Embed Size (px)
Citation preview

CELLULAR IMMUNOLOGY 79, 403-406 ( 1983)
Successful Rat Pancreatic Islet Allotransplantation without Recipient Immunosuppression’
KELLY TUCKER,* MASAOSUZUKI,* NANCY J. WALDECK,* GREG JONES,* AND M. ARTHUR CHARLES*‘?”
Departments of *Medicine and tPhysiology, University of California, Iwine. Calqornia 92717
Received March 23, 1983; accepted April 7, 1983
Pancreatic islets from Wistar Furth (RT 1”) rats are rejected by 5 days after transplantation into the liver of the diabetic Lewis (RTl’) rat. Pretreatment of Wistar Furth islets by culture for 7-10 days in 95% Or 5% CO2 reduces immunogenicity permitting successful allotransplantation as defined by normal blood and 24-hr urinary glucose values.
INTRODUCTION
Prolonged survival of pancreatic islet allografts has been reported after in vitro culture of islets prior to transplantation (l-3). In mice 100% successful islet allografts were performed after in vitro high oxygen exposure without recipient immuno- suppression treatment (3). Ia antisera and complement treatment of mouse islets prior to transplantation also results in 100% successful allografts in nonimmunosup- pressed diabetic mice (4). In the rat islet allograft model, however, 100% successful transplants are only reported after in vitro room temperature culture and antilym- phocyte serum treatment of recipients (2). There is now evidence suggesting that specific cells (e.g., macrophages and/or endothelial cells) present within the transplanted islets play a central role in allograft rejection (5-8). The beneficial role of in vitro culture prior to transplantation has been suggested to be due to depletion of these immune stimulator cells and, in the case of rat islets, depletion of Ia antigen-bearing capillary endothelial cells (3, 5, 6). This premise is supported by the acute rejection of successful islet allografts when recipients are injected with donor (syngeneic with the allografted islets) peritoneal cells, mixed-spleen cells, or spleenderived T lym- phocytes (7-9) and by the fact that successful islet allografts have been performed using islets treated with monoclonal antibodies to Ia determinants and com- plement (4).
In this paper, we describe a procedure that permits successful pancreatic islet allotransplantation in a rat model after in vitro islet culture in high oxygen without immunosuppression of recipient diabetic rats.
’ This study was in part funded by the UC President’s Undergraduate Research Fellowship award. ’ To whom correspondence should be addressed: Department of Medicine, Medical Sciences I, Rm C240,
University of California, Irvine, Calif. 927 17.
403
0008-8749/83 $3.00 Copyright 0 1983 by Academic Press, Inc. All rights of reproduction in any form reserved.

404 SHORT COMMUNICATIONS
600s
100
O / I 1 I 1 1 1 0 IO 20 30 40 50 60 1, % 70
TIME (DAYS)
i-
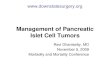
FIG. 1. Blood glucose values in allograft recipients (n = 9) of high oxygen-treated islets (closed circles, solid line, 02Rx) are similar to values obtained from control recipients (n = 3) of high oxygen-cultured, syngeneic islets (open circles, dashed lines, 02Rx). Allografi recipients (n = 10) receiving nontreated islets (closed squares, solid line, no 02Rx) are shown to have persistently elevated blood glucose levels.
MATERIALS AND METHODS
Islet allograft donors were inbred Wistar Furth (RTl”) rats and recipients were Lewis (RTl ‘) rats previously made diabetic using iv streptozotocin (65 mg/kg). Donor pancreatic islets were isolated by the method of Lacy and Kostianovsky (10). Islet yields ranged from 450 to 600 islets per donor. Islets from five Wistar Furth donors were used for each allograft. Groups of approximately 150 islets were transferred to 12 X 75-mm polystyrene tubes (Falcon 2054) and washed with two changes each of Hanks-Hepes solution, Dulbecco’s modified Eagle’s medium (DMEM, GIBCO, Santa Clara, Calif.), and DMEM supplemented with 10% fetal calf serum (FCS, GIBCO). Resulting islets were then transferred to 35 X IO-mm hydrophobic tissue culture dishes (Falcon 3001) containing 2 ml of DMEM with 10% FCS. Islet clumps were formed by gentle manual oscillation of the tissue culture dish for 2-3 min. Islet clumps were then incubated at 37“C and reclumped at 6- to 8-hr intervals over the next 24 hr. Medium volume was then reduced to 0.5 ml and islets were reincubated at 37’C in an atmosphere of 95% O2 and 5% CO2 for a period of 7-10 days. Culture medium and atmosphere were changed daily. Cultured islets were washed with two changes of DMEM with 10% FCS and transplanted via the portal vein route as previously described (11, 12). Urine and serum glucose levels were measured using the Ames Dextrosystem (Dextrostix and Glucometer).
RESULTS
When 7- to lo-day high oxygen-cultured islet clusters from Wistar Furth rats were transplanted via the portal vein into diabetic Lewis recipients, no allograft rejection

URINE GLUCOSE
(gm/24 hr)
SHORT COMMUNICATIONS
0 10 20 30 40 50 60 70 3
TIME (DAYS)
405
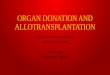
FIG. 2. Twenty-four-hour urinary glucose values in allograft recipients (n = 9) of high oxygen-treated islets (closed circles, solid line, 02Rx) are shown to be similar to values obtained from control recipients (n = 3) of high oxygen-cultured syngeneic islets (open circles, dashed line, OzRx). Allograft recipients receiving nontreated islets (closed squares, solid line, no OzRx) are shown to have persistently elevated urinary glucose levels.
was observed. Nonfasting blood glucose levels decreased from the diabetic range of 500-600 mg/dl to the range of 100 mg/dl (Fig. 1). Similarly urine glucose decreased from the diabetic range of 8 g/24 hr to the range of 0.004-0.010 g/24 hr by 10 days (Fig. 2). These glucose values do not vary significantly from values observed in control syngeneic high oxygen-treated islet transplant recipients, but are markedly different from glucose values derived from recipients of non-high oxygen-cultured islets (Figs. 1 and 2). All high oxygen-associated allografts remain successful with blood and urine glucose levels remaining normal in excess of 100 days.
DISCUSSION
Islet clusters of approximately 150 islets, unlike single islets, survive when cultured in an atmosphere of 95% O2 and 5% COz for 7-10 days. Our findings indicate that islets so cultured can be used for successful islet allotransplantation in a rat model. Further, this method permits long-term cure of diabetes in nonimmunosuppressed recipient animals.
It appears that in vitro culture at high oxygen concentration alters or diminishes both passenger hematogenous immune cells and/or capillary endothelial cells normally present in islets. Lymphocytes, macrophages, and capillary endothelial cells from rat islets have all been shown to express Ia antigens (6, 13). Since Ia antigens are considered important in allograft rejection, removal of cells bearing high concentrations of these antigens may explain, at least in part, allograft survival after in vitro high oxygen.
ACKNOWLEDGMENTS
The authors thank Penny Gebert and Susan Bums for excellent preparation of the manuscript.

406 SHORT COMMUNICATIONS
REFERENCES
1. Kedinger, M., Haffen, K., Grenier, J., and Eloy, R., Nufure (London) 270, 736, 1977. 2. Lacy, P. E., Davie, J. M., and Finke, E. A., Science, 204, 312, 1979. 3. Bowen, K. M., Andrus, L., and Lafferty, K. J., Diabetes 29,(Suppl. 1), 98, 1980. 4. Faustman, D., Hauptfeld, V., Lacy, P., and Davie, J., Proc. Nat. Acud. Sci. USA 78, 5 156, 1981. 5. Lafferty, K. J., and Woolnough, J., Immunol. Rev. 35,231, 1977. 6. Rabinovitch, A., Alejandro, R., Noel, J., Brunschwig, J. P., and Ryan, U. S., Diabetes Jl(Supp1. 4),
48, 1982. 7. Lacy, P., Davie, J., and Finke, E., Transplantation 28, 415, 1979. 8. Bowen, K. M., Prowse, S. J., and Lafferty, K. J., Science 213, 1261, 198 1. 9. Zitron, I. M., Ono, J., Lacy, P. E., and Davie, J. M., Diubaes 30, 242, 1981.
10. Lacy, P. E., and Kostianovsky, M., Diabetes 16, 35, 1967. 11. Kemp, C. B., Knight, M. J., Scharp, D. W., Lacy, P. E., and Ballinger, W. F., Nature (London) 244,
447, 1973. 12. Charles, M. A., Imagawa, W., Forsham, P. H., and G&sky, G. M., Endocrinology 98, 738, 1976. 13. Parr, E. L., Bowen, K. M., Lafferty, K. J., Transplantation 30, 135, 1980.