Embed Size (px)
Citation preview
Submarine Pitchers
EXERCISES TAILORED TO MEET THE NEEDS OF SUBMARINE PITCHERS
Independent Research
Presented to
The Faculty of the College of Health Professions and Social Work
Florida Gulf Coast University
In Partial Fulfillment
Of the Requirement for the Degree of
Doctorate of Physical Therapy
By
Kurtis Mullaney and Michael Klein
2015

Submarine Pitchers
APPROVAL SHEET
This independent research is submitted in partial fulfillment
of the requirements for the degree of
Doctorate of Physical Therapy
______________________________________
Kurtis Mullaney
Michael Klein
Approved: May 2015
______________________________________
Dr. Shawn Felton, EdD, ATC, LAT
Committee Chair
______________________________________
Professor Kelley Henderson, M.Ed., LAT, ATC
Committee Member
The final copy of this independent research has been examined by the signatories, and we find that both the content and the form meet acceptable presentation standards of scholarly work in the above mentioned discipline.
Submarine Pitchers
Acknowledgements
Mike and I would like to thank several people for helping us to complete our independent
research project. First of all, we would like to thank the overwhelming support we have
always received from our families and loved ones, including Kelly, Michael, Kyle, Kameron,
Karson, and Kolby Mullaney, and Candice, Hannah, and Eva Klein. Also, we would like to
thank Dr. Shawn Felton and Professor Kelley Henderson for always rapidly responding,
being attentive to detail, showing immense patience, and working tirelessly to help us with
this research. We would also like to thank Dr. Arie van Duijn for his contributions in terms
of helping us learn and utilize the equipment needed for this project. Other faculty that aided
in completing this study included Dr. Mollie Venglar, Professor Tom Bevins, and Dr. Dennis
Hunt. This project took a lot of time, effort, and patience from all of us involved and we are
extremely grateful for the help. We would also like to thank all of the participants involved,
who sacrificed their time to help make this research happen. Lastly we would like to thank
our classmates, who were always there to support us and to keep us encouraged even when
we hit major roadblocks along the way. This has been a difficult but rewarding journey, and
we would not have been able to complete it without the support of all of those involved.
Submarine Pitchers 4
Table of Contents
Acknowledgements ................................................................................................................... 3
Abstract ..................................................................................................................................... 5
Introduction ............................................................................................................................... 6
Phases of Throwing ............................................................................................................... 9
Electromyography ............................................................................................................... 12
Motion Analysis .................................................................................................................. 14
Purpose .................................................................................................................................... 15
Research Question .................................................................................................................. 16
Hypothesis ............................................................................................................................... 16
Methods ................................................................................................................................... 16
Subjects ............................................................................................................................... 18
Instrumentation ................................................................................................................... 19
Procedure ............................................................................................................................ 20
Exercise Descriptions .......................................................................................................... 23
Data Analysis ...................................................................................................................... 26
Results ..................................................................................................................................... 26
Discussion ............................................................................................................................... 33
Limitations .......................................................................................................................... 35
Future Research .................................................................................................................. 36
Conclusion .............................................................................................................................. 37
References ............................................................................................................................... 39
Submarine Pitchers 5
Abstract
Background: In order to remain healthy while performing at a high level, athletes must
exercise in a manner that is functional and translatable to the movement being produced
during sport. In order to accomplish this, exercises are often modified to meet the specific
demands of different sporting activities. Purpose: Although many studies have been
performed on several aspects of baseball pitching, few studies have focused on the submarine
pitcher. This pilot study investigated the difference in the activation patterns of select
muscles for subjects conducting two exercises: the cable retraction with external rotation
exercise and the modified version of the same exercise, which had been tailored to the
submarine pitcher. The following research was performed to advance the literature devoted
to the specific needs of submarine pitchers, and to raise awareness on the lack of literature
devoted to this style of throwing. Subjects: 16 healthy males ages 18-35 with previous high
school, college, and/or professional baseball experience participated in this study. Methods:
Each subject was observed performing five repetitions of the two exercises, while motion and
muscle activation patterns of the posterior deltoid, the infraspinatus, the middle trapezius,
and the lower trapezius were captured using the Qualisys Motion Capture System in
conjunction with the Noraxon SEMG system. Results: No significant differences were found
between the two exercises in terms of muscle activation patterns of the four muscles being
studied. A positive correlation was found between the muscle activation patterns of the two
exercises, indicating that both exercises may accomplish the same goal when it comes to
strengthening the four targeted muscles. A significant difference was found in the angle of
abduction in which peak muscle activation occurred for the posterior deltoid (13°), the
middle trapezius (17°), and lower trapezius (14°).
Submarine Pitchers 6
Introduction
The motion of throwing a baseball is widely considered one of the most dynamic
and demanding motions of the human body (Fleisig, Andrews, Dillman, & Escamilla,
1995). Overhead throwing places an extreme amount of stress on the structures of the
shoulder at end ranges of motion. When pitching, the internal torque of the shoulder at
the glenohumeral joint during arm acceleration has been reported to reach 10,000°/sec,
and the distraction force placed on the glenohumeral joint during arm deceleration has
been reported to reach 947 N (Pretz, 2004). As a result of the stresses that are placed on
the glenohumeral joint, and the inherent instability of the glenohumeral joint, pitching
accounts for 75% of all collegiate baseball injuries, with rotator cuff tendonitis being the
leading injury (Scher, Anderson, Weber, Bajorek, Rand, & Bey, 2010). In order to pitch a
baseball without causing injury to the upper extremity, the athlete must have adequate
strength, endurance, power, and neuromuscular control of the involved musculature. A
goal of sports medicine clinicians is to decrease the incidence of injury and maximize
performance by prescribing exercises that maximize these attributes (Carter, Kaminski,
Douex, Knight, & Richards, 2007). Therefore, it is imperative clinicians continue to
conduct research and determine the most effective methods of developing the upper
extremities of pitchers to prepare them to address the demands associated with throwing a
baseball. It is also vital to acknowledge the current lack of literature regarding
biomechanics and muscle activation of the unconventional baseball pitcher, specifically
the underhand or submarine pitcher, and appropriate training methods for these athletes.
Two factors determine an individual’s style of pitching. These include the lateral
trunk flexion angle at ball release and the amount of shoulder abduction of the throwing
Submarine Pitchers 7
arm at ball release (Truedson, Sexton, & Pettitt, 2012). There are four described styles of
pitching, which are loosely defined based on the factors stated above. These include the
overhand, sidearm, three-quarter, and submarine pitching styles (Figure 1). Pitchers are
labeled as overhand style pitchers when there is significant trunk side flexion
contralateral to the throwing arm and the throwing arm is angled vertically from the
ground during ball release. Sidearm pitchers are characterized by having no lateral trunk
flexion during release and roughly 90° of shoulder abduction which creates an arm angle
horizontal to the ground during ball release. The three-quarter pitcher is given this label
when the arm angle falls in-between these two categories, roughly three-quarters of the
way from a horizontal plane to a vertical plane, with minimal lateral trunk flexion
present. Submarine style pitchers are much less common than the other three styles. The
submarine pitcher laterally flexes the trunk towards the throwing side and abducts the
glenohumeral joint less than 90° during ball release. The resulting motion can give the
impression that the pitcher is throwing the ball in an underhand fashion (Matsuo, Takada,
Matsumoto & Saito, 2000; Whiteley, 2007). Submarine throwing mechanics allow for
the pitcher to release the baseball from the ball’s bottom two-thirds, thus creating a
downward or “topspin” on the ball, as apposed to the upward or “backspin” which is
created during an overhand pitch. This topspin is presumed to cause the fastball to sink
to a much greater degree than the other three styles of pitching (Pavlovich, 2011).

Submarine Pitchers 8
Figure 1. Types of Pitching Styles.
Adapted from “Biomechanical Characteristics of Sidearm and Underhand Baseball Pitching: Comparison with Those of Overhand and Three-quarter Pitching”, by Matsuo, T., Takada, Y., Matsumoto, T., Saito, K., 2000. Japanese Journal of Biomechanics in Sports and Exercise, 4, 245-252.
The researchers found limited evidence based research that focused on the
submarine pitcher; two studies have mentioned some differences in throwing
biomechanics for submarine pitchers when compared to overhand and three-quarter
pitchers (Matsuo et al., 2000; Matsuo et al., 2003). Matsuo et al. (2000) compared ball
release height, pitch velocity, lateral trunk tilt, glenohumeral abduction, and peak elbow
varus torque between two submarine pitchers and thirteen overhand and three-quarter
pitchers. The limited sample size did not allow for significant conclusions to be drawn
from this study, but it was noted that the submarine pitchers had a lower ball release
height, a lower pitch velocity, less glenohumeral abduction, decreased elbow varus
torque, and a lateral trunk tilt of 10-25° in the opposite direction of the lateral trunk tilt of
the overhand and three-quarter pitchers. In a later study by Matsuo et al. (2002), nine
overhand and three-quarter pitchers were compared to two submarine pitchers. Results
demonstrated a small decrease in peak wrist velocity, a large decrease in glenohumeral
abduction, and an increase in peak elbow varus torque for the submarine pitchers when
compared to the overhand and three-quarter pitchers. A limitation of the study was
Submarine Pitchers 9
sample size, as the sample was too small to provide researchers with statistically
significant information.
Phases of Throwing
Dillman, Fleisig, & Andrews (1993) split the overhead pitching motion up into six
phases. Regardless of style of pitching, the phases of the throwing motion remain the
same for all baseball pitchers. The biomechanics and kinematics of the conventional
baseball pitcher during these six phases have been extensively studied since the early
1980’s. Phase 1, known as the windup, begins when the pitcher steps backward with his
stride foot, rotates his body to the throwing side, shifts his weight to the supporting foot,
and lifts his stride foot. Phase 2, stride, is initiated when the stride foot is moved toward
the plate and the ball is brought out of the glove. As the stride foot moves closer to the
plate, the throwing arm is moved in a rhythmic down and then upward motion to ensure
that the upper and lower body are synchronized properly when the stride foot contacts the
ground. Phase 3, cocking, occurs once the stride foot contacts the ground. During this
phase, the hips rotate towards the plate, followed by trunk rotation and extension, elbow
flexion, and shoulder external rotation. Phase 4, arm acceleration, happens when maximal
external rotation is reached, and the arm begins to accelerate forward through shoulder
internal rotation, horizontal adduction, and elbow extension, until the ball is released.
Phase 5, arm deceleration, occurs when the posterior shoulder rotator cuff muscles
contract eccentrically to slow down the internal rotation torque created during the
acceleration phase. Elbow extension also happens during this phase. The 6th and final
phase, the follow-through, allows the pitcher to decelerate the forward momentum placed
Submarine Pitchers 10
on the entire body by shifting all weight to the stride foot and allowing the back foot to
leave the mound and fall in front of the stride foot (Dillman, Fleisig, & Andrews, 1993).
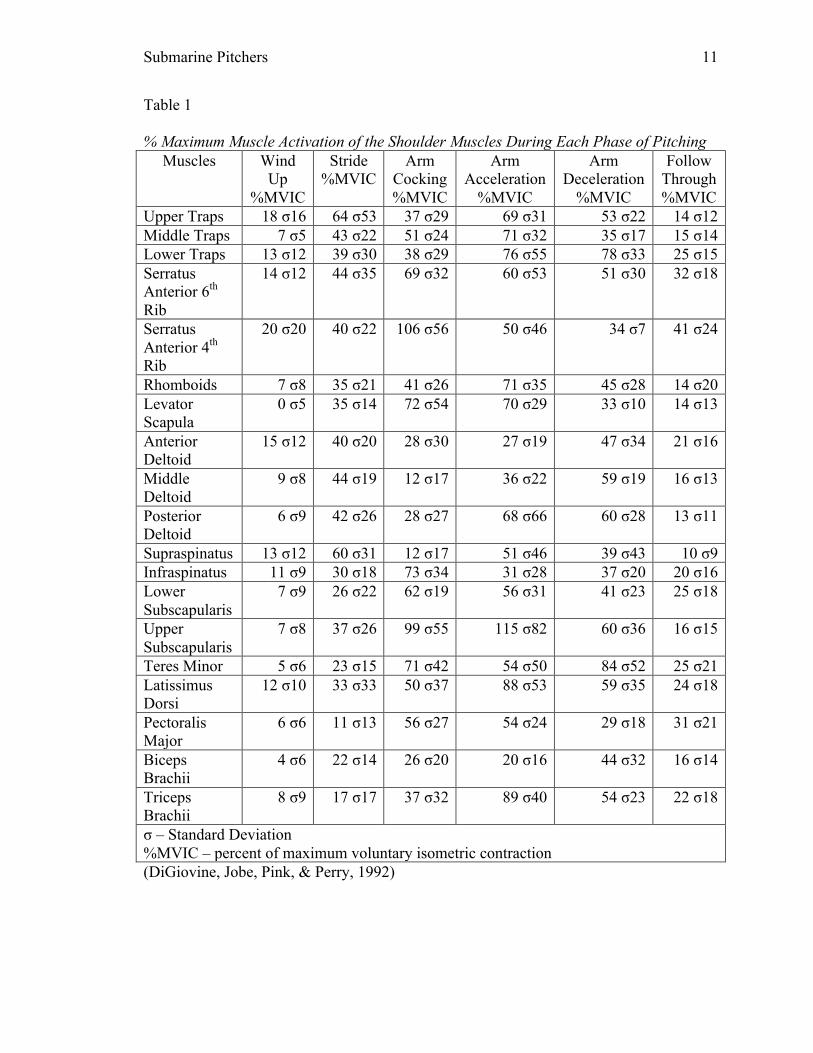
Tables 1 and 2 describe the biomechanics of the glenohumeral joint and the
muscle firing patterns that occur during the baseball pitch. With the exception of the
anterior deltoid, every muscle involved in glenohumeral and scapulothoracic motion
contracts to over 50% of their maximum voluntary isometric contractions at some phase
during the throwing motion, further illustrating the extremely dynamic nature of throwing
a pitch (see Table 1). Knowing this information can help offer clinicians an improved
sense of understanding of which muscles are activated in specific glenohumeral joint
positions during a pitch. Knowledge of this information could enable clinicians to
practice in an evidenced based manner, fostering accurate and efficient diagnoses and
treatments of baseball pitchers. Limited research was found to provide this kind of
information for the submarine pitcher to date; which could result in limited evidence
based clinical practices when training or treating the submarine pitcher. Continued
research focused on this style of throwing should be conducted, as the research findings
could potentially have a profound impact on how submarine pitchers are to be treated
compared to the rest of the population of pitchers.
Submarine Pitchers 11
Table 1 % Maximum Muscle Activation of the Shoulder Muscles During Each Phase of Pitching
Muscles Wind Up
%MVIC
Stride %MVIC
Arm Cocking %MVIC
Arm Acceleration
%MVIC
Arm Deceleration
%MVIC
Follow Through %MVIC
Upper Traps 18 σ16 64 σ53 37 σ29 69 σ31 53 σ22 14 σ12 Middle Traps 7 σ5 43 σ22 51 σ24 71 σ32 35 σ17 15 σ14 Lower Traps 13 σ12 39 σ30 38 σ29 76 σ55 78 σ33 25 σ15 Serratus Anterior 6th Rib
14 σ12 44 σ35 69 σ32 60 σ53 51 σ30 32 σ18
Serratus Anterior 4th Rib
20 σ20 40 σ22 106 σ56 50 σ46 34 σ7 41 σ24
Rhomboids 7 σ8 35 σ21 41 σ26 71 σ35 45 σ28 14 σ20 Levator Scapula
0 σ5 35 σ14 72 σ54 70 σ29 33 σ10 14 σ13
Anterior Deltoid
15 σ12 40 σ20 28 σ30 27 σ19 47 σ34 21 σ16
Middle Deltoid
9 σ8 44 σ19 12 σ17 36 σ22 59 σ19 16 σ13
Posterior Deltoid
6 σ9 42 σ26 28 σ27 68 σ66 60 σ28 13 σ11
Supraspinatus 13 σ12 60 σ31 12 σ17 51 σ46 39 σ43 10 σ9 Infraspinatus 11 σ9 30 σ18 73 σ34 31 σ28 37 σ20 20 σ16 Lower Subscapularis
7 σ9 26 σ22 62 σ19 56 σ31 41 σ23 25 σ18
Upper Subscapularis
7 σ8 37 σ26 99 σ55 115 σ82 60 σ36 16 σ15
Teres Minor 5 σ6 23 σ15 71 σ42 54 σ50 84 σ52 25 σ21 Latissimus Dorsi
12 σ10 33 σ33 50 σ37 88 σ53 59 σ35 24 σ18
Pectoralis Major
6 σ6 11 σ13 56 σ27 54 σ24 29 σ18 31 σ21
Biceps Brachii
4 σ6 22 σ14 26 σ20 20 σ16 44 σ32 16 σ14
Triceps Brachii
8 σ9 17 σ17 37 σ32 89 σ40 54 σ23 22 σ18
σ – Standard Deviation %MVIC – percent of maximum voluntary isometric contraction (DiGiovine, Jobe, Pink, & Perry, 1992)
Submarine Pitchers 12
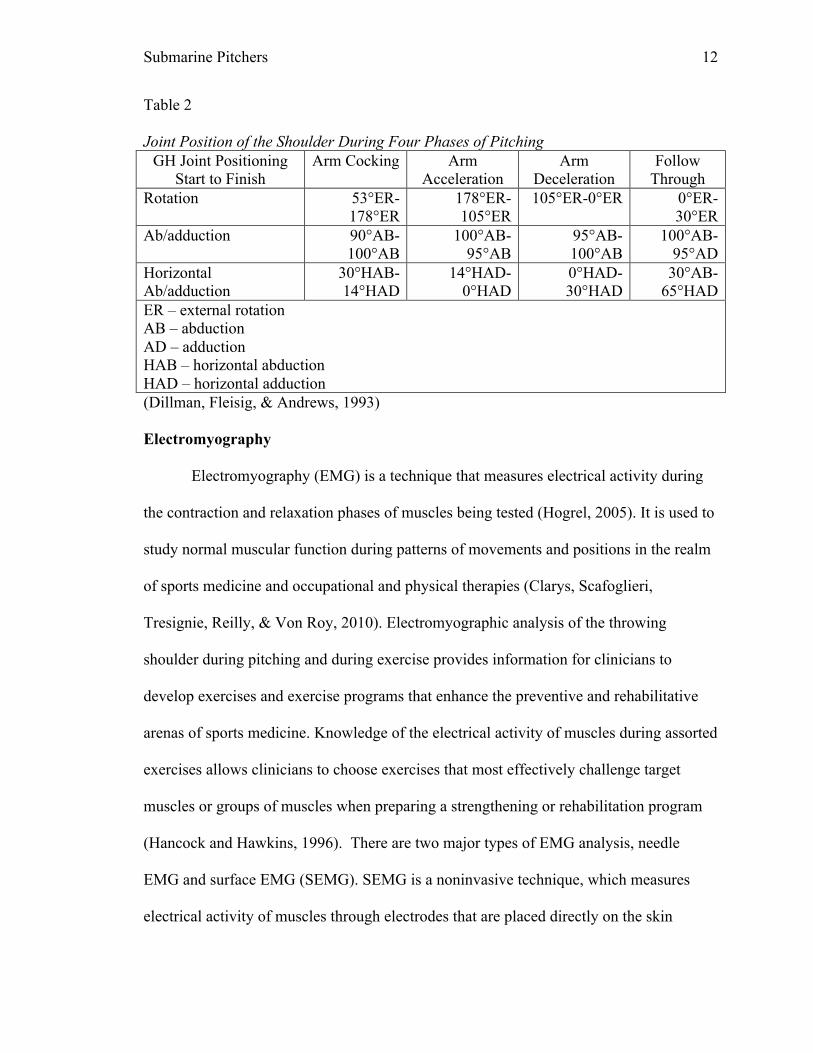
Table 2 Joint Position of the Shoulder During Four Phases of Pitching
GH Joint Positioning Start to Finish
Arm Cocking Arm Acceleration
Arm Deceleration
Follow Through
Rotation 53°ER-178°ER
178°ER-105°ER
105°ER-0°ER 0°ER-30°ER
Ab/adduction 90°AB-100°AB
100°AB-95°AB
95°AB-100°AB
100°AB-95°AD
Horizontal Ab/adduction
30°HAB-14°HAD
14°HAD-0°HAD
0°HAD-30°HAD
30°AB-65°HAD
ER – external rotation AB – abduction AD – adduction HAB – horizontal abduction HAD – horizontal adduction (Dillman, Fleisig, & Andrews, 1993) Electromyography
Electromyography (EMG) is a technique that measures electrical activity during
the contraction and relaxation phases of muscles being tested (Hogrel, 2005). It is used to
study normal muscular function during patterns of movements and positions in the realm
of sports medicine and occupational and physical therapies (Clarys, Scafoglieri,
Tresignie, Reilly, & Von Roy, 2010). Electromyographic analysis of the throwing
shoulder during pitching and during exercise provides information for clinicians to
develop exercises and exercise programs that enhance the preventive and rehabilitative
arenas of sports medicine. Knowledge of the electrical activity of muscles during assorted
exercises allows clinicians to choose exercises that most effectively challenge target
muscles or groups of muscles when preparing a strengthening or rehabilitation program
(Hancock and Hawkins, 1996). There are two major types of EMG analysis, needle
EMG and surface EMG (SEMG). SEMG is a noninvasive technique, which measures
electrical activity of muscles through electrodes that are placed directly on the skin
Submarine Pitchers 13
(Hogrel, 2005). Needle EMG assesses the same electrical activity through thin needle
electrodes, which are inserted through the skin and directly into the belly of the muscle
being assessed. Unlike the needle electrode, which penetrates the muscular tissue and
permits the detection of the virtually undistorted myoelectric signal, surface electrodes
detect the signal only after filtering through all the biological tissues between the many
signal sources (i.e. the activated muscle fibers) as well as filtering through the interaction
of other electrodes placed on the skin. Because of this, the validity of the SEMG has been
questioned, and tested in comparison to needle EMG. One study observed the accuracy of
SEMG signals coming from the vastus intermedius muscle compared to needle EMG
signal of the same muscle. The researchers found no significant differences between the
readings of the invasive procedure (needle EMG) and non-invasive procedure (SEMG)
when testing the vastus intermedius muscle. They concluded that SEMG is a valid
instrument that can be used to accurately determine the electrical activity of select
muscles. This same study acknowledged that proper electrode placement is vital to
obtaining accurate and valid SEMG readings, especially with muscles that have very
small superficial areas (Watanabe & Akima, 2011). Another study was conducted to
determine the reliability of SEMG readings for upper extremity muscles. This study was
conducted with 30 healthy subjects participating in 10 different exercises to discover
which high-intensity exercises produce the greatest level of SEMG activity of the
trapezius and serratus anterior muscles. The researchers found the reliability of the
SEMG recordings to be 0.91- 0.98 when muscles worked as prime movers, with the
exclusion of the upper trapezius where reliability was found to be 0.81 – 0.89, concluding
that using SEMG to detect the muscle activity of upper extremity muscles is highly to
Submarine Pitchers 14
moderately highly reliable (Ekstrom, Donatelli and Soderburg, 2003).
SEMG does have some accuracy concerns, which are mostly a result of the
techniques employed by examiners. The conduction properties of biological tissues may
cause interference; therefore skin preparation, electrode placement, and measurement
protocols must be performed consistently to gather data that is accurate and consistent
(Hogrel, 2005). There is limited research available that has been focused on the
relationship of human body composition, the anatomical variation of cutaneous and
subcutaneous adipose patterning, and the effects they have on the accuracy of SEMG
readings (Clarys et al., 2010). However, research has described the best way to prepare
the skin for electrode placement. (1) If the skin is dry, place a moist tissue soaked with
water over the target area. (2) If the skin is oily, rub it with alcohol. (3) Whatever the
condition of the skin, it is important to keep the skin impedance as low as possible by
rubbing it with a cotton swab to remove dead cells. (4) Rub in conductive gel and dry the
skin carefully where the electrode will be placed (Blanc and Dimanico, 2010).
The noninvasiveness and decrease in risk of injury made SEMG the technique of
choice for this study as opposed to needle EMG. The SEMG technique can also expedite
the research process due to the simplistic and efficient manner to which the electrodes
can be applied to the subjects.
Motion Analysis
The addition of motion analysis technology to the research and clinical arenas
made the study of human motion more accessible while maintaining objectivity (Vander
Linden, Carison, & Hubbard, 1992). Several motion analysis systems use a computer
based software system in combination with cameras designed to capture the signals
Submarine Pitchers 15
transmitted from special sensors strategically placed on the subject resulting in the
capture of human motion providing an objective picture of joint kinematics in real time
(Tucker et al., 2008). The use of three-dimensional imaging is an invaluable tool for
quantifiable evaluation of movement in all planes of motion (Murphy, Sunnerhagen,
Johnels, & Willen, 2006). Surface electromyography and motion analysis technology can
be used in conjunction as a means to measure muscle activation via SEMG in real-time
with accurate knowledge of joint motion and joint position during muscle action.
Purpose
It is common in physical therapy for exercises to be modified to meet the needs of
each individual patient. An article written by Truedson, Sexton, and Pettitt (2012)
proposed that exercises should be tailored to meet the sport specific needs of submarine
pitchers. To the knowledge of the researchers, this is the only published article that
discussed this topic. It described two exercises commonly used for strengthening and
rehabilitation: the kneeling deceleration exercise and the cable retraction with external
rotation (ER) exercise. It explained how these exercises were modified to meet the needs
of the submarine pitcher. This raised the question of whether or not the modifications are
successful at altering muscle recruitment patterns to make these exercises more beneficial
to this population of pitchers. The exercise studied during this experiment was the cable
retraction with external rotation (ER). The purpose of this study was to determine if
muscle recruitment patterns differ during the modified cable retraction with ER exercise
compared to when the exercise is conducted in the traditional manner.
Submarine Pitchers 16
Research Question
Was there a difference in muscle activation for patients conducting the modified
cable retraction with ER exercise when compared to performing the traditional method of
this exercise?
Hypothesis
In order to test the research question, the following hypothesis was developed.
HO: There was no significant difference in muscle recruitment patterns when comparing
the modified form of the exercise to the traditional form of the exercise.
HA: There was a significant difference in muscle recruitment patterns when comparing
the two methods of the exercise.
Methods
This study was a pilot study intended to address two major objectives. The
researchers aimed to determine if there were differences in muscle activation between
two similar upper extremity exercises, and also aimed to raise awareness of the lack of
literature that exists on submarine pitchers and to stimulate interest in this subject. The
independent variables in this study were the two different exercises, the cable retraction
with external rotation exercises, and the modified cable retraction with external rotation
exercise. The dependent variables were the muscle activity readings of each individual
muscle and the angle of glenohumeral abduction at peak EMG activity. The particular
muscles being observed included; the middle trapezius, lower trapezius, posterior deltoid,
and infraspinatus muscles. There were several reasons why these muscles were observed.
For one, these are superficial muscles that can readily be studied using SEMG (Bitter el
al., 2007; Kibler, Sciascia, Uhi, Tambay, & Cunningham, 2008; Marta et al., 2013).
Submarine Pitchers 17
Another reason is that the traditional method of the cable retraction with ER exercise is
designed to target the middle trapezius and rhomboids, the lower trapezius, and the
posterior rotator cuff (Paine & Voight, 2013). The posterior deltoid was studied due to its
high MVIC readings during the deceleration phase of throwing, as well as its high MVIC
readings during exercises involving horizontal abduction with the humerus in external
rotation (DiGiovine et al., 2007; Marta et al., 2013). The infraspinatus was studied due to
its importance as a dynamic stabilizer of the glenohumeral joint during the throwing
motion. One of the major causes for shoulder injury in the overhand thrower is muscle
imbalance between the internal rotators of the glenohumeral joint (subscapularis,
pectoralis major, latissimus dorsi, and teres major) that forcefully internally rotate the
humerus during arm acceleration, and the external rotators (infraspinatus and teres minor)
that work to overcome the internal rotation torque to decelerate the humerus. Due to the
role of the infraspinatus as a decelerator and major dynamic stabilizer of the
glenohumeral joint, it is important that strengthening and rehabilitative exercises be
conducted to target this muscle. Weakness of the infraspinatus can cause an increase in
humeral head translation during throwing, an increase the risk of subluxation of the
humeral head, and can lead to shoulder pain, impairment, and disability. Along with
glenohumeral stability, throwing also requires a significant amount of scapular stability.
The middle and lower trapezius musculature were studied due to their roles as scapular
stabilizers. These muscles support and control the scapula in an effort to provide a stable
glenoid, which enables the glenohumeral muscles to maintain optimal length-tension
relationships during throwing (Donatelli, et al., 2000).
Submarine Pitchers 18
Subjects
Sixteen male volunteers were recruited from the student body of a local university
and from local minor league baseball teams by means of convenience sampling. The
inclusion criteria consisted of males ages 18-35, a history of participation in the sport of
baseball at least at the high school level, no history of elbow or shoulder surgery in the
past 2 years, no electrode adhesive allergies, no history of shoulder instability, no history
of shoulder or elbow pain in the past 6 months, no participation is shoulder or elbow
rehabilitation is the past 6 months, and no participation in activities that could fatigue the
upper extremities 24 hours prior to the study. Therefore, the exclusion criteria consisted
of being outside the age range of 18-35, female, no history of participation in baseball at
least a the high school level, history of elbow or shoulder surgery in the past 2 years,
electrode adhesive allergies, history of shoulder instability, history of shoulder or elbow
pain or rehab in the past 6 months, failure to refrain from upper extremity fatiguing
exercises 24 hours prior to the study, unsafe resting heart-rate or blood pressure on the
day of the study, and any other contraindications to exercise as indicated on the medical
screening form or observed by the researchers. No females were included due to the fact
most baseball pitchers are male, hence male only participation provides a more accurate
sample of the population being studied. To ensure the level of wellness of the research
participants, all members involved filled out a PAR-Q Health/Medical History
Questionnaire. Participants were instructed not to participate in any activities that may
fatigue the muscles of the upper extremity at least 24 hours before testing. To ensure the
participants followed the research protocol of no activities that would fatigue the muscles
of the shoulder, all participants filled out an activity log the day before the study, which
Submarine Pitchers 19
was reviewed by the researchers prior to data collection. The participants provided
written informed consent and the Florida Gulf Coast University Institutional Review
Board approved this study.
Instrumentation
SEMG via the Noraxon system and the Qualisys motion capture system were
integrated together to establish a means to measure muscle activation while gaining
insight to the position of the upper extremity and the line of action of the targeted
muscles. The combination of the two systems provided a failsafe during data collection
and analysis. The incorporation of the two systems allowed the researchers to eliminate
erroneous data collected when an exercise was performed in the wrong plane. By
identifying exercises performed in the proper manner and eliminating those that were not,
the researchers eliminated a potential skew of the data and facilitated a more accurate
depiction of how the two exercises compared to one another.
The researchers followed the electrode placement utilized by Kibler, Sciascia,
Uhi, Tambay, and Cunningham (2008) who performed electromyographic analysis of
specific exercises for scapular control in early phases of shoulder rehabilitation. The
lower trapezius electrodes were located 2 cm apart at an oblique angle, 5 cm down from
the scapular spine, and outside the medial border of the scapula. The posterior deltoid
electrodes were positioned 2 cm apart, 2 cm inferior to the lateral border of the spine of
the scapula, and located at an oblique direction toward the humerus, running parallel with
muscle fiber direction. The middle trapezius electrodes were located between the spine of
the scapula and the spinous processes of the vertebrae at the same level, in accordance
with Marta et al. (2013). Placement of the infraspinatus muscle electrode was performed
Submarine Pitchers 20
in accordance with a study performed by Bitter el al. (2007) who studied the
contributions of the infraspinatus and deltoid during shoulder external rotation of subjects
with healthy shoulders. The infraspinatus electrode was positioned 4 cm below and
parallel to the scapular spine over the infrascapular fossa.
A trained practitioner placed Qualisys soft markers appropriately on each
landmark. Markers were placed on the acromions, medial and lateral epicondyles of the
humerus, radial and ulnar styloid processes, the sternum, the iliac crests, the posterior
superior iliac spines and the anterior superior iliac spines, the greater trochanters, the
medial and lateral femoral epicondyles, the medial and lateral malleoli, the calcaneous,
and the base of the 5th metatarsals. Cluster sets of markers were placed on the arms,
forearms, the lower back, the thighs, and the lower legs.
The complex movement of the exercises observed in this study provided some
challenges due to the difficulty of capturing the signal from each marker through the
entire motion of the activity. Therefore, it was imperative that the researchers in this
study established proper marker placement to ensure the capture of motion being
transmitted from all points of reference. For the purposes of this study, a segment link
model was developed through digitization of joint centers of the shoulder and
sternojugular notch.
Procedure
Each data collection session began with a system calibration of the Qualisys
motion capture system to ensure accurate and consistent data capture. Upon arrival, each
participant provided written informed consent. Each participant was asked to complete
the PAR-Q Health/Medical History Questionnaire while the researchers reviewed his 24-
Submarine Pitchers 21
hour activity log. Next, the participant’s resting heart rate and blood pressure were taken
to ensure the subject was safe to exercise. Each participant was educated on the research
procedures, and instructed how to perform the traditional and modified cable retraction
with ER exercises for shoulder rehabilitation and strengthening. Once the researchers
determined that it was safe for the subjects to participate the following scientific
procedures were performed. The skin was prepared for electrode placement and SEMG
electrodes were placed on each participant in accordance with the instructions outlined in
the methods section. Following electrode placement, each participant completed the
upper body dynamic warm-up that included trunk rotations, arm circles, arm swings, and
pendulums. The maximum voluntary isometric contractions (MVICs) of the
infraspinatus, lower and middle trapezius, and posterior deltoid muscles of each subject
were collected for normalization of the EMG data collected during this study. The
MVICs were collected utilizing standard manual muscle testing (MMT) techniques
described by Kendall, McCreary, Provance, Rodgers, and Romani (2005). Two
researchers performed MVIC capture; one researcher performed the muscle testing
procedure while the second researcher simultaneously captured the MVIC data via the
integrated Qualisys/Noraxon system. For each muscle being tested, the subjects were
placed in the appropriate position and the researcher applied a force through the upper
extremity of the subject for five seconds. Three trials were preformed for each muscle
tested. Data for the MVICs were collected from the trial that elicited the greatest MVIC
for each respected muscle. These MVICs were measured to provide a reference point for
the electrical activity of each muscle being studied. Within each subject, the EMG values
for each muscle during each exercise were normalized as a percentage of the highest
Submarine Pitchers 22
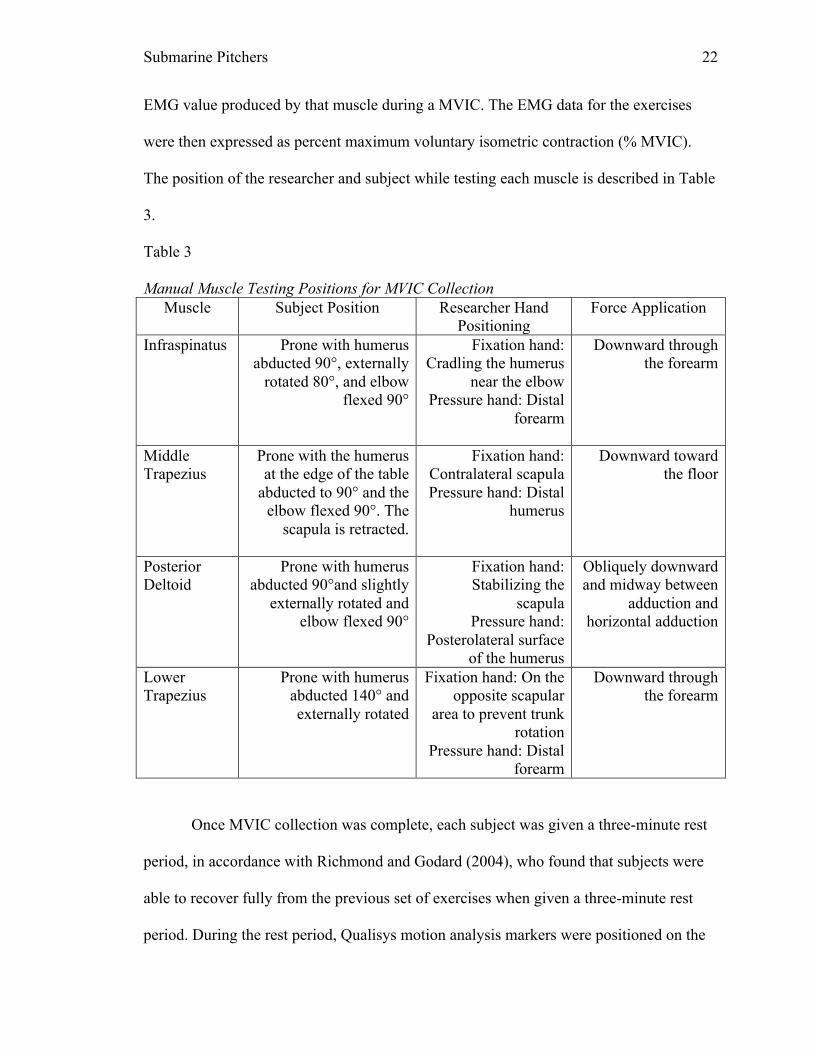
EMG value produced by that muscle during a MVIC. The EMG data for the exercises
were then expressed as percent maximum voluntary isometric contraction (% MVIC).
The position of the researcher and subject while testing each muscle is described in Table
3.
Table 3 Manual Muscle Testing Positions for MVIC Collection
Muscle Subject Position Researcher Hand Positioning
Force Application
Infraspinatus Prone with humerus abducted 90°, externally
rotated 80°, and elbow flexed 90°
Fixation hand: Cradling the humerus
near the elbow Pressure hand: Distal
forearm
Downward through the forearm
Middle Trapezius
Prone with the humerus at the edge of the table
abducted to 90° and the elbow flexed 90°. The
scapula is retracted.
Fixation hand: Contralateral scapula Pressure hand: Distal
humerus
Downward toward the floor
Posterior Deltoid
Prone with humerus abducted 90°and slightly
externally rotated and elbow flexed 90°
Fixation hand: Stabilizing the
scapula Pressure hand:
Posterolateral surface of the humerus
Obliquely downward and midway between
adduction and horizontal adduction
Lower Trapezius
Prone with humerus abducted 140° and externally rotated
Fixation hand: On the opposite scapular
area to prevent trunk rotation
Pressure hand: Distal forearm
Downward through the forearm
Once MVIC collection was complete, each subject was given a three-minute rest
period, in accordance with Richmond and Godard (2004), who found that subjects were
able to recover fully from the previous set of exercises when given a three-minute rest
period. During the rest period, Qualisys motion analysis markers were positioned on the
Submarine Pitchers 23
individual as described in the previous section. Next, each subject completed two model
captures: a static model and a dynamic model. Then, the subjects were re-educated on
how to conduct the exercises being tested, and each participant performed trial repetitions
of the exercises until the researchers were assured that the participant could conduct the
exercise correctly. Finally, each subject completed one set of 5 repetitions of the
traditional exercise. Each repetition was performed in four seconds (two seconds for the
concentric phase and two seconds for the eccentric phase) and in rhythm with a
metronome set at 90 beats per minute. The metronome was utilized to ensure that the
rhythm and speed in which the exercise was conducted was universal to all participants,
decreasing the variability of the muscle activation patterns between subjects. The
participant then rested for three minutes while the next exercise was explained and
demonstrated. Then the participant demonstrated the proper exercise technique and then
completed five repetitions of the modified exercise in the same manner as the previous
exercise. Data were captured for all five repetitions of each exercise. Repetitions two
through four were utilized from the data set and analyzed for the results of this study.
Exercise Descriptions
The exercises involved in the study were the cable retraction with external
rotation exercise and a modified version of the same exercise. The exercise was
performed using a cable pulley system set to a resistance of five pounds for each
participant. The resistance was set to five pounds because each participant was able to
perform multiple repetitions of the exercises at this weight with proper form and
technique.
Submarine Pitchers 24
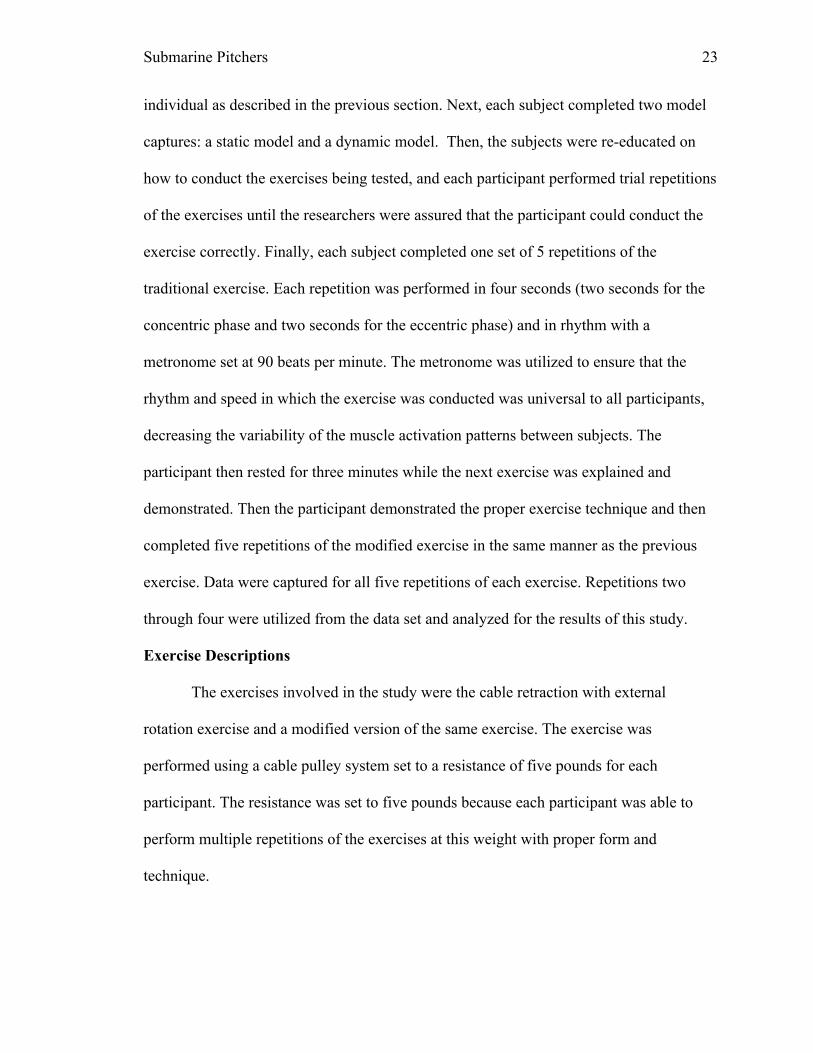
Cable retraction with external rotation. The cable retraction with external
rotation was performed using a cable column weight system with the handle at the height
of the participants mid tibia. The participant stood in front of the cable system with his
feet staggered in such a way in which he simulated the stance of a pitcher at ball release.
He then grasped the handle that was attached to the cable with the dominant hand. The
starting position of the shoulder and elbow consisted of slight glenohumeral internal
rotation, glenohumeral abduction of 90°, glenohumeral horizontal adduction of 20°, and
elbow flexion of approximately 20°. The trunk started in a forward flexed position. The
concentric phase of the exercise consisted of simultaneous trunk extension, glenohumeral
external rotation, horizontal abduction, scapular retraction, and slight elbow flexion. The
ending position of the exercise was full external rotation and horizontal abduction of the
glenohumeral joint, retraction of the scapula, and 70° of elbow flexion. The patient then
used an eccentric contraction to slowly reverse the motion until the arm has returned to
the starting position (Paine & Voight, 2013). The exercise is shown in figure 2.
Submarine Pitchers 25
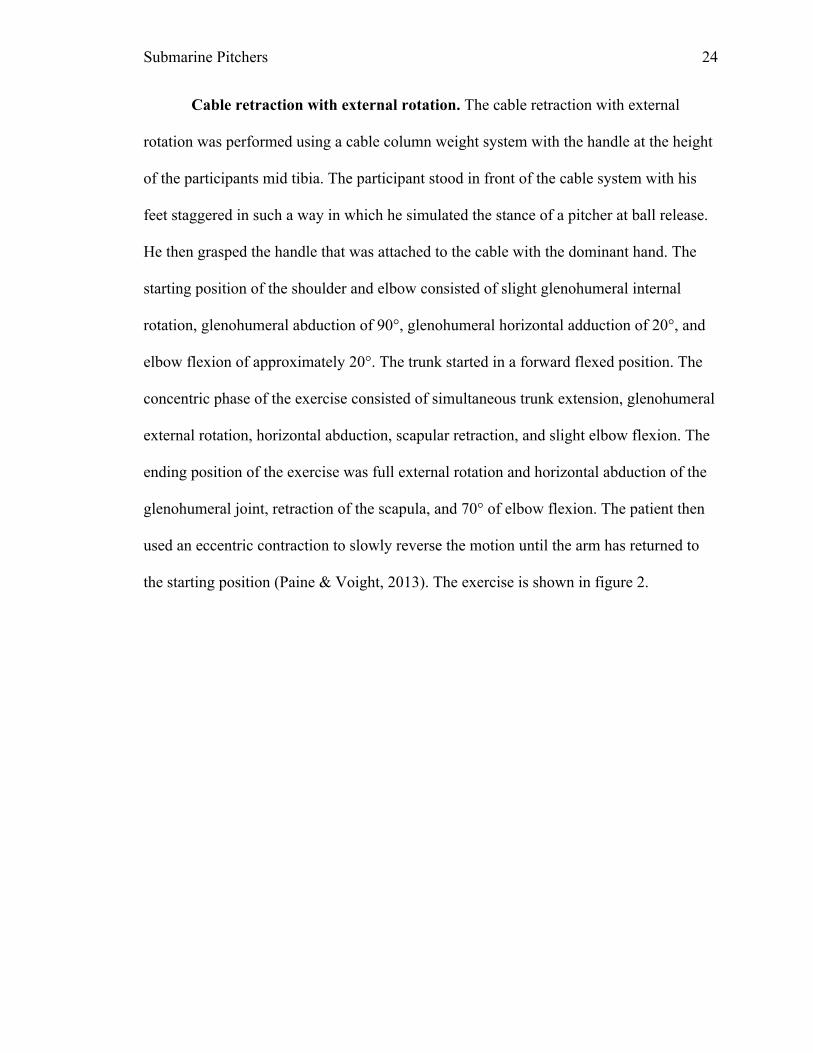
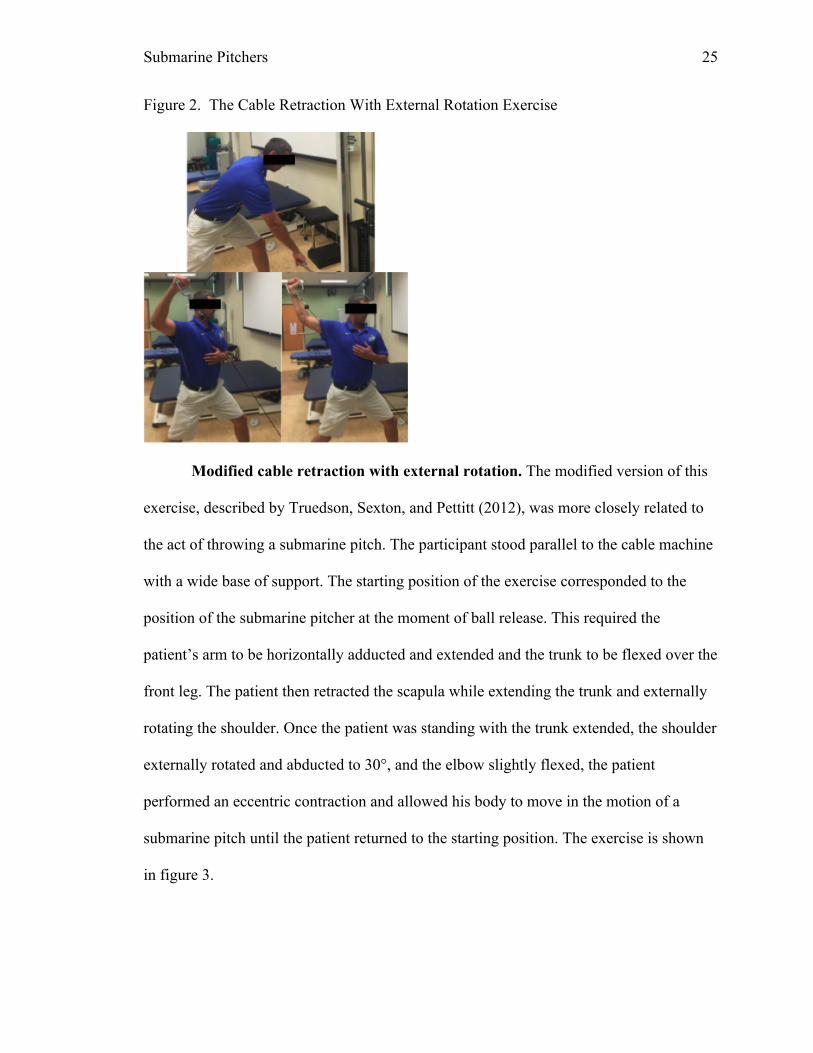
Figure 2. The Cable Retraction With External Rotation Exercise
Modified cable retraction with external rotation. The modified version of this
exercise, described by Truedson, Sexton, and Pettitt (2012), was more closely related to
the act of throwing a submarine pitch. The participant stood parallel to the cable machine
with a wide base of support. The starting position of the exercise corresponded to the
position of the submarine pitcher at the moment of ball release. This required the
patient’s arm to be horizontally adducted and extended and the trunk to be flexed over the
front leg. The patient then retracted the scapula while extending the trunk and externally
rotating the shoulder. Once the patient was standing with the trunk extended, the shoulder
externally rotated and abducted to 30°, and the elbow slightly flexed, the patient
performed an eccentric contraction and allowed his body to move in the motion of a
submarine pitch until the patient returned to the starting position. The exercise is shown
in figure 3.

Submarine Pitchers 26
Figure 3. The Modified Cable Retraction With External Rotation Exercise
Data Analysis
The data from this study compared peak muscle activity of the muscles being
studied between the two exercises described above. It also compared the angles of
abduction of the glenohumeral joint for when each muscle reached peak activity between
the two exercises. The data were recorded using the 3-D motion analysis system and
Visual 3D© in conjunction with the Noraxon surface EMG system. The IBM SPSS
statistics GRAD PACK 22.0 base program was used to analyze the data. A Paired
samples test was used to determine differences in peak muscle activity between the two
exercises, as well as the difference in the angle of glenohumeral abduction at the time of
peak muscle activity for the two exercises. A Pearson correlation coefficient was used to
determine if correlations in peak muscle activity were present between the two exercises,
as well as whether or not correlations in the angle of glenohumeral abduction at the time
of peak muscle activity for the two exercises were present.
Results
Data analysis revealed statistically significant correlations between the peak
muscle activities of the four select muscles when observing the SEMG of the two
Submarine Pitchers 27
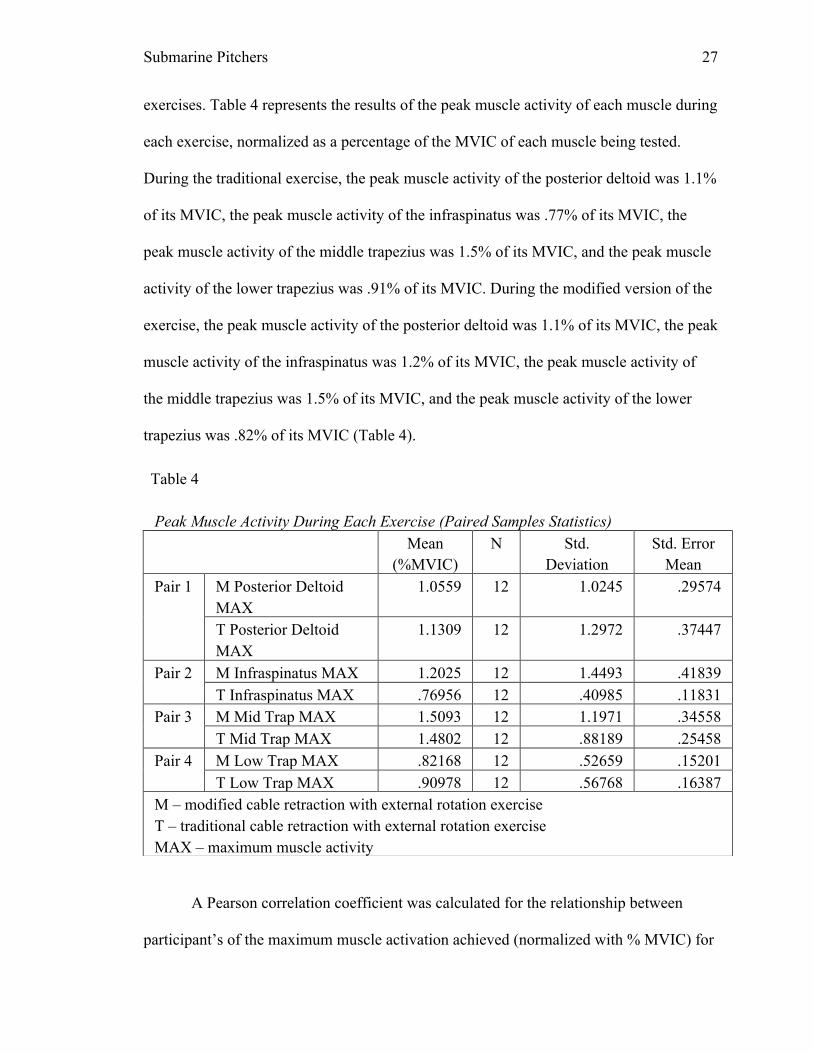
exercises. Table 4 represents the results of the peak muscle activity of each muscle during
each exercise, normalized as a percentage of the MVIC of each muscle being tested.
During the traditional exercise, the peak muscle activity of the posterior deltoid was 1.1%
of its MVIC, the peak muscle activity of the infraspinatus was .77% of its MVIC, the
peak muscle activity of the middle trapezius was 1.5% of its MVIC, and the peak muscle
activity of the lower trapezius was .91% of its MVIC. During the modified version of the
exercise, the peak muscle activity of the posterior deltoid was 1.1% of its MVIC, the peak
muscle activity of the infraspinatus was 1.2% of its MVIC, the peak muscle activity of
the middle trapezius was 1.5% of its MVIC, and the peak muscle activity of the lower
trapezius was .82% of its MVIC (Table 4).
A Pearson correlation coefficient was calculated for the relationship between
participant’s of the maximum muscle activation achieved (normalized with % MVIC) for
Table 4 Peak Muscle Activity During Each Exercise (Paired Samples Statistics) Mean
(%MVIC) N Std.
Deviation Std. Error
Mean Pair 1 M Posterior Deltoid
MAX 1.0559 12 1.0245 .29574
T Posterior Deltoid MAX
1.1309 12 1.2972 .37447
Pair 2 M Infraspinatus MAX 1.2025 12 1.4493 .41839 T Infraspinatus MAX .76956 12 .40985 .11831
Pair 3 M Mid Trap MAX 1.5093 12 1.1971 .34558 T Mid Trap MAX 1.4802 12 .88189 .25458
Pair 4 M Low Trap MAX .82168 12 .52659 .15201 T Low Trap MAX .90978 12 .56768 .16387
M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise MAX – maximum muscle activity
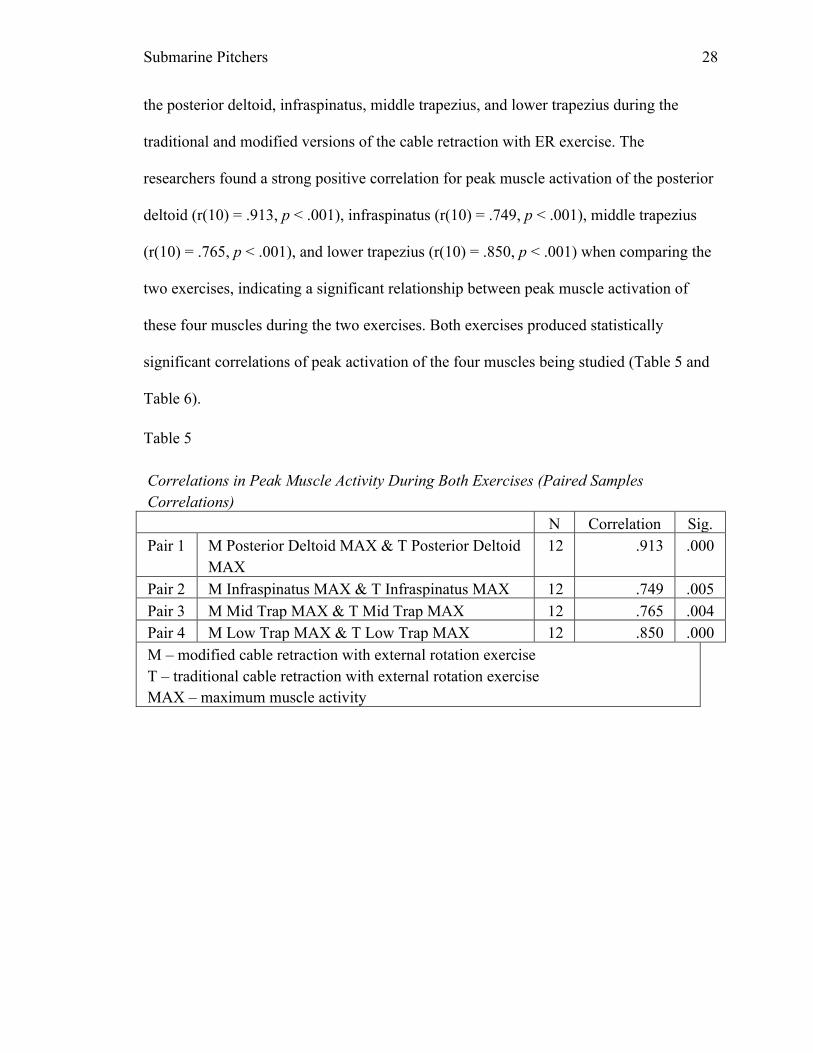
Submarine Pitchers 28
the posterior deltoid, infraspinatus, middle trapezius, and lower trapezius during the
traditional and modified versions of the cable retraction with ER exercise. The
researchers found a strong positive correlation for peak muscle activation of the posterior
deltoid (r(10) = .913, p < .001), infraspinatus (r(10) = .749, p < .001), middle trapezius
(r(10) = .765, p < .001), and lower trapezius (r(10) = .850, p < .001) when comparing the
two exercises, indicating a significant relationship between peak muscle activation of
these four muscles during the two exercises. Both exercises produced statistically
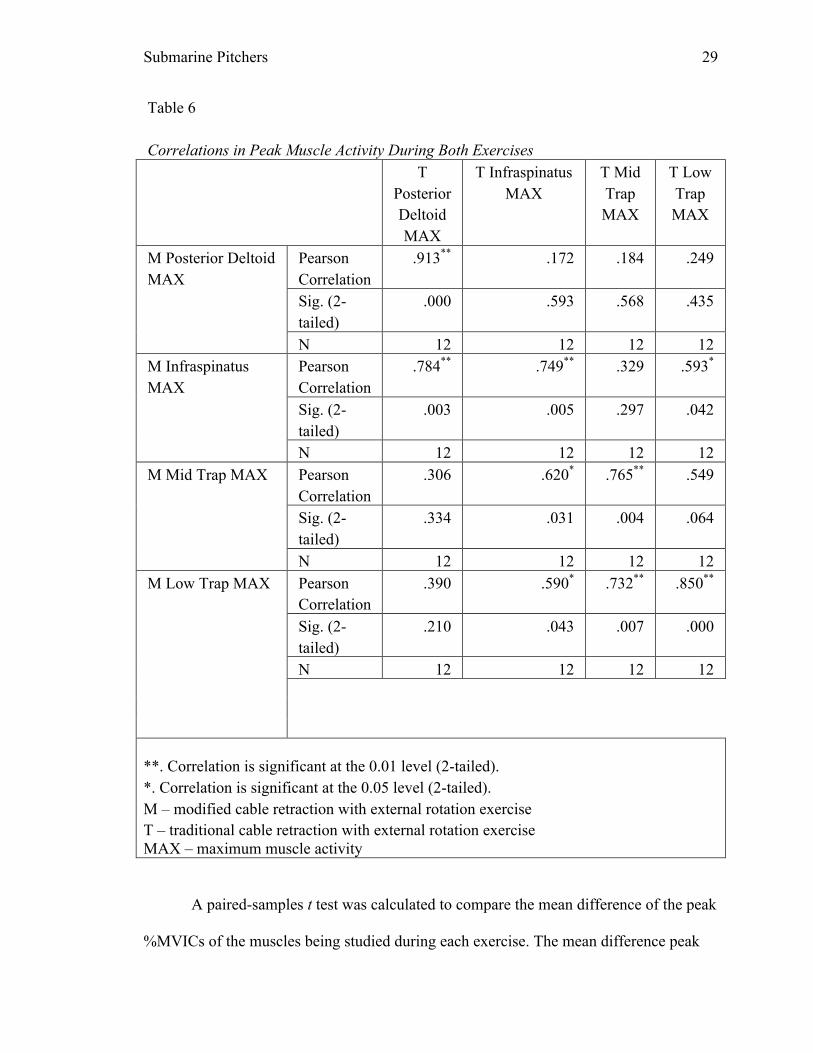
significant correlations of peak activation of the four muscles being studied (Table 5 and
Table 6).
Table 5 Correlations in Peak Muscle Activity During Both Exercises (Paired Samples Correlations) N Correlation Sig. Pair 1 M Posterior Deltoid MAX & T Posterior Deltoid
MAX 12 .913 .000
Pair 2 M Infraspinatus MAX & T Infraspinatus MAX 12 .749 .005 Pair 3 M Mid Trap MAX & T Mid Trap MAX 12 .765 .004 Pair 4 M Low Trap MAX & T Low Trap MAX 12 .850 .000 M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise MAX – maximum muscle activity
Submarine Pitchers 29
Table 6 Correlations in Peak Muscle Activity During Both Exercises T
Posterior Deltoid MAX
T Infraspinatus MAX
T Mid Trap MAX
T Low Trap MAX
M Posterior Deltoid MAX
Pearson Correlation
.913** .172 .184 .249
Sig. (2-tailed)
.000 .593 .568 .435
N 12 12 12 12 M Infraspinatus MAX
Pearson Correlation
.784** .749** .329 .593*
Sig. (2-tailed)
.003 .005 .297 .042
N 12 12 12 12 M Mid Trap MAX Pearson
Correlation .306 .620* .765** .549
Sig. (2-tailed)
.334 .031 .004 .064
N 12 12 12 12 M Low Trap MAX Pearson
Correlation .390 .590* .732** .850**
Sig. (2-tailed)
.210 .043 .007 .000
N 12 12 12 12
**. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed). M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise MAX – maximum muscle activity
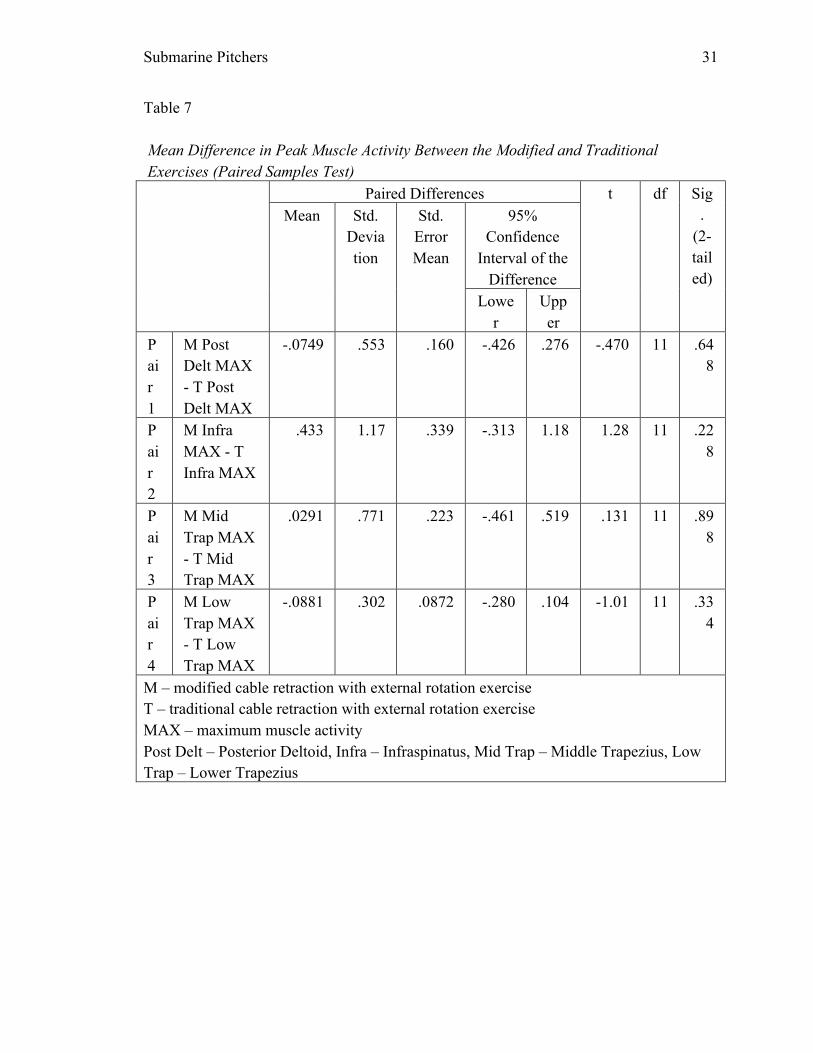
A paired-samples t test was calculated to compare the mean difference of the peak
%MVICs of the muscles being studied during each exercise. The mean difference peak
Submarine Pitchers 30
%MVIC between the two exercises was .0749 (sd = .5527) for the posterior deltoid,
.4329 (sd = 1.174) for the infraspinatus, .02914 (sd = .7711) for the middle trapezius, and
.08810 (sd = .3021) for the lower trapezius. The results indicated that there was no
significant difference between average peak muscle activation between the two exercises
with the four muscles being studied (Table 7).
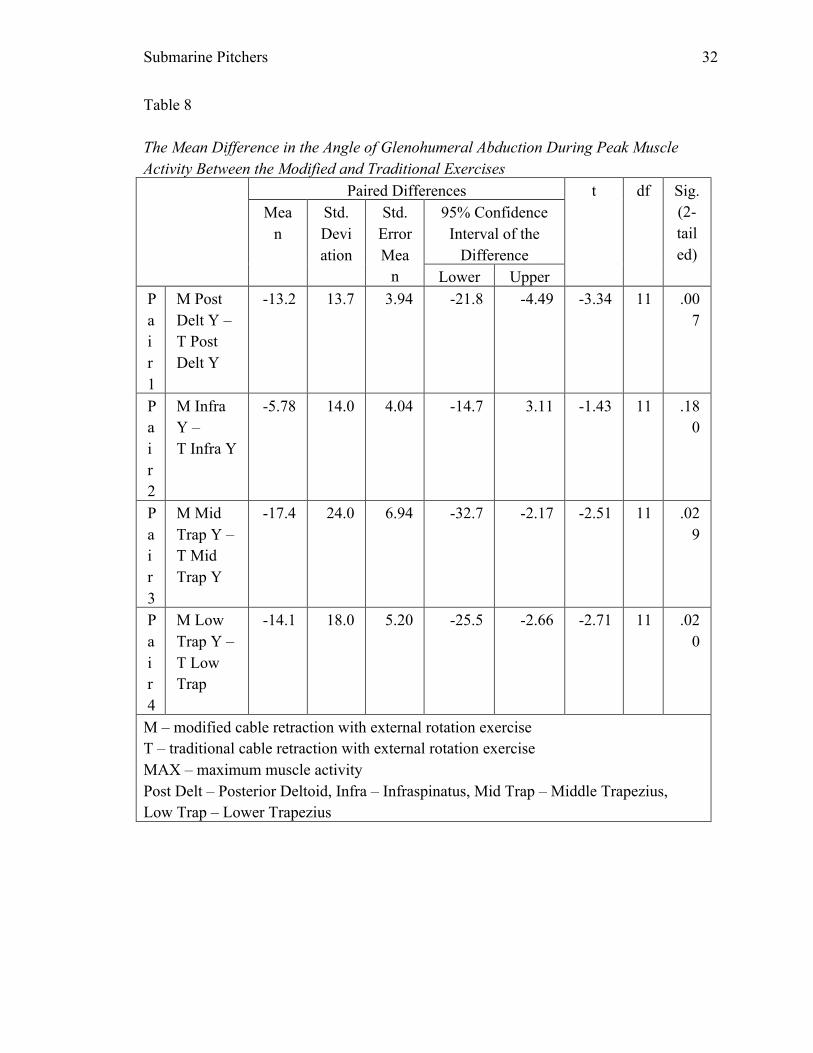
A paired-samples t test was calculated to compare the mean difference of the
glenohumeral abduction angle of the peak muscle activity of the muscles being studied
during each exercise. The angle of abduction was significantly less during the modified
exercise for the posterior deltoid (13.17°, sd = 13.66°), middle trapezius (17.45°, sd =
24.04°), and lower trapezius (14.10°, sd = 18.01°) (Table 8).
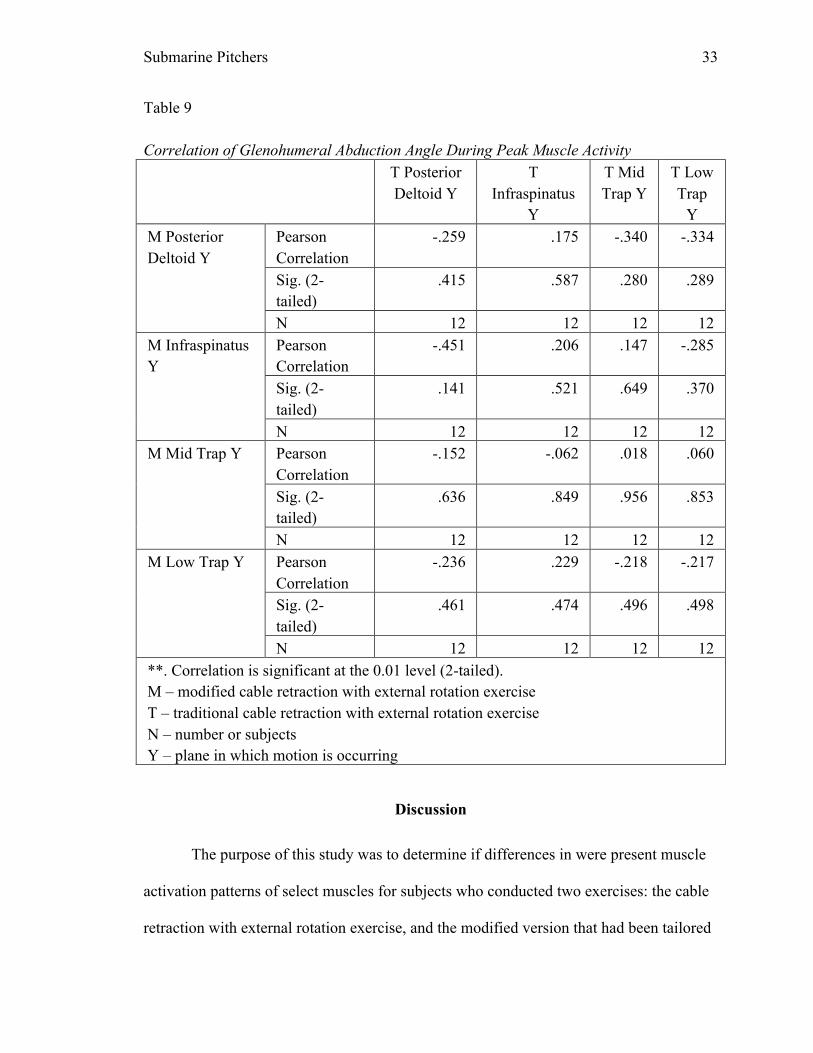
A Pearson correlation coefficient was calculated examining the relationship
between the glenohumeral abduction angles during the peak muscle activity of the
muscles being studied during each exercise. No strong or weak correlations were found
between the two exercises when comparing where peak muscle activation is occurring in
terms of glenohumeral abduction angles. This indicated that peak muscle activity of the
muscles being studied did not occur at the same level of glenohumeral abduction during
the modified version of the exercise, as it did during the traditional version of the exercise
(Table 9).
Submarine Pitchers 31
Table 7 Mean Difference in Peak Muscle Activity Between the Modified and Traditional Exercises (Paired Samples Test) Paired Differences t df Sig
. (2-tailed)
Mean Std. Deviation
Std. Error Mean
95% Confidence
Interval of the Difference
Lower
Upper
Pair 1
M Post Delt MAX - T Post Delt MAX
-.0749 .553 .160 -.426 .276 -.470 11 .648
Pair 2
M Infra MAX - T Infra MAX
.433 1.17 .339 -.313 1.18 1.28 11 .228
Pair 3
M Mid Trap MAX - T Mid Trap MAX
.0291 .771 .223 -.461 .519 .131 11 .898
Pair 4
M Low Trap MAX - T Low Trap MAX
-.0881 .302 .0872 -.280 .104 -1.01 11 .334
M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise MAX – maximum muscle activity Post Delt – Posterior Deltoid, Infra – Infraspinatus, Mid Trap – Middle Trapezius, Low Trap – Lower Trapezius
Submarine Pitchers 32
Table 8 The Mean Difference in the Angle of Glenohumeral Abduction During Peak Muscle Activity Between the Modified and Traditional Exercises Paired Differences t df Sig.
(2-tailed)
Mean
Std. Deviation
Std. Error Mea
n
95% Confidence Interval of the
Difference Lower Upper
Pair 1
M Post Delt Y – T Post Delt Y
-13.2 13.7 3.94 -21.8 -4.49 -3.34 11 .007
Pair 2
M Infra Y – T Infra Y
-5.78 14.0 4.04 -14.7 3.11 -1.43 11 .180
Pair 3
M Mid Trap Y – T Mid Trap Y
-17.4 24.0 6.94 -32.7 -2.17 -2.51 11 .029
Pair 4
M Low Trap Y – T Low Trap
-14.1 18.0 5.20 -25.5 -2.66 -2.71 11 .020
M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise MAX – maximum muscle activity Post Delt – Posterior Deltoid, Infra – Infraspinatus, Mid Trap – Middle Trapezius, Low Trap – Lower Trapezius
Submarine Pitchers 33
Table 9 Correlation of Glenohumeral Abduction Angle During Peak Muscle Activity T Posterior
Deltoid Y T
Infraspinatus Y
T Mid Trap Y
T Low Trap
Y M Posterior Deltoid Y
Pearson Correlation
-.259 .175 -.340 -.334
Sig. (2-tailed)
.415 .587 .280 .289
N 12 12 12 12 M Infraspinatus Y
Pearson Correlation
-.451 .206 .147 -.285
Sig. (2-tailed)
.141 .521 .649 .370
N 12 12 12 12 M Mid Trap Y Pearson
Correlation -.152 -.062 .018 .060
Sig. (2-tailed)
.636 .849 .956 .853
N 12 12 12 12 M Low Trap Y Pearson
Correlation -.236 .229 -.218 -.217
Sig. (2-tailed)
.461 .474 .496 .498
N 12 12 12 12 **. Correlation is significant at the 0.01 level (2-tailed). M – modified cable retraction with external rotation exercise T – traditional cable retraction with external rotation exercise N – number or subjects Y – plane in which motion is occurring
Discussion
The purpose of this study was to determine if differences in were present muscle
activation patterns of select muscles for subjects who conducted two exercises: the cable
retraction with external rotation exercise, and the modified version that had been tailored
Submarine Pitchers 34
to meet the demands of the submarine pitcher. As indicated in the results, no significant
differences were found between the two exercises in terms of muscle activation patterns
of the four muscles being studied, which supported the null hypothesis. However, there
was a strong correlation between peak muscle activation of the posterior deltoid,
infraspinatus, and middle and upper trapezius muscles during the two exercises (Tables
5&6). Truedson, Sexton, and Pettitt (2012) stated that in order to remain healthy while
performing at a high level, athletes must exercise in a manner that is functional and
translatable to the movement being produced during sport. The researchers’ findings in
this study indicated that the modified exercise was able to target the same shoulder
musculature as the traditional exercise, while the athlete was performing a functional
movement pattern that is concordant with the motion performed by the submarine
pitcher. Therefore, it may be more beneficial for the submarine pitcher to train using the
modified version of the exercise.
The researchers found differences in the glenohumeral abduction angle in which
peak muscle activation was occurring when the two exercises were compared. The angle
of abduction when peak muscle activity was occurring was significantly less during the
modified exercise (Table 9). A significant difference was found in the angle of abduction
in which peak muscle activation occurred for the posterior deltoid (13°), the middle
trapezius (17°), and lower trapezius (14°). This may warrant the utilization of this
exercise because it allowed for peak muscle activation to occur in a position that was less
likely to cause subacromial impingement than the traditional exercise. Park et al. (2003)
stated that when analyzing baseball pitchers, impingement occurs with the arm in 90° or
greater abduction, with movement into an internally rotated and horizontally adducted
Submarine Pitchers 35
position. Based on the results of this study, the modified cable retraction with external
rotation exercise is able to be used to train the posterior deltoid, middle trapezius, and
lower trapezius as efficiently as the traditional version, while decreasing the risk of an
exercise acquired impingement syndrome in the shoulder.
In summary, there were no differences found between the two exercises in terms
of peak muscle activation of the posterior deltoid, infraspinatus, and middle & lower
trapezius. However, there was a strong correlation between peak muscle activation of the
muscles being tested, as well as a significant difference in the angle of abduction in
which peak muscle activation occurred when performing the modified cable retraction
with external rotation exercise compared to the traditional exercise. The researchers of
this study deem that modifying the traditional exercise is unnecessary if the clinician is
targeting the four muscles tested in this study. However, it may be beneficial to the
submarine pitcher to perform the modified version of the exercise because it replicates
the submarine throwing motion while still exercising the targeted muscles as efficiently
and the traditional exercise. There is no evidence present to suggest that this exercise
meets the physiological demands of this activity, due to the currently existing gap in the
literature on the biomechanics and muscle activation patterns of the shoulder during a
submarine pitch.
Limitations
All aspects of this study were attempted to be controlled by the researchers.
However, there were still limitations to the study. The sample size of sixteen participants
is adequate for a pilot study, but it was too small for strong conclusions to be drawn from
this study. Also, each participant conducted the two exercises differently. The exercises
Submarine Pitchers 36
involved multiple joint motions and were complex in nature. They were difficult to
perform for some individuals, and no two participants performed each exercise exactly
the same. However, all subjects were able to perform the exercises adequately and within
the scope of this study. Extraneous variables could have affected the validity of the
results of the study and include the fact that two different clinicians were used to place
the Qualisys soft markers on the participants, and the Noraxon electrodes were placed on
each participant by means of vision and palpation.
Future Research
As previously stated, this study was meant to be a pilot study to increase the
scholarly interest in the submarine pitcher, and how exercises may be modified to create
more efficient training and rehabilitation routines for them. An important area in baseball
research that is currently lacking is the biomechanics and kinematics of the submarine
pitcher. Future research needs to be performed to determine the biomechanics and muscle
activation patterns of the submarine pitcher in order to develop a better understanding of
the physiological demands of this activity. This knowledge will aid clinicians in
developing appropriate exercise programs and techniques to train these athletes utilizing
evidenced based practices focused on function. Currently, when utilizing the modified
version of the cable retraction exercise, the thought that the exercise is targeting the
muscles needed for decelerating the arm of a submarine pitcher it is base solely on
theory, as there is inadequate evidence on the true physiological demands placed on the
soft tissues of these pitchers. One element of difference when comparing the throwing
motion of submarine pitcher and traditional is that there is a significant difference in the
angle abduction of the glenohumeral joint. Consequently, the forces applied the shoulder
Submarine Pitchers 37
during this activity must be researched to better serve this athletic population in order to
better train or rehabilitate these throwers through evidence based practice.
Conclusion
There are over thirty pitchers currently in professional baseball that are
considered to be submarine pitchers. Expert opinion theorizes that it is more popular in
the collegiate setting due to the effectiveness it can have on younger hitters who have
never seen pitching from this arm angle. This style of pitching, although rare, is prevalent
enough to warrant investigation into the biomechanics of the motion as well as the stress
it places on the shoulder, elbow, and spine. Although there is limited research focused on
the difference in stresses placed on the body between the overhand thrower and the
submarine thrower, clinicians must still be able to train and rehabilitate submarine
pitchers effectively. The results of the present study demonstrated that the modified cable
retraction with external rotation exercise could be as effective at training the posterior
shoulder musculature as the traditional version of the exercise, while training the athlete
in a motion functional to the athlete’s style of pitching. This is important, because in
order to decelerate the arm during throwing and prevent injury to the shoulder, the
posterior deltoid, infraspinatus, middle trapezius, and lower trapezius (along with several
other muscles) must be adequately trained to safely counteract the velocity of the
throwing arm, as well as stabilize the scapula (DiGiovine, Jobe, Pink, & Perry, 1992).
The findings of this study support the theory that the cable retraction with external
rotation exercise can be modified to meet the specific needs of the submarine pitcher,
without decreasing the effectiveness of the exercise, while also exercising the shoulder in
a position that is less likely to cause impingement syndrome. However, without proper
Submarine Pitchers 38
knowledge of what is occurring within the body during the submarine pitch, clinicians
cannot be positive that modifying exercises for submarine pitchers is more beneficial than
traditional pitching exercises.
Submarine Pitchers 39
References
10- camera Oqus 300 1.3MP infrared motion capture system (Qualisys, Gothenburg, Sweden) and Noraxon electromyography plug-in system (Scottsdale, Arizona) SPSS software (Version 20.0. Armonk, NY: IBM Corp)
Bitter, N. L., Clisby, E. F., Jones, M. A., Magarey, M. E., Jaberzadeh, S., & Sandaw, M.
J. (2007). Relative contributions of infraspinatus and deltoid during external rotation in healthy shoulders. The Journal of Elbow and Shoulder Surgery, 16, 563-568.
Blanc, Y. & Dimanico, U. (2010). Electrode placement in surface electromyography
(semg) "minimal crosstalk area" (mca). The Open Rehabilitation Journal, 3, 110-126.
Carter, A., Kaminski, T., Douex, A., Knight, C.,& Richards, J. (2007). Effects of high
volume upper extremity plyometric training on throwing velocity and functional strength ratios of the shoulder rotators in collegiate baseball players. Journal of Strength and Conditioning Research, 21, 208-215.
Clarys, J. P., Scafoglieri, A., Tresignie, J., Reilly, T., & Von Roy, P. (2010, June).
Critical appraisal and hazards of surface electromyography data acquisition in sport and exercise. Asian Journal of Sports Medicine, 69-80.
DiGiovine, N., Jobe, F., Pink, M., & Perry, J. (1992). An electromyographic analysis of
the upper extremity in pitching. Journal of Shoulder and Elbow Surgery, 1, 15-25. Dillman, C., Fleisig, G., & Andrews, J. (1993). Biomechanics of pitching with emphasis
upon shoulder kinematics. Journal of Orthopaedic & Sports Physical Therapy, 18(2), 402-408.
Donatelli, R., Ellenbecker, T., Ekedahl, S., Wilkes, J., Kocher, K., Adam, J. (2000).
Assessment of shoulder strength in professional baseball pitchers. Journal of Orthopaedic & Sports Physical Therapy, 30(9), 544-551.
Ekstrom, R., Donatelli, R., & Soderberg, G. (2003). Surface electromyographic analysis
of exercises for the trapezius and serratus anterior muscles. Journal of Orthopedic and Sports Physical Therapy, 23(5), 247-258.
Ehrman, J. K. (Ed.). (2010). ACSM's resource manual for guidelines for exercise testing
and prescription (6th ed.). Baltimore, MD: Lippincott Williams & Wilkins. Fleisig, G., Andrews, J., Dillman, C., & Escamilla, R. (1995). Kinetics of baseball
pitching with implications about injury mechanisms. American Journal of Sports Medicine, 23(2), 233-239.
Submarine Pitchers 40
Franklin, B., Conviser, J., Stewart, B., Lasch, J., Timmis, G. (2005) Sporadic exercise: a trigger for acute cardiovascular events? Circulation, 102, 6II–612.
Hancock, R., & Hawkins, R. (1996). Applications of electromyography in the throwing
shoulder. Clinical Orthopaedics and Related Research, 330, 84-97. Hogrel, J. (2005). Clinical applications of surface electromyography in neuromuscular
disorders. Neurophysiologie Clinique, 35, 59-71. Kendall, F., McCreary, E., & Provance, P. (1993). Muscles: Testing and function.
Baltimore, MD: Williams and Wilkins. Kibler, W. B., Sciascia, A. D., Uhi, T. L., Tambay, N., & Cunningham, T. (2008).
Electromyography analysis of specific exercises for shoulder scapular control in early phases of shoulder rehabilitation. The American Journal of Sports Medicine, 36(9), 1789 - 1798.
Marta, S., Pezarat-Correia, P., Fernandes, O., Carita, A., Cabri, J., Moraes, A. (2013).
EMG analysis of the shoulder external rotator and trapezius muscles in different exercises. International Sports Medicine Journal, 14, 1-15.
Matsuo, T., Matsumoto, T., Mochizuki, Y., Takada, Y. and Saito, K. (2002), Optimal
shoulder abduction angles during baseball pitching from maximal wrist velocity and minimal kinetics viewpoints. Journal of Applied Biomechanics, 18, 306-320.
Matsuo, T., Takada, Y., Matsumoto, T., Saito, K. (2000). Biomechanical characteristics
of sidearm and underhand baseball pitching: Comparison with those of overhand and three-quarter pitching. Japanese Journal of Biomechanics in Sports and Exercise, 4, 245-252.
Murphy, M., Sunnerhagen, K., Johnels, B., & Willen, C. (2006). Three-dimensional
kinematic motion analysis of a daily activity drinking from a glass: A pilot study. Journal of NeuroEngineering and Rehabilitation, 3(18).
Paine, R., Voight, M. (2013). Invited clinical commentary the role of the scapula. The
International Journal of Sports Physical Therapy, 8, 617-629. Park, S., Loebenberg, M., Rokito, A., & Zuckerman, J. (n.d.). The Shoulder in Baseball
Pitching: Biomechanics and Related Injuries – Part 1. NYU- Hospital for Joint Disease, 61(1&2), 68-79.
Pavlovich, L. (2011, October 1). Former Submarine Pitcher Kent Tekulve Explains
Mechanics. Retrieved July 6, 2013, from http://www.baseballnews.com/old/features/stories/2012/former_submarine_pitcher_kent_tekulve_explains.htm
Submarine Pitchers 41
Pennock, A., Pennington, W., Torry M., Decker, M., Vaishnav, s., Provencher, M., Millett, P., Hackett, T. (2011). The influence of arm and shoulder position on the bear-hug, belly-press, and lift-off tests: an electromyographic study. American Journal of Sports Medicine, 39(11), 2338-2346.
Pezzullo, D., Karas, S., & Irrgang, J. (1995). Functional plyometric exercises for the
throwing athlete. Journal of Athletic Training, 30(1), 22-26. Pretz, R. (2004). “Ballistic six” plyometric training for the overhead throwing athlete.
Strength and Conditioning Journal, 26(6), 62-66. Richmond, S., Godard, M. (2004). The effects of varied rest periods between sets to
failure using the bench press in recreationally trained men. Journal of Strength & Conditioning Research, 18(4), 846-849.
Scher, S., Anderson, K., Weber, N., Bajorek, J., Rand, K., & Bey, M. (2010).
Associations among hip and shoulder range of motion and shoulder injury in professional baseball players. Journal of Athletic Training, 45(2), 191-197.
Truedson, T., Sexton, P., & Pettitt, R. (2012). Unconventional baseball pitching styles,
part 1: Biomechanics and pathology. International Journal of Athletic Therapy & Training, 17, 35-39.
Truedson, T., Sexton, P., & Pettitt, R. (2012). Unconventional baseball pitching styles,
part 2: Upper extremity rehabilitation. International Journal of Athletic Therapy & Training, 17, 40-44.
Tucker, C., Bagley, A., Wesdock, K., Church, C., Henley, J., & Masiello, G. (2008).
Kinematic Modeling of the shoulder complex in tetraplegia. Topics in Spinal Cord Rehabilitation, 73-85.
Vander Linden, D. W., Carison, S. J., & Hubbard, R. L. (1992, Yes). Reproducibility and
accuracy of angle measurements obtained under static conditions with the Motion Analysis video system. Physical Therapy Journal, 72(4), 60-65.
Whiteley, R. (2007). Baseball throwing mechanics as they relate to pathology and
performance – a review. Journal of Sports Science and Medicine, 6, 1-20. Watanabe, K., & Akima, H. (2011, June). Validity of surface electromyography for
vastus intermedius muscle assessed by needle electromyography. Journal of Neuroscience Methods, 198(2), 332-335.