Embed Size (px)
Citation preview

Subtyping Eating Disorders: Is It Justified?
DAVID B. HERZOG, M.D., ALISON E. FIELD, B.A., MARTIN B. KELLER, M.D., JENNIFER C. WEST, B.A.,
WENDI M. ROBBINS, A.B., JANET STALEY, B.A., AND GRAHAM A. COLDITZ, M.D., DR.P.H.
ABSTRACT
Objective: DSM-/V subtypes anorexia nervosa by the presence or absence of bulimic symptoms. Assessing whether
bulimic symptoms are related to the probability of recovery can provide justification for subtyping of anorexia. Method:
Two hundred twenty-five treatment-seeking women with anorexia and/or bulimia nervosa were interviewed every 3
months for up to 4 years. Survival methods were used for analyses. Results: Less than half of the entire cohort
recovered; however, the great majority of the women became less symptomatic over time. Contrary to findings from
previous studies, bulimic anorexics had a higher rate of recovery than restricting anorexics. Conclusion: Differences
in course provide some support for the subtyping of anorexia nervosa. Additional prospective studies are needed before
subtyping can be warranted. J. Am. Acad. Child Ado/esc. Psychiatry, 1996, 35(7):928-936. Key Words: anorexia
nervosa, bulimia nervosa, recovery.
The diagnostic criteria for anorexia nervosa (AN) andbulimia nervosa (BN) have changed three times in thepast 15 years, despite at times a lack of substantialempirical data to warrant revisions. On the basis ofthe findings that among treatment-seeking anorexics,patients presenting with bulimic symptoms are morelikely to suffer from comorbid depression, substanceabuse, a lack of impulse control, general emotionaldistress, and greater psychopathology and are morelikely to have a greater family history of affective
AcceptedJanuary 4, 1996.Dr. Herzog is Associate Proftssor of Psychiatry, Harvard Medical School,
and Director, Eating Disorders Unit, Massachusetts General Hospital, Boston.
Ms. Field is a doctoral candidate in the Department ofEpidemiology, Harvard
SchoolofPublic Health, Boston. Dr. Keller is Professor and Chair, Department
ofPsychiatry and Human Behavior, Brown University, Providence, RI. Ms.WestandMs. Robbins are ProjectCoordinators, andMs. Staley isBiostatistician,
Eating Disorders Unit, Massachusetts General Hospital. Dr. Colditz isAssociateProftssor ofMedicine, Harvard Medical School, Brigham and Women sHospital.
Thispaper waspresentedat the Societyfor EpidemiologicResearch, Snowbird,
UT, June 24, 1995.This project was supported in part by grants from the NIMH (R01
MH38333), the Rubenstein Foundation, Eli Lilly and Co., and The BostonObesity Nutrition Research Center (DK 42600). The authors thank Carrie
Wager, B.S., for her programming assistance, Karin Nussbaum, B.A., for herhelp in preparing this manuscript, and B. Timothy Walsh, M.D., KatharineLoeb, B.A., Michael Devlin, M.D., and Maurizio Faua, M.D., for their
reviews and imightful comments.Reprint requests to Dr. David B. Herzog, ACC 725, Massachusetts General
Hospital, 15 Parkman Street, Boston, MA 02114.
0890-8567/96/3507-0928$03.00/0©1996 by the American Academyof Child and Adolescent Psychiatry.
928
disorders, anxiety disorders, alcohol use, and obesitythan restricting anorexics (DaCosta and Halrni, 1992;Garfinkel et al., 1980; Garner et al., 1985, 1993;Halmi et al., 1991; Laessleet al., 1987, 1989; Mickalideand Anderson, 1985; Strober et al., 1982), the DSMIVsubtyped AN into restricting anorexics and bulimicanorexics (American Psychiatric Association, 1994).The DSM-IVTask Force on Eating Disorders, however,identified the need for more data on observed differences to justify subtyping. We can contribute to thiseffort by providing data on the course of illness fromthe Massachusetts General Hospital Longitudinal Studyof Anorexia and Bulimia Nervosa (MGH study). Theprospective comparison of the long-term course ofbulimic and restrictor anorexics can provide valuabledata regarding classification.
In 1987 we initiated a prospective, naturalistic studyof eating disorders in order to delineate the course ofAN and BN. The 225 women in the cohort areinterviewed at frequent intervals. The attrition rate isless than 6%. The sample was originally divided intosubgroups based on intake diagnoses of AN and BN.Subjects who met DSM-III-R criteria for both AN andBN within their intake eating disorder episode, andwhose AN and BN episodes were not separated by aremission ofeight or more weeks, were given a diagnosisof AN/BN. We recently reported recovery rates aftera minimum of 1 year of follow-up (Herzog et al.,1993). Only 10% of the ANs and 18% of the ANI
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:7, JULY 1996

BNs were able to achieve an asymptomatic state forat least eight consecutive weeks, compared to 56% ofthe BNs. To investigate the subtyping of AN andBN, subjects were regrouped into five separate eatingdisorder categories.We are reporting on 75 AN subjectsand 150 BN subjects followed for a mean of30 months.
Prior long-term studies of AN and BN have notfollowed subjects prospectively with frequent assessments (Herzog et al., 1988; Steinhausen et al., 1991).Instead, assessments have typically been made onlyonce, years after the patient was initially interviewed.Thus, there is limited information on the naturalcourse of illness; this information would be necessaryto determine true recovery rates and to empiricallydetermine the utility of the existing classificationscheme for eating disorders set forth in the DSM-IV(American Psychiatric Association, 1994). The designof the MGH study aimed to circumvent the limitationsof many of the previous outcome studies, such as longintervals between entry and follow-up, small samplesizes, and high attrition rates.
In this article, we assess the rates of recovery forrestrictor and bulimic anorexics to determine whetherbulimic behavior significantly affects the course of AN,and we assess possible subtypes of BN based on thepresence or absence of a history of AN. If ANs withbulimic symptoms are thought to have a more persistentand serious disorder than restrictor anorexics (DaCostaand Halmi, 1992; Hsu, 1988), then it seems plausiblethat BNs with subdiagnostic AN or a past history ofAN may constitute a particularly ill group and mayneed to be differentiated from bulimics without ahistory of AN; thus, we assess whether coexistingsubdiagnostic AN or a history of AN significantlyaffects the course of BN. We also assess whether.any of these subtypes differ on intake characteristics,including age at onset, age at presentation, durationofepisode, percentage ofideal body weight, and comorbidity rates.
METHOD
Sample
Five hundred fifty-four women were initially screened over thetelephone for entry into this longitudinal study of eating disorders.All participants had sought evaluation for an eating disorder atthe MGH Eating Disorders Unit and at other Boston-area eatingdisorder programs between October 1987 and June 1990. Allsubjects were required to meet DSM-III-R criteria for BN and/or
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 35:7. JULY 1996
SUBTYPING EATING DISORDERS
AN (using the 1983 Metropolitan Insurance Company norms asthe expected weight standards). Subject selection was independentof compliance with inpatient or outpatient treatment recommendations given at evaluation. Forty-eight percent (n = 268) of thewomen screened met criteria for AN and/or BN, and 229 (85%)of these 268 women agreed to participate in the study withreimbursement for their participation. This protocol was approvedby the MGH Institutional Review Board.
Ninety subjects who had mixed disorder (AN/BN) originallydiagnosed at intake into this study have been regrouped in thepresent analysis with the 41 anorexic and 98 bulimic subjects intofive separate eating disorder classifications: (l) subjects meetingfull criteria for AN who do not regularly engage in binge eatingor purging behavior (AN.R, n = 39); (2) subjects meeting fullcriteria for AN who regularly engage in either binge eating orpurging behavior (purging being defined by either self-inducedvomiting or the misuse of laxatives or diuretics) (AN.BP, n = 37);(3) subjects meeting full criteria for BN who have a prior historyof AN (BN.PAN, n = 28); (4) subjects meeting full criteria forBN who are underweight at intake but do not meet full criteriafor AN (BN.SAN, n = 36); and (5) subjects meeting full criteriafor BN who have no prior history of AN (BN, n = 89). Subjectsmeeting full criteria for both AN and BN have been placed in anAN subgroup (AN.BP), reflecting the hierarchy set forth in DSMIV (American Psychiatric Association, 1994). Four subjects (oneAN.BP, one BN.PAN, and two BN.SAN) dropped out of thestudy prior to the first follow-up interview; thus 225 womenremained for analysis.
Procedure
The intake and follow-up procedures of this study have beendescribed in detail in previous reports (Herzog et al., 1993). Tobriefly summarize, a semistructured interview was used at intaketo ascertain the current and lifetime psychiatric histories of allwomen. Follow-up interviews have been conducted every 3 monthsby trained clinical interviewers (see Herzog et al., 1992a, for adescription of training procedures). Anniversary (e.g., 12, 24, 36month) follow-ups have been conducted in person wheneverpossible.
Our study is naturalistic (i.e., not assigning or sampling ontreatment) and does not control for treatment in the analyses;however, nearly all of our subjects have received one or more formsof treatment at some point during the follow-up time. Our reasonsfor choosing a naturalistic design are described elsewhere (Herzoget al., 1985, 1992b).
Instruments
Subjects' lifetime Axis I psychiatric histories were assessed witha version of the Schedule for AffectiveDisorders and SchizophreniaLifetime Version (SADS-L) (Spitzer and Endicott, 1979) thatwas modified to include diagnostic criteria for DSM-III-R eatingdisorders (EAT SADS-L). The section on eating disorders wasderived from the Diagnostic Interview Schedule (Robins et al.,1981). The 1983 Metropolitan Insurance Company height andweight norms (Metropolitan Life Insurance Company, 1983) wereused to calculate the subjects' percentage of ideal body weight.Psychosocialfunctioning was assessed with the Longitudinal IntervalFollow-up Evaluation-Baseline Version (LIFE Base) (Keller andShapiro, 1979). Axis II disorders were assessed in all subjects 18 yearsor older using the Structured Interview for DSM-III PersonalityDisorders (Pfohl et al., 1982).
929

HERZOG ET AL.
Follow-up assessments used the semistructured Eating DisordersLongitudinal Follow-up Evaluation (LIFE-EAT-II), a modifiedversion of the LIFE II (Keller et al., 1987). The LIFE-EAT-II,which has been described in detail in a previous article (Herzoget al., 1992a), was designed for collecting longitudinal data oneating disorders, Research Diagnostic Criteria (RDC) (Spitzer et al.,1985) comorbid diagnoses, treatment participation, and psychosocial functioning.
Information on Axis I psychopathology is recorded by meansof the Psychiatric Status Rating (PSR) scale, an ordinal, symptombased scale (see Herzog et al., 1993, for a description and outlineof PSR scales). PSR scores range from 1 to 6. Scores greater than4 indicate that an individual meets full criteria for a disorder andscores less than 3 indicate that an individual is asymptomatic. Atevery follow-up, PSRs are rated for all disorders which were currentat intake or which have developed at any point after intake. Oncea diagnosis is made, the disorder is given a PSR for each week ofevery succeeding follow-up. In addition to overall AN and BNPSRs, the presence or absence of each eating disorder symptomand the level of severity of key eating disorder symptoms (for AN,weight; for BN, binging frequency) are assessed week by week.Although ratings for compulsive exercising and restrictive eatingare not incorporated into the overall AN and BN PSRs, they arerecorded weekly because they are valuable descriptors of associatedpsychopathology commonly observed among individuals witheating disorders.
Definition of Recovery
We have defined full recovery from an eating disorder as remaining asymptomatic (having a PSR less than 3) for at least eightconsecutive weeks. The 2-month requirement is based on the RDC(Spitzer et al., 1985) criteria for recovery from a depressive episode.Partial recovery is defined as maintaining for at least eight consecutive weeks a PSR level of 3 or 4. Partially recovered subjects arethose who do not meet full criteria for AN or BN, yet who maystill experience significant symptomatology.
Statistical Methods
Baseline differences between the subtypes, including age at onset,age at intake, duration of episode, percentage of ideal body weightat intake, and intake comorbidity rates (Axis I disorder, Axis IIdisorder, affective disorder, suicide attempt, disorder involvingimpulse control [drug use, alcohol abuse, kleptomania]), were testedwith Fisher's Exact Test (for dichotomous variables) and WilcoxonRank Sum Test (for continuous variables). The Kaplan-Meiersurvival method was used to estimate the cumulative probabilityof recovery, starting at time of intake.
Cox proportional hazards models were used to identify prognosticfactors. To consider the predictiveness of the individual diagnosticcriteria, the sample was stratified by intake diagnosis (AN versusBN), and models were run on the stratified samples. Covariatesconsidered as prognostic factors include age at onset of first eatingdisorder episode, age at onset of intake eating disorder episode,age at intake into the study, duration of intake episode, time sinceonset of first eating disorder, any current Axis I disorder, currentdepression, lifetime history of any Axis II disorder, current disorderinvolving impulse control (kleptomania, drug use, alcohol abuse,or suicide attempt), history of attempted suicide, past history ofAN (only for bulimic subjects), and percentage of ideal bodyweight. Duration of intake episode was included in all models
930
because conceptually the starting point of follow-up should be thetime of onset of the episode, not enrollment into the study.
All analyses (Fisher's Exact Tests, Wilcoxon Rank Sum Tests,Kaplan-Meier methods, and Cox proportional hazards models)were conducted using Splus software (Becker et al., 1988).
RESULTS
Baseline Characteristics
The mean age of the sample at intake was 24.5(±6.7 years), ranging from 13 to 45 years (Table 1).Episode duration across the sample ranged from 3months to more than 10 years, with a mean durationof79 (±74) months. There were high levels of currentand past psychiatric comorbidity for all eating disorder groups.
There were no significant baseline differences between the AN.R and AN.BP groups; however, therewere several differences between the bulimic subgroups.BN.SANs had been bulimic for significantly longerthan either the BNs (median = 74 months versusmedian = 39 months; Wilcoxon p < .05) or theBN.PANs (median = 32; Wilcoxon p < .05). MoreBN.SANs (59%) had a disorder involving impulsecontrol (kleptomania, drug use, alcohol abuse, or suicide attempt) than BNs (31%; Fisher's exact p < .001)and BN.PANs (22%; Fisher's exact p < .00l). Inaddition, BN.SANs were also significantly more likelyto have a diagnosis of a personality disorder than werethe BNs (41% versus 16%; Fisher's exact p < .001).
Recovery
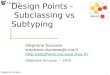
Full recoverywas more common among the bulimicsthan among the anorexics (Table 2). As can be seenin Figure 1, in contrast to all three bulimic subtypes,recovery occurred only early in the follow-up amongthe anorexics. Dividing the sample into five subtypesbased on the degree of anorexia, with pure restrictorAN on one end of the spectrum, underweight BN inthe middle, and pure BN on the other end, we foundthat recovery was inversely related to the degree of AN(p for trend < .00l). The percentage of women whofully recovered ranged from 8% among AN.Rs to 62%among pure bulimics (without a history of anorexia).Moreover, intake diagnosis was the strongest predictorof recovery. AN.BPs were more likely to fully recoverthan were AN.Rs (relative risk [RR] = 4.6, 95% confidence interval [CI] 0.98 to 21.9). Moreover, BN.SANs
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:7, JULY 1996

SUBTYPING EATING DISORDERS
TABLE 1Baseline Characteristics of 225 Treatment-Seeking Women with an Eating Disorder
AN.R AN.BP BN.SAN BN.PAN BN(n = 39) (n = 36) (n = 34) (n = 27) (n = 89)
Age (yr)" 21 (18-27) 22 (19-25) 25 (21-29) 23 (20-27) 24 (20-30)Age at onset of first
disorder (yr)" 17 (15-20) 17 (15-19) 17 (14-19) 16 (15-18) 18 (16-20)Time since onset of
current episode(rno)" 27 (10-99) 58 (23-109) 74 (29-120)* 32 (9-100) 39 (12-81)
% of ideal bodyweight" 73 (63-81) 76 (70-81) 87 (84-88) 100 (93-110) 100 (96-110)
% with any currentAxis I diagnosis 59 67 65 70 64
% with a current af-fective disorder 49 58 47 48 53
% with a person-ality disorder 21 33 41** 30 16
% who have at-tempted suicide 18 33 53*** 19 28
% with current dis-order involvingimpulse control" 31 39 59**'*** 22 31
Note: AN.R = subjects meeting full criteria for anorexia nervosa (AN) who do not regularly engage in binge eating orpurging behavior; AN.BP = subjects meeting full criteria for AN who regularly engage in either binge eating or purgingbehavior; BN.SAN = subjects meeting full criteria for bulimia nervosa (BN) who are underweight at intake but do notmeet full criteria for AN; BN.PAN = subjects meeting full criteria for BN who have a prior history of AN; BN = subjectsmeeting full criteria for BN who have no prior history of AN.
a Median (25th and 75th percentiles).b Kleptomania, substance use disorder, suicide attempt.*P < .05 for BN versus BN.SAN; **P ::; .001 for BN versus BN.SAN; *** P ::; .001 for BN.PAN versus BN.SAN.
were less likely to fully recover than were BNs (RR =
0.65, 95% CI 0.36 to 1.16), though the differencewas not significant. The majority of subjects in allsubgroups achieved at least partial recovery, rangingfrom 54% of the AN.Rs to 91% of the BNs.
Because full recovery was uncommon among theANs and becausemostAN.BPs engaged in both bingingand purging behavior, we were unable to assess the
TABLE 2Rates of Recovery
AN.R AN.BP BN.SAN BN.PAN BN(n = 39) (n = 36) (n = 34) (n = 27) (n = 89)
% at leastpartiallyrecovered 54 81 85 81 91
% fullyrecovered 8 17 44 59 62
Note: Eating disorder subtypes are defined in the first footnoteto Table 1.
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:7, JULY 1996
independent predictiveness of binging and purging.Among anorexics, but not bulimics, the duration ofthe intake episode was inverselyassociatedwith recovery(Table 3). For every 2 years that an anorexic had beenill prior to intake, her probability of recovery, afteradjusting for bulimic behaviors, decreased by approximately 50% (RR = 0.50, 95% CI 0.27 to 0.94).Comorbid Axis I and Axis II disorders were not associated with recovery, nor was age at onset of the currentdisorder, age at onset of the first disorder, or engagingin impulse-related behaviors (kleptomania, suicide attempts, and drug abuse).
DISCUSSION
We observed high rates of partial recovery in bothAN subgroups; however, only a small percentage ofANs fully recovered. Approximately 8% of the AN.Rsand 17% of the AN .BPs were able to remain asymptomatic for at least 8 weeks. The bulimic women had
931

H ERZO G ET AL.
a significantly better outcome than the anorexics. Fiftyseven percent of the BNs were able to remain asymptomatic for at least 8 weeks.
Despite the paucity of research on the validity ofsubryping, Garner et al. (1985) and DaCosta andHalmi (1992) have argued that the existing data suppottconsidering restrictor and bulimic anorexia separatelybecause of differences in comorb idity and family history(Garfinkel et al., 1980; Garner et al., 1985, 1993;Halm i et al., 1991; Laessle et al., 1987, 1989; Mickalideand Anderson, 1985; Strober et al., 1982). In addition,Kaye et al. (1984) reported differences in brain serotonergic metabolism between bulimic and restrictor ANs.Some studies have reported a longer duration of illnessand an older age at onset of the disorder amongAN.BPs (Vandereycken and Pierloot, 1983; Viesselmanand Roig, 1985). These two factors are importantpotential confounders because they might independently predict outcome. Unfortunately, the majority of
the studies cited above are based on single-follow-updata; thus it cannot be inferred from the data thatthe observed differences persist over time or predictoutcome . Contrary to expectations, we found no differences in intake characteristics between the AN.Rs andthe AN.BPs, such as age, duration of episode, percentage of ideal body weight, and comorbidity rates.
There have been numerous follow-up studies of ANpatients, with length of follow-up ranging from 35days to 22 years. Among the studies with 2 to 5 yearsof follow-up, reported recovery rates range from 22%to 68% and mortality rates range from 0% to 15%(Martin, 1985; Morgan and Russell, 1975; Nussbaumet al., 1985; Seidensticker and Tzagournis, 1968; Touyzand Beaumont, 1984). Despite the abundance of follow-up studies of AN patients, data are lacking onfactors that affect the likelihood of recovery.The factorsmost consistently found to be associated with outcomeare age at onset (or referral) (Bryant-Waugh et al.,
eo AN_BPc:i
o'iiiE0aE co>. c:i(/)
Clc:'c'iiiE~ -.:tc: c:i0t0a.e BNa.
C\lc:i
oc:i
o 50 100 150 200 250
wee ks since intake
Fig. 1 Probability of remaining symptomatic among five eating disorder subtypes. The lines are the diagnosis-specific Kaplan-Meier estimates of survival(i.e., remaining symptomatic). Recovery was defined as being asymptomatic for eight consecutive weeks. AN.R = subjects meeting full criteria for anorexianervosa (AN) who do not regularly engage in binge eating or purging behavior (n = 39); AN.BP = subjects meeting full criteria for AN who regularlyengage in either binge eating or purging behavior (purging being defined by either self-induced vomiting or the misuse of laxatives or diuretics) (n = 37);BN.SAN =subjects meeting full criteria for bulimia nervosa (BN) who are underweight at intake but do not meet full criteria for AN (n =36); BN.PAN =women meeting full criteria for BN who have a prior history of AN (n = 28); BN = subjects meeting full criteria for BN who have no prior history ofAN (n = 89).
932 J . AM. ACAD. CHILD ADOL ESC. PSYCHI AT RY, 35 :7 , JUL Y 1996

SUBTYPING EATING DISORDERS
TABLE 3Predictors of Recovery from an Eating Disorder among 225 Treatment-Seeking Women
BN (n = 150) AN (n = 75)
Unadjusted Adjusted" Unadjusted Adjusted"
RR CI RR CI RR CI RR CI
Duration of currentepisode" 0.96 0.91-1.07 0.98' 0.91-1.07 0.59 0.32-1.07 0.50' 0.27-0.94
Age at onset ofeating disorder 1.00 0.96-1.04 1.00 0.95-1.04 1.02 0.94-1.1 I 1.01 0.92-1.09
Age at onset of firsteating disorder 0.98 0.93-1.03 0.98 0.93-1.03 1.03 0.95-1.12 1.01 0.95-1.09
Current disordersinvolving a lack ofimpulse control 0.98 0.62-1.54 0.98 0.62-1.54 0.83 0.20-3.42 1.14 0.28-4.74
Bulimic behaviors" NA NA 2.37 0.59-9.55 4.63 0.98-21.9Weight <90% of
ideal 0.71 0.41-1.23 0.71 0.41-1.25 NA NABinging frequency 0.97 0.93-1.02 0.97 0.93-1.02Purging frequency 0.96 0.92-1.01 0.96 0.92-1.01Current depression 1.15 0.75-1.76 1.15 0.75-1.76 3.56 0.73-17.3 3.57 0.74-17.2Personality disorder 0.92 0.55-1.54 0.94 0.56-1.57 J' J'
Any current Axis Idisorder 1.26 0.80-1.99 1.27 0.80-2.00 2.11 0.44-10.2 2.49 0.52-12.0
Note: Relative risks (RR) and 95% confidence intervals (CI) from univariate and multivariate Cox proportional hazards models. Eightyfive of the bulimics and nine of the anorexics recovered during the study. Eating disorder subtypes are defined in the first footnote toTable 1. NA = not applicable.
a Adjusted for duration of the current episode.b Time from onset of the current episode to enrollment in the study.'Adjusted for overlap between anorexia and bulimia (i.e., AN.R versus AN.BP, BN versus BN.PAN versus BN.SAN).d Comparing restrictor anorexics (AN.R) to bulimic anorexics (AN.BP).'Too few subjects to assess independent predictiveness of frequency of binging and purging.J'No anorexics with an Axis II disorder recovered; thus the relative risk cannot be estimated.
1988; Hall et al., 1984; Ratnasuriya et al., 1991;Sohlberg et al., 1989), percentage of desirable weight(Herzog et al., 1993; Hsu, 1988), and duration ofillness (DaCosta and Halmi, 1992). In addition, somefollow-up studies have reported that binge eating (Hsuet al., 1979) and vomiting (DaCosta and Halmi, 1992;Halmi et al., 1973; Ratnasuriya et al., 1991; Seidensticker and Tzagournis, 1968; Steinhausen et al., 1991;Steinhausen and Glanville, 1983; Tolstrup et al., 1985)are associated with a poor outcome, although othershave not found them to be predictive (Morgan et al.,1983; Nussbaum et al., 1985; Santonastaso et al.,1987; Sohlberg et al., 1989). Due to the small samplesizes in most of these srudies, the authors were unableto control for confounding factors, such as age at onsetand duration of illness.
Eckert et al. (1987) directly assessed whether differences between bulimic and restrictor ANs persistedover time. They found that bulimic ANs presentedwith more psychopathology; however, after controlling
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:7. JULY 1996
for treatment and weight at presentation, they foundno difference in outcome between restrictor and bulimicANs. Although these results suggest that AN shouldnot be subryped, the authors followed the subjects foronly 35 days after treatment. To make decisions aboutsubtyping, longer follow-up is clearly necessary.
Contrary to the findings based on single-follow-updata, our large-scale, prospective, naturalistic studyfound that AN.Rs were less likely to recover than wereAN.BPs. The proportion of women who recovered inthis study should be interpreted in light of findingsreported by other studies. However, methodologicallimitations of many of the studies, such as long intervalsbetween entry and follow-up, small sample sizes, univariate analyses which ignore baseline differences in thesamples (such as age at intake, age at onset of illness,and duration of illness), high attrition rates, and crosssectional or retrospective study designs, make comparisons difficult. Moreover, the definition of recoveryfrom AN that we used is more stringent than the
933

HERZOG ET AL.
Morgan-Russell general outcome criteria (Morgan andRussell, 1975) used in many studies. A good outcomeaccording to the Morgan-Russell criteria is regularmenstruation and body weight within 15% of averagebody weight. We have employed a lesslenient definitionof recovered weight (within 5% of ideal body weight),as well as regular menstruation, as necessary criteriafor recovery. Since we used a stricter definition ofrecovery, our observed recovery rates are lower thanmany of the studies using the Morgan-Russell criteria.Studies with 2 to 6 years of follow-up, using theMorgan-Russell criteria, report that 25% to 67%achieve a good outcome (Gillberg et al., 1994; Hsuet al., 1979; Kohle and Mall, 1983; Morgan er al.,1983; Stuttzenberger et al., 1977). Further follow-upwill enable us to see whether long-term course berweenthe subtypes differs and will allow us to make meaningful comparisons with other outcome srudies.
Fifty-seven percent of the bulimics in our sampleachieved a full recovery. However, comparing resultsof outcome studies of BN is also problematic. Definitions of outcome used in studies of BN are diverse,reflecting the lack of agreement among eating disorderresearchers in outcome terminology. Thus, some outcome studies of BN define recovery as no binging orpurging in the 6 months prior to follow-up (Hsuand Sobkiewicz, 1989), while other studies consider asubject who binges and putges monthly as fully recovered (Abraham et al., 1983; Swift et al., 1987). Furthermore, the diagnostic criteria for BN under DSM-IIIwere much less stringent than the more recent DSMIII-R and DSM-IV criteria (Lancelot et al., 1991).
Our definition of recovery, abstinence from bingingand purging for at least eight consecutive weeks, as wellas the diagnostic criteria (DSM-III-R) we employed, aremore stringent than those used in many studies. Thusour observed recovery rates for BN are in the low-tomiddle end of the range reported in the literature ,13% to 69% (Abraham et al., 1983; Fallon er al.,1991; Fichter et al. , 1992; Hsu and Holder, 1986;Keller et al., 1992; Lancelot et al., 1991; Mitchellet al., 1989; Swift et al., 1987).
Our finding that BN.SANs experienced more psychopathology at intake but had a similar age at onsetand similar binge-eating frequency as the BNs withouta history ofAN is consistent with the literature (Garfinkel et al., 1980; Garner et al., 1985; Herzog et al.,1992a; Johnson-Sabine et al., 1992; Mickalide and
934
Anderson, 1985; Mitchell et al., 1990). Moreover, ourresults are compatible with those ofFallon et al. (1991),Hsu and Holder (1986), and Johnson-Sabine et al.(1992), who have observed that a self-reported historyof AN does not predict outcome of BN. However,bulimics who were currently underweight were lesslikely to recover, though the difference was not significant. Thus our results are consistent with those ofFichter et al. (1992), whose study of inpatient bulimicsfound that low weight at intake was predictive of apoor outcome 2 years later. Further follow-up willenable us to determine whether long-term course differentiates the bulimic subgroups.
Several limitations of this study should be noted.This study is not a random sample of all women witheating disorders. All subjects were treatment-seekingwomen who met full DSM-III-R criteria for an eatingdisorder. Our AN cohort consists of a relatively smallnumber of subjects, particularly after subtyping intorestrictor (AN.R) and bulimic (AN.BP) subgroups. Tocompare baseline differences, such as duration of illnessand presence of a comorbid disorder, we used exactand nonparametric tests which are the most powerfultests with sparse and nonnormally distributed data.We had considerably less power to identify predictorsof recovery among anorexics since not only was thesample small, but also recovery was rare and multivariate exact methods were not available.
After subryping bulimia (n = 150), we had similarpower issues. We subdivided the sample into thosebulimics with subthreshold AN (BN.SAN), a pasthistory ofAN (BN.PAN), and no history of AN (BN)to test whether subtyping was warranted. As a resultof subtyping anorexics and bulimics and the low recovery rate among anorexics, our confidence intervals arewide. When interpreting the predictors of recovery itis essential to use confidence intervals instead of Pvalues. We have reported the 95% confidence intervalswhere the risk appeared to be elevated, but unstable(i.e., association berween AN subtype and time torecovery: RR = 4.6, 95% CI 0.98 to 21.9) . If wesimply reported predictors of recovery as significant(p < .05) or not significant (p ;::: .05), readers wouldbe unable to differentiate the above result from onethat appears to be truly null (i.e., association berweenage at onset of eating disorder and time to recoveryfrom BN in our study: RR = 1.0, 95% CI 0.95 to 1.04).
J . AM . ACAD. CHILD ADOLESC. PSYCHIATRY, 35 :7. JULY 1996

A multiphase method for validating psychiatric illness has been proposed by Robins and Guze (1970).We have chosen to focus on the outcome of thesubtypes of AN and BN in order to evaluate thejustification for subryping. Some investigators havenoted an improved outcome among restrictor anorexicscompared with bulimic anorexics and have found thatcomorbidity, family histories, and neurobiological characteristics between restricting and bulimic anorexicsdiffered (Garfinkel et al., 1980; Garner et al., 1985,1993; Halmi et al., 1991; Kaye et al., 1984; Laessleet al., 1987, 1989; Mickalide and Anderson, 1985;Strober et al., 1982). Our unexpected finding thatbulimic anorexics had a better recovery rate than restrictive anorexics in this large-scale, prospective study usingstate-of-the-art methodology provides some support forthe subtyping of AN. The outcome studies whichfound that bulimic anorexics have a worse outcomethan restricting anorexics differed from our study inat least one of several ways: they were retrospective,used hospitalized populations, had longer follow-updurations, and/or did not follow their samples at frequent intervals. Although recovery was uncommonamong both subtypes of anorexia, our data on coursemay lend support to the subtyping of anorexia intorestricting and bulimic anorexia. Nevertheless, the decision to subtype should not be based on the results of anyone study. Our finding of similar rates of comorbiditybetween the two anorexic subgroups, which is contraryto findings of other studies, also speaks to the needfor additional studies comparing the recovery and comorbidity rates of these subtypes. Replication of ourfindings in other prospective studies of both hospitalized and nonhospitalized eating-disordered women areneeded before it would be prudent to make any finaldecisions regarding the utility of subtyping anorexia.
The DSM-IVTask Force considered subtyping BNby a history of AN for those individuals who hadpreviously had AN and then had become normalweight bulimics but concluded that data on this subgroup were lacking (Wilson and Walsh, 1991). However, it was decided that there were substantial datato support the subclassification of BN by the presenceof purging behaviors (vomiting and using laxatives).Due to the insufficient number of nonpurging BNsin our sample (n = 11), we were unable to examinethe course and outcome for these two subgroups. Thelow number of nonpurging bulimics in our large sample
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 35:7, JULY 1996
SUBTYPING EATING DISORDERS
of consecutive treatment-seeking women with eatingdisorders suggests that this subtype may be an uncommon treatment-seeking subgroup and that other subtypes should be considered in the classification of BN.Our longitudinal study allows for a description ofbulimics who have previously experienced AN or whoare currently underweight, and we chose to examinecourse and outcome in these subgroups. Our findingssuggest that AN symptomatology may have a negativeeffect on the course ofBN, as we observed that bulimicswith a low weight at intake had a lower rate of recovery.The finding that full recovery was more commonamong the bulimics than the anorexics may also inpart reflect our definition of recovery, as well as thecurrent state of therapeutic knowledge. From a clinicalperspective, bulimics tend to relapse intermittentlywhile anorexics tend to experience a sustained patternof pathology, as well as recovery.
Future research should focus on mapping a moreaccurate and comprehensive picture of the course ofAN and BN. Essential to this effort is the developmentof more accurate, and universally accepted, definitionsof outcome. Such information on course and outcomecan contribute to the classification of eating disorders,improve the design of research protocols on treatment,and increase patient and public education about ANand BN.
REFERENCES
Abraham SF, Mira M, Llewellyn-Jones D (1983), Bulimia: a study ofoutcome. Int J Eat Disord2:175-180
American Psychiatric Association (1994), Diagnostic and Statistical ManualofMental Disorders, 4th edition (DSM-lV). Washington, DC: AmericanPsychiatric Association
Becker R, Chambers J, Wilks A (1988), The New S Language. PacificGrove, CA: Wadsworth and Brooks/Cole Advanced Books and Software
Bryant-Waugh R, Knibbs J, Fosson A, Kaminski Z, Lask B (1988), Longterm follow-up of patients with early-onset anorexia nervosa. Arch DisChild 63:5-9
DaCosta M, Halmi KA (1992), Classification of anorexia nervosa: questionof subrypes. Int J Eat Disord 11:305-313
Eckert ED, Halmi KA, Marchi P, Cohen J (1987), Comparison of bulimicand non-bulimic anorexia nervosa patients during treatment. PsycholMed 17:891-898
Fallon BA, Walsh BT, Sadik C, Saoud JB, Lukasis V (1991), Outcomeand clinical course in inpatient bulimic women: a 2-9 year follow-upstudy. J Clin Psychiatry 52:272-278
Fichter MM, Quadflieg N, Rief W (1992), The German longitudinalbulimia study. In: The Course ofEating Disorders: Long-Term Followup Studies ofAnorexia and Bulimia Neruosa, Herzog W, Deter HC,Vandereycken W, eds. Berlin, Heidelberg, New York: Springer-Verlag,pp 133-149
Garfinkel PE, Moldofsky H, Garner DM (1980), The heterogeneiry ofanorexia nervosa: bulimia as a distinct subgroup. Arch Gen Psychiatry37:1036-1040
935

H ERZ O G ET AL.
Gar ner DM, Garfinkel PE, O 'Shaughne ssy M (1985), The validity of thedistinction between bulimia with and without anorexia nervosa. Am JPsychiatry 142:581-587
Garner DM, Garner MV, Rosen LW (1993), Anorexia nervosa "restrictors"who purg e: implications for subryping anorexia nervosa. Int J EatDisord 13:171-186
Gillbe rg IC, Rastam M, Gillberg C (1994), Anore xia nervosa out comes:six-year controlled longitudinal study of 51 cases including a popul ationcohort . JAm Acad Child Adolesc Psychiatry 33:729- 739
Hall A, Slim E, Hawker F, Salmond C (1984) , Anorexia nervosa: longterm Outcome in 50 female patients. BrJ Psychiatry 145:407-413
Halmi KA, Brodland G, Loney J (1973). Prognosis in anorexia nervosa.Ann Intern Med 78:907-909
Halmi KA, Eckert E, Mar chi P, Sampingaro V, Apple R, Cohen J (199 1),Comorbidity of psychiatr ic diagnosis in ano rexia nervosa. Arch GenPsychiatry 48:712-718
Herzog DB, Keller MB, Lavori PW (1988 ), Outcome in anorexia nervosaand bulimia nervosa. J Neru Ment Dis 176:131-143
H erzog DB , Keller MB, Sacks NR, Yeh q , Lavori PW (1992a), Psychiatriccomorbidiry in treatment-seeking anor exics and bulimics. JAm AcadChildAdolesc Psychiatry 31:810-818
Herzog DB, Keller MB , Strob er M, Yeh C, Pai S (l992b), The currentstatus of treatment for anorexia nervosa and bulim ia nervosa. Int J EatDisord 12:215-220
Herzo g DB, Pepose M, Norman DK, Rigoni NA (1985), Eating disorde rsand social maladjustment in female medical students. J Nero MentDis 173:734-737
H erzog DB, Sacks NR, Keller MB, Lavoti PW, von Ranson KB, GrayHM (1993), Patterns and predic tors of recovety in anor exic and bulimicwomen. JAm Acad Child Adalesc Psychiatry 32:835- 842
Hsu LKG (1988), The out come of anorexia nervosa: a reappr aisal. Psycho!Med 18:807-812
Hsu LKG , Crisp AH , H arding B (1979), Outcome in anorexia nervosa.Lancet 2:61-65
Hsu LKG, Holder D (1986), Bulimia nervosa: treatment and short-termoutcome . Psycho!Med 16:65-70
Hsu LKG, Sobkiewicz TA (1989), Bulimia nervosa: a four-to-six yearstudy. Psycho! Med 19:1035-1038
Johnson-Sab ine E, Reiss D , Dayson D (1992) , Bulimia nervosa: a 5-yearfollow-up study. Psycho!Med 22:951-959
Kaye WH, Ebert MH, Gwirtsman HE , W eiss SR (1984) , Differences inbrain serotonergic metabolism between nonbulimic and bulimi c patien tswith anorexia nervosa. Am J Psychiatry 141:1598-1601
Keller MB, Herzog DB, Lavori PW , Ott IL, Bradburn IS, Mahoney EM(1992), The natural history of bulimia nervosa: extraordinarily highrates of chronicity, relapse, recurren ce, and psychosocial morbidity. IntJ Eat Disord 12:1-9
Keller MB, Lavori PW, Freidman B et al. (1987), The Longitudinal IntervalFollow-up Evaluation. Arch Gen Psychiatry 44:540- 548
Keller MB , Shapiro RW (1979), U FE Base Schedule. Boston : Massachu settsGeneral Hospital
Kohle K, Mall H (1983), Follow-up study of 36 ano rexia nervosa patientstreated on an integrat ed inrernistic-psychosomatic ward. Int J EatDisord 2:215-219
Laessle RD, !Gtrl S, Gitchter MM, Wi ttchen HU, Pirke KM (1987),Majo r affective disorder in anorexia and bulim ia: a descriptive diagnosticstudy. Br J Psychiatry 151:785-789
Laessle RG, Wittchen HU, Fichter M M, Pirke KM (1989), The significanceof subgroups of anorexia nervosa: lifetime frequency of psychiatri cdisorders. Int J Eat Disord8:569-574
Lancelot C , Brooks-GunnJ, Warren MP , Newman DL (199 1), Comparisonof DSM-III and DSM-III-R bulimia nervosa classification for psychopatholo gy and other eating disorders. lnt J Eat Disord10:57-66
Martin F (198 5), The treatment and out come of anorexia nervosa inadolescence: a prospect ive study and five-year follow-up. J PsychiatrRes 19:509-514
936
Metropolitan Life Insurance Comp any (1983), Metropolitan height andweight tables. Stat Bull Metrap Life Found64:2- 9
Mickalide AD , Anderson AE (1985 ), Subgroups of anorexia nervosa andbulimia: validity and utility. J Psychiatr Res 19:121-128
Mitchell JE, Pyle RL, Eckert ED , H atsukami D, Soil E (1990), Bulim ianervosa with and without a history of anorexia nervosa. Compr Psychiatry 31:171- 175
Mitchell JE, Pyle RL, Hatsukam i D, Goff G , Glotter D, Harper J (1989 ),A 2-5 year follow-up study of pat ients treated for bulimia . Int J EatDisord 8:157-165
Morgan HG, Purgold J, Welbourne J (1983), Management and out comein anorexia nervosa: a standardized prognostic stud y. Br J Psychiatry143:282-287
Morgan HG, Russell GM (1975), Value of family background and clinicalfeatures as predictors of long-term outcome in anorexia nervosa: astandardized prognostic study. Br J Psychiatry 143:282-287
Nussbaum M, Shenker IR, Baird D , Saravay S (1985), Follow-up investigation in patients with anorexia nervosa. J Pediatr 106:835-840
Pfohl B, Stangl D, Zimmerman M (1982) , The Structured Interview forDSM-III Personality Disorders (SIDP), 2nd ed. Iowa City: Universityof Iowa
Ratn asuriya RH, Eisler I, Szmukler GI , Russell GFM (1991), Anorex ianervosa: outcome and prognostic factors after 20 years. Br J Psychiatry 158:495-50 2
Robins E, Guze SB (1970), Establishm ent of diagnostic validity in psychiatric illness: its application to schizophrenia. AmJ Psychiatry126:983-987
Robins L, Helzer ] , Croughan J, Ratcliff K (1981) , National Institute ofMental Health Diagnostic Interview Schedule. Arch Gen Psychiatry38:381-389
Santonastaso P, Favaretto G, Canton G (1987), Anorexia nervosa inItaly: clinical features and OUtCOme in a long-term follow-up study.Psychopathology 20:8-17
Seidensticker JF, Tzagournis M (1968), Anore xia nervosa: clinical featuresand long-term follow-up . J Chronic Dis 21:361- 367
Sohlberg S, Norring C, Holmgren S, Rosmark B (1989 ), Impulsivity andlong-term prognosis of psychiatr ic patients with anorexia nervosa/bulim ia nervosa. J Nero Ment Dis 177:249-258
Spitzer R, Endi cott] (1979), ScheduleforAffective Disordersand Schizophrenia Lifetime Version. New York: Biometrics Research, New York StatePsychiatr ic Institute
Spitzer RL' End icorr ] , Robin s E (1985). Research Diagnostic Criteria (RD C)fora Selected Group ofFunctiona!Disorders, 3rd ed. New York: BiometricsResearch, New York State Psychiatri c Institute
Steinhausen HC, Glanville K (1983), Follow-up studies ofanorexia nervosa:a review of research findings. Psycho! Med 13:239-249
Steinhausen HC, Rauss-Mason C, Seidel R (1991), Follow-up studies ofanorexia nervosa: a review of four decades of outcome research. Psycho!Med 21:447-454
Strob er M, Salkin B, Burroughs], Morell W (1982), Validity of the bulimicrestricror distinction in anorexia nervosa. J NeruMent Dis 170:345-351
Sturtzenberger S, Cantwell DP , Burroughs], Salkin B, Green JK (1977),Follow-up study of adolescent psychiatric inpat ients with anorexianervosa: the assessment o f outcome. JA m Acad Child Psychiatry16:703-715
Swift W], Ritho ltz M, Kalin NH, Kaslow N (1987), A follow-up studyof thirty hospitalized bulimics. Psycbosom Med 49:45- 55
Tolsrrup K. Brinch M. lsager T et al. (1985) , Long-term outcome of 151cases of anorexia nervosa. Acta Psychiatr Scand7 1:380- 387
Touyz SW , Beaumont P] (1984) , Ano rexia nervosa: a follow-up investigation. Med J Aus: 141:219-2 22
Vandereycken W , Pierloot R (1983) , The significance of subclassificationin anorexia nervosa: a comparative study of 141 patients . Psycho!Med 13:543-549
Viesselman JO , Roig M (1985), Depression and suicidality in eatingdisorders. J Clin Psychiatry 46:118-1 24
W ilson GT, Walsh BT (1991), Eatin g disorders in the DSM-lV. J AbnormPsycho! 100:362-365
J. AM . ACAD. CHILD ADOLESC . PSYCHIATRY. 35:7, JULY 1996