Embed Size (px)
Citation preview

Special populationS
Substance use and suicidal behaviourRachel Jenkins
AbstractSuicide and self-harm are receiving increased attention and awareness
from policymakers, professionals, researchers and the public. Globally,
suicide is thought to be the 15th leading cause of death, although this
may be an underestimate because it does not take into account – ‘unoffi-
cial’ suicides (deaths that are suicides but not recorded as such, i.e. open
verdicts), and many countries do not yet have vital registration systems.
Self-harm is not recorded nationally, although there are a number of
good studies within and between countries. this contribution discusses
the relationship of substance abuse with suicide and self-harm. alcohol
has long been recognized as a major contributor to suicide and, as the
abuse of other substances has risen, there is now increasing evidence
of their contribution to suicidal behaviour and suicide. thus, substance
abuse is the second most frequent precursor to suicide after depressive
illness. the negative consequences of substance abuse accumulate in a
vicious circle of diminishing social support and increased exposure to
life events, subsequent affective disorder and increased suicidal risk.
Help is infrequently sought and poorly used. Health and social care pro-
fessionals need to be aware that depression and substance abuse form a
lethal combination, and that vigorous treatment of comorbid depression
is the most promising avenue for prevention of suicide in people with
substance abuse.
Keywords alcohol; life events; self-harm; social support; substance
abuse; suicidal risk; suicide
Suicide and self-harm are receiving increased attention and awareness from policymakers, professionals, researchers and the public.1,2 Globally, suicide is thought to be the 15th leading cause of death,3 although this may be an underestimate because it does not take into account ‘unofficial’ suicides (deaths that are suicides but not recorded as such, i.e. open verdicts), and many countries do not yet have vital registration systems.4 Self-harm is not recorded nationally, although there are a number of good studies within and between countries.
Rachel Jenkins FRCPsych FFOHM Dist. FAPA is Director of the WHO
Collaborating Centre at the Institute of Psychiatry, London, UK, and
Visiting Professor. She is a psychiatrist and epidemiologist, and
collaborates with international organizations to give mental health
policy and research support to low-income countries. She is currently
on secondment from the Department of Health, where she was
principal medical officer for mental health from 1987 to 1996.
Conflicts of interest: none declared.
pSYcHiatRY 6:1 1
This contribution discusses the relationship of substance abuse with suicide and self-harm. Alcohol has long been recog-nized as a major contributor to suicide and, as the abuse of other substances has risen, there is now increasing evidence of their contribution to suicidal behaviour and suicide.5
Contribution of substance abuse to suicide
Psychological autopsy studies show that while psychiatric illness is the central antecedent in 90–100% of cases of completed sui-cide, alcoholism or other substance abuse is found in 20–50% of cases; it is thus second only to depressive disorder as a psychi-atric contributor to suicide.5 Indeed, it is when substance abuse is comorbid with affective disorder that it contributes most to sui-cide. Nearly all diagnosed cases of personality disorder identified retrospectively in suicides are complicated by substance abuse.6
Lifetime risk of suicide in alcohol abuse
It used to be thought that the lifetime risk of suicide in alcoholics was 15%,7 but subsequent longitudinal studies have shown that the lifetime risk is much lower and is influenced by both indi-vidual clinical status and the contextual national suicide rate. For countries with historically low and intermediate suicide rates (e.g. low: Norway, Scotland, Trinidad; intermediate: USA, Canada, England and Wales) (Table 1), the lifetime risk of sui-cide in alcoholics is between 2.5% and 3.5%, depending on clini-cal status; this risk is nearly doubled in countries with relatively high suicide rates (e.g. Sweden, Austria, Germany).8,9
Sex differences: women generally have lower suicide rates than men, except in some countries in the West Pacific region and Southeast Asia; they also have lower rates of substance abuse. The proportion of suicides attributable to substance abuse is accordingly lower. In the ten published psychological autopsy studies providing data by sex, nearly one-third of male suicides are identified as ‘alcoholics’, compared with only 1 in 7 female suicides.5
Role of social factors
Stressful life events are key contributors to suicide, especially in people with substance abuse,10 and social support is a protective factor in suicide. The UK Office for National Statistics survey showed that stressful life events are more common and social support is more restricted in people who abuse alcohol and in people who abuse drugs than in the general population.11
Contribution of substance abuse to suicidal thoughts and to suicide attempts
Substance abuse substantially increases the risk of suicidal thoughts. For example, in the second British Psychiatric Morbid-ity Survey,12 35% of men with moderate or severe alcohol depen-dence had suicidal thoughts in the last year and 10% had made an actual attempt in the last year, compared with 3% and 0.3% respectively of men with no alcohol dependence. There were too few women in the survey with moderate or severe dependence to present figures, but even mild alcohol dependence in women
6 published by elsevier ltd.

Special populationS
increased the risk of suicidal thoughts to 12.5% and suicidal attempts 3.4% in the last year, compared with 3.8% and 0.4% respectively of women with no alcohol dependence.
Similarly, 12% of men with cannabis dependence had suicidal thoughts in the last year, and 0.4% had made an actual suicide attempt, compared with 3% and 0.5% respectively of men with no cannabis abuse. Eighteen percent of women with cannabis dependence had suicidal thoughts in the last year and 4% had made an actual attempt, compared with 4% and 0.5% respec-tively of women with no cannabis dependence.
In a similar large national psychiatric morbidity survey of Brit-ish prisoners, of those with suicidal thoughts in the last year, 37% had an AUDIT score of over 16, and 49% were dependent on stimulants or opiates or both. Of those who made suicidal attempts in the last year, again 40% had an AUDIT score of over 16, and 50% were dependent on stimulants or opiates or both. Of prisoners with suicidal attempts in last week, the relationship with substance abuse was even more marked, with 55% having an AUDIT score of over 16, while 64% were dependent on opi-ates or stimulants. Suicide attempters were twice as likely to be heavy smokers as those who had never attempted suicide.13
A 25-year prospective study of Swedish male conscripts showed that those who abused alcohol had a highly elevated risk
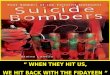
Characteristics of 4859 suicides in contact with mental health services in england and Wales
number (n = 4859) % (95% CI)
Sociodemographic
characteristicsMedian age (range) 41 yrs (13–95 yrs)
Male 3198 66 (64–67)
ethnic minority 282 6 (5–7)
not currently married 3405 71 (70–73)
unemployed/long-term sick 2765 58 (58–60)
living alone 2006 43 (41–44)
Clinical characteristicsany secondary diagnosis 2460 52 (51–54)
over 5 previous
admissions
712 16 (15–17)
History of previous
self-harm
3077 64 (63–66)
History of violence 920 19 (18–21)
History of alcohol misuse 1899 40 (38–41)
History of drug misuse 1348 28 (27–30)
Aspects of clinical carelast contact with services
within 7 days
2308 48 (47–50)
Symptoms at last contact 2990 64 (63–65)
out of contact with
services
1153 9 (27–30)
non-compliant with
treatment
929 22 (21–24)
Source: Department of Health, 2001.
Table 1
pSYcHiatRY 6:1 17
of suicide attempts (odds ratio 27.1) and of completed suicide (odds ratio 2.4). Hawton et al. found that in a series of self-harm patients in Oxford, UK, 12% of males and 6% of females were drug users. They also found that substance-abusing suicide attempters had a particularly high rate of repetition of suicide attempts.14 Substance abuse was the key diagnostic predictor of eventual suicide.15
Prevention of suicide in people with substance abuse
Clinical monitoring of the known psychosocial risk factors for suicide in people with substance abuse is important. Murphy found in a retrospective series of suicides in people with severe alcohol abuse that more than four-fifths had communicated suicidal thoughts, verbally or behaviourally, or both, and 38% had made a previous attempt. Two-thirds had little or no social support, half were unemployed and half had significant medical problems. Nearly two-fifths were living alone. Murphy argues that with nine out of ten ‘alcoholic’ suicides having at least three of these factors, close monitoring of these factors may help in the assessment of the changing suicidal risk in alcoholics.10
TreatmentTreatment of the substance abuse would be very helpful but remains difficult. However, effective treatments exist for the comorbid depression,16 which should be treated vigorously. Ready access to means of suicide should be restricted (e.g. by restricting pack sizes of paracetamol).
Conclusion
Substance abuse is the second most frequent precursor to suicide after depressive illness. The negative consequences of substance abuse accumulate in a vicious circle of diminishing social sup-port and increased exposure to life events, subsequent affective disorder and increased suicidal risk. Help is infrequently sought and poorly used. Health and social care professionals need to be aware that depression and substance abuse form a lethal com-bination, and that vigorous treatment of comorbid depression is the most promising avenue for prevention of suicide in people with substance abuse. ◆
RefeRenCeS
1 Jenkins R, Singh B. General population strategies for suicide
prevention. in: Hawton K, van Heeringen K, eds. the international
handbook of suicide and attempted suicide. chichester: Wiley, 2000.
2 Hawton K, van Heeringen K, eds. the international handbook of
suicide and attempted suicide. chichester: Wiley, 2000.
3 World Health organization. World health report. Geneva:
WHo, 2000.
4 Jenkins R. addressing suicide as a public-health problem. Lancet
2002; 359: 813–14.
5 Murphy Ge. psychiatric aspects of suicidal behaviour: substance
abuse. in: Hawton K, van Heeringen K, eds. the international
handbook of suicide and attempted suicide. chichester: Wiley, 2000.
6 cheng at, Mann aH, chan Ka. personality disorder and suicide.
a case-control study. Br J Psychiatry 1997; 170: 441–46.
published by elsevier ltd.

Special populationS
7 Miles cp. conditions predisposing to suicide: a review. J Nerv Ment
Dis 1977; 164: 231–46.
8 Murphy Ge, Wetzel RD. the lifetime risk of suicide in alcoholism.
Arch Gen Psychiatry 1990; 47: 383–92.
9 Rossow i, amundsen a. alcohol abuse and suicide: a 40-year
prospective study of norwegian conscripts. Addiction 1995; 90:
685–91.
10 Murphy Ge. Suicide in alcoholism. new York: oxford university
press, 1992.
11 coulthard M, Farrell M, Singleton n, Meltzer H. tobacco, alcohol and
drug use and mental health. london: Stationery office, 2002.
12 Meltzer H, lader D, corbin t, Singleton n, Jenkins R, Brugha t.
non-fatal suicidal behaviour among adults aged 16 to 74 in Great
Britain. london: Stationery office, 2002.
13 Jenkins R, Bhugra D, Meltzer H, et al. psychiatric and social aspects
of suicidal behaviour in prisons. Psychol Med 2005; 35: 257–69.
14 Hawton K, Sinton S, Fagg J. Deliberate self-harm in alcohol and
substance misuse: patient characterstics and patterns of clinical
care. Drug Alcohol Rev 1997; 16: 123–29.
pSYcHiatRY 6:1 1
15 Hawton K, Fagg J, platt S, Hawkins M. Factors associated with
suicide after parasuicide in young people. Br Med J 1993; 306:
1641–44.
16 Mason BJ, Kocsis JH. Desipramine treatment of alcoholism.
Psychopharmacol Bull 1991; 27: 155–61.
fuRTheR ReAdIng
Department of Health. national suicide prevention strategy for england.
london: Stationery office, 2001.
Farrell M, Howes S, taylor c, et al. Substance misuse and psychiatric
morbidity: an overview of the opcS national psychiatric Morbidity
Survey. Addict Behav 1998; 23: 909–18.
World Health organization collaborating centre for Research and
training for Mental Health. WHo guide to mental health in primary
care. london: Royal Society of Medicine press, 2000.
8 published by elsevier ltd.