Kay, S., Fiszbein, A., Opler, L., 1987. The Positive and NegativeSyndrome Scale (PANSS) for schizophrenia. Schizophr. Bull. 13,261–276.
Marshall, M., Lewis, S., Lockwood, A., Drake, R., Jones, P.,Croudace, T., 2005. Association between duration of untreatedpsychosis and outcome in cohorts of first episode patients. Asystematic review. Arch. Gen. Psychiatry 62, 975–983.
McGirr, A., Tousignant, M., Routhier, D., Pouliot, L., Chawky, N.,Margolese, H.C., Turecki, G., 2006. Risk factors for completedsuicide in schizophrenia and other chronic psychotic disorders: acase-control study. Schizophr. Res. 84 (1), 132–143.
Melle, I., Larsen, T.K., Haahr, U., Friis, S., Johannessen, J.O.,Opjordsmoen, S., Simonsen, E., Rund, B.R., Vaglum, P.,McGlashan, T., 2004. Reducing the duration of untreated first-episode psychosis: effects on clinical presentation. Arch. Gen.Psychiatry 61 (2), 143–150.

225M. Clarke et al. / Schizophrenia Research 86 (2006) 221–225
Melle, I., Johannesen, J.O., Friis, S., Haahr, U., Joa, I., Larsen, T.K.,Opjordsmoen, S., Rund, B.R., Simonsen, E., Vaglum, P.,McGlashan, T., 2006. Early detection of the first episode ofschizophrenia and suicidal behavior. Am. J. Psychiatry 163 (5),800–804.
Murphy, G.E., Wetzel, R.D., Robins, E., McEvoy, L., 1992. Multiplerisk factors predict suicide in alcoholism. Arch. Gen. Psychiatry49, 459–463.
Nordentoft, M., Jeppesen, P., Abel, M., Kassow, P., Petersen, L.,Thorup, A., Krarup, G., Hemmingsen, R., Jorgensen, P., 2002.OPUS study: suicidal behaviour, suicidal ideation and hope-lessness among patients with first-episode psychosis. One-yearfollow-up of a randomised controlled trial. Br. J. Psychiatry 43,98–106 (Suppl.).
Radomsky, E.D., Haas, G.L., Mann, J.J., Sweeney, J.A., 1999.Suicidal behavior in patients with schizophrenia and otherpsychotic disorders. Am. J. Psychiatry 156, 1590–1595.
Schwartz, R.C., Smith, S.D., 2004. Suicidality and psychosis: thepredictive potential of symptomatology and insight into illness.J. Psychiatr. Res. 38 (2), 185–191.
Sletten, I., Brown, M., Evenson, R., 1972. Suicide in mental hospitalpatients. Dis. Nerv. Syst. 33, 328–334.
Spizter, R.L., Williams, J.B., Gibbon, J., 1995. Structured ClinicalInterview for DSM-IV — Patient Version (SCID-P). New YorkState Psychiatric Institute, New York.
Verdoux, H., Liraud, F., Gonzales, B., Assens, F., Abalan, F., van Os,J., 1999. Suicidality and substance misuse in first-admittedsubjects with psychotic disorder. Acta Psychiatr. Scand. 100 (5),389–395.