Embed Size (px)
Citation preview

Case Report
DepartmenWatford, Hertf
CorrespondHospital, VicaKingdom; E-m
Ann Vasc Surghttp://dx.doi.or� 2014 Elsevi
Manuscript rec
2014; publishe
Successful Thrombolysis of a Late AcuteThrombotic Occlusion of an Aortic Prosthesisafter Endovascular Aneurysm Repair
James Waiting, Abigail Dias, Tulsi Patel, Tim Pencavel, Kevin Rosenfeld, and Sanjeev Sarin,
Watford, United Kingdom
A 79-year-old man with a previous endovascular aneurysm repair (EVAR) for a 5.4-cm abdom-inal aortic aneurysm presented 3 years after the procedure with sudden onset lower limb paral-ysis and pain. The diagnosis of acute aortic thrombosis within the aortic prosthesis graft wasmade and confirmed on computed tomography. Thrombolysis delivered into the graft via a radio-logically placed catheter successfully dissolved the thrombus and resulted in improvement of thepatient’s symptoms. We discuss the presentation of, and role in management of thrombolysis in,this rare complication of aneurysm repair.
Endovascular repair of aortic aneurysms is a well-
recognized and commonly used surgical technique,
with the incidence of endovascular aneurysm repair
(EVAR) techniques increasing in recent years as
both technique and technology evolve. We present
a case of complete occlusion of an EVAR graft and
its treatment and resolution with thrombolysis.
As far as we are aware, this is the only reported
case of successful thrombolysis to an acutely throm-
bosed aortic segment of an EVAR graft.
CASE REPORT
A 79-year-old man presented with a 1-day history of sud-
den onset of bilateral lower limb paralysis and pain, with
absent pulses femoral pulses. Three years previously, he
had undergone an EVAR for a 5.4-cm aneurysm. An oc-
clusion of the right limb of the EVAR was diagnosed 9
t of Vascular Surgery, Watford General Hospital,ordshire, UK.
ence to: James Waiting, MBBS, iBSc, Watford Generalrage Road, Watford, Hertfordshire, WD18 0HB, Unitedail: [email protected]
2014; -: 1–4g/10.1016/j.avsg.2014.02.027er Inc. All rights reserved.
eived: April 28, 2013; manuscript accepted: February 24,
d online: ---.
months after the EVAR and resultant limb ischemia
treated by a femorofemoral crossover graft with an 8-
mm diameter Dacron graft.
He was initially investigated by way of computed to-
mography (CT) angiography of the abdominal aorta
and arterial duplex scanning, which excluded spinal pa-
thology as a cause of his symptoms and revealed an
occluded EVAR graft at a level just below the renal ar-
teries (Fig. 1).
In view of the acute nature of the presentation and
limited alternative surgical reconstructive options, we
elected to attempt intraarterial thrombolysis. Under radio-
logic guidance, a catheter was inserted into the proximal
end of the occluded graft via a percutaneous left femoral
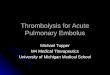
approach. Angiography confirmed complete graft occlu-
sion (Fig. 2). The patient was transferred to the high de-
pendency unit for monitoring and thrombolysis with
recombinant tissue plasminogen activating factor (r-
TPA) delivered through the catheter at a dose of 1 mg/hr
for 20 hr, before a repeat catheter angiography to check
success. After 16 hr thrombolysis, the feet were warmer
and pedal pulses easily palpable on the left with no evi-
dence of ‘‘trash’’ embolization. An angiogram performed
20 hr after thrombolysis was initiated confirmed the clin-
ical findings, in that the EVAR graft, left lower and left
external iliac arteries were patent. There was persistent
thrombus in the right side of the femorofemoral bypass
graft. The catheter was withdrawn into the left iliac artery
and the dose of r-TPA reduced to 0.5 mg/hr for a further
24 hr. A check angiogram following this revealed
1

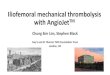
Fig. 1. Coronal section of CT angiogram, showing
thrombus within the stent graft, starting just distal to
the renal arteries.
Fig. 2. Angiogram showing thrombosis of aortic pros-
thesis graft. (Catheter used to deliver local thrombolysis).
2 Case Report Annals of Vascular Surgery
complete lysis of the acute thrombus. The chronically
occluded right limb of the EVAR graft remained occluded.
The angiogram suggested fibrointimal hyperplasia of the
femorofemoral graft, which may have been the precipi-
tating factor in the acute occlusion (Fig. 3A). There was
no iliac stenosis within either the native vessel or EVAR
graft to account for the occlusion.
After thrombolysis, the patient’s paralysis and pain
resolved. He was treated with low-molecular-weight hep-
arin and commenced on life-long oral anticoagulation
withwarfarin, with a target international normalized ratio
(INR) of 2.5e3.5. The patient was treated on the high de-
pendency unit for 8 days and then stepped down to a sur-
gical ward from where he was discharged 4 days later
when his INR was within the target range. At routine
follow-up, the patient has made an excellent recovery
with no signs of recurrent occlusion (Fig. 3B). Elective
angioplasty to the crossover graft, with bridging heparin
therapy, has been considered but may be unnecessary as
he has had no further symptoms on oral anticoagulation.
Currently, at 1 year since the acute event, there is no sign
of reocclusion either clinically or on CT scanning.We plan
for the patient to undergo ultrasound surveillance once in
3 months, with Doppler flow analysis, for the next year
and once in 6 months for a further 3 years, at which stage
if he remains asymptomatic, he will be considered for
discharge.
DISCUSSION
EVAR is a commonly used surgical intervention for
aneurysm repair. It has advantages over open
repair of aneurysms as it is minimally invasive
and leads to shorter hospital stays, decreased blood
loss, and decreased early mortality rates.1,2 Howev-
er, EVAR is associated with a greater complication
and reintervention rate, which necessitates long-
term monitoring of the patient.3 Complications
include graft migration, endoleak, limb occlusion,
limb kinking, and continued expansion of the
aneurysm.4,5
Limb occlusion is a common complication of
EVAR. It is highly dependent on the type of graft
used, occurring in up to 40%of unsupported grafts.4
Modern grafts, however, would be expected to have
limb occlusion rates of around 5e10%.6e8 Various
risk factors have been postulated, including deploy-
ment within the external iliac artery (rather than
common iliac), younger age patients, and kinking
of grafts.6,9 In the postoperative period, the presence
of raised peak systolic velocities on Doppler ultra-
sound is also predictive of occlusion.10,11 Intraoper-
ative intravascular ultrasound has been shown to be
a feasiblemethod of assessing EVAR, but as yet there

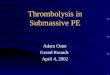
Fig. 3. (A) Catheter angiography showing resolution of
thrombus at 48 hours with fibrointimal hyperplasia in
femorofemoral crossover graft, which may have been
the precipitating factor for graft thrombosis. (B) Coronal
section of CT angiogram at 3 months showing persistent
flow through aorta and femorofemoral crossover graft.
Vol. -, No. -, - 2014 Case Report 3
is limited evidence on its use in preventing limb
occlusion.12
Occluded limbs of EVAR grafts may be treated
surgically with a femorofemoral crossover graft to
treat the occlusion and restore flow or through an
endovascular approach such as balloon catheteriza-
tion, thrombolysis, and/or stent placement.13e15
Success rates for thrombolysis in the literature are
in the region of 50%, although in the setting of
acute limb ischemia, it has been noted that patients
treated initially with thrombolysis require less
traumatic secondary intervention.16e18 The distal
embolus rate after thrombolysis for acute ischemia
is reported as being in the region of 10%, with an
increase in stroke and hemorrhage risk. More
recently, a technique has been described using
catheter thrombectomy in conjunction with a voll-
mar ring stripper.19 However, experience with all
these techniques is sufficiently limited as to make
generalizable conclusions impossible. Reconstruc-
tive options include extra-anatomical bypass or
aortofemoral bypass grafting; in the current case,
we felt that the acute presentation, coupled with
the patient’s comorbid state, made at least a trial
of thrombolysis an attractive therapeutic option.
Informed written consent, including a discussion
of risks, was obtained before commencement of
therapy, and the patient was keen to avoid further
invasive surgery. However, thrombolysis may not
be appropriate in cases where the thrombosis is
detected later, when the thrombus has organized
and would not be amenable to thrombolysis, or if
there was acute limb-threatening ischemia, in
which situation rapid restoration of circulation by
definitive surgical means would reduce the risk of
limb loss.
The occurrence of complete occlusion of the
EVAR graft is rare. As a consequence, it is not as
well described in the literature as limb occlusion,
which is often included as a secondary outcome in
studies of novel EVAR devices7,8 and its presenta-
tion and management are described only in case re-
ports with treatment by combined surgical and
endovascular techniques.2,13
In the case of our patient, limb occlusion had
occurred as an early complication (within 9 months
of surgery) and was initially treated successfully
with a femorofemoral crossover graft. Complete
occlusion of the graft due to thrombus formation
subsequently occurred as a late complication
approximately 3 years after the initial endovascular
repair. The likely mechanism of this was turbulent
flow within the femorofemoral crossover graft
because of fibrointimal hyperplasia, with subse-
quent proximal propagation of the thrombus. The
postthrombolysis angiography showed typical ap-
pearances of fibrointimal hyperplasia (Fig. 2).
The acute occlusion was treated with thromboly-
sis. This is a recognized treatment for EVAR graft
limb thrombosis and acute limb or peripheral graft
occlusion but has not been reported in the treatment
of a completely thrombosed endograft. Thromboly-
sis is not without complications and carries inherent
risks of bleeding (minor, locally, and intracranial),
distal embolization of thrombotic material, and
anaphylaxis.20 In the present case, we concluded
that the risk of these side effects was likely to be
lower than the morbidity associated with emer-
gency axillobifemoral reconstruction, but this deci-
sion was reached after lengthy discussion between
the patient, admitting surgical team, and specialist
radiologists. Of note, the acute thrombus resolved

4 Case Report Annals of Vascular Surgery
with thrombolysis, but the treatment had no effect
on the established occlusion of the right limb of
the graft. We conclude that thrombolysis has a role
in the treatment of acute endograft occlusion, but
it is of lower utility if the patient presents late once
the thrombus has organized.
Anticoagulant therapy with warfarin has been
shown to bemore effective than aspirin alone at pre-
venting graft occlusion.21 The patient was consid-
ered to be high risk for further graft occlusion and
therefore initiated on warfarin. This will be
continued lifelong.
Thrombus formation in the body of an endograft
is a rare complication of EVAR. It may occur second-
ary to thrombus formation in a distal graft in the
presence of a predisposing factor such as fibrointi-
mal hyperplasia. Thrombolysis has a role in the
treatment of acute occlusion of endografts; howev-
er, the potential risks must be considered. With
the rarity of the presentation, it is unlikely to be
possible to conduct a randomized control trial study-
ing the effect of thrombolysis in this condition, and
thrombolysis should be considered on a case-by-
case basis.
REFERENCES
1. Greenhalgh RM, Brown LC, Kwong GP, et al. Comparison of
endovascular aneurysm repair with open repair in patients
with abdominal aortic aneurysm (EVAR trial 1), 30-day
operative mortality results: randomised controlled trial. Lan-
cet 2004;364:843e8.
2. Thurley PD, Glasby MJ, Pollock JG, et al. Endovascular man-
agement of delayed complete graft thrombosis after endo-
vascular aneurysm repair. Cardiovasc Intervent Radiol
2010;33:840e3.
3. EVAR Trial Participants. Endovascular aneurysm repair
versus open repair in patients with abdominal aortic aneu-
rysm (EVAR trial 1): randomised controlled trial. Lancet
2005;365:2179e86.
4. Maleux G, Koolen M, Heye S. Complications after endovas-
cular aneurysm repair. Semin Intervent Radiol 2009;26:
3e9.
5. Subramanian K, Woodburn KR, Travis SJ, et al. Secondary
interventions following endovascular repair of abdominal
aortic aneurysm. Diagn Interv Radiol 2006;12:99e104.
6. Cochennec F, Becquemin JP, Desgranges P, et al. Limb graft
occlusion following EVAR: clinical pattern, outcomes and
predictive factors of occurrence. Eur J Vasc Endovasc Surg
2007;34:59e65.
7. Mertens J, Houthoofd S, Daenens K, et al. Long-term re-
sults after endovascular abdominal aortic aneurysm repair
using the Cook Zenith endograft. J Vasc Surg 2011;54:
48e57.e2.
8. van Zeggeren L, Bastos Goncalves F, van Herwaarden JA,
et al. Incidence and treatment results of Endurant
endograft occlusion. J Vasc Surg 2013;57:1246e54. dis-
cussion 54.
9. Conway AM, Modarai B, Taylor PR, et al. Stent-graft limb
deployment in the external iliac artery increases the risk of
limb occlusion following endovascular AAA repair. J Endo-
vasc Ther 2012;19:79e85.
10. Blom AS, Troutman D, Beeman B, et al. Duplex ultrasound
imaging to detect limb stenosis or kinking of endovascular
device. J Vasc Surg 2012;55:1577e80.
11. Karthikesalingam A, Kumar S, Anandarajah JJ, et al. Predic-
tive value of peak systolic velocity for the development of
graft limb complications after endovascular aneurysm
repair. J Endovasc Ther 2012;19:428e33.
12. Eriksson MO, Wanhainen A, Nyman R. Intravascular ultra-
sound with a vector phased-array probe (AcuNav) is feasible
in endovascular abdominal aortic aneurysm repair. Acta
Radiol 2009;50:870e5.
13. Erzurum VZ, Sampram ES, Sarac TP, et al. Initial manage-
ment and outcome of aortic endograft limb occlusion.
J Vasc Surg 2004;40:419e23.
14. Moll FL, Powell JT, Fraedrich G, et al. Management of
abdominal aortic aneurysms: clinical practice guidelines of
the European society for vascular surgery. Eur J Vasc Endo-
vasc Surg 2011;41(Suppl 1):S1e58.
15. Polat A, Mert B, Gumus F, et al. Rare complication of EVAR:
thrombus in endograft. Eur J Vasc Endovasc Surg Extra
2011;22:e15e7.
16. Becquemin JP, Kelley L, Zubilewicz T, et al. Outcomes of
secondary interventions after abdominal aortic aneurysm
endovascular repair. J Vasc Surg 2004;39:298e305.
17. Byrne RM, Taha AG, Avgerinos E, et al. Contemporary out-
comes of endovascular interventions for acute limb
ischemia. J Vasc Surg 2014;59:988e95.18. Berridge DC, Kessel DO, Robertson I. Surgery versus throm-
bolysis for initial management of acute limb ischaemia.
Cochrane Database Syst Rev 2013;(6):CD002784.
19. Ronsivalle S, Faresin F, Franz F, et al. A new management
for limb graft occlusion after endovascular aneurysm repair
adding a vollmar ring stripper: the unclogging technique.
Ann Vasc Surg 2013;27:1216e22.20. Working Party on Thrombolysis in the Management of Limb
Ischaemia. Thrombolysis in the management of lower limb
peripheral arterial occlusionda consensus document.
J Vasc Interv Radiol 2003;14(9 Pt 2):S337e49.
21. Tangelder MJ, Lawson JA, Algra A, et al. Systematic review
of randomized controlled trials of aspirin and oral anticoag-
ulants in the prevention of graft occlusion and ischemic
events after infrainguinal bypass surgery. J Vasc Surg
1999;30:701e9.