Embed Size (px)
Citation preview
Sue-Jane Wang, Ph.D.
Associate Director Adaptive Design and Pharmacogenomics
Office of Biostatistics, Office of Translational SciencesCenter for Drug Evaluation and Research, U.S. FDA
Presented at “Graybill Conference VII”, Fort Collin, Colorado, June 12, 2008
Adaptive Designs that Prospectively Learn vs. Test Biomarker Sensitive Patients

Wang SJ, Graybill 06.12.2008 2
AcknowledgmentsH.M. James Hung
Robert T. O’Neill
Thanks are due to Dr. Robert Temple and Dr. Norman Stockbridge of FDA for bringing the interesting problem to our attention
The research work was supported by the RSR funds #02-06, #04-06, #05-2, #05-14, #08-48 awarded by the Center for Drug Evaluation and Research, U.S. Food and Drug Administration
*The research view presented are those of the author’s professional views and not necessarily those of the US FDA

Wang SJ, Graybill 06.12.2008 3
Outline (Genomic) Biomarker as a Classifier
AD in Preliminary Biomarker Exploratory Studies
AD in A&WC Setting
Examples
Mechanics of Sample Size Formula
Concluding Remarks

Wang SJ, Graybill 06.12.2008 4
Biomarker
• A characteristic recognized as an indicator• Regulatory impact
– Single Biomarker– Composite Biomarker

Wang SJ, Graybill 06.12.2008 5
A Genomic Composite Biomarker* (genomic classifier)
• Consists of a set of gene expressions or SNPs• Defined by a prediction algorithm • Used to classify patients as likely responsive
patients (efficacy or safety)
GCB = 1 if patient’s risk score beyond threshold
= 0 otherwise
* Wang SJ (2007, Pharmaceutical Statistics)

Wang SJ, Graybill 06.12.2008 6
Genomic Composite Biomarker
Developed from
Microarray,
Whole Genome Scan,
Other Technology Platforms

Wang SJ, Graybill 06.12.2008 7
Tumor Staging Might not Predict Cancer Risk Level

Wang SJ, Graybill 06.12.2008 8
GCB - Added Value to Clinical ?%
res
po
nd
ers
50%
70%
overall
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Placebo
Experimental Treatment
GCB, like baseline clinical covariate, might be associated with placebo alone, drug treatment alone, or interacting with disease & therapy simultaneously
Typical Prognostic Factor
Wang SJ, Graybill 06.12.2008 9
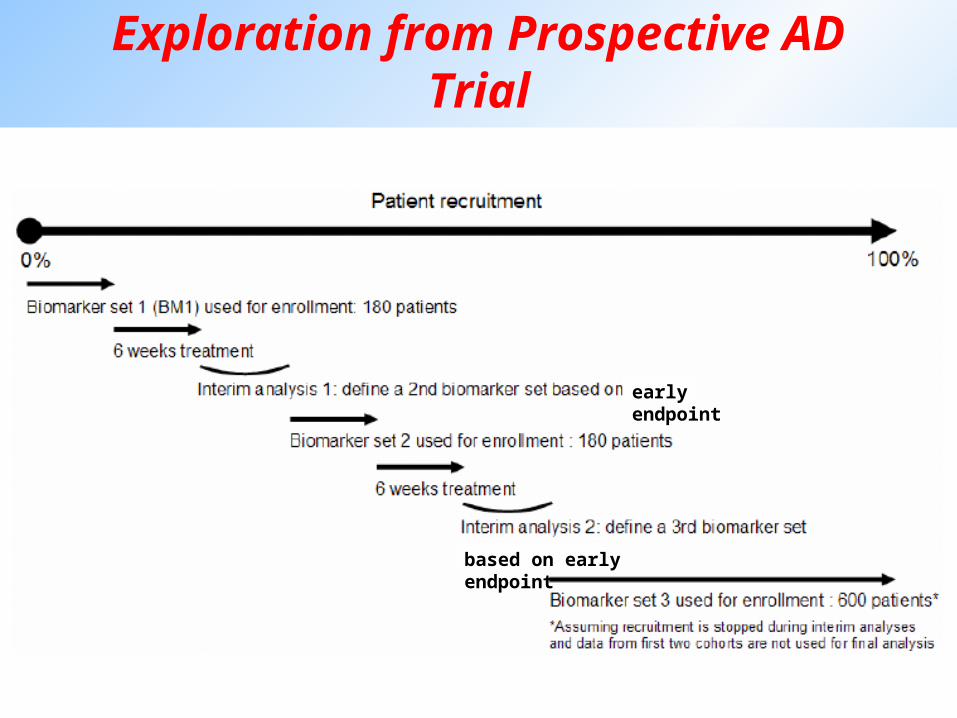
Exploration from Prospective AD Trial
early endpoint
based on early endpoint

Wang SJ, Graybill 06.12.2008 10
ACR: A Clinical Response
Prospective Learning of Patient Population

Wang SJ, Graybill 06.12.2008 11
ex: Baseline DAS4 (Fransen, 2005) (range 0-10)
DAS4 = 0.53938*(Ritchie) + 0.06465*(swollen joints) + 0.330* ln (ESR) + 0.00722* (General Health)
Ritchie: Ritchie articular index Swollen joints: 44 swollen joint count
ESR: erythrocyte sedimentation rateGH: 100 mm VAS
DAS ≤ 2.4 (LDA) DAS28 ≤ 3.2 2.4 < DAS ≤ 3.7 (MDA) DAS28 > 3.2 DAS > 3.7 (HDA)

Wang SJ, Graybill 06.12.2008 12
Adaptive Designs in Adequate and Well-Controlled Setting
When a (composite) genomic biomarker is developed (not a preliminary biomarker panel that is continually refined), preliminary utility of biomarker as a classifier needs analytic validation and feasibility study
To prospectively assess the biomarker’s clinical utility, adaptive design in adequate and well-controlled setting may be considered

Wang SJ, Graybill 06.12.2008 13
Prognostic Biomarker
* Wang SJ (2007, Pharmaceutical Statistics)

Wang SJ, Graybill 06.12.2008 14
Predictive Biomarker
* Wang SJ (2007, Pharmaceutical Statistics)

Wang SJ, Graybill 06.12.2008 15
Prognostic-Predictive Biomarker
* Wang SJ (2007, Pharmaceutical Statistics)

Wang SJ, Graybill 06.12.2008 16
A Study Adequate to Support Effectiveness Claims Should
Reflect a Clear Prior HypothesisDocumented In The Protocol
*FDA Guidance on “providing clinical evidence of effectiveness for human drug and biological products” for Industry, 1998
Prospective Testing of Biomarker Sensitive Patient Subset
Wang SJ, Graybill 06.12.2008 17
Strategy #1 (e.g., Freidlin, Simon 2005)(1) Learn potential GCB+ responsive patients in stage 1(2) Test T-effect in all comers from both stages at 0.02 level, allow test for GCB+ subset at 0.005 level using only stage 2 GCB+ patients, if all comers failed
Strategy #2 (e.g., Wang, O’Neill, Hung, 2007)(1) GCB+ is defined and not learned from current trial(2) stage 1, assess if T futile or toxic in GCB- for accrual decision(3) Test T-effect in all comers and in GCB+ subset from both stages using, e.g., p-value combination, adaptive Hochberg with strong control at 0.05 level
Prospective Testing of Biomarker Sensitive Patient Subset
Wang SJ, Graybill 06.12.2008 18
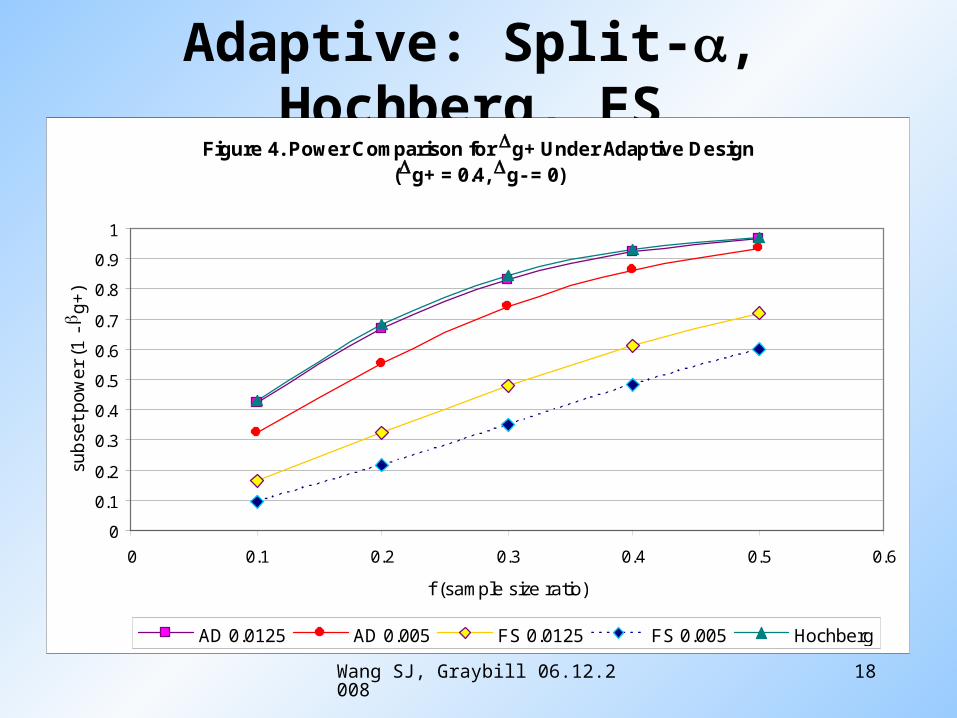
Adaptive: Split-, Hochberg, FS
Figure 4. Power Comparison for Dg+ Under Adaptive Design(Dg+ = 0.4, Dg- = 0)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6
f (sample size ratio)
sub
set
po
we
r (1
- b
g+
)
AD 0.0125 AD 0.005 FS 0.0125 FS 0.005 Hochberg

Wang SJ, Graybill 06.12.2008 19
Is RF a GCB classifier for treatment?
Primary Endpoint PBO Treatment p-value
Ph2 n RF+ only
4038%
4073% < 0.005
Ph3 n RF+ (74%) RF– (26%) ITT
13128%53%31%
17654%47%51%
< 0.0001 (1O)ns<0.001
Ph3 n RF+ (79%) RF– (21%) ITT
20119%12%18%
29854%41%51% < 0.0001

Wang SJ, Graybill 06.12.2008 20
Nested Subsets: Two Markers
Consider 2 indicators:
Subgroups formed: G0, G1, G2
G0: all patients randomized (ITT)
G1: patients w/ biomarker present
G2: patients w/ biomarkers present in
Prevalence: f1 | G0, f2 | G1
Prevalence relative to originally intended patient population
f0=1, f1’=f1 for G1, f2’ = f1*f2 for G2
*0D*1D*2D
GB GB-1 … G2 G1 G0 (ITT)
21, II
21 II 1I

Wang SJ, Graybill 06.12.2008 21
Rationale of Sensitive Patient Adaptation
At time t, based on interim data,
N or Nmax
Upper bound for CP & lower bound if futility or N
Compute or Remaining
(1-t)N or (1-t)N+(Nmax-N) recruits only the selected jth patient subset
Pre-specified weighting in weighted z-statistic
Let selection rule denoted by Bttott ZZZfD ,,1, BDt ,,2,1,0
jtjt
Gj ZZjCP ,| D jtjGj ZZjCP ,| D

Wang SJ, Graybill 06.12.2008 22
Empirical Power Comparison – Some Pattern
Figure 2c. Empirical Powers Among 8 Strategies (Some Pattern) (f =.5, .5)
00.1
0.20.3
0.4
0.50.6
0.7
0.8
0.91
g0 g1 g2
Prospectively Specified Patient (Sub)sets
Ind
ivid
ual P
ow
ers
R A B C D E F G
D2=.300D1=.125D
0=.113
T=0.495
**
*
* *
*

Wang SJ, Graybill 06.12.2008 23
Mechanics of Sample Size Formula Sample size planning based on , , , b
n/arm n formula – does not distinguish types of
patients
PainFree approved for (i) back pain, (ii) Nerve Pain
Adaptive Design – In/Exclusion ITT Patients
EOS I EOS II
Chronic Pain Interim Enrichment
Non-nested subset: Back pain or Nerve PainNested subset: Back pain & Nerve Pain
iid (n1) iid (n2)Br-CA CHF
Randomization stratify on Back pain, Nerve Pain

Wang SJ, Graybill 06.12.2008 24
Concluding Remarks
Replication of the finding needed
Improvement from conventional null, sample size caveats
Exploratory biomarker development - flexible AD design
Two-stage adaptive design in A&WC setting provides flexibility for assessing sensitive patients prospectively and effectively
For A&WC trials, recommend stratified randomization based on biomarker status to avoid bias
Biomarker status for ITT patients should be available

Wang SJ, Graybill 06.12.2008 25
Cui, Hung, Wang. (1999, Biometrics)
Wang, Chen. (2004, Journal of Computational Biology)
Wang. (2005, Flexible Design Genomic Drug Trial, NCI-FDA Biomarker Wksp)
Wang. (2005, Special report in 1st Multi-track DIA WKSP, Japan)
Tsai, Wang, Chen, Chen. (2005, Bioinformatics)
Simon, Wang (2006, The Pharmacogenomics Journal (TPJ))
Trepicchio, Essayan, Hall, Schechter, Tezak, Wang, et al. (2006, TPJ)
Wang, Cohen, Katz, et al. (2006, TPJ)
Chen, Wang, Tsai, Lin (2006, TPJ)
Microarray Quality Control Project: (2006, Nature Biotechnology)
Wang. (2007, Taiwan Clinical Trials)
Wang, O’Neill, Hung. (2007, Pharmaceutical Statistics)
Wang. (2007, Pharmaceutical Statistics): Biomarker as a classifier in pharmacugenomics clinical trials: a tribute to 30th anniversary of PSI (Statistician in the Pharmaceutical Industry)
Wang et al. (2008, invited Biometrical J. in progress)
Some References