Embed Size (px)
Citation preview

1
Successfully Using Six Sigma
(6σ) to Improve Nursing Quality
Indictors
Joann Hatton, RN MS, 6σ Black Belt
Director of Nursing Professional Practice
Heritage Valley Health System
Beaver, PA
Objectives
1. Describe how Six Sigma can be used to
improve nursing quality indicators.
2. Describe how the DMAIC process
identified the critical steps surrounding
the incidence or pressure ulcers.

2
About Heritage Valley Health System
• The Medical Center, Beaver, with 358 beds
• Sewickley Valley Hospital, with 191 beds
• Five affiliated physician groups: Tri-State Medical
Group, Sewickley Valley Medical Group, Tri-State
Obstetrics and Gynecology, Tri-State Gynecology,
Tri-State Pediatric Associates
• Sewickley Valley Hospital and The Medical Center
foundations
•• Quality Method: Six SigmaQuality Method: Six Sigma
Recommended by the JCAHO
““Best PracticeBest Practice””
for Six Sigma for Six Sigma
ImplementationImplementation
(April 2005)(April 2005)
The Medical Center was recently named as one of
the nation's 2005 Performance Improvement
Leaders by Solucient® 100 Top Hospitals
What is Six Sigma?
• A method to analyze VariationVariation
• Has a strong metric component; it is Data DrivenData Driven
• A process to reduce variation so that acceptable
performance is within Six Standard Deviations (6 σ)

3
Reducing variability is the essence of six sigma
Six Sigma Concept
Every Human Activity Has Variability...
MeanMean
1σσσσ1σσσσ
TargetTarget
Errors
UpperCustomer
Specification
LowerCustomer
Specification
Six Sigma Concept
A process to reduce defects per million
opportunities (DPMO)
σσσσσσσσ DPMODPMO
2
3
4
5
6
308,537
66,807
6,210
233
3.4
Quantitative methodology, utilizing measurements and
scientific process
Defect
pressure ulcer, patient fall,
antibiotic delay, central line
infection, med omitted

4
DMAIC: A Problem Solving Methodology
DefineDefine MeasureMeasure AnalyzeAnalyze ImproveImprove ControlControl
Project Selection
Team Formation
Define
Opportunities
Project Selection
Team Formation
Define
Opportunities
Measure the ProcessMeasure the Process
Analyze Data
Collected
Analyze Data
Collected
Innovate
Solutions
Make
Improvements
Innovate
Solutions
Make
Improvements
“Sustain
The
Gain”
““SustainSustain
The The
GainGain””
We are forced, after improvement, to remeasure,
analyze and then control the process
Six Sigma: A Set of ToolsSix Sigma: A Set of Tools
Process Flow DiagramProcess Flow Diagram
RISK PRIORITY NUMBER (RPN) =
SEVERITY X 0CCURRENCEX ESCAPED DETECTION
5 4 3 2 1
Severe High Moderate Minor Negligible
Occurrence Very High High Moderate Low Very Low
(OCC)
Severity
(SEV)
Escaped Very High High Moderate Low Very Low
Detection
(DET)
Category
Score
Failure Modes and Effects Analysis - FMEAFailure Modes and Effects Analysis - FMEA
Control ChartsControl Charts
Item
Operator 1 Operator 3
Test 1 Test 2 Test 1
Operator 2
Test 1 Test 2 Test 2
1
2
3
4
5
6
7
8
9
1
0
Glass Inspection Test
Measurement System Analysis
Measurement System Analysis
Cause and Effect DiagramCause and Effect Diagram
Procedures
GOAL
EquipmentMeasurement
Environments
People
Material

5
Six Sigma Project:
Preventing Hospital Acquired Pressure Ulcers
Why Reduce Hospital Acquired Pressure Ulcers?
1. Nursing Quality Indicator (NDNQI)- Magnet Status- Regulatory Agencies - DOH
2. Health Care Cost- Increase Health Care Cost - Increase LOS- Increase Use of Resources/Materials- Potential For Litigation
3. Increased Mortality - Due to complications (Sepsis)
4. Patient Satisfaction 5. Perception that the rate of hospital acquired pressure ulcer was higher than expected.
define
Our Profile of a Patient with
“Decubitus Ulcer”
A review of 226 cases from July 2005 to Jan 2006 with ICD-9
Principle or Secondary diagnosis of 707 (decubitus ulcer)
showed:
– Mean age 71 with a range of 17-92
– 56% female and 44% male
– Top 5 diagnosis codes:
• heart failure, hypertension, urinary track infection, atrial fibrillation and COPD.
– Top 2 DRGs: heart failure and septicemia
– Discharging nursing unit:
• A1 (46%), B3 (32%) and A3 (9%)
– 49% Medicare and 25% Security Blue
– LOS average 7.6 days +/- 6.3 days
– Discharge Status: SNF 40%, Home 23%, HH 18%
• Expired n = 16 (7%)
define

6
Skin Care Committee Team Members
• Nursing Administration
– Joann Hatton RN Director of Nursing
– Kathy Hoffman RN CWOCN Nurse
– Gail Inman RN CWOCN Nurse
• Critical Care
– Cheryl Decker RN
• CardioPulmonary Step Down
– Kathy Starkey RN Level 3
• Medical Surgical Units
– Kristen Majetic RN A3 Med Surg
– Lisa McLean RN Level 2 Med Surg
– Kristen Coster RN Level 1 Med Surg
– Ting Andrews LPN Level 1 Med Surg
• Psychiatric Unit
– Pat Martyak RN
define
IPO
Preventing
Hospital
Acquired
Pressure
Ulcers
•People
•Patients
•Families
•Nurses
•Clinical Techs
•CWOCN Nurse
•Physicians
•Policies / Procedures
•Risk Assessment
•Nutrition Screen
•Documentation Tool
•Event Reporting
•Training /Education
•Skill/knowledge
•Competency
•Equipment / Supplies
•Bed Surfaces
•Pressure Relief Devices
•Dressings
•Wound care products
•Quality
•Reduced Incidence pressure
ulcers
•Practicing evidenced based
nursing (ie risk assessment)
•Competent and
knowledgeable staff
•Customer Satisfaction
•Improved patient/family
satisfaction
•Improved physician
satisfaction
•Improved relationships
•HR
•Improved nursing satisfaction
•Positive impact on nursing
retention
•Financial
•Reduced patient costs
•Reduced LOS
Inputs Outputs
define

7
PROCESS
FLOW
Skin / Risk Assessment Process FlowPatient Admitted to
Hospital
At Risk?
Skin Assessment Completed
by RN (Admission
Assessment)
Skin
Breakdown
Present?
Stage 1
Stage 2
Stage 3
Stage 4
Unstageable
Event Report
Risk Assessment Completed
by RN (Braden Scale)
High Risk < 12
Low to Moderate Risk
12-18
Not Currently at Risk
>18
Risk Assessment Completed
by RN (Braden Scale)
Follow Skin Care
Protocol according to
Risk and Stage
yes
no
Implement Prevention Strategies and
reassess Braden Scale daily.
Implement Prevention Strategies and if
other major risk factors are present,
advance to next level of risk
Implement Prevention Strategies and
consult CWOCN
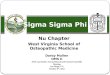
TMC: All Units
measure
Data Source: NDNQIData Source: NDNQI
Percent of Surveyed Patients w ith Hospital Aquired Pressure Ulcers
The Medical Center
25.00
6.12
8.86
13.33
8.30
4.10
6.10
25.00
4.16 4.34
8.67
15.80
2.17
0 0 0 0
3.00
7.10
10.10
0 0
8.3
0
4.804.8
2.51.38
0 0 0
1.38
0
5
10
15
20
25
30
Critical Care CardioPulmonary Level 1 Level 2 A3 Psych TMC
4Q04 1Q05 2Q05 3Q05 4Q05
Target < 11.29 Target < 7.42 Target < 5.39 Target < 8.03

8
Hillrom Study March 2005
= TMCAnalysis: TMC rates below Benchmarks
measure
TMC DataTMC Data
What Have We Learned?
MANPOWERMANPOWER
� Staff Education
– Lack of knowledge on protocol/policy
– Lack of knowledge on products
– Competency (has not been one for past 4
years)
– Policy / Protocol not up to date
analyze / improve
1. Revised Skin Care Protocol Aug 2005 to
reflect evidence based practice. Included
easy to follow tables on equipment and
products. Completed
2. Provided Staff Education In Progress
� On line learning module for RNs on
Risk Assessment
� Incorporated Assessment / Staging
into Annual Nursing Seminar.
� Skills lab for CTs (turning,
positioning, reducing shearing and
friction)
1. Revised Skin Care Protocol Aug 2005 to
reflect evidence based practice. Included
easy to follow tables on equipment and
products. Completed
2. Provided Staff Education In Progress
� On line learning module for RNs on
Risk Assessment
� Incorporated Assessment / Staging
into Annual Nursing Seminar.
� Skills lab for CTs (turning,
positioning, reducing shearing and
friction)
Analysis: Failure ModesAnalysis: Failure Modes Improvement StepsImprovement Steps

9
What Have We Learned?
MANPOWER
� Role of CWOCN nurse not clear
– Hospital culture (expect ET to do it)
– Inappropriate consults
– CWOCN workload
analyze /improve
Further study and define role of CWOCN
Completed
1. July 2005 Kathy Hoffman CWOCN
reassigned full time at TMC with Gail Inman
providing support coverage.
2. In addition to seeing patients, focus on
customer service and coaching / mentoring of
RNs, CTs and students
3. Monthly tracking of caseloads – looking at
workload and types of consults.
4. Focus on improved event reporting / FU
5. Job Description revised
6. Participation in Western PA WOCN Assoc.
Further study and define role of CWOCN
Completed
1. July 2005 Kathy Hoffman CWOCN
reassigned full time at TMC with Gail Inman
providing support coverage.
2. In addition to seeing patients, focus on
customer service and coaching / mentoring of
RNs, CTs and students
3. Monthly tracking of caseloads – looking at
workload and types of consults.
4. Focus on improved event reporting / FU
5. Job Description revised
6. Participation in Western PA WOCN Assoc.
Analysis: Failure ModesAnalysis: Failure Modes Improvement StepsImprovement Steps
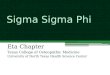
Role of CWOCN
32%
30%
11%
11%
12%4%
Pressure Ulcers
Ostomies
Leg Ulcers
Wounds
Derm
Other (burns, fistulas,
tubes,drains)
CWOCN Monthly Visits
189
219219
161
222
202
0
50
100
150
200
250
Ju
ly
Se
pte
mb
er
Oc
tob
er
No
ve
mb
er
De
ce
mb
er
Ja
nu
ary
Average 202 visits per monthCWOCN Visits per Day
10.410.1
9.69.5
11.0
7.7
9.2
6
7
8
9
10
11
12
July
Septe
mber
Octo
ber
Novem
ber
Decem
ber
January
Fy06
Average visits per day
Visits by Reason for Consult
Volume of Visits

10
What Have We Learned?
MANPOWER
� Skin Care Committee
– Only meets quarterly
– Ill defined - unclear focus other than
audits
– focus not on PI
– No management involvement /
accountability
– Not all units represented
– Managers not really aware of what they
did
analyze /improve
Resurrect Skin Care Committee with
newly defined charter. Completed1. Decided quarterly was sufficient in
2006
2. All units now represented
3. NDNQI results shared with members
4. Each meeting focus on a PI topic and
education
5. Competency completed on all members
Aug 2005
6. DON Professional Practice attends
mtgs
7. Summary of meeting and findings
communicated via email to nursing
leadership within 24 hours of mtg.
Resurrect Skin Care Committee with
newly defined charter. Completed1. Decided quarterly was sufficient in
2006
2. All units now represented
3. NDNQI results shared with members
4. Each meeting focus on a PI topic and
education
5. Competency completed on all members
Aug 2005
6. DON Professional Practice attends
mtgs
7. Summary of meeting and findings
communicated via email to nursing
leadership within 24 hours of mtg.
Analysis: Failure ModesAnalysis: Failure Modes Improvement StepsImprovement Steps
What Have We Learned?
MEASUREMENTMEASUREMENT
• Question validity of data
– Audit process not clearly defined
– Not using current NDNQI forms and data
definitions
• Only completed quarterly
– No real time feedback to Mgrs
• “feel” rates are higher than reported in
prevalence studies
analyze /improve
Revised Measurement / Auditing Process Aug
2005 Completed
1. Using current NDNQI forms
2. DON PP and CWOCN completed NDNQI
online tutorial
3. Review data collection methodology with skin
care committee prior to each quarterly audit.
4. Attended conference call by NDNQI on
improving reliability and validity of data.
5. Review audits at mid day and at end of day to
ensure accuracy and completeness
6. Nursing assumed responsibility for data entry
into NDNQI web based system.
7. Manager’s review and initial audit tool at the
end of the day.
8. CWOCN weekly tracks incidence of pressure
ulcers.
Revised Measurement / Auditing Process Aug
2005 Completed
1. Using current NDNQI forms
2. DON PP and CWOCN completed NDNQI
online tutorial
3. Review data collection methodology with skin
care committee prior to each quarterly audit.
4. Attended conference call by NDNQI on
improving reliability and validity of data.
5. Review audits at mid day and at end of day to
ensure accuracy and completeness
6. Nursing assumed responsibility for data entry
into NDNQI web based system.
7. Manager’s review and initial audit tool at the
end of the day.
8. CWOCN weekly tracks incidence of pressure
ulcers.
Analysis: Failure ModesAnalysis: Failure Modes Improvement StepsImprovement Steps

11
What Have We Learned?
MACHINESMACHINES
� Bed Utilization - high rental fees
– over and under utilization
– monitoring bed usage (what reports are
out there?)
– mattresses and beds are old
analyze /improve
Plan for replacing all beds in 5 year
capital plan In Progress1. All Critical Care beds replaced Nov 05
2. Preventive surface included in all beds
3. Stopped using mattress overlays
Plan for replacing all beds in 5 year
capital plan In Progress1. All Critical Care beds replaced Nov 05
2. Preventive surface included in all beds
3. Stopped using mattress overlays
MATERIALS
� Lack of knowledge on
- which products available at TMC
- when to use which product
- where products are kept
MATERIALSMATERIALS
� Lack of knowledge on
- which products available at TMC
- when to use which product
- where products are kept
Included one page tables on equipment
and products as an attachment in the
Skin Care Protocol. In Progress
1. CWOCN focus on 1:1 coaching /
mentoring at the bedside.
2. CWOCN participates in value analysis
process / committee.
Included one page tables on equipment
and products as an attachment in the
Skin Care Protocol. In Progress
1. CWOCN focus on 1:1 coaching /
mentoring at the bedside.
2. CWOCN participates in value analysis
process / committee.
Analysis: Failure ModesAnalysis: Failure Modes Improvement StepsImprovement Steps
What Have We Learned?
1. Policy on Admission Assessment
revised
− Moved Braden Scale with
Integumentary section of the form
− defined areas of responsibilities
2. Skin Care Protocol revised to
specifically define the process for
documentation, risk assessment and
event reporting.
− Changed from on admission to daily
− Added risk tools to daily graphics
3. Focus on event reporting of pressure
ulcers noted on admission by Mgrs,
supervisors and CWOCN.
4. Educational sessions for nursing to
focus on Risk Assessment and
documentation.
Completed
METHODSMETHODS
� Documentation
– New admission assessment form:
• Small print, limited education on use
• Unclear who completes what section of form
– Patient not “captured” on admission
• Event Report not always completed
• Patients not “captured” ICDM coding on discharge
� Risk Assessment
– Skin Assessment not consistently completed on admission
– Braden Scale not done or not done correctly on admission
• Practice varies on some units from 0-100%!
• Mean is around 45-50%
– No reassessment of Braden during hospital stay
– Protocol not initiated when risk present
analyze /improve

12
Documentation
• Document the patient’s initial Braden Scale on the Admission Assessment as usual
• Record the daily reassessment on the Clinical Record
Documentation
Document pressure ulcer prevention measures on the Clinical Record and update plan of care.
Can I delegate the
documentation of
the frequent
observations to my
ClinTech?
YES, you are
encouraged to do
this!

13
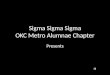
ResultsThe project results so far have been
impressive:
1. Reduction in hospital acquired
pressure ulcers from 6.9 to 3.5 (Sigma
level from 2.9 to 3.5)
2. Incorporation of risk assessment from
“on admission” to daily with an
improvement in documentation of risk
assessment from 50% to 96%.
control
Hospital Acquired Pressure Ulcers
The Medical Center
UCL=18.281
LCL=-4.296
CEN=6.993UCL=9.806
LCL=-2.728
CEN=3.539
-10
-5
0
5
10
15
20
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 161Q03 2Q03 3Q03 4Q03 1Q04 2Q04 3Q04 4Q04 1Q05 2Q05 3Q05 4Q05 1Q06 2Q06 3Q06 4Q06
Sigma level 2.9 (69,444 DPM) Sigma level 3.5 (23,148 DPM)
Results Hospital comparison to NDNQI

14
Results: Critical Care
Summary
• Skin care remains an important measure of quality for nursing
• Incidence of pressure ulcers remains a significant problem in most hospitals. Using a six sigma problem solving approach within nursing can identify and eliminate barriers nurses face in caring for their patients.
• The FMEA assisted us in developing processes to prevent and mitigate those instances that escaped the initial process.


























![Six Sigma (6 Sigma)[1]](https://img.pdfslide.us/doc/110x75/577d35cc1a28ab3a6b91711a/six-sigma-6-sigma1.jpg)