Embed Size (px)
Citation preview

INTRODUCTION
Lower extremity superficial thrombophlebitis is a common vascularcondition. While in the majority of cases the condition under-goes a benign self-limiting course usually associated with thepresence of varicose veins, the condition can reflect primaryhypercoagulable states where an increased risk of thrombosis iscaused by a measurable defect in proteins of coagulation andfibrinolytic systems. This condition is also associated with less wellunderstood secondary hypercoagulable states associated withmalignancy and pregnancy. A rare but definite risk of fatal pulmonary embolization exists from involvement of the thromboticprocess at the sapheno–femoral junction and from the high inci-dence of concurrent deep venous thrombosis.
We present a series of case reports reflecting the spectrumof hypercoagulable conditions associated with this disease. Wereport cases of superficial thrombophlebitis as manifestations ofunsuspected underlying malignancy, antiphospholipid syndrome andinherited protein S deficiency. Duplex imaging of the venoussystem for diagnostic purposes and in particular in assessing theextension of thrombus into the femoral vein is emphasized in thecases reported. Minimal handling and mobilization of thesapheno–femoral junction at the time of sapheno– femoral dis-connection when the thrombus extends into the superficial andcommon femoral veins eliminates the risk of embolization ofthrombus existing in the sapheno–femoral system.
CASE REPORTS
Case 1: Superficial thrombophlebitis as aparaneoplastic phenomena
A 60-year-old previously well male patient presented to hisgeneral practitioner with bilateral acute ascending thrombo-phlebitis involving both long saphenous veins from the ankle to theknee. There were no underlying varicose veins. The patient was otherwise well. He was commenced on oral antibiotics andnon-steroidal anti-inflammatory drugs. On review after 1 week, thepatient had made no improvement and the thrombophlebitis in bothlegs had progressed in a cephalad manner with the saphenousvein in the thigh being involved close to the sapheno–femoraljunction. A duplex scan of the lower limb venous system was performed. This showed floating thrombus within the
sapheno–femoral junction with non-occlusive extension of clotinto the common femoral vein on the left side. On the right side thethrombus was shown to be limited to the long saphenous veinterminating 12 cm distal to the right sapheno–femoral junction.There was no evidence of deep vein thrombosis in either lowerlimb. Routine coagulation profile was performed on the patientincluding prothrombin time (PT), partial thromboplastin time(PTT) and D-Dimer assay. These were within normal limits. On thebasis of the duplex study, the patient was therapeutically antico-agulated with intravenous heparin. Bilateral sapheno–femoraldisconnections were then performed under general anaesthesia.At operation, a tongue of thrombus was noted extending fromthe left long saphenous vein into the left common femoral vein. Thiswas extruded in continuity just proximal to the sapheno–femoraljunction. The patient made an uneventful recovery from the pro-cedure. Heparin was ceased postoperatively and the patient was notcommenced on oral anticoagulants.
In the absence of underlying varicose veins and an obviousprimary coagulopathy, an underlying malignancy was suspectedand the patient was investigated for this. A computed tomogram(CT) of the abdomen revealed a lesion in the left lobe of theliver consistent with a malignant growth. Computed tomogram-guided biopsy of the liver lesion revealed it to be a cholangio-carcinoma of the proximal common bile duct close to theconfluence of the hepatic ducts. The patient underwent a hepatictrisegmentectomy during the same admission.
Three months following surgery, the patient developed acutesymptomatic bilateral deep venous thrombosis (DVT) with the rightdeep venous system involving the right external iliac system. Hewas therapeutically anticoagulated with heparin and transjugularcatheter lysis was performed with placement of a temporarycaval filter. Despite this, the patient developed phlegmasiacaerulea dolens and venous gangrene of the right leg (Fig. 1)and died soon after. A post-mortem examination revealed multiplemetastatic tumour deposits in the remaining liver and largethrombus in the proximal inferior vena cava (IVC), above thelevel of the temporary filter.
Case 2: Superficial thrombophlebitis and theantiphospholipid syndrome
A 24-year-old G2P0 was referred by her obstetrician with atender, palpable cord on the medial aspect of her left thighextending into the groin. She was in the first trimester of hersecond pregnancy having had a spontaneous second semesterabortion 2 years previously. A duplex scan of the affected limbrevealed extensive thrombus at the sapheno–femoral junctionwith discontinuous clot in the ipsilateral external iliac vein. The
Aust. N.Z. J. Surg. (1999) 69, 461–463
CASE REPORT
SUPERFICIAL THROMBOPHLEBITIS: UNDERLYINGHYPERCOAGULABLE STATES
P. SUBRAMANIAM * AND S. VAN DOORNUM†
*Austin and Repatriation Hospital, Heidelberg and †Royal Melbourne Hospital, Parkville, Victoria, Australia
Keywords: hypercoagulable states, superficial thrombophlebitis.
Correspondence: Mr Peter Subramaniam, 4/40 Export Lane, Kensington, Vic. 3031, Australia.Email: <[email protected]>
Accepted for publication 15 June 1998.
Australian and New Zealand Journal of Surgery CASE REPORT CR 1599 EN

patient was taken to theatre and, under a spinal anaesthetic, thesapheno–femoral junction was incised and soft thrombus evacuated.An embolectomy catheter was carefully placed upstream and asecond clot removed resulting in good antegrade and retrogradeflow. The sapheno–femoral junction was then disconnected.Postoperative duplex study showed a patent deep venous system inthe affected limb with no evidence of residual clot. A full coagu-lation profile revealed the patient to have significantly elevatedlevels of lupus anticoagulant and mildly elevated levels of anti-cardiolipin antibodies with normal antithrombin III, protein Cand protein S assays. The platelet countwas at the lower end ofnormal but bleeding time was normal. A diagnosis of anti-phospholipid syndrome was made and the patient was placed indaily low-molecular weight heparin injections until delivery afterwhich she was commenced on warfarin. At the 2-year follow up thepatient had hadno further thrombotic episodes.
Case 3: Recurrent superficial thrombophlebitis and familialprotein S deficiency
A 45-year-old female office-worker presented with recurrentmigratory superficial thrombophlebitis. Clinical examinationwas consistent with ascending superficial thrombophlebitis inthe left long saphenous system. The patient had had a previousepisode of spontaneous migratory thrombophlebitis affectingher left arm. This was treated with oral non-steroidal anti-inflammatory drugs and settled. On closer questioning, thepatient revealed that her sister had had DVT following a kneeathroscopy and that her father had also suffered a spontaneousDVT. A duplex examination revealed occlusive thrombus in thelong saphenous vein propagating into the left superficial femoralvein in the affected limb. A decision was taken to explore thesapheno–femoral junction and this was performed under a spinalanaesthetic. At operation, the sapheno–femoral junction wasincised and the clot was extruded from the superficial femoralvein with patency being established in the deep venous system. Thesapheno–femoral junction was ligated and an arterio–venousfistula created by anastomosing the superficial external pudendalartery to the superficial epigastric vein, which in this patient wasa tributary of the common femoral vein. Postoperatively, thepatient was investigated with a full coagulation screen whichuncovered a reduced free protein S level with a normal anti-
thrombin III and protein C assay. Two first-degree relatives (hersymptomatic father and sister) were also discovered to have sig-nificant reductions in free protein S levels.
DISCUSSION
While the majority of cases of thrombosis of the superficialvenous system limbs are benign, generally self-limiting condi-tions,1 a failure to recognize this condition as a manifestation of an underlying hypercoagulable state can be detrimental to thepatient. This is particularly true in cases of primary hypercoagulablestates where the increased risk of thrombosis can be reducedwith therapeutic anticoagulation. In the main, these primaryhypercoagulable states are inherited conditions. Recognition ofthese conditions, a better understanding of the pathogeneticmechanisms associated with the increased risk of thrombosisand the development of increasingly sensitive assays for coagulantand fibrinolytic factors allows for early detection and appropriateintervention in asymptomatic at-risk family members.2,3 In Case 3,a failure to either elicit or to appreciate the significance of thehistory of two first-degree relatives with thrombotic episodesmay have led to the delay in the diagnosis of the inherited defi-ciency of protein S, an inhibitor of the coagulation system. In itsfree form, protein S combines with activated protein C (APC)to inhibit factor V and VIII in the coagulation cascade.4 In Case 2,the spontaneous abortion, lowered platelet count and the episodeof thrombosis are manifestations of the antiphospholipid syn-drome,5 where the increased risk of thrombosis is attributed tothe presence of lupus anticoagulants (LAC) and anticardiolipinantibodies (ACA), which are directed against proteins such asprotein C and S and some endothelial cell heparin-related com-pounds. Thus, the net effect is to decrease the inhibition of anti-coagulant factors which is increasing the risk of spontaneousthrombosis. In the case of the antiphospholipid syndrome wedescribe, the presence of a pregnancy6 is likely to have com-pounded the hypercoagulable state.
The presence of spontaneous superficial continuous throm-bosis or migratory thrombophlebitis in a patient with no under-lying coagulopathy or varicose veins should alert the physician tothe possibility of an underlying malignant process, as in Case1.This thrombophilic state is likely to be a paraneoplastic pheno-mena7 related to release of tumour generated factors.
Whatever the cause of thrombosis of the superficial venoussystem, the aim of the management of the condition is identifiablythe alleviation of symptoms as well as prevention of potentialcomplications, in particular the risk of pulmonary embolism.This latter risk arises from an involvement of the deep venoussystem either by propagation from the superficial system (clotextension at the sapheno–femoral junction or via regurgitantperforating veins lower in the leg) or by simultaneous occur-rence of deep venous thrombosis unrelated to thrombosis ofthe superficial system. The incidence of simultaneous DVT isreported as being up to 30%.8,9 Duplex scan imaging hasemerged as the non-invasive investigative tool of choice,10 not onlyfor establishing patency of the deep venous system but also forvisualizing the extent and location of thrombosis in the superficialveins allowing assessment of risk of proximal embolization.
While anticoagulant therapy alone, or with non-steroidalagents,11 have been shown to alleviate the symptoms of superficialthrombophlebitis, neither deals with the risk of embolizationwhen this risk is present. Fibrinolytic agents have shown recentpromise in trials12 but as yet have not proven to be as effective as
462 SUBRAMANIAM AND VAN DOORNUM
Fig. 1. Clinical photograph showing phlegmasia caerulia dolens andvenous gangrene in a patient with extensive ilio-femoral occlusivethrombus.

surgery in terms of length of hospital stay and effective eliminationof risk of proximal embolization.
Careful exploration of the sapheno–femoral junction is requiredwhen the clot approximates this junction or is in fact propagated intothe deep femoral system. Minimal mobilization of the junctionprior to incision of the junction reduces the risk of clot fracture andproximal embolization. We position an opened Satinsky clamparound the junction prior to incision and extrusion of clot. Theclamp is applied only once the clot is evacuated and efficientback-bleeding is established. In cases of varicophlebitis, we donot perform varicectomy at the time of acute presentation because wefind the vein is usually friable at this stage, with bleeding andhaematoma being a common occurrence if stripping is attempted.
In conclusion, the cases reported here clearly demonstrate the needfor further investigation for either unsuspected underlying malig-nancy or a primary hypercoagulable condition when superficialthrombophlebitis presents in the absence of varicose veins in thelower limb, and in the upper limb, a history of recent intravenouscannulation. When an underlying hypercoagulable condition issuspected, we advocate routine anticoagulation screen (inter-national normalized ratio, activated partial thromboplastin time,prothrombin time ratios with D-Dimer assay) as well as a specialanticoagulation screen, which should include assays for anti-thrombin III, protein C and S, antiphospholipid and anticardio-lipin antibody, activated protein C Factor V Leiden mutation andhomocystein assays, and rheumatoid factor assay. The use ofDuplex scanning is critical in these cases in order to identify theextension of clot into the deep venous system as well as synchronous DVT of the lower limb. We believe early andcareful disconnection of the sapheno–femoral junction in cases atrisk of distal pulmonary embolization is the appropriate management.
REFERENCES
1. Husni EA, Williams WA. Superficial thrombophlebitis of lowerlimbs. Surgery1981; 90: 70–4.
2. Guex JJ. Thrombotic complications of varicose veins. A literaturereview of the role of superficial venous thrombosis. Dermatol.Surg.1996; 22: 378–82.
3. Samlaska CP, James WD. Superficial thrombophlebitis 1. Primaryhypercoagulable states. J. Am. Acad. Dermatol.1990; 22: 975–89.
4. Samama MM, Simon D, Horellou MH et al. Diagnosis and clini-cal characteristics of inherited activated protein C resistance.Haemostasis1996; Suppl. 4: 315–30.
5. Shapiro SS. The lupus anticoagulant/antiphospholipid syndrome.Ann. Rev. Med. 1996; 47: 533–53.
6. Cranley JJ. Venous thrombotic complications of pregnancy.Cardiovasc. Surgery1996; 4: 777–82.
7. Samlaska CP, James WD. Superficial thrombophlebitis 2. Sec-ondary hypercoagulable states. J. Am. Acad. Dermatol.1990;23: 1–18.
8. Skillman JJ, Kent KC, Porter DH et al. Simultaneous occurence ofsuperficial and deep thrombophlebitis in the lower extremity. J. Vasc. Surg.1990; 11: 818–24.
9. Prountjos P, Bastounis E, Hadjinikolaou L et al. Superficialvenous thrombosis of the lower extremities co-existing withdeep venous thrombosis. A phlebographic study on 57 cases.Int. Angiology1991; 10: 63–5.
10. Lutter KS, Kerr TM, Roesdersheimer R et al. Superficialthrombophlebitis diagnosed by duplex scanning. Surgery1991;110: 42–6.
11. Lofgren EP, Lofgren KA. The surgical treatment of superficialthrombophlebitis. Surgery1981; 90: 49–54.
12. Belcaro G. Evolution of superficial vein thrombosis treated withdefibrotide: A comparison with low-dose subcutaneous heparin.Int. J. Tissue Reactions1990; 12: 319–24.
SUPERFICIAL THROMBOPHLEBITIS 463
Aust. N.Z. J. Surg. (1999) 69, 463–465
CASE REPORT
SUCCESSFUL RECONSTRUCTION OF LEFT MAIN BRONCHUSFOLLOWING TRAUMATIC RUPTURE
QIANG CHEN AND BEDE H. SQUIRE
Department of Cardiothoracic Surgery, Wellington Hospital, Wellington, New Zealand
Key words: bronchial rupture, chest trauma, surgical reconstruction.
INTRODUCTION
Traumatic bronchial rupture is rarely presented. We report acase of uncommon traumatic left main bronchial rupture in a27-year-old woman. The mechanism, early diagnosis and surgicaltreatment of bronchial rupture are reviewed. This case demon-strates the need to have a very high index of suspicion in cases ofblunt thoracic trauma.
CASE REPORT
On 4 April 1997, a 27-year-old woman fell from her horsewhile riding. The horse then rolled on top of her. She wasadmitted to a local hospital where a chest X-ray showed amoderate-sized left pneumothorax with multiple pulmonarycontusions. An intercostal tube was inserted for 48h and herlung expanded promptly. However, her pulmonary contusionstook longer to resolve and she stayed in hospital longer for vig-orous physiotherapy. She was discharged 10days after the accidentwith a normal chest X-ray. However, she remained breathlessand was admitted to another local hospital 7 weeks after injury.The chest X-ray at this time showed some atelectasis of the left
Correspondence: Dr B. H. Squire, Cardiothoracic Surgery Unit, WellingtonHospital, Wellington, New Zealand.
Accepted for publication 19 February 1998.

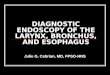
lung and the computed tomographic scan showed occlusion of theleft main bronchus (Fig.1). She was hypoxic and breathless at rest.She was then transferred to the Cardiothoracic Unit of WellingtonHospital, New Zealand.
On examination she was slightly cyanosed. The trachea wasdeviated to the left, and there was no air entry on the left side. Thechest X-ray showed complete collapse of the left lung (Fig.2). A ventilation/perfusion scan showed some perfusion but no ventilation of the left lung. Perfusion and ventilation of the right lungwas normal. Her forced expiratory volume in 1s (FEV1) was 1.66and forced vital capacity (FVC) was 1.96 about half predicted andconsistent with the left lung collapse. Immediate bronchoscopywas performed after admission, which showed total obstruction of theleft main bronchus about 1.5cm from the carina, highly suggestiveof a ruptured bronchus with some healing. She was given anti-biotics and vigorous physiotherapy but remained generally unwell.
Ten weeks after trauma the patient underwent surgery. A right-sided double-lumen tube was placed. Left posterolateral thoracotomywas performed. There were light adhesions between the anterior
surface of the upper lobe and chest wall. The tissues around the lefthilum were moderately inflamed and scarred. It was found thatthere was a complete rupture of the bronchus 2cm from its originwith separation of the ends by about 1.5cm. There was a pin-head sized hole through the obstruction. The distal bronchus wasopened and the bronchial tree sucked out. The proximal bronchuswas then identified and opened and the edges trimmed. The left lungwas fully mobilized. End-to-end anastomosis was performedusing interrupted 4-0 PDS sutures. Haemostasis was secured and thelung was re-expanded. The bronchial suture line was tested withairway pressures up to 40cmH2O. A pleural flap was then raised offthe aorta and passed around the bronchial suture line and sutured infront to cover the suture line. The chest was closed after the insertionof two chest drains.
Her postoperative recovery was satisfactory and her respiratoryfunction improved immediately. Postoperative expiratory testsshowed a FEV1 of 2.6, FVC of 2.87. Air entry was excellent to aus-cultation of the left lung and her chest X-rays showed satisfactoryappearances (Fig.3). She was discharged 8 days after surgery in goodclinical condition. Four weeks after surgery, follow-up bronchos-copy showed satisfactory healing of the anastomosis. There was nogranulation tissue nor narrowing at the site of the anastomosis.
DISCUSSION
Traumatic bronchial rupture is rarely presented. It may bebecause most patients die before reaching hospital.1,2 On review of1178 autopsies of blunt trauma, Bertelsen and Howitz foundonly 33 (0.03%) patients had bronchial trauma, and among thesepatients, 27/33 died before reaching hospital.1
Bronchial rupture usually results from motor vehicle acci-dents.1,2 There are two groups of traumatic rupture.2 In the firstgroup, rupture is intrapleural with free communication with thepleural space. This presents with a large pneumothorax andpersistent large air leak. Respiratory distress may be increased whensuction is applied to intercostal chest drains. In the second
464 CHEN AND SQUIRE
Fig. 1. Computed tomographic scan shows occlusion of the leftmain bronchus.
Fig. 2. The chest X-ray shows complete collapse of the left lung.
Fig. 3. Postoperative chest X-ray shows a satisfactory appearance.

group, rupture is limited to the mediastinum, with no or littlecommunication between the extrapleural tear and the pleuralcavity. The patient may present with mediastinal and cervicalemphysema, but this may be only slight and sometimes withsmall pneumothorax. Distinct from the first group, the lungusually re-expands with insertion of a chest drain. Tracheo-bronchial stricture may form later by granulation tissue andextensive scarring.
Pathogenically, three mechanisms of bronchial rupture havebeen described.3,4 First, forceful compression of the thorax pullseach lung apart; with the resulting traction on the carina theforce of traction exceeds the elasticity of the bronchus. Second,reflex closure of the glottis occurs when the thorax is com-pressed, which produces a rapid increase of intrabronchial pressure.Third, rapid acceleration/deceleration may create shearingforces between the bronchus and trachea. Our patient was lyingdown when the horse fell on to her chest, this position favouredforceful compression. A patient with a serious thoracic injurymay not have any accompanying bony injury. High energy may betransferred to the body through the soft tissues particularly inyoung patients whose chests are more flexible.
The symptoms and signs of bronchial rupture are dyspnoea,subcutaneous emphysema, cyanosis, and pneumothorax.5 Latesymptoms such as cough, dyspnoea, wheezing or stridor may par-ticularly present in type 2 patients since the distal lung may beaffected by recurrent infections or bronchiectasis.5,6 Bronchos-copy is the most useful method for diagnosis and should be used inany chest trauma patient if bronchial rupture is suspected.3 It mostcommonly gives the definitive diagnosis, but should be repeated if the diagnosis is not clear in the early stages.7,8 Computed tomo-graphic scan may be useful to show any related lesions.7
Primary repair of the ruptured bronchus results in restoration oflung function and leads to good long-term results,2,8 even thoughresection of lung tissue in some situations such as extensive injuryor severe infection may not be avoided.5,9 The majority of ruptures aresituated within 2.5cm of the carina,6 as it was in our patient.
When recognition of bronchial rupture is delayed, repair withgood results is still possible. If the stenosis is incomplete, thedistal lung may become seriously infected and destroyed andneed to be resected.5,9 In cases with complete stricture of thebronchus, the distal lung is often relatively healthy despite theatelectasis, and may make a good recovery towards normalfunction after the re-establishment of a patent airway.4
Follow-up bronchoscopy should always be performed becauserecurrent stenosis may occur in both primary and secondaryrepair of bronchial rupture.10,11This stenosis can be treated eitherwith endoscopic laser therapy or by reoperation.11,12
In conclusion, a ruptured bronchus must be suspected in cases ofhigh energy blunt injury. The patient may present late with dysp-noea, stridor or wheezing when a bronchial stenosis is formedby granulation tissue. Bronchoscopy is the main method fordiagnosis. A good clinical outcome can be achieved with surgicalresection of the stenotic segment of ruptured bronchus and re-anastomosis with absorbable sutures.
REFERENCES1. Bertelsen S, Howitz P. Injuries of the trachea and bronchi.
Thorax1972; 27: 188–94.2. Kirsh MM, Orringer MB, Behrendt DM, Sloan H. Management
of tracheobronchial disruption secondary to non penetratingtrauma.Ann. Thorac. Surg.1976; 22: 93–101.
3. Taskinen SO, Salo JA, Halttunen PEA. Tracheobronchialrupture due to blunt chest trauma: A follow-up study.Ann.Thorac.Surg.1989; 48: 846–9.
4. Chesterman JT, Satsangi PN. Rupture of the trachea and bronchiby closed injury.Thorax. 1966; 21: 21–7.
5. Roxburgh JC. Rupture of the tracheobronchial tree [Review].Thorax. 1987; 42: 681–8.
6. Jones WS, Mavroudis C, Richardson JD, Gray LA, Howe WR.Management of tracheobronchial disruption resulting from blunttrauma.Surgery1984; 95: 319–22.
7. Rupprecht H, Rumenapf G, Petermann H, Gunther K. Transthoracicbronchial intubation in a case of main bronchus disruption.J.Trauma1996; 41: 895–8.
8. Symbas PN, Justicz AG, Ricketts RR. Rupture of the airways fromblunt trauma: Treatment of complex injuries.Ann. Thorac. Surg.1992; 54: 177–83.
9. Deslauriers J, Beaulieu M, Archambault G, LaForge J, Bernier R.Diagnosis and long-term follow-up of major bronchial disruptionsdue to nonpenetrating trauma.Ann. Thorac. Surg.1982; 33: 32–9.
10. Lazar HL, Thomashow B, King TC. Complete transection ofthe intrathoracic trachea due to blunt trauma.Ann. Thorac.Surg.1984; 37: 505–7.
11. Amauchi W, Birolini D, Branco PD, de Oliveira MR. Injuries tothe tracheobronchial tree in closed trauma.Thorax. 1983; 38:923–8.
12. Muysoms FE, Van Swieten HA. Primary repair of a main andlobar bronchus.J. Thorac. Cardiovasc. Surg.1997; 113: 415–17.
RECONSTRUCTION OF BRONCHUS 465