Embed Size (px)
Citation preview
Submucous Lipoma of the Colon *
LEON GINZBURG, M.D., MICHAEL WEINGARTEN, M.D., MuRRY G. FiscHER, M.D.
From the Department of Surgery and the Division of Gastroenterology,Department of Medicine, Beth Israel Hospital, New York, N. Y.
LIPOMATA occur in all parts of the gastro-intestinal tract but the most common site isin the colon.5 Their recognition is of greatimportance since they are benign tumorsand can at times be easily removed bycolotomy, without resorting to major colonicresection. They may be present for longperiods of time but probably only becomesymptomatic when they cause intussuscep-tion of the colon with obstruction or whenulceration of the dome occurs as a resultof recurrent intussusception of a moreminor nature.
If one excludes adenomas, lipomata arethe most frequent benign tumors of thelarge bowel. Despite this, they are foundrelatively infrequently in colonic surgery.Long, Dockerty and Waugh 2 reported on33 lipomata of the colon in 125,000 ab-dominal explorations. In 23 of these thecolonic lipoma was the primary pathology(an incidence of 0.018%o) while in tencases it was found as an incidental finding(associated with carcinoma of the colon ineight). Staemmler,6 in a series of 17,000 con-secutive autopsies, found nine lipomata ofthe colon, an incidence of 0.05 per cent.Palazzo 4 recorded 20 large bowel lipomataof which 11 were symptomatic and nineasymptomatic.
Colonic lipomata are usually single tu-mors but may occasionally be multiple.Ninety per cent arise from the submucosaand 10 per cent from the serosa. Both typesmay be concomitantly found in 10 per centof cases. The predominant submucous vari-ety may be sessile or pedunculated. Theyare covered either by an atrophic mucosa
* Submitted for publication November 22,1957.
767
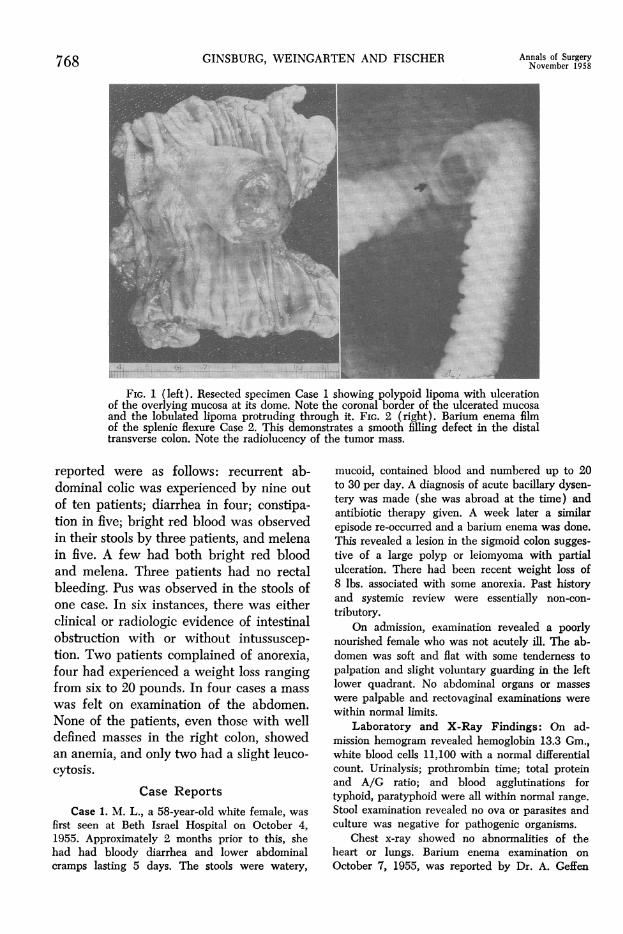
with congestion and inflammatory foci orare frequently partially ulcerated with ero-sion of the overlying mucosa at the domeof the lipoma (Fig. 1). The bleeding ac-companying the congestion or ulcerationmay be one of the earliest signs it produces.They range in size from 1 to 30 cm. 7 indiameter.At Beth Israel Hospital 19 cases of lipo-
mata of the colon have been observed since1930. In ten of these 19 instances, the li-poma was the primary and sole pathologicdiagnosis, while in the remaining nine pa-tients, it was an incidental finding in speci-mens resected for carcinoma of the colon.Of the ten primary cases, 50 per cent werein males and 50 per cent in females. Theyoungest patient was 36 years of age, andthe oldest 72 years; 70 per cent of the pa-tients were in the fifth and sixth decades.The location of the primary lesion was asfollows: Four (or 40%o) were in the cecumand ascending colon; two (or 20% ) werein the sigmoid colon; and there was oneeach in the hepatic flexure, transversecolon, splenic flexure and descending colon.The admission diagnosis was neoplasm
of the colon in seven instances, polyp of thecolon in two, and acute intestinal obstruc-tion in one case. In no instance, was anadmission diagnosis of lipoma made. How-ever, in three cases, the correct diagnosis oflipoma of the colon was made preopera-tively after radiologic examination of thecolon because of the radiolucency of theobserved tumor (Fig. 2).Submucous lipomata, per se, without
complications probably only give rise tominimal symptoms. The major symptomsand signs in the ten primary cases herein
GINSBURG, WEINGARTEN AND FISCHER Annals of SurgeryNovember 1958
FIG. 1 (left). Resected specimen Case 1 showing polypoid lipoma with ulcerationof the overlying mucosa at its dome. Note the coronal border of the ulcerated mucosaand the lobulated lipoma protruding through it. FIG. 2 (right). Barium enema filmof the splenic flexure Case 2. This demonstrates a smooth filling defect in the distaltransverse colon. Note the radiolucency of the tumor mass.
reported were as follows: recurrent ab-dominal colic was experienced by nine outof ten patients; diarrhea in four; constipa-tion in five; bright red blood was observedin their stools by three patients, and melenain five. A few had both bright red bloodand melena. Three patients had no rectalbleeding. Pus was observed in the stools ofone case. In six instances, there was eitherclinical or radiologic evidence of intestinalobstruction with or without intussuscep-tion. Two patients complained of anorexia,four had experienced a weight loss rangingfrom six to 20 pounds. In four cases a mass
was felt on examination of the abdomen.None of the patients, even those with welldefined masses in the right colon, showedan anemia, and only two had a slight leuco-cytosis.
Case ReportsCase 1. M. L., a 58-year-old white female, was
first seen at Beth Israel Hospital on October 4,1955. Approximately 2 months prior to this, shehad had bloody diarrhea and lower abdominalcramps lasting 5 days. The stools were watery,
mucoid, contained blood and numbered up to 20to 30 per day. A diagnosis of acute bacillary dysen-tery was made (she was abroad at the time) andantibiotic therapy given. A week later a similarepisode re-occurred and a barium enema was done.This revealed a lesion in the sigmoid colon sugges-tive of a large polyp or leiomyoma with partialulceration. There had been recent weight loss of8 lbs. associated with some anorexia. Past historyand systemic review were essentially non-con-
tributory.On admission, examination revealed a poorly
nourished female who was not acutely ill. The ab-domen was soft and flat with some tendemess topalpation and slight voluntary guarding in the leftlower quadrant. No abdominal organs or masses
were palpable and rectovaginal examinations were
within normal limits.Laboratory and X-Ray Findings: On ad-
mission hemogram revealed hemoglobin 13.3 Gm.,white blood cells 11,100 with a normal differentialcount. Urinalysis; prothrombin time; total proteinand A/G ratio; and blood agglutinations fortyphoid, paratyphoid were all within normal range.
Stool examination revealed no ova or parasites andculture was negative for pathogenic organisms.
Chest x-ray showed no abnormalities of theheart or lungs. Barium enema examination on
October 7, 1955, was reported by Dr. A. Geffen
768
SUBMUCOUS LIPOMA OF THE COLON
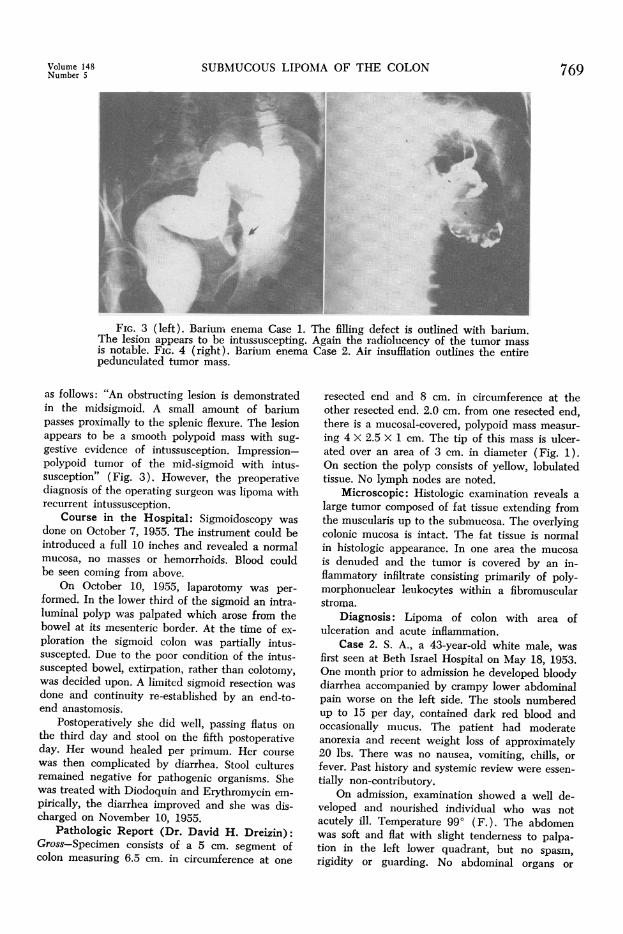
FIG. 3 (left). Barium- enema Case 1. The filling defect is outlined with barium.The lesion appears to be intussuscepting. Again the radiolucency of the tumor massis notable. FIG. 4 (right). Barium enema Case 2. Air insufflation outlines the entirepedunculated tumor mass.
as follows: "An obstructing lesion is demonstratedin the midsigmoid. A small amount of bariumpasses proximally to the splenic flexure. The lesionappears to be a smooth polypoid mass with sug-gestive evidence of intussusception. Impression-polypoid tumor of the mid-sigmoid with intus-susception" (Fig. 3). However, the preoperativediagnosis of the operating surgeon was lipoma withrecurrent intussusception.
Course in the Hospital: Sigmoidoseopy wasdone on October 7, 1955. The instrument could beintroduced a full 10 inches and revealed a normalmucosa, no masses or hemorrhoids. Blood couldbe seen coming from above.
On October 10, 1955, laparotomy was per-formed. In the lower third of the sigmoid an intra-luminal polyp was palpated which arose from thebowel at its mesenteric border. At the time of ex-ploration the sigmoid colon was partially intus-suscepted. Due to the poor condition of the intus-suscepted bowel, extirpation, rather than colotomy,was decided upon. A limited sigmoid resection wasdone and continuity re-established by an end-to-end anastomosis.
Postoperatively she did well, passing flatus onthe third day and stool on the fifth postoperativeday. Her wound healed per primum. Her coursewas then complicated by diarrhea. Stool culturesremained negative for pathogenic organisms. Shewas treated with Diodoquin and Erythromycin em-
pirically, the diarrhea improved and she was dis-charged on November 10, 1955.
Pathologic Report (Dr. David H. Dreizin):Gross-Specimen consists of a 5 cm. segment ofcolon measuring 6.5 cm. in circumference at one
resected end and 8 cm. in circumference at theother resected end. 2.0 cm. from one resected end,there is a mucosal-covered, polypoid mass measur-ing 4 X 2.5 X 1 cm. The tip of this mass is ulcer-ated over an area of 3 cm. in diameter (Fig. 1).On section the polyp consists of yellow, lobulatedtissue. No lymph nodes are noted.
Microscopic: Histologic examination reveals alarge tumor composed of fat tissue extending fromthe muscularis up to the submucosa. The overlyingcolonic mucosa is intact. The fat tissue is normalin histologic appearance. In one area the mucosais denuded and the tumor is covered by an in-flammatory infiltrate consisting primarily of poly-morphonuclear leukocytes within a fibromuscularstroma.
Diagnosis: Lipoma of colon with area ofulceration and acute inflammation.
Case 2. S. A., a 43-year-old white male, wasfirst seen at Beth Israel Hospital on May 18, 1953.One month prior to admission he developed bloodydiarrhea accompanied by crampy lower abdominalpain worse on the left side. The stools numberedup to 15 per day, contained dark red blood andoccasionally mucus. The patient had moderateanorexia and recent weight loss of approximately20 lbs. There was no nausea, vomiting, chills, orfever. Past history and systemic review were essen-
tially non-contributory.On admission, examination showed a well de-
veloped and nourished individual who was notacutely ill. Temperature 990 (F.). The abdomenwas soft and flat with slight tenderness to palpa-tion in the left lower quadrant, but no spasm,rigidity or guarding. No abdominal organs or
Volume 148Number 5 769
GINSBURG, WEINGARTEN AND FISCHER Annals of SurgeryNovember 1958
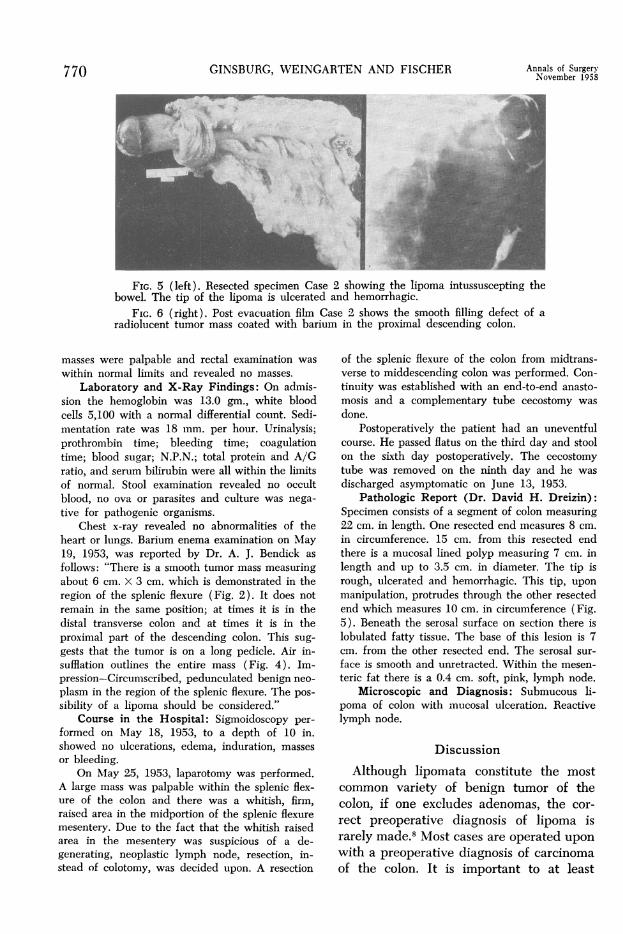
FIG. s (left). Resected specimen Case 2 showing the lipoma intussuscepting thebowel. The tip of the lipoma is ulcerated and hemorrhagic.
FIG. 6 (right). Post evacuation film Case 2 shows the smooth filling defect of aradiolucent tumor mass coated with barium in the proximal descending colon.
masses were palpable and rectal examination was
within normal limits and revealed no masses.
Laboratory and X-Ray Findings: On admis-sion the hemoglobin was 13.0 gm., white bloodcells 5,100 with a normal differential count. Sedi-mentation rate was 18 mm. per hour. Urinalysis;prothrombin time; bleeding time; coagulationtime; blood sugar; N.P.N.; total protein and A/Gratio, and serum bilirubin were all within the limitsof normal. Stool examination revealed no occultblood, no ova or parasites and culture was nega-tive for pathogenic organisms.
Chest x-ray revealed no abnormalities of theheart or lungs. Barium enema examination on May19, 1953, was reported by Dr. A. J. Bendick as
follows: "There is a smooth tumor mass measuringabout 6 cm. x 3 cm. which is demonstrated in theregion of the splenic flexure (Fig. 2). It does notremain in the same position; at times it is in thedistal transverse colon and at times it is in theproximal part of the descending colon. This sug-
gests that the tumor is on a long pedicle. Air in-sufflation outlines the entire mass (Fig. 4). Im-pression-Circumscribed, pedunculated benign neo-
plasm in the region of the splenic flexure. The pos-
sibility of a lipoma should be considered."Course in the Hospital: Sigmoidoscopy per-
formed on May 18, 1953, to a depth of 10 in.showed no ulcerations, edema, induration, masses
or bleeding.On May 25, 1953, laparotomy was performed.
A large mass was palpable within the splenic flex-ure of the colon and there was a whitish, firm,raised area in the midportion of the splenic flexuremesentery. Due to the fact that the whitish raisedarea in the mesentery was suspicious of a de-generating, neoplastic lymph node, resection, in-stead of colotomy, was decided upon. A resection
of the splenic flexure of the colon from midtrans-verse to middescending colon was performed. Con-tinuity was established with an end-to-end anasto-mosis and a complementary tube cecostomy was
done.Postoperatively the patient had an uneventful
course. He passed flatus on the third day and stoolon the sixth day postoperatively. The cecostomytube was removed on the ninth day and he was
discharged asymptomatic on June 13, 1953.Pathologic Report (Dr. David H. Dreizin):
Specimen consists of a segment of colon measuring22 cm. in length. One resected end measures 8 cm.
in circumference. 15 cm. from this resected endthere is a mucosal lined polyp measuring 7 cm. inlength and up to 3.5 cm. in diameter. The tip isrough, ulcerated and hemorrhagic. This tip, upon
manipulation, protrudes through the other resectedend which measures 10 cm. in circumference (Fig.5). Beneath the serosal surface on section there islobulated fatty tissue. The base of this lesion is 7cm. from the other resected end. The serosal sur-
face is smooth and unretracted. Within the mesen-
teric fat there is a 0.4 cm. soft, pink, lymph node.Microscopic and Diagnosis: Submucous li-
poma of colon with mucosal ulceration. Reactivelymph node.
DiscussionAlthough lipomata constitute the most
common variety of benign tumor of thecolon, if one excludes adenomas, the cor-
rect preoperative diagnosis of lipoma israrely made.8 Most cases are operated upon
with a preoperative diagnosis of carcinomaof the colon. It is important to at least
770
Volume 148 SUBMUCOUS LIPCNumber 5
suspect the diagnosis so that colotomy andexcision or a less extensive surgical resec-tion can be performed. Unfortunately, themajority of cases are not recognized andradical colectomy is unnecessarily per-formed.
In the group of ten cases herein reported,a preoperative diagnosis of lipoma wasmade in three instances based on the find-ings on barium enema examination. Theypresented the typical signs of an intramural,extramucosal tumor: a smooth filling de-fect, which when seen in profile view,shows an abrupt sharp angle at the pointwhere the edge of the tumor meets the un-involved wall of the bowel. Seen face-on,the lesion is sharply outlined in the reliefpicture of the bowel. In addition the radio-lucency of the tumor, due to the fact thatadipose tissue is the most radiolucent ofall body tissues, was most striking (Fig. 6).Although ulceration of the mucosa over thedome of the lipoma frequently occurs, thisis not demonstrable radiologically for rea-sons which will be discussed below. Anoccasional lipoma has been visualized sig-moidoscopically.There are no pathognomonic symptoms
of lipoma of the colon. Actually these le-sions are probably asymptomatic unless in-tussusception occurs. The clinical picture isthen that of intussusception of the colonwith the resulting symptomatology of acute,chronic, or recurrent intestinal obstruction.The tumor itself does not cause obstruction,but this is due rather to the intussusception.Once the tumor starts to serve as the headof the intussusceptum it may become con-gested, with subsequent ulceration, causingthe appearance of blood in the stool. Themucosa itself, over the dome of the lipoma,becomes ulcerated and the lipoma seems toprotrude beyond the mucosa which forms acoronal border (Fig. 7). In our series of tencases, five showed such ulcerations. Theseulcerations, as stated above, cannot bedemonstrated radiologically because theulceration is superficial and does not in-
)MA OF THE COLON 771
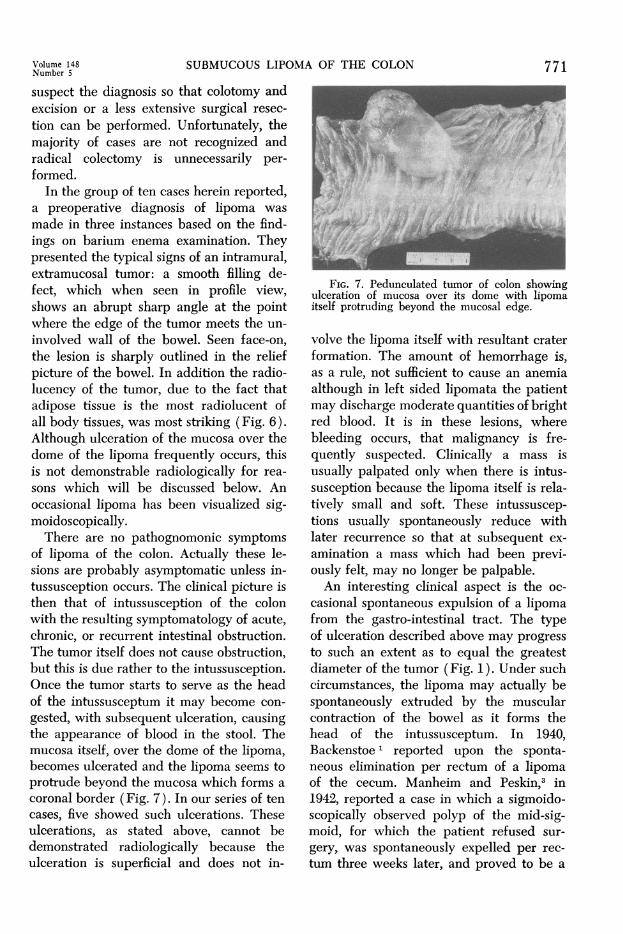
FIG. 7. Pedunculated tumor of colon showingulceration of mucosa over its dome with lipomaitself protruding beyond the mucosal edge.
volve the lipoma itself with resultant craterformation. The amount of hemorrhage is,as a rule, not sufficient to cause an anemiaalthough in left sided lipomata the patientmay discharge moderate quantities of brightred blood. It is in these lesions, wherebleeding occurs, that malignancy is fre-quently suspected. Clinically a mass isusually palpated only when there is intus-susception because the lipoma itself is rela-tively small and soft. These intussuscep-tions usually spontaneously reduce withlater recurrence so that at subsequent ex-amination a mass which had been previ-ously felt, may no longer be palpable.An interesting clinical aspect is the oc-
casional spontaneous expulsion of a lipomafrom the gastro-intestinal tract. The typeof ulceration described above may progressto such an extent as to equal the greatestdiameter of the tumor (Fig. 1). Under suchcircumstances, the lipoma may actually bespontaneously extruded by the muscularcontraction of the bowel as it forms thehead of the intussusceptum. In 1940,Backenstoe 1 reported upon the sponta-neous elimination per rectum of a lipomaof the cecum. Manheim and Peskin,3 in1942, reported a case in which a sigmoido-scopically observed polyp of the mid-sig-moid, for which the patient refused sur-gery, was spontaneously expelled per rec-tum three weeks later, and proved to be a
772 GINSBURG, WEINGARTEN AND FISCHER Annals of Surgery
lipoma. These authors reviewed the litera-ture and found 19 instances of previouslyreported spontaneous elimination of acolonic lipoma.At laparotomy three types of cases are
encountered:Type 1: The tumor is very soft, exceed-
ingly mobile and sometimes difficult topalpate and fix. It is in this type of case thatsimple colotomy and excision should bedone. In some cases a purely mucosalpseudopedicle is present or can be artifi-cially developed. In these cases transec-tion of the pedicle suffices. In others wherethere is no true pedicle, the mucosa over thedistal portion is circumcised and the lipomamanually, but gently, extruded, clampingany small visible submucosal vessels. Thedefect is then oversewn; this also controlsany ooze from the cut mucosal edge.Type 2: This group closely resembles
the preceding one except that due to recentintussusception the bowel wall in the vicin-ity of the lipoma is edematous and some-what friable. Although the palpatory find-ings and radiologic picture are stronglysuggestive of lipoma the local condition ofthe bowel wall at the site of origin will notsafely permit colotomy. In these instances,local segmental resection is performed.Type 3: This last type is one where, due
to chronic recurrent intussusception thereis marked thickening of the bowel wall inthe vicinity and the development of con-siderable induration in the lipoma itself. Insuch cases it is difficult to be sure that oneis not dealing with a polypoid carcinomaand in this group, colonic resection shouldbe undertaken.
In our ten primary cases, colotomy andexcision was feasible in three instances;limited segmental resection of the colonwas done in one case because of the localcondition of the bowel wall (Case 1); andmajor colonic resection as for carcinomaperformed in six patients because the diag-nosis was either in doubt (Case 2) or notsuspected at all.
Summary
1) Ten primary cases of lipomata ofthe colon were encountered at laparotomybetween 1930 and 1956. An additional ninelipomata were found in association withcarcinoma of the colon.
2) The correct preoperative diagnosiswas made in three cases after radiologicexamination of the colon. These all oc-curred in the last few years. A radiolucenttumor with the characteristics of a benignneoplasm was the basis for the radiologicdiagnosis.
3) The importance of a correct preop-erative diagnosis is stressed so that simplecolotomy and lipectomy can be done ratherthan extensive resection with its corre-spondingly increased morbidity and mor-tality.
4) The clinical manifestations are re-viewed, emphasizing the importance of re-current intussusception with subsequentulceration of the overlying mucosa in theproduction of the clinical picture.
Bibliography1. Backenstoe, G. S.: Spontaneous Expulsion of
Submucous Lipoma of Cecum. Penn. M. J.,44:21, 1940.
2. Long, G. C., M. D. Dockerty and J. M. Waugh:Lipoma of Colon. Surg. Clin. North Amer.,29:1233, 1949.
3. Manheim, S. D. and H. Peskin: SpontaneousElimination of Lipoma from Sigmoid Flexure.J. A. M. A., 118:1214, 1942.
4. Palazzo, W. L.: Lipomas of the GastrointestinalTract. Am. J. Roentgenol., 62:823, 1949.
5. Pemberton, J. de J. and C. J. McCormack:Submucous Lipomas of Colon and Rectum.Am. J. Surg., 37:205, 1937.
6. Staemmler, Martin: Das. Lipom. In: Reicheland Staemmler: Die Neubildungen des Dar-mes. Part I. Stuttgart: Enke, 1924, p. 273-279.
7. Weinberg, T. and M. Feldman: Lipomas of theGastrointestinal Tract. Amer. J. Roentgenol.,25:272, 1955.
8. Wolf, B. S., M. Melamed and M. T. Khilnani:Lipoma of the Colon. J. Mt. Sinai Hosp., 21:80, 1954.

![Large buccal fat pad lipoma: A rare case report...gland lipoma in 2 cases, angiolipoma in 2 cases, and spindle cell lipoma in 3 cases [10]. The most common presentation of BFP lipoma](https://img.pdfslide.us/doc/110x75/5e610a1252021369db53e163/large-buccal-fat-pad-lipoma-a-rare-case-report-gland-lipoma-in-2-cases-angiolipoma.jpg)