Embed Size (px)
Citation preview

8/3/2017
1
Dentsply SironaThe Start of Something Great
The Keys to… Successful, Predictable, and Efficient Direct Posterior Composite
Restorations
Clinical Education Manager
Clinical Affairs
DENTSPLY Sirona Restorative
Associate Professor & Chair
Department of Diagnostic Sciences
Creighton University School of Dentistry
Jason H. Goodchild, DMD
• From Philadelphia, PA
• Private Practice (Havertown, PA)
• Education
– Univ. of Pennsylvania School of Dental Medicine
• Dept. of Oral Medicine
– Creighton University School of Dentistry
• Chairman, Dept. of Diagnostic Sciences
– Dentsply Sirona Restorative• CE Manager, North America
Introduction As of 2016… Dentsply Sirona
Why Dentsply Sirona?
Unmatched clinical education platform
World‐class sales, service, and support
Increased product breadth and scale
Integrated solutions that optimize workflow
Better, safer, and faster dental care
Single‐visit dentistry portfolio
Success in dentistry is mainly dependent on doing the basics well
Success is not an accident!~ Tony Robbins
Ultimate Power

8/3/2017
2
Simple Class
• Preparation
• Caries removal
• Isolation
• Adhesion
• Material placement
• Light curing
• Occlusion
• Finishing / Polishing
Class 1 Posterior Composite
BEFORE
AFTER
Class 1 Posterior Composite
Complex Class
• Preparation• Caries removal• Etching?• Isolation• Adhesion• Material placement• Light Curing• Occlusion• Finishing / Polishing
Class 2 Posterior Composite
BEFORE
AFTER

8/3/2017
3
Filler Particle Size
Incremental Curing
Polymer shrinkage
Shades
FlowableComposites
THENFiller particles quite large, not silanated→ par cles to break out, ditching, increased wear.
Cured in quantities of 2mm or less→ lengthy technique‐sensitive process
Volumetric shrinkage of 7% was common → Various placement techniques to minimize effects of leakage and debonding
Few shades and lack of translucency
Much less filled→ Decreased wear resistance, increased shrinkage upon curing
NOWSilanated micro‐, micro‐hybrid, nano particles→ allows chemical adhesion, decreased wear, increased polishability.
Bulk cured up to 5mm→ elimina ng need for incremental curing
Much lower polymerization shrinkage
More shade options varying in translucency and opacity
Much more highly filled→ Used not only as bases but also universally in most restorative applications.
&
Overcoming Dentist Perceptions
No Post-op
sensitivity
Low film thickness
Cavity adaptation
Bulk fill w/ 3 year clinicals
Radiopaque
Low stress –reduced microleakage
Preferred Handling
Simplified Shading
Radiopaque
Dependable Cure
Smooth surface
One component
Dentsply SironaClass II Solution
Class II Success!Dependable.
Simple.Efficient.
Predictable Tight Contacts
Isolation
Less flash, less finishing
Direct Restoratives: The Class II Solution
Posterior Class I
Posterior Class II
Posterior Class V
Anterior Class III Facial
Anterior Class III Lingual
Anterior Class V
Anterior Class IV
Why Focus on Class II?
45%
22%
7%
7%6%
11%
3%
Source: American Dental Association
Good Local Anesthesia is VITAL!
Local Anesthesia
The Right Drug for the Right Procedure
Average Durations of Local Anesthesia after Intraoral Injection (mins)
Maxillary Infiltration Inferior Alveolar Block
Pulpal Soft Tissue PulpalSoft Tissue
2% Lidocaine w/ 1:100K or 1:50k epi 60 170 85 190
3% Mepivacaine 25 90 40 165
4% Prilocaine 20 105 55 190
4% Prilocaine w/ 1:200k epi 60 150 75 180
4% Articaine w/ 1:100k or 1:200k epi 60 170 90 220
0.5% Bupivacaine w/ 1:200k epi 40 340 240 440

8/3/2017
4
Local Anesthetic Maximum Dosages
Local Anesthetic Maximum Dose# of Carpules
Adult
# of Carpules
50 lb Child
Lidocaine w/ 1:100k epi (2%-36 mg)Lidocaine w/ 1:50k epiLidocaine w/o epi
3.3 mg/lb (500 mg) 3.3 mg/lb (500 mg)2.0 mg/lb (300 mg)
13.8*5.58.3
4.6NR2.8
Mepivacaine (3% - 54 mg)Mepivacaine (2% w/ 1:20k levo)
2.6 mg/lb (400 mg)7.411.1
2.53.7
Prilocaine plain (4% - 72 mg)Prilocaine w/ 1:200k epi
4.0 mg/lb (600 mg) 8.38.3
2.82.8
Bupivacaine (0.5% - 9mg) 0.6 mg/lb (90 mg) 10 NR
Articaine (4% - 72 mg) 3.3 mg/lb (500mg) 6.9 2.3
Dent Clin N Am 2010;54:587–599.*Maximum dose of epinephrine in healthy patients is 0.2mg, accounting for
epinephrine the maximum dose of lidocaine w/1:100k epi is 11 cartridges.
Dental Landscape
Composite Resins
In Today’s Dental Landscape……
• The most common direct composite procedure in dentistry is posterior amalgam replacement
• The average posterior composite lasts 6 years1
estimated annual failure rate of Class I and Class II posterior composites is 1‐3%2
• Cavity forms for many amalgam replacements and large carious lesions prove too time consuming to fill with vertical incremental layering
1 Journal of Dentistry 29 (2001) 317‐324.2 Dental Materials 2012; 28:87‐101.
In Today’s Dental Landscape……
• What does the future look like?
– “Bulk Fill” placement increment
– Simplified shading
– Fast polishing
– Stain resistance
No Post-op
sensitivity
Low film thickness
Cavity adaptation
Bulk fill w/ 3 year clinicals
Radiopaque
Low stress –reduced microleakage
Preferred Handling
Simplified Shading
Radiopaque
Dependable Cure
Smooth surface
One component
Dentsply SironaClass II Solution
Class II Success!Dependable.
Simple.Efficient.
Predictable Tight Contacts
Isolation
Less flash, less finishing
Oops!

8/3/2017
5
What are the Challenges facing the Dentist for a Class II?
• Isolation from the “hostile environment”
• Abrading the adjacent tooth during preparation
• Getting the band into place
• Sealing the gingival margin with the matrix band
• Sealing the line angles in the box
• Creating the ideal hybrid layer
• Proper light curing
• Achieving an “ideal contact”
• Adaptation of the material within the box
• Proper finishing and polishing
February 2014
Creating the “Ideal Contact” and Contour?
Nice looking restoration… until you look at the radiograph!
Incidence of damage done to the adjacent tooth during the preparation
procedure
100%

8/3/2017
6
• Accurate contacts/contours
Avoid food traps fractures and redos
• Tight marginal seal
less flash
less required finishing
• Procedure efficiency
multiple restorations at once
wedgeguard speeds up prep
Palodent Plus – Providing Tangible Solutions
Wedge guard
Performance Components
Protects adjacent tooth and soft tissue during preparation, pre‐expands contact, and metal guard can be removed and wedge left in place for
subsequent sectional matrix and Palodent Plus ring
Palodent Plus Wedge Guard Why use a Wedge Guard?
The ring can be used to generate separation and facilitate placement of the wedge guard and matrix, and
creation of tight contact!
Consider this case…

8/3/2017
7
Another case…
Wedge Guards are not impenetrable!

8/3/2017
8
Problem and Solution
Matrix Bands…Tofflemire vs. Sectional
Problem & SolutionTofflemire v. Sectional Matrices
Tofflemire System
Fails to restore proximal anatomy
Thin contact at the marginal ridge
Large food trap below
Increased likelihood of fracture, occlusalinterference, recurrent caries and periodontal disease
Sectional Matrices
Operator‐friendly retaining system
Naturally contoured bands
Anatomically correct contacts
Contacts at the height of contour
Contacts so tight you’ll need a hemostat to get the band out!
Palodent Plus Rings Clean Your Rings!
Palodent Plus Matrix

8/3/2017
9
Palodent Plus Pin Tweezers
Palodent Plus EZ Coat Matrices
‐ Same innovative features and benefits of the Palodent® Plus Matrices
‐ Micro‐thin, non‐stick finish to make matrix removal easier
‐ Greater matrix curvature to improve anatomical accuracy and avoid interference with the ring during placement
Active Wedging – Wood Wedges Passive Wedging – Wave Wedges

8/3/2017
10
Anatomic flexible “wedge” protects tissue and holds the band tightly against the tooth
Passive Wedging – Wave Wedges
Consider this example…
Pre‐operative view, caries #29‐distal
Pre‐operative view, caries #29‐distal Completed preparation, wedge guard in‐place

8/3/2017
11
Isolation of the prep with Palodent Plus, placement of Prime & Bond Elect Universal Adhesive The proximal box is filled with Surefil SDR flow
TPH3 is used to restore the occlusal 2mm of the preparation Oblique layers are used to avoid connecting walls, minimizing stress
The preparation has been filled and cured, prior to matrix removal Occlusal reduction and shaping with a fluted composite bur

8/3/2017
12
Finishing of the restoration with Enhance The completed restoration on tooth #29
What about an MOD restoration?
Consider this MOD example…

8/3/2017
13
Caries on #30‐mesial Completed prep with wedge guards in‐place
Isolation with rubber dam and Palodent Plus
Completed restoration
One more…

8/3/2017
14
#4‐MOD & #5‐MO Isolated with Palodent Plus
Final layer of composite light cured Final Restorations
There still may be times we need to use a
circumferential matrix…
There still may be times we need to use a Tofflemire…

8/3/2017
15
There still may be times we need to use a Tofflemire…
There still may be times we need to use a Tofflemire…
What about the Garrison System? What about the Garrison System?
Both systems are excellent and can be used to create great
results…

8/3/2017
16
Pre‐op Pre‐op
Rubber dam placed Prep isolated using Garrison system
Restored with Scotchbond Universal and Filtek Bulk Fill
Adhesives
Adhesives Market Data
• $121 Million market
• Market is split almost evenly between TE, SE, Univ
• In 2016, adhesive category was +2.5% according to latest data– Total etch ‐3.8%
– Self etch ‐2.4%
– Universal +15.8%
• New category of Universal Bonding Agents started in early 2011 (Optibond XTR → ScotchbondUniversal → Prime & Bond Elect)
SDM 2016

8/3/2017
17
• 60% of dentists use 2 or more adhesives
• Dentists are very divided on the impact of etchants and phosphoric acids on sensitivity
• 74% of clinicians will use phosphoric acid with self etch products…..expecting to improve clinical results!
• If we had to have a rule it would be…… “anterior applications require etching”
“etch enamel whenever you can”
SDM 2012
Adhesive User Information Evolution of Dental Adhesives
• 4th Generation Etch and Rinse Systems 3 Step‐Total Etch
• 5th Generation Total Etch 2 component‐Traditional
• 6th Generation‐ Self Etching 2 Bottle System
• 7th Generation Self Etching 1 Bottle System
• 7½th Generation??? Self‐Adhesive Flowables
Evolution of Dental Adhesives
• 4th Generation Etch and Rinse Systems 3 Step‐Total Etch
• 5th Generation Total Etch 2 component‐Traditional
• 6th Generation‐ Self Etching 2 Bottle System
• 7th Generation Self Etching 1 Bottle System
• Universal Dental Adhesives Total or Self Etch Options
Top Reasons for Post‐Operative Sensitivity
• Over‐etching dentin
• Over‐drying dentin
• Solvents not removed during drying step
• Incomplete material coverage
• Under curing (importance of lights)
• Polymerization shrinkage and stress (SDR)
Smear Layer
The Evolution of Dentin Adhesion Based on Treatment of the “Smear Layer” What is a “Smear Layer”
• Freshly cut surface of dentin created by rotary instruments
• Generally 1 – 5 microns thick, but extends into tubules in the form of amorphous “plugs” – “Biologic Band‐Aid”
• Smear layer components
– Hydroxyapatite crystals
– Partially denatured collagen
• Weakly attached to dentin surface (2‐6 mPa’s)
• Is partly porous, but dramatically reduces fluid flow from the underlying dentin tubules

8/3/2017
18
Total‐Etching Systems
Proper Total‐Etch Technique
Ambiphilic Primer or Primer/ Adhesive Combination
Smear Layer
Collagen “Noodles” embedded in dentinDentin Odontoblasts Tubule
After 15 Seconds…
Demineralizes hydroxyapatite and exposes collagen fibrils
Condition of Dentin After Preparation
Smear Layer and Demineralized Remnants Rinsed Away – Dentin
Left MOIST
Composite
“Hybrid Layer”
Hybrid Layer
Bonding area between the demineralized dentin… and the composite
Area where there is little to no “mineral” … only resin impregnated collagen
Composite
Intact Dentin
Over‐DryingDessicating the prep removes the moisture needed to properly suspend the delicate collagen
fibers.
Over‐DryingDessicating the prep removes the moisture needed to properly suspend the delicate collagen
fibers.
Effect of Etching Time on Dentin Demineralization
15 sec3-4 µm
30 sec
7-8 µm
Latta, M. Dean of Clinical Research, Creighton University, 2003
What about Enamel? Does it have to be DRY?
Am J Dent 2002; 15: 85‐90
• Our early adhesion training taught us to dessicate enamel –dry until we saw a “frosty” appearance
• This concept was essential prior to the creation of primers when only hydrophobic unfilled resins were available
• When primers followed by adhesive (4th Gen), primer/adhesive combination (5th Gen), or self‐etching systems (6th Gen) are used on enamel, Enamel can be “moist”

8/3/2017
19
Self‐Etching Systems
Self‐Etching Reaction
Self‐Etch Acidic Monomers – Scrub/agitate 10‐20 seconds
Smear Layer
Smear layer is “solubalized” into the adhesive and acidic monomers demineralize hydroxyapatite while simultaneously filling voids created with resin
Composite
• Etching, demineralization and infiltration of primers all occur simultaneously
• Smear layer and demineralized hydroxyapatitebecome incorporated into the bond
• Reaction is self‐limiting: The pH of the product is neutralized by dentinal Ca+
– pH of SEA approximately 2.5
– pH of phosphoric acid is < 1
Self‐Etching Reaction Importance of Air Drying
Evaporating the solvent is critical to maximizing the effectiveness of the
bonding agent
How difficult is it not to contaminate
Your working field?
Steady stream of oil‐ and moisture‐free air is applied until “rippling” motion ceases
Proper Evaporation of Solvents
Clinical Tip: Try to avoid aiming the air stream directing the into the preparation
Proper Evaporation of Solvents

8/3/2017
20
3 Distinct Mechanisms of Adhesion
Total‐Etch Self‐Etch
Selective‐EtchConcept has existed for years but
product robustness has been limiting factor
Viscosity of Etchant Gels
Caulk vs. Bisco Phosphoric Acid Conditioning Gel

8/3/2017
21
Preparation Classification & Technique
Class I Class II Class 3 Class IV Class V
Amount of available enamel, not the cavity classification is the primary determining factor in selecting application mode for the adhesive:
Total Etch, Self Etch or Selective Etching
Application of Phosphoric Acid Gel
Traditional application vs. Prime&Bond Elect
Enamel time vs. Dentin Time
How easy is it to selective etch?!? Etch enamel whenever you can!
`
The Importance of Light Curing

8/3/2017
22
Consequences of Improper Light Curing
• Insufficient polymerization adversely affects both physical and chemical properties of the restoration*– Inflammatory response
– Lower bond strengths
– More water sorption
– Weaker properties
– Microleakage
– Sensitivity
– Recurrent decay
*J Esthet Restor Dent 2010;22:86-103.
Light energy delivered lessens as distance of the material from the light tip increases
Light Performance over Distance
2mm
6mm
200
300
400
500
600
700
800
900
7mm 8mm 9mm 10mm
Output (m
W/cm
2)
Irradiance Over Distance 7‐10mm
SmartLite Focus
Radii
Bluephase Style
Demi Plus
Valo (Std Mode)
Elipar S10
SmartLite® Focus loses LESS energy over distance, making it more effective at delivering energy at clinically relevant
distances than many major competitors
Beam Collimation and Performance Over Distance
Collimated Not Collimated
Light energy delivered lessens as distance of the material from the light tip
increases
Light Performance over Distance
Curing Meter: Distance from the target makes a difference
There are hot and cold spots within the curing light tip, and they vary with every light.
Distribution of LEDs

8/3/2017
23
Beam Profile
The effective part of the light beam should be evenly distributed across the face of the light tip to maximize curing effectiveness, and minimize the
negative impact of operator technique.
Effect of Light Angle on Curing
undercured
Curing Light Tip
Clinical Tips for Light Curing
• Position the patient so you can access the tooth
• Stabilize with finger rests while curing
• Position as close to tooth as possible
• Position at right angle to the tooth/restoration
• Increase curing time for deeper preparations or darker shades
• Air cool or wait in between cycles
• Use orange shields so you can “look at the light”
• Keep light guide tip clean and free of debris
Light Curing Technique
Composite Resin
The Importance of Managing Shrinkage Stress

8/3/2017
24
Shrinkage vs. Stress
• Shrinkage is the process of volumetric contraction upon curing of the composite
• Stress is the force that the shrinking composite exerts on the surrounding tooth structure
• Stress = Modulus X Shrinkage
“shrinkage stresses are transferred to the surrounding tooth structure because the elastic modulus of tooth is
far greater than the restorative material”Materials Research 2010;13(3):381‐384.
To measure Shrinkage… Composite is cured unconstrained
To measure Shrinkage… Composite is cured unconstrained
Silanized Surface
Adhesive
Composite Resin
Tensiometer
To measure Stress… Composite is Always bonded
To measure Stress… Composite is Always bonded
Silanized Surface
Adhesive
Composite Resin
Stress
The resulting force is called Stress!!
Silanized Surface
Adhesive
Composite Resin
Stress

8/3/2017
25
If the stress is too high :Adhesive fracture may occur!
In extreme cases even tooth fractures!
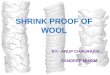
Schematic representation of the flowable composite increment (1) and wedge‐shaped increments (2‐7) used to build up dentin; two increments (8 and 9) are used to build up enamel using the successive cusp buildup technique. F: Facial
aspect. L: Lingual aspect.
Surefil SDR flow+ Bulk Fill Flowable
• Low‐stress resin matrix
• The low stress resin matrix and the moderately filled formulation decrease stress on the bond interface upon curing…
Even in 4mm increments!
• Can be used for bulk base placement in all posterior cavity forms
• MUST be covered with a durable hybrid composite in all stress bearing areas
• Introduced 2016
• Improved wear resistance
• Improved radiopacity (2.2 → 2.6 mm Al)
• Added indications: Class III and V
• No change in handling
Shrinkage Stress ComparisonDepth
of Cure
(mm)
Curing
Time (secs)
Filler (by
weight)
Filler (by
volume)
Shrinkage
(%)
Elastic
Modulus
(MPa)
Shrinkage
Stress
(mPA)
Fracture
Toughness
(MPa*m½)
Surefil SDR
Flow (Dentsply
Sirona)
4
20 (Univ)
40
(A1,A2,A3)
68% 45.1% 3.5 6335 1.6 2.18
Filltek Bulk Fill
(3M ESPE)4
40
(20
Universal)
64.5% 42.5% 3.4 4658 1.9 1.78
Venus Bulk
Flow (Heraeus
– Kulzer)
4 20 65% 38% 3.4 4080 2.0 2.01
X‐tra Base
(Voco)4
10
(Universal)
(20‐40 A2)
75% unknown 3.3 9330 2.9 1.44
Revolution Formula 2 (Kerr)
2 20 59% unknown 4.9 4500 3.2 1.38
Sonic‐fil (Kerr) 5 20/40 83.5% unknown 1.6 12900 2.5 unknown
Filtek Supreme
Ulta Flow (3m
ESPE)
2 20/40 65% 55% 4.2 6895 3.13 1.45
Esthet‐X Flow
(Dentsply
Sirona)
2 20 77% 60% 4.5 5622 3.2 1.5

8/3/2017
26
SonicFill™ (Kerr)
SDR resin is flowable and self‐levels within a couple of seconds after dispensing.
Flow Characteristics
Doctors report that they are using flowable composites to maximize material adaptation to the internal walls (pulpal) of the cavity preparation and to absorb shrinkage stress…….Concern for adaptation to the pulpal wall of
preparation but what about adaptation to axial walls?
Flow Characteristics
SureFil SDR flow EsthetX Flow
Doctors report that they are using flowable composites to maximize material adaptation to the internal walls (pulpal) of the cavity preparation and to absorb shrinkage stress…….Concern for adaptation to the pulpal wall of
preparation but what about adaptation to axial walls?
Radiopacity Radiopacity is important to
afford the clinician the opportunity to visualize the material radiographically
Radiolucent material is difficult to judge‐voids, open margins, recurrent decay!
** Look for 2.0+mm/al for excellent visualization**
Natural enamel= 2.0mm/alNatural dentin= 1.mm/al
Importance of Radiopacity RadiopacityDepth of Cure (mm) Radiopacity (mm Al)
Surefil SDR Flow+ (Dentsply Sirnona) 4 2.6
Filltek Bulk Fill (3M ESPE) 4 2.18
Venus Bulk Flow (Heraeus – Kulzer) 4 1.5
X‐tra Base (Voco) 4 2.2
Sonic‐fil (Kerr) 5 1.86
Filtek Supreme Ultra Flow (3M ESPE) 2 1.8
Esthet‐X Flow (Dentsply Sirona) 2 1.5
Dyract Flow (Dentsply Sirona) 2 2.0
Revolution Formula 2 (Kerr) 2 1.0
Grandio Flow (Voco) 2 1.0
Note: enamel = 2.0 mm Al, dentin = 1.0 mm Al

8/3/2017
27
Consider this example…
Surefil SDR flow
Pre‐operative radiograph showing needed RCT and restoration of tooth #4
Surefil SDR flow
Two Year Follow‐Up
SDR as cavity „floor sealer“
• SDR being used to seal the cavity floor (liner)
• Dentist decides which final restorations will be placed
• Easy re‐entry for post placement/core build‐up due to transparency of SDR

8/3/2017
28
Placement Time Comparison
4mm is not a rule!
Modify the amount of the Surefil SDR flowused to provide more opacity from the
hybrid composite and “mask out” the dark discolored dentin
4mm is not a rule!
Modify the amount of the Surefil SDR flowused to provide more opacity from the
hybrid composite and “mask out” the dark discolored dentin
Launched February 2013
What matters most?
• In real estate it is all about…
• In dentistry its all about…
HANDLING
LOCATION

8/3/2017
29
Composite Handling Challenges
• A sticky material will be difficult to manipulate and leave the doctor feeling like the material is not well adapted to the cavity preparation
• Compensate by wiping instruments with alcohol, dipping in adhesive or lubricant blocks, using titanium or plastic instruments
• Satisfies handling preferences of dentists– Dual viscosities (LV and HV)
• Simplified shading system– Chameleon effect of material‐shade
blending– Reduced inventory
• Improved durability of restorations– Excellent stain resistance– High Polish
Which do you like? Creamy or Packable?
Matching Instrument to Technique
Use existing anatomy to guide material placement
TPH Spectra‐Physical Properties Summary
TPH Spectra – technical data Value Unit
Fracture Toughness 1.69 MPa*m1/2
Flexural Strength (ISO 4049) 137 MPa
Flexural Modulus 9636 MPaCompressive Strength 351 MPaVolumetric Shrinkage 2.6 %Water Sorption (ISO 4049) 11.0 µg/mm3
Water Solubility (ISO 4049) 0.0 µg/mm3
Depth of Cure (A2, ISO 4049) 2.8 mm
Radiopacity (ISO 4049) 2.1 mm AlWork Time (ISO 4049) 68 secondFiller Content (weight / volume)
LV (75.5 / 54.6)HV (77.2 / 57.0)
%
Filler Size (average) pending µm

8/3/2017
30
Finishing and PolishingThe Importance of
Finishing and Polishing Composites
• Rough and reflective vs. smooth and shiny
• Adds to the longevity of the restoration
– Plaque and biofilm adherence
– Stain resistance
The Benefits of Enhance Finishers
• Can be used for both intermediate finishing and final finishing
• No damage to natural tooth structure
• Dissipates heat
• Comes in cups, points, and discs
One last case to wrap it all up…
Pre‐op, caries #29‐DO Finished Preparation Rubber Dam Isolation Enamel Etching

8/3/2017
31
After etching and rinsing Applying P&B elect adhesive Placing Surefil SDR flow Light curing for 20 seconds
Placing TPH Spectra LV (A2) After light curing for 20 seconds Finishing and pre‐polish with Enhance
Finishing and pre‐polish with Enhance Completed restoration on #29
Conclusions
• Despite frequency of directcomposite placement, successful completion of composite resins is tedious and technique sensitive
• Longevity of a direct composite restoration is related to the successful completion of all the steps discussed– Preparation, isolation, adhesion, composite placement, finishing, polishing
• Procedural solutions – using materials designed and intended to be used together to generate optimized clinical outcomes