Embed Size (px)
Citation preview

Successful Integrated
Care Systems
February, 2015
CONFIDENTIAL AND PROPRIETARY
Any use of this material without specific permission of McKinsey & Company is strictly prohibited

| McKinsey & Company 1
Known context: aging populations drive care demand
SOURCE: McKinsey team analysis, HES 2010/11, FIMS, Q research/NHS Information centre, PSSEX;
NHS Reference Costs
Exhibit 7: Strong relationship between age and prevalence of long-term
conditions
19-390-18 40-64 65-74 75-84 85+
50
40
30
20
10
0
AgeYears
Percent of total
100
90
80
70
60 5+ conditions
4 conditions
3 conditions
2 conditions
1 condition
0 conditions
SOURCE: McKinsey team analysis, HES 2010/11, FIMS, Q research/NHS Information centre, PSSEX; NHS Reference Costs
64% of those
aged 75-84
have more
than one LTC
69% of those
aged 85+
have more
than one LTC

| McKinsey & Company 2
Integrating care: from art to professional management
SOURCE: McKinsey
1) Remarkable success on managing populations around the
world
2) All successful players do 3 things
- Understand their patient population really well
- Build new care model around the patient
- Tailor key enablers IT, payments, and workforce to their
specific local context
3) Much can be done in 2 years

| McKinsey & Company 3
Australia – Diabetes Care
Project
Successful integrated care systems exist in many countries
Valencia:
Integrated HC
UK – Torbay
integrated care
UK – Tower
Hamlets
UK – NWL
integrated care
Montefiore Bronx
Pioneer ACO
Germany - Bundesknappschaft
UK – Greenwich
South Central
Foundation Alaska
Camden Coalition of
Healthcare Providers
State of Arkansas BCBS CareFirst
BCBSMA AQC
Geisinger
ChenMed
CareMore
New York Care
Coordination Program
Colorado
Children’s Health
Access Program
SOURCE: McKinsey analysis of public source material; details in appendix

| McKinsey & Company 4
Integrating care: from art to professional management
SOURCE: McKinsey
1) Remarkable success on managing population around the world
2) Most successful players do 3 things
- Understand their patient population really well
- Build new care model around the patient
- Tailor key enablers IT, payments, and workforce to their
specific local context
3) Much can be done in 2 years

| McKinsey & Company 5
McKinsey research shows that in all these case examples, 3 building
blocks to a successful integrated care systems
Support with Enablers
Payment Governance Information Leadership Patient Centred
Success in coordinated care
Organise Delivery
Care
Coordi-
nation
Self-
empowerment
and education
Individual
care plans
Multi-disciplanary
teams
Understand Needs 2 1
3
SOURCE: 40 leaders in integrated care research programme

| McKinsey & Company 6 SOURCE: Example health economy, McKinsey analysis
Understanding needs of population requires segmentation 1 UNDERSTAND NEEDS
Joe, 34
No LTC 1
Mostly
healthy adults
Susie, 10
Diagnosed
with epilepsy
4 Children with
one or more
LTCs
Janet, 25
Diagnosed
with
schizophrenia
5 Adults and
elderly people
with SEMI
Frank, 79
Diagnosed
with CVD,
COPD and
diabetes
3
Elderly
people with
one or more
long term
conditions
Abbie, 1
No LTC 2
Mostly
healthy
children
Patient story
▪ Joe is a healthy adult
▪ He rarely visits his GP
▪ Joe was admitted to hospital with
appendicitis 5 years ago but made a full
recovery
▪ Susie was diagnosed after being
admitted to hospital after experiencing a
partial seizure
▪ Janet was diagnosed at 19
▪ She lives with her parents
▪ She has recently been discharged from
hospital after a 45 day stay in the
psychiatric ward
▪ Frank has multiple long term conditions,
and is having trouble navigating disease
pathways
▪ He was admitted to hospital twice this
year with complications for diabetes,
including a foot ulcer
▪ Abbie is a healthy child, attending GP
mainly for planned appointments (e.g.
immunisations)
▪ She receives care from GP, practice
nurses, health visitor
Annual
cost
£
▪ 800
▪ 3,600
▪ 27,000
▪ 9,500
▪ 650
Non-elective
ad-missions
per year
▪ <1
▪ 2
▪ 1 (45 day
stay)
▪ 2
▪ <1
GP
contacts
per year
▪ 1 visit
▪ 5 visits
▪ 8 visits
▪ 9 visits
▪ 1 visit
| McKinsey & Company 7
Age
Learning
disability
Socially
excluded
groups
Mostly
healthy
Defined
episode of
care Single LTC
Multiple
LTC
2 5 8 10 11
12 1 4 7
0-15
16-74
75+
6 3
26,72932,081
9,497
661
808
n/a
NA
NA
NA
3,588
4,017
Serious
and
enduring
mental
illness
Intensive
continuing
care needs
NA NA 1.4 44.3 2.4 64.5 NA NA
13.9 131.5
109.6 72.5 3.2 11.3 NA NA
64.2 257.9 503.0 406.6
12.5 55.0
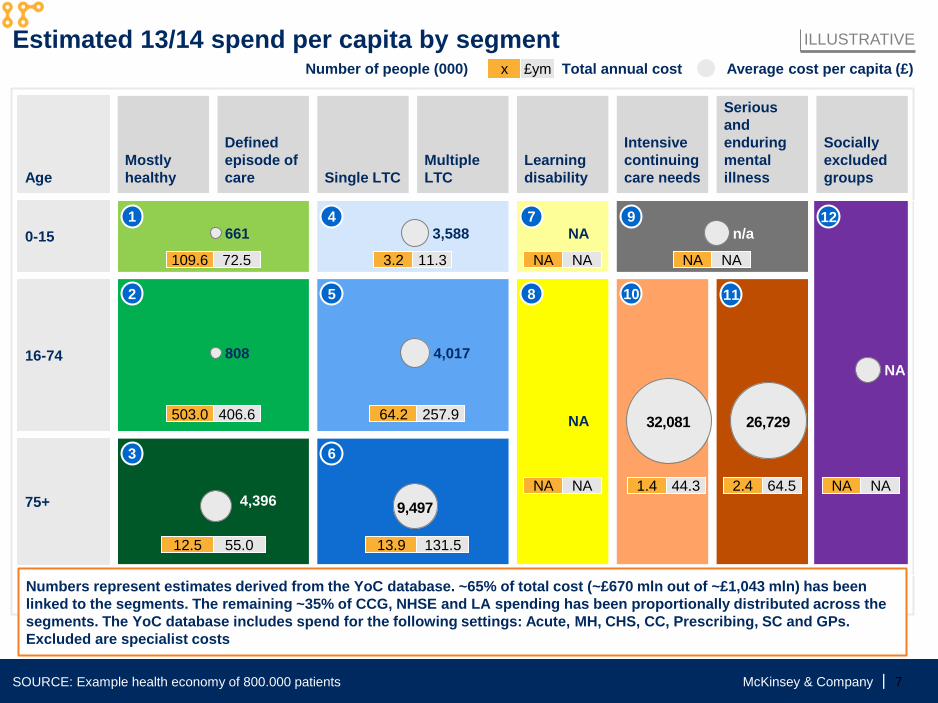
x £ym Number of people (000) Total annual cost Average cost per capita (£)
Estimated 13/14 spend per capita by segment
Numbers represent estimates derived from the YoC database. ~65% of total cost (~£670 mln out of ~£1,043 mln) has been
linked to the segments. The remaining ~35% of CCG, NHSE and LA spending has been proportionally distributed across the
segments. The YoC database includes spend for the following settings: Acute, MH, CHS, CC, Prescribing, SC and GPs.
Excluded are specialist costs
4,396
9
NA NA
SOURCE: Example health economy of 800.000 patients
ILLUSTRATIVE

| McKinsey & Company 8
Organise delivery around the person 2 ORGANISE DELIVERY
Individual
Home-care team
▪ Provide health and
social care
multidisciplinary support
▪ Modify home
environment to facilitate
independence
Named GP
▪ Provides regular monthly
review and same day
care when needed, 20-
40 minute appointments
▪ High service user/GP
continuity
▪ Manages list of ~450
service users
▪ Develops trusting
relationship with patient
▪ Leads multidisciplinary
team
▪ Facilitates production
of care plan
Individual
▪ Takes ownership of care
▪ Seeks education on condition
▪ Makes decisions on best care
to suit preferences
▪ Self-manages some conditions
Other GPs
▪ Participate in regular
review of patient care
within practice/network
▪ Provide informal advice
when necessary
▪ Provide peer review of
named GP’s outcomes
▪ Provide out of hours care
as part of network
Other providers
▪ Provide social and
mental health input
where required
▪ Provide specialist advice
on site and remotely
▪ Provide inpatient beds
and treatment

| McKinsey & Company 9
5 key enablers are crucial to change behaviour SUPPORT WITH ENABLERS
SOURCE: Carter, Chalouhi, Richardson – What it takes to make integrated care work (McKinsey Health International, 2011); Latkovic - The
trillion dollar prize (Health International 2013) and Fountaine, Richardson and Wilson - Changing behaviour in primary care
(Health International 2013)
3
Governance Information Leadership Payment Patient Centred
▪ Significant
(30%+)
▪ At scale
(30%+)
▪ Sustained
(3-5 years)
▪ Align risk and
reward across
system
▪ Support
– Citizen
records
– Clinical
decision
making
– Peer
pressure
– Payment
▪ Solve
Information
governance
▪ CEOs &
Boards
commitment
of resources
▪ Bind in
payors,
hospitals,
primary care
and local
government
▪ Hold to
account
▪ Role model
behaviour
▪ Deliver
consistently
▪ Hold peers to
account
▪ Work within
team
▪ New ways of
doing things
requires
support to
learn how
▪ Encourage
self care and
patient
empowerment
throughout

| McKinsey & Company 10
Integrating care: from art to professional management
SOURCE: McKinsey
1) Remarkable success on managing population around the world
2) All successful players do 3 things
- Understand their patient population really well
- Build new care model around the patient
- Tailor key enablers IT, payments, and workforce to their
specific local context
3) Much can be done in 2 years

| McKinsey & Company 11
To build a coherent population management system is 10 year+ journey,
but impact at scale can be done in 2 years (examples)
SOURCE: McKinsey
- Activity incenting
products, e.g.
Discovery
- Social marketing in
infectious diseases,
e.g. PSI
- Smoking bans
- Urban planning, e.g.
MA road tax
- Care packages plus
OD, e.g. diabetes
- Home-telecare, e.g.
Airdale
- I triage, e.g. Aetna
- System care
planning, e.g. stroke
- Carve out, e.g.
Clinicas Azucar,
Chenmed
- Switch to episode
based payment, e.g.
Arkansas
- Ueber homecare
Action
complete in 2
years, and
time to
impact
Within 2
years
Fast to
milestone,
but longer
to impact
Primary prevention LTC management
Thrust

| McKinsey & Company 12
Case Example – Integrated care models in
Tower Hamlets are now nationally recognised best practice
▪ Patients in Tower
Hamlets suffered
worse outcomes,
especially for long
term conditions,
than peers
elsewhere
▪ Local CCG was
committed to
delivering significant
improvements in
long term conditions
and public health
Impact Context Approach
▪ Designed a comprehensive
organisational development
programme to support groups of GP
practices working together as networks
of 4-5 practices, jointly delivering care
packages for diabetes and
immunisations.
▪ Developed care packages led by
clinical working groups and testing
with patient representative groups
▪ Facilitated design of new care delivery
model co-developed by GPs. This
required them to have joint Multi
Disciplinary Teams, share patient lists,
and share resources (including being
paid as one group).
▪ Facilitated and ran trainings,
coaching, and other tailored support
to the clinicians, both in large group
settings and through individual visits to
practices
▪ Increased investment in
primary care from 9.4% to
13.8% of total spend
▪ Diabetes pilots achieved 11%
increase in people with
BP<140/80; 10.4% increase
with cholesterol <4.5; 7.7%
increase with HbA1c<7.5;
600% increase in patients with
diabetes care plans; modelling
suggests 12-14% fall
in acute spend
▪ Immunisation rates rose by 50
% to achieve herd immunity at
92%
▪ Impact of work cited in BMJ
Quality and Safety Journal 1
1 Hull et al., Improving outcomes for patients with type 2 diabetes using general practice networks: a quality improvement project in
east London, BMJ Qual Saf, 2013;0:1-6

| McKinsey & Company 13
Case example – Arkansas Medicaid has become a leader in the US
▪ Arkansas undertook
the design and/or
implementation of
episode-based
payments for
behavioral health
conditions, maternity
and neonatal care,
as well as for
persons with
developmental
disabilities (DD) and
those in need of
Long-Term Services
and Supports
(LTSS)
Impact Context Approach
The integrated solution for behavioral health
centered on four components
▪ Behavioral health homes and patient-
centered medical homes to manage
integrated care plan and coordinate care
across settings to improve adherence and
align services to needs
▪ Behavioral health episodes: Payment
systems to increase provider accountability,
align interests, support accurate diagnoses
and increase adoption of evidence-
informed practices
▪ Independent assessment & care
planning: Increase utilization of cost
effective home & community based
services and detailed assessment to
improve care planning to better align
services with needs and to improve
outcomes
▪ Provider accountability: Monitoring and
reporting to increase provider transparency
and empower continuous improvement
activities among BH stakeholders
▪ Largest implementation of
episode-based payment in the
U.S., involving >1,000
providers in Wave 1 across a
diverse range of medical,
surgical, and behavioral
episodes: ADHD, CHF, joints,
pregnancy, upper respiratory
infections
▪ Achieved savings of up to 22%
in initial wave of episodes
▪ Won $42M in CMS support
through a SIM Model
Testing grant
▪ Credited by Governor for
contributing to the lowest
growth rate in Medicaid
spending in 30 years

| McKinsey & Company 14
Case Example – Through defined processes supported by innovative
technology, ChenMed has become a clear leader in elderly care
▪ The program is
aimed at low to
middle income
Medicare Advantage
patients with
complex chronic
care needs
▪ There are currently
36 ChenMed health
centers across 8 US
states
▪ Organisation is
clinician-led, with
strong cultures and
shared values going
back to founder
Impact Context Approach
▪ 38.2% lower hospital bed days
18% lower hospitalization rate
and 17% lower readmissions
rates compared to national
averages for patient group
▪ 73% medication adherence for
people with diabetes,
compared to 44% previously1
▪ Average Net Promoter Score
of 92 in 2011 (30% of patients
surveyed each day)
▪ Very strong IT infrastructure
supports care delivery, performance
management and revenue
optimization e.g., physicians and
patients communicate through mobile
channels outside of appointments
supported by the EMR
▪ Patients are offered high-frequency
consultations (minimum 1/month),
enhanced services in a single location
and free transport to appointments
▪ Physicians are offered small panel
sizes (typically 1:400) and financial
incentives to manage patient care out-
of-hospital
▪ High staff-to-physician ratios
support task-shifting – with onsite
specialists, pharmacy, diagnostic
dental and acupuncture services all
available
1 Medication possession ratio measured from 2009 to 2011 by University of Miami research team following introduction of new dispensing system
SOURCE: Health Affairs, 32, no.6 (2013):1078-1082; ChenMed website; Concierge medicine for the poorest, Forbes, 23/02/12