Embed Size (px)
Citation preview

Successful revascularization of
isolated SMA dissection
Department of Cardiovascular Medicine, Graduate School of Medicine, Kyoto University
Junichi Tazaki, Takeshi Kimura

Case Fifty-five y.o male was admitted to our hospital due to acute abdominal pain nausea and vomit with acute onset. CT revealed dissection at ostium of superior mesenteric artery (SMA), and true lumen was compressed by false lumen.
Risk factor: Hypertension, Current smoker ECG: Sinus rhythm ABG: pH7.414 pO2 71 pCO2 38 K 3.5 BE -0.8

SMA
SMA
Entry point
Hematoma at False lumen
CT at onset

SMA
Entry was closed with thrombus.
Blood flow of true lumen was improved.
Day 1 CT

Entry point
False lumen
True lumen
Abdominal pain relapsed many times . Therefore we performed endovascular therapy.
Day 4, Severe abdominal pain relapsed. The patient could not tolerate complete bed rest
because he is medical doctor.

EVT to SMA Lt brachial approach Guiding sheath : 6.5Fr sheathless PV angle 90cm
SMA

EVT to SMA
Entry point
Lt brachial approach Guiding sheath : 6.5Fr sheathless PV angle 90cm
Non-touch technique
0.014 Agosal (Rinato) wire
0.035 wire

Lt brachial approach Guiding sheath : 6.5Fr sheathless PV angle 90cm
Entry point
False lumen
True lumen
EVT to SMA
Entry point
False lumen
True lumen

After first wire pass

IVUS after first wire cross
False lumen was blind end

After 1st stent
Misago 8-40mm

Final Angiogram
Misago 6-80mm

5 Month after EVT

Discussion
Spontaneous isolated dissection of the superior mesentric artery(SIDSMA) mainly occurs in fifth decade male.
Sakamoto I,etal. Imaging appearances and management of isolated spontaneous dissection of the superior
mesenteric artery. Eur J Radiol. 2007;64:103–110
I. Sakamoto et al. / European Journal of Radiology 64 (2007) 103–110 105
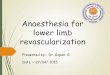
Fig. 1. Drawings illustrate imaging classification of spontaneous dissection of the superior mesenteric artery. Type I: patent false lumen with both entry and re-entry;
type II: ‘cul-de-sac’ shaped false lumen without re-entry; type III: thrombosed false lumen with ulcer like projection (ULP), which is defined as a localized blood-filled
pouch protruding from the true lumen into the thrombosed false lumen; type IV: completely thrombosed false lumen without ULP.
In all of them, the false lumen of the SMA remained unchanged
in size during the follow-up period of 12–48 months (Fig. 2).
One patient with type II dissection underwent urgent surgery
because of occlusion of the true lumen, attributing to small
bowel ischemia (Fig. 3). In this case, catheter angiography
demonstrated not only occlusion of the SMA, but also severe
stenosis of the celiac trunk due to compression by the median
arcuate ligament. His postoperative course was uneventful dur-
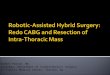
Fig. 2. 49-year man with type I dissection of the superior mesenteric artery (SMA). (A) Coronal MPR images at the onset clearly depict an intimal flap in the SMA
and compression of the true lumen by the dilated false lumen, together with the entry (arrow) and re-entry sites (open arrow). (B) SMA arteriograms demonstrate the
dilated false lumen and the entry (arrow) located a few centimeters from the vessel origin. The re-entry site (open arrow) is also revealed. The patient was followed
up conservatively, and the false lumen remained unchanged during the follow-up period of 36 months. F: false lumen.
Initial and middle-term results of treatment for symptomatic spontaneous isolated dissection of superior
mesenteric artery Eur J Vasc Endovasc Surg 2013. 45. 502-508
Sakamoto classification

Discussion
patients with severe symptoms should be considered EVT with self expanding stent
Min, et. Al Current strategy for the treatment of symptomatic spontaneous isolated dissection of superior mesenteric artery JVascSurg2011; 54:461-6.

Summary
We report the successful revascularization of intestinal ischemia due to isolated SMA dissection supported by CT and IVUS.

Thank you for your attention!