Embed Size (px)
Citation preview

Subjective and physiological emotional response in euthymic bipolarpatients: A pilot study
Mathieu Lemaire a,b,n, Nadia Aguillon-Hernandez a, Frédérique Bonnet-Brilhault a,b,Joëlle Martineau a, Wissam El-Hage a,c
a UMR INSERM U930 - Université François Rabelais de Tours “Imaging and Brain”, Boulevard Tonnellé, 37044 Tours Cedex 9, Franceb CHRU de Tours, Centre Universitaire de Pédopsychiatrie, Boulevard Tonnellé, 37044 Tours Cedex 9, Francec CHRU de Tours, Clinique Psychiatrique Universitaire, Boulevard Tonnellé, 37044 Tours Cedex 9, France
a r t i c l e i n f o
Article history:Received 3 November 2013Received in revised form14 April 2014Accepted 2 July 2014
Keywords:Bipolar disorderEmotionsPupilAffective pictures
a b s t r a c t
The euthymic phase of bipolar disorders may be associated with residual emotional and/or subsyndromalsymptoms. The aim of this study was to compare subjective and physiologic emotional response tonegative, neutral and positive emotion eliciting pictures between euthymic bipolar patients (n¼26) andhealthy controls (n¼30). We evaluated emotional response using an emotional induction method withemotional pictures from the International Affective Picture System. We measured subjective emotionalresponse with the Self-Assessment Manikin and physiological emotional response by measuring pupil size.No difference was found between euthymic bipolar patients and controls regarding subjective emotionalresponse. However, upon viewing positive pictures, pupil dilation was significantly lower in euthymicbipolar patients compared to controls. This finding suggests that euthymic bipolar phase may be associatedwith reduced physiologic emotional response to positive valence, which is consistent with a more generalnegative emotional bias or can be understood as a residual emotional subsyndromal symptom.
& 2014 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Bipolar disorder (BD) is a common disabling mood disorder.Classically, the euthymic phase was considered to be symptom-free, although current literature highlights the high prevalence ofresidual symptoms, comorbid disorders and/or specific tempera-ments (Akiskal et al., 2006; Perugi et al., 2010; Samalin et al., 2014)implicated in the prognosis of the disorder. Moreover, the euthy-mic phase was recently linked with persistent emotional reactivitydisturbances (M'bailara et al., 2009). A study by Henry et al.(2008b) showed that the lability and intensity of emotions arehigher in euthymic subjects compared to controls, according to theuse of two self-rating scales. Moreover, the study by M’bailaraet al. (2009) using an emotional induction method showed thatthe subjective evaluation of valence, arousal and the startle reflexwhile viewing neutral images was greater among euthymicpatients than controls. Some of these results were confirmedby Giakoumaki et al. (2010) who found that euthymic patientsscored neutral pictures more positively than did the controls.These studies suggested a higher level of emotional reactivity in
euthymic patients, although this finding was not confirmed by twoadditional studies that used only subjective measures of emotionalreactivity in euthymic BD patients (Chang et al., 2004; Aminoff etal., 2011). Thus, the question of emotional response in euthymicpatients remains controversial.
According to Kleinginna and Kleinginna's definition of emotion,there are three components of an emotional response: subjective/experiential, physiological, and behavioral/expressive (Kleinginnaand Kleinginna, 1981). To measure these components, questionnairescan be used for the subjective/experiential component, whereas arecording of skin conductance, heart rate, startle reflex, or pupildiameter can be used for the physiological component, and facialexpression measurements can be used for the behavioral/expressivecomponent. The current study used subjective (the Self-AssessmentManikin; SAM) and physiological (pupil diameter) measurements.Compared to other methods, pupil diameter measurements are oneof the most sensitive physiological variables that can control for theorientation of visual attention and be recorded without any equip-ment placed on the subject (Tursky et al., 1969; Bradley et al., 2008).
Quantification of emotional response also requires controllingfor variables known to influence emotional response, such as age(Grühn and Scheibe, 2008), sleep deprivation (Franzen et al., 2009;Baglioni et al., 2010; Tempesta et al., 2010), life events (Myin-Germeys et al., 2003), emotional regulation strategies (Gross, 1998,2002; Gross and John, 2003) and treatments (El-Mallakh and
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/psychres
Psychiatry Research
http://dx.doi.org/10.1016/j.psychres.2014.07.0020165-1781/& 2014 Elsevier Ireland Ltd. All rights reserved.
n Corresponding author at: CHRU de Tours, Centre Universitaire de Pédopsychia-trie, 2 Boulevard Tonnellé, 37044 Tours Cedex 9, France. Tel.: þ33 2 47 47 84 12;fax: þ33 2 47 47 38 46.
E-mail address: [email protected] (M. Lemaire).
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i
Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎

Karippot, 2005). Because these variables are not always accountedfor, they can contribute to conflicting results between studies. Inthis study, we evaluated different variables that influence emo-tional response, including sleep, life events, emotional regulationstrategies and treatments.
The aim of this study was to investigate subjective andphysiological emotional response in euthymic BD patients usingan emotional induction method. Physiological measures of emo-tional response were assessed with a new approach using an eye-tracking device to measure pupil size.
2. Methods
2.1. Participants
Twenty-six type I and II bipolar patients (16 women) as defined by the DSM-IV(American Psychiatric Association, 2000), with symptomatic remission at least forone month were recruited according to the following inclusion criteria (seeTable 1): age of 20–60 years, a Montgomery and Åsberg Depression Rating Scale(MADRS) (Montgomery and Asberg, 1979; Hawley et al., 2002) score r10 and aYoung Mania Rating Scale (YMRS) (Favre et al., 2003; Rosso et al., 2009; Younget al., 1978) score o6. The diagnostic for each patient was made by the treatingpsychiatrist. It was confirmed by the psychiatrist investigator using the DSM-IVcriteria and the Mini International Neuropsychiatric Interview 5.0.0 (MINI) forbipolar disorder (Sheehan et al., 1998). Thirty comparison participants (17 women)were recruited from the university and hospital staff according to the followingcriteria: age of 20–60 years and no history of personal/familial BD, suicide attemptsor addiction. All participants provided informed written consent, and all proce-dures were conducted in accordance with the Helsinki Declaration of 1975.
2.2. Clinical data
All participants underwent a clinical evaluation on the day of testing, andclinical data, including the number of previous mood episodes, psychiatrichospitalizations, suicide attempts and psychotropic medications were collected.Comorbid psychiatric disorders were assessed using the MINI.
Current mood state was assessed with the MADRS to evaluate the severity ofdepressive symptoms, the YMRS rating of mania symptoms (Young et al., 1978;Favre et al., 2003) and the Multidimensional Assessment scale of Thymic States(MAThyS) (Henry et al., 2008a). The MAThyS was designed as a multi-dimensional,self-administered questionnaire comprising 20 items relating to the individualstates perceived by patients during the preceding week. The MAThyS evaluates fivedimensions (emotional reactivity, cognition speed, psychomotor function, motiva-tion and sensory perception), which can fluctuate from inhibition to excitation, todescribe quantitative dimensions of mood episodes. Furthermore, a secondcomponent of this scale evaluates the frequency of seven emotions (sadness, joy,irritability, panic, anxiety, anger, and euphoria) using a Likert scale (never,occasionally, often, very often, and constantly) (Henry et al., 2008a).
All participants completed self-report measures of sleep quality retrospectivelyover a 1-month period using the Pittsburgh Sleep Quality Index (PSQI) (Buysse et al.,1989; Blais et al., 1997; Carpenter and Andrykowski, 1998). The PSQI consists of 19items that produce a global sleep quality score as well as 7 subscores (concerning sleepquality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use ofsleeping medication and daytime dysfunction). Moreover, we recorded the number ofhours that the participants slept during the night prior to the day of testing.
The number of stressful life events during the last year and their impact wereinvestigated using the Social Readjustment Rating Scale (SRRS) (Holmes and Rahe,1967). Emotion regulation strategies (reappraisal and suppression) were investi-gated using the Emotion Regulation Questionnaire (ERQ) (Gross and John, 2003;Christophe et al., 2009).
2.3. Emotional response investigations
2.3.1. StimuliThree sets of visual stimuli were selected from the International Affective
Picture System (IAPS) (Lang et al., 2008), including 12 negative (mean valence/arousal¼2.1/6.2), 12 neutral (mean valence/arousal¼5.1/3.3) and 12 positive (meanvalence/arousal¼7.6/5.8) pictures.1 As Bradley et al. (2008), we presented thepictures in greyscale, because the human eye is differentially sensitive to light in
the green, red, and blue spectra. All of the pictures were displayed in 8-bit grayscale using the GNU Image Manipulation Program (Gimp v2.6.11, Open sourcesoftware, http://www.gimp.org/). The mean luminosity of the pictures was mod-ified to produce comparable means and distributions of luminosity values for eachof the pictures sets (Bradley et al., 2008). Importantly, as demonstrated by previousstudies (Bradley et al., 2001, 2003; Bradley and Lang, 2007), whether the pictureswere presented in color or gray-scale had little or no effect on affectiveengagement.
Picture presentation was controlled by a computer using the GazeTrackerssoftware (Eye Response Technologies Inc., Charlottesville, VA 22902, USA), whichallowed for stimuli presentation and recording, data synchronization, data analysisand visualization. Pupil diameter was recorded using a FaceLABs eye tracker(Seeing Machine Inc., Tucson, AZ 85711, USA). This eye-tracking system consisted ofa computer equipped with two numeric cameras that filmed the eyes of a subjectwhile he/she looked at images on the computer screen and permitted the subject tomove freely. Pictures were displayed on a 21.5-in. flat screen located in theexperimental room 110 cm (43.3 in.) away from where the participant was seated.
2.3.2. ProcedureWe presented the pictures to subjects while their eyes were being tracked. The
IAPS pictures were displayed as a succession of 12 trios, each trio including onenegative, one neutral, and one positive picture. Each picture was displayed for 6 s.The effect of presentation order was limited by ensuring that negative, neutral, andpositive images were revealed in a balanced presentation order (M'bailara et al.,2009). A gray-scale slide with the mean luminosity of the presented pictures wasdisplayed during the 2-s intertrial interval to control the levels of illumination priorto picture onset (Bradley et al., 2008). The subject was instructed to focus on theimages presented and to remain silent during the experiment.
2.3.3. Subjective emotional responseThe participants were asked to provide a subjective evaluation of each picture
using the Self-Assessment Manikin (SAM). The SAM is a non-verbal pictorialassessment technique that directly measures the valence and arousal associatedwith a person's affective reaction to a wide variety of stimuli (Bradley and Lang,1994). The nine-point Likert-type scale version of the SAM was used. For valenceevaluation, low scores indicated unpleasantness, high scores indicated pleasantnessand middle range scores indicated neutrality. For arousal evaluation, low scoresindicated weak emotions and high scores indicated strong emotions (M'bailara etal., 2009). The participants' responses were recorded using PXLab© software(Psychological Experiment Laboratory) (Irtel, 2007) to avoid experimenter influ-ence. This software presented each picture twice to allow for the self-rating ofemotional valence and arousal scores in a pseudo-random manner.
2.3.4. Physiological emotional responseThe pupil size was recorded with an acquisition frequency of 60 Hz (i.e., every
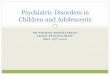
17 ms). For each stimulus or inter-trial slide, pupil data were inspected to eliminateartifacts (blinking, loss of tracking or non-physiological measures). Only pupil sizesbetween 1 and 9 mmwere considered for the analysis (Beatty and Lucero-Wagoner,2000). As described by Martineau et al. (2011), pupil size measurements wereaveraged between the two eyes due to consensual reflex. An average pupil size wascomputed every 100 ms. These averages were plotted over time to obtain a pupilwaveform. The pupil waveform was obtained in response to negative, neutral, andpositive categories of stimuli. The pupil diameter fluctuates according to thepupillary light reflex during the first 2 s of exposure (slight pupil dilation followedby a large pupil constriction) and the psychosensory reflex (pupil dilation) (cf.Fig. 1). The magnitude of the change in pupil diameter during the pupillary lightreflex depends mainly on the luminance of the stimuli, whereas the magnitude ofthe psychosensory reflex depends on the cognitive load and emotions of theindividual (Beatty and Lucero-Wagoner, 2000). To measure the magnitude of thepsychosensory reflex, we calculated the Area Under the Curve (AUC) of the pupilwaveform between 2 and 6 s after the presentation of each type of stimuli(negative, neutral, and positive).
2.4. Data analysis
The normality of distribution of all variables was examined. Sociodemographicdata (age, gender, number of years of education, and employment) were comparedbetween groups using either Mann-Whitney U tests or Pearson's chi-squared test.The prevalence of psychiatric comorbidities was compared using either Pearson'schi-squared test or Fisher exact test. Scores from the rating scales (MADRS, YMRS,PSQI, MAThyS, SRRS, ERQ), the number of life events and the number of hours ofsleep the day before the experiment were compared between groups using Mann-Whitney U tests.
We used mixed-effects regression models to assess the effect of valence ofpicture (negative, neutral and positive), group (control, bipolar), valence x group,sex, valence x sex, age, number of hours of sleep and scores from the rating scales(MADRS, YMRS, MAThyS emotion reactivity subscale, SRRS, ERQ reappraisal, ERQsuppression) on psychophysiological data (AUC) and subjective ratings of valence
1 Negative: 2683, 2710, 2800, 3180, 3350, 3530, 6212, 6312, 6350, 6510, 9810,9910; Neutral: 2038, 2102, 2191, 2214, 2393, 2396, 2411, 2514, 2595, 2635, 2880,2890; Positive: 1441, 2035, 2340, 2347, 4659, 4660, 4668, 4680, 5621, 5825,5833, 8370.
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎2
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

and arousal. The initial multivariate model was based on a theoretical independentvariable selection. The best fitting model was selected after dropping out step-by-step the less significant term was from previous models. Valence, group, valence xgroup, were forced in the model even if they were not significant. Furthermore, tomeasure the potential effects of psychotropic medications on pupil size, wecompared the AUCs for pupil waveform between BD patients taking psychotropicmedications (lithium, anticonvulsants, antipsychotics, antidepressants, and anxio-lytics) and those not taking medications. This analytic strategy has been proposedto resolve the potential confounding effects of psychotropic medication use amongindividuals taking a variety of medications (Phillips et al., 2008). Hence, we usedmixed-effects regression models to assess the effect of valence (negative, neutraland positive), and treatment (lithium, anticonvulsants, antipsychotics, antidepres-sants, and anxiolytics) on psychophysiological data (AUC).
Fitted models were inspected graphically in order to examine whether theunderlying distributional assumption holds for the data (Pinheiro and Bates, 2009).All statistics analyses and graphics were done using R 3.0.1 (R Development CoreTeam, 2013). The mixed models were fitted using “nlme” R package (Pinheiro et al.,2013). For factors showing a significant main fixed effect, pairwise comparisons
were conducted with False Discovery Rate (FDR) correction (Benjamini andHochberg, 1995), that may be the best for physiological data (Curran-Everett,2000), using “multcomp” R (Hothorn et al., 2008).
3. Results
3.1. Clinical data
We recruited 26 euthymic BD patients and 30 controls. Controlsand patients did not differ significantly in terms of their sexratio or mean age. According to the MADRS and YMRS scores,all participants were euthymic. Tables 1 and 2 show the clinicaldescription of the study groups.
Table 1Clinical characteristics of the participants.
Controls (n¼30) Euthymics (n¼26) Test p
Sex (female/male), n 17/13 16/10 χ²¼0.14 nsAge (years), mean7S.D. 41.2712 46.7710 U¼273 0.055Years of education, mean7S.D. 16.872.8 14.472.3 U¼559 o0.01Unemployed, % (n) 0 (0) 34.6 (9) χ²¼9.94y o0.01
Bipolar disorderType I, % (n) 0 (0) 61.5 (16) – –
Type II, % (n) 0 (0) 38.5 (10) – –
Time since the previous episode (months), mean7S.D. – 55.8 (95.2) – –
Previous manic episodes, mean7S.D. – 4.475.2 – –
Previous depressive episodes, mean7S.D. – 7.977.6 – –
Polarity of the last episode, % (n)Depressive – 65.4 (17) – –
Manic/Hypomanic – 34.6 (9) – –
History of psychiatric admissions, mean7S.D. – 5.676 – –
Current psychotropic drugs, % (n)Lithium – 57.7 (15) – –
Anticonvulsant – 53.9 (14) – –
Typical Antipsychotic – 7.7 (2) – –
Atypical Antipsychotic – 30.8 (8) – –
Antidepressant – 23.1 (6) – –
Benzodiazepine – 23.1 (6) – –
MADRS score, mean7S.D. 1.272.2 3.973.2 U¼182 o0.001YMRS score, mean7S.D. 0.370.7 0.771.2 U¼295 nsSuicidal attempts, mean7S.D. 0 1.572.2 – –
MADRS: Montgomery and Asberg Depression Rating Scale; YMRS: Young Mania Rating Scale; χ²: Chi-squared test (y: Yates correction); U: Mann-Whitney U test.
Fig. 1. Changes in pupil diameter (from the trough of the initial pupillary lightreflex) during stimuli viewing. The influence of pupillary light reflex (PLR) andpsychosensory reflex (PSR) on pupil diameter at different times. The Area Under theCurve (AUC) represents between 2 and 6 s of the picture presentation.
Table 2Current psychiatric comorbidities according to the MINI.
Controls(n¼30)
Euthymics(n¼26)
χ² p
Panic disorder 3.3 (1) 34.6 (9) 7.28Y o0.01Agoraphobia 0 (0) 15.4 (4) ‡ o0.05Social phobia 6.7 (2) 26.9 (7) 2.87 0.09Generalized anxietydisorder
3.3 (1) 38.4 (10) 10.89 o0.001
Obsessive compulsivedisorder
0 (0) 7.7 (2) ‡ ns
Post-traumatic stressdisorder
0(0) 3.9(1) ‡ ns
Alcohol dependence 0 (0) 0 (0) – –
Alcohol abuse 3.3 (1) 7.7 (2) ‡ nsDrug dependence(non-alcohol)
0 (0) 11.5 (3) 3.66 0.06
Drug abuse (non-alcohol) 3.3 (1) 3.9 (1) 0.01 nsPsychotic disorder 0 (0) 0 (0) – –
Anorexia nervosa 0 (0) 0 (0) – –
Bulimia 0 (0) 3.9 (1) ‡ ns
Percentage (number); χ²: Chi-squared test; y: Yates correction; ‡: Fisher exact test.
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 3
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

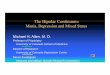
No difference was found between groups concerning the totalMAThyS score of approximately 100, which was used to defineeuthymia (cf. Table 3). Compared to the controls, euthymicpatients demonstrated higher scores for emotional reactivity aswell as higher sensory perception subscores of the MAThyS. Therewere no differences between groups for other MAThyS subscores:cognition speed, psychomotor function and motivation. Examiningfrequency of emotion showed that euthymic patients experienceda higher frequency of sadness (U¼253, po0.05, d¼0.77), anxiety(U¼182.5, po0.001, d¼1.08) and anger (U¼276.5, po0.05,d¼0.64) than did controls (cf. Fig. 2). There were no differencebetween groups for joy (U¼477, ns, d¼0.48), irritability (U¼306.5,ns, d¼0.44), panic (U¼301, p¼0.07, d¼0.50), and euphoria(U¼376, ns, d¼0.10).
Both groups presented comparable results concerning the num-ber of stressful life events, SRRS scores, suppression and reappraisalscores, and the ERQ total score. No significant difference (U¼348,ns, d¼0.20) in sleep duration was found between the euthymicpatients (7.0671.82 h) and the controls (6.7471.45 h). Regardingthe PSQI, the euthymic patients demonstrated significantly higherglobal scores, longer sleep latency, a greater use of sleeping medica-tions and higher levels of daytime dysfunction than controls (cf.Table 3). Both groups were comparable in terms of sleep quality,sleep duration, habitual sleep efficiency and sleep disturbances.
3.2. Subjective emotional response
The affective picture ratings (mean7S.D.) for the entire sampleconfirmed the categorization of the pictures as negative (2.070.79),neutral (5.2370.43), and positive (7.170.89).
Valence. After model selection, the final model only includevalence, group, valence x group as independent variables, all othervariable were dropped out of the theoretical model because therewere highly not significant (all p40.05). There was a significantmain effect of valence of picture (F(2,108)¼700.14, po0.0001) butnot of group (F(1,54)¼0.03, ns) or interaction between group andvalence (F(2,108)¼2.12, ns). For all participants, valence values for
negative pictures are lower than for neutral (β¼3.35, SE¼0.19,po0.0001), and positive pictures (β¼5.36, SE¼0.19, po0.0001),and valence for neutral pictures are lower than for positivepictures (β¼2.01, SE¼0.19, po0.0001) (cf. Fig. 3).2
Arousal. After model selection, the final model only includevalence, group, valence x group as independent variables, allother variable were dropped out of the theoretical model becausethere were highly not significant (all p40.05). There was asignificant main effect of valence of picture (F(2,108)¼178.92,po0.0001) but not of group (F(1,54)¼0.02, ns) or interactionbetween group and valence (F(2,108)¼0.71, ns). Arousal wasgreater for emotionally valenced compared to neutral pictures(negative: β¼4.25, SE¼0.29, po0.0001; positive: β¼2.52,SE¼0.29, po0.0001) and for negative compared to positivepictures (β¼1.73, SE¼0.29, po0.0001) (cf. Fig. 3).
Table 3Result for the scales.
Controls (n¼30) Euthymics (n¼26) U p d
Emotion Regulation Questionnaire (ERQ)Total (12–66) 36.3710.6 36.5712.5 378.5 ns 0.02Reappraisal (6–42) 24.578 22.979 415.5 ns 0.19Suppression (6–24) 11.874.8 13.675.9 310.0 ns 0.34
Social Readjustment Rating Scale (SRRS)Number of life events (0–43) 6.673.7 5.873.4 445.5 ns 0.23Score (0–1466) 161.87109.2 167.17119.6 398.5 ns 0.05
Pittsburgh Sleep Quality Index (PSQI)Global score (0–21) 4.4372.95 7.0874.65 251.0 o0.05 0.71Sleep quality (0–3) 0.9770.76 1.3171.09 328.0 ns 0.32Sleep latency (0–3) 0.5770.82 1.0871.06 278.5 o0.05 0.56Sleep duration (0–3) 0.8070.89 0.8871.14 393.5 ns 0.10Habitual sleep efficiency (0–3) 0.4770.73 0.5471.03 412.0 ns 0.08Sleep disturbance (0–3) 1.1370.35 1.3570.57 305.0 0.07 0.47Use of sleep medications (0–3) 0.1070.30 0.9271.29 267.0 o0.01 0.92Daytime dysfunction (0–3) 0.4070.56 1.0070.98 252.0 o0.05 0.78
MAThySTotal (0–200) 101.0174.03 103.30718.85 325.5 ns 0.18Emotional reactivity (0–40) 20.3571.37 22.7875.79 209.5 o0.01 0.61Cognition speed (0–40) 20.0471.06 21.0075.30 347.5 ns 0.27Psychomotor function (0–30) 14.9671.86 13.6774.83 497.5 0.08 0.37Motivation (0–40) 20.5671.89 19.5375.60 451.5 0.08 0.27Sensory perception (0–50) 25.1071.42 26.3275.31 230.0 o0.01 0.33
Mean7S.D.; For each subscale (range); MAThyS: Multidimensional Assessment scale of Thymic States, for each score, low score is indicative of inhibition and high score ofactivation; U: Mann-Whitney U test; d: Cohen's d; ns: non significant.
Sadness Joy Irritability Panic Anxiety Anger Euphoria
Freq
uenc
y of
Em
otio
ns
Nev
erO
ccas
iona
llyO
ften
Ver
y O
ften
Con
stan
tly
Controls
Euthymics BD
Fig. 2. Mean (7S.D.) frequency of emotions experienced during the weak prior tothe study for euthymic bipolar patients (n¼26) and controls (n¼30). npo0.05;nnpo0.001.
2 Detailed result in Supplementary Tables 1 (subjective response) and 2(physiological response).
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎4
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

3.3. Physiological emotional response
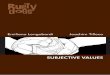
Fig. 4 illustrates the changes in pupil diameter that areobserved when the subjects viewed negative, neutral or positivepictures, and these results are compared between euthymicbipolar patients and healthy controls.
After model selection, the final model only include valence,group, age, valence x group as independent variables, all othervariable were dropped out of the theoretical model because therewere highly not significant (all p40.05). For the AUC values, therewas a significant main effect of valence of picture (F(2,108)¼7.45,po0.01), group (F(1,54)¼5.83, po0.02), age (β¼�0.18, SE¼0.05,po0.01), and interaction between group and valence (F(2,108)¼4.15, po0.02). For the controls, the AUC was significantly greater foremotionally valenced compared to neutral pictures (negative:β¼2.08, SE¼0.65, po0.01; positive: β¼2.46, SE¼0.65, po0.01)although no significant difference in the AUC was observed betweennegative and positive pictures (β¼0.38, SE¼0.65, ns) (cf. Fig. 5). Forthe euthymic group, the AUC was significantly greater for negativepictures compared to positive pictures (β¼1.60, SE¼0.69, po0.05)although no significant difference in the AUC was observed betweennegative and neutral pictures (β¼1.44, SE¼0.69, p¼0.07) andbetween positive and neutral (β¼0.17, SE¼0.69, ns). When compar-ing between groups there was a statistical significant difference forpositive picture, AUC was greater for the control group in compar-ison with the euthymic group (β¼4.03, SE¼1.28, po0.01) but notfor negative and neutral pictures (negative: β¼2.06, SE¼1.28, ns;neutral: β¼1.41, SE¼1.28, ns). None of the other variables orinteractions were significant (all p40.05).
Concerning the effect of treatment on pupil size (AUC) ineuthymic patients, the mixed model demonstrated no significant
effect of treatment, with lithium (F(1,20)¼1.79, d¼0.55), antic-onvulsants (F(1,20)¼0.03, d¼0.07), antipsychotics (F(1,20)¼1.16,d¼0.45), antidepressants (F(1,20)¼0.20, d¼0.22), or benzodiaze-pines (F(1,20)¼0.01, d¼0.05).
3.4. Link between physiological and subjective emotional response
In control group, there was a significant positive correlationbetween AUC and subjective arousal (β¼0.36, SE¼0.14, po0.02)that was not present in the euthymic group (β¼0.14, SE¼0.15, ns).
4. Discussion
The goal of the study was to examine subjective and physio-logical emotional response in euthymic BD patients using an
Negative Neutral Positive
Vale
nce
scor
e
1
2
3
4
5
6
7
8
9
Controls
Euthymics BD
ns
ns
ns
Negative Neutral Positive
Aro
usal
sco
re
1
2
3
4
5
6
7
8
9
ns
ns
ns
Fig. 3. Mean (7S.D.) ratings of picture valence and arousal by euthymic bipolarpatients (n¼26) and controls (n¼30). npo0.001. ns: not significant.
0 1 2 3 4 5 6
0.3
0.2
0.1
0.0
0.1
Time (s)
Pup
il di
amet
er (m
m)
NEGATIVE
Controls
Euthymics BD
0 1 2 3 4 5 6
0.3
0.2
0.1
0.0
0.1
Time (s)
Pup
il di
amet
er (m
m)
NEUTRAL
Controls
Euthymics BD
0 1 2 3 4 5 6
0.20
0.10
0.00
0.05
0.10
0.15
Time (s)
Pup
il di
amet
er (m
m)
POSITIVE
Controls
Euthymics BD
Fig. 4. Changes in pupil diameter when viewing negative, neutral and positivepictures among euthymic bipolar patients (n¼26) and controls (n¼30).
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 5
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

emotional induction method. We found that pupil dilation wassignificantly lower in euthymic patients than controls during theviewing of only positive pictures. This finding was independent ofsex, depression scores, manic scores, sleep duration, life events,subjective emotional reactivity and emotion regulation strategy.This result suggests that euthymic patients had less emotionalphysiological response to positive stimuli than controls, whileno difference was found between groups regarding subjectiveemotional response. This finding is consistent with a more generalnegative emotional bias or can be understood as a residualemotional subsyndromal symptom.
In our study, both groups were comparable on variables knownto influence emotional response, including age, sleep duration onthe night preceding the study, and the number of life eventsexperienced during the last year and their associated psychologicalimpact (Grühn and Scheibe, 2008; Franzen et al., 2009; Baglioni etal., 2010; Tempesta et al., 2010). However and as expected, BDpatients had more psychiatric comorbidities, particularly anxietydisorders (Merikangas et al., 2007; El-Mallakh and Hollifield,2008). Sleep duration was not different between groups eventhough the PSQI scores were higher among bipolar patients,suggesting that BD patients had poorer sleep quality than controls.Therefore, the impact of these variables (anxiety, sleep quality) onemotional response requires further investigation.
Increased emotional response in euthymic patients has beenpreviously demonstrated. In our study, the MAThyS total score iscoherent with euthymic state in patients and controls. However,emotional reactivity subscores were higher among the patientsthan controls, suggesting a subjective emotional hyperreactivityperceived by the bipolar patients during the euthymic phase.These results replicate previous data (Henry et al., 2008b) thatdemonstrated increased subjective emotional response duringeuthymia. This subjective emotional hypereactivity may be par-tially explained by the imbalance in emotional response betweennegative and positive stimuli. Furthermore, using the MAThySscale, we found that some negative emotions were more fre-quently experienced among euthymic patients than controls, i.e.,sadness, anxiety, and anger. This increased frequency of negativeemotions supports the findings of Havermans et al. (2010), whichis also consistent with the observed decreased emotional responsefor positive valence among euthymic patients as compared tocontrols.
Our findings demonstrated that the subjective rating of affec-tive pictures did not differ between groups. Contrary to previousstudies (M'bailara et al., 2009; Giakoumaki et al., 2010), our
patients demonstrated no emotional hyperreactivity for neutralpictures, which may result from methodological differences asneutral pictures likely differ between studies. For instance, pre-vious studies have used neutral pictures of objects, animals andvegetation (M'bailara et al., 2009; Giakoumaki et al., 2010, Aminoffet al., 2011), whereas we used neutral pictures involving humanscenarios. However, Aminoff et al. (2011) used neutral pictures ofobjects, and not social neutral pictures like in our study, and alsofound no significant difference between patients with bipolardisorder and healthy controls in subjective evaluation of valenceor arousal. We assume that healthy subjects are more reactive tohuman scenarios, attenuating the differences regarding the sub-jects' abilities to react to visual stimuli. This hypothesis is sup-ported by recent research highlighting the salience of social cuescontained in faces (Little et al., 2011), which are better recognizedby healthy subjects than bipolar patients (Versace et al., 2010).Furthermore, in our study, the pictures were not presented in colorbut in gray scale, unlike previous studies (M'bailara et al., 2009;Giakoumaki et al., 2010). Although wewould argue that there is noeffect of color versus gray scale on many indices of affectiveengagement (Bradley et al., 2001, 2003; Bradley and Lang, 2007),this topic remains controversial for bipolar studies and may play asignificant role in their emotional response. Thus, our resultsmay have been modulated by this variable as well as others, suchas sleep duration or life events, which were not controlled inprevious studies.
One of the objectives of this study was to demonstrate differ-ences in subjective emotional response, although we assumed sucha task would be difficult because euthymic patients and controls donot share the same emotional experiences. Subjects with BDexperience unusually intense emotional states during mood epi-sodes; this issue may explain why subjective evaluations are oftencomparable, whereas physiological evaluations of emotionalresponse often differ between bipolar patients and controls.
Concerning the physiological measurements of emotionalresponse, we showed that pupil dilation during psychosensoryreflex was significantly lower among controls for neutral picturesthan for emotional pictures. Pupil dilation among controls was notdifferent between negative and positive pictures, supportingprevious results (Bradley et al., 2008). However, we observed adifferent pattern in euthymic BD patients, as pupil dilation washigher for negative than positive pictures. Furthermore, pupildilation was significantly lower in euthymic patients during theviewing of positive pictures compared to controls. Thus, weshowed that euthymic patients had less physiological emotionalresponse to positive valence than did controls. Although ourresults suggest that psychotropic medication did not influencepupil size in this study, we need to be careful about the potentialeffects of psychotropic medication on these measures. Neverthe-less, we argue that if our physiological results were only attribu-table to a treatment effect, this effect would have been similar forthe different sets of pictures. Furthermore, it is often clinicallyunfeasible and ethically problematic to withdraw patients frommedication, and bipolar individuals who can tolerate beingmedication-free may not accurately represent the BD population(Hassel et al., 2008). The psychosensory reflex is also correlated tocognitive load (Loewenfeld, 1999) and is therefore partially corre-lated to the mobilization of attentional resources. We assumed thatincreased pupil size in patients is related to the impact of negativeimages on their cognitive load. Furthermore, we believe that amongthe patients studied here, the negative images seemed to capturevisuo-spatial attention more strongly than did neutral or positivepictures, and this finding is consistent with the hypothesis of anegativity bias present among euthymic patients. Altogether theseresults suggest that pupil dilation may be a possible endophenotypefor BD highlighting emotion response dysregulation.
Negative Neutral Positive
AU
C
0
5
10
15
Controls
Euthymics BD
Fig. 5. Mean (795% confidence interval) area under the curve between 2 and 6 s ofpicture presentation for euthymic bipolar patients (n¼26) and controls (n¼30).npo0.05; nnpo0.01.
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎6
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

Emotional response in bipolar illness is a clinically relevantdimension, as it influences large aspects of a patient's life. How-ever, very few studies have explored this dimension in euthymia.In our study, no difference was found between euthymic bipolarpatients and controls regarding subjective emotional response.However, upon viewing positive pictures, pupil dilation wassignificantly lower in euthymic bipolar patients compared tocontrols suggesting a reduced physiologic emotional response topositive valence, which is consistent with a more general negativeemotional bias. Additional investigations should replicate theresults presented here and focus on specific re-education programs.
Role of funding
During the study period, ML received a research grant fromEutherapie, which was unrelated to the content of this manuscript.
Conflict of interest
None declared.
Acknowledgments
We thank Pr. Chantal Henry for her helpful comments on thedraft of the manuscript. We are also grateful to the psychiatristswho have helped in the study recruitment, to all patients andhealthy volunteers for their participation.
Appendix A. Supplementary material
Supplementary data associated with this article can be found inthe online version at http://dx.doi.org/10.1016/j.psychres.2014.07.002.
References
Akiskal, H.S., Kilzieh, N., Maser, J.D., Clayton, P.J., Schettler, P.J., Traci Shea, M.,Endicott, J., Scheftner, W., Hirschfeld, R.M.A., Keller, M.B., 2006. The distincttemperament profiles of bipolar I, bipolar II and unipolar patients. Journal ofAffective Disorders 92, 19–33.
American Psychiatric Association, 2000. (Text Revision (DSM-IV-TR). Diagnostic andStatistical Manual of Mental Disorders, Fourth Edition American PsychiatricAssociation, Arlington, VA.
Aminoff, S.R., Jensen, J., Lagerberg, T.V., Andreassen, O.A., Melle, I., 2011. Decreasedself-reported arousal in schizophrenia during aversive picture viewing com-pared to bipolar disorder and healthy controls. Psychiatry Research 185,309–314.
Baglioni, C., Spiegelhalder, K., Lombardo, C., Riemann, D., 2010. Sleep and emotions:a focus on insomnia. Sleep Medicine Reviews 14, 227–238.
Beatty, J., Lucero-Wagoner, B., 2000. The pupillary system (In:). Handbook ofPsychophysiology. Cambridge University Press, Cambridge, pp. 142–162.
Benjamini, Y., Hochberg, Y., 1995. Controlling the false discovery rate: a practicaland powerful approach to multiple testing. Journal of the Royal StatisticalSociety. Series B (Methodological), 289–300.
Blais, F.C., Gendron, L., Mimeault, V., Morin, C.M., 1997. [Evaluation of insomnia:validity of 3 questionnaires]. Encephale 23, 447–453.
Bradley, M.M., Codispoti, M., Cuthbert, B.N., Lang, P.J., 2001. Emotion and motiva-tion I: defensive and appetitive reactions in picture processing. Emotion 1,276–298.
Bradley, M.M., Lang, P.J., 1994. Measuring emotion: the Self-Assessment Manikinand the Semantic Differential. Journal of Behavior Therapy and ExperimentalPsychiatry 25, 49–59.
Bradley, M.M., Lang, P.J., 2007. The International Affective Picture System (IAPS) inthe study of emotion and attention. In: Coan, J.A., Allen, J.J.B. (Eds.), Handbookof Emotion Elicitation and Assessment, Series in Affective Science. OxfordUniversity Press, Oxford; New York, pp. 29–46.
Bradley, M.M., Miccoli, L., Escrig, M.A., Lang, P.J., 2008. The pupil as a measure ofemotional arousal and autonomic activation. Psychophysiology 45, 602–607.
Bradley, M.M., Sabatinelli, D., Lang, P.J., Fitzsimmons, J.R., King, W., Desai, P., 2003.Activation of the visual cortex in motivated attention. Behavioral Neuroscience117, 369–380.
Buysse, D.J., Reynolds, C.F., Monk, T.H., Berman, S.R., Kupfer, D.J., 1989. ThePittsburgh Sleep Quality Index: a new instrument for psychiatric practice andresearch. Psychiatry Research 28, 193–213.
Carpenter, J.S., Andrykowski, M.A., 1998. Psychometric evaluation of the PittsburghSleep Quality Index. Journal of Psychosomatic Research 45, 5–13.
Chang, K., Adleman, N.E., Dienes, K., Simeonova, D.I., Menon, V., Reiss, A., 2004.Anomalous prefrontal-subcortical activation in familial pediatric bipolar dis-order: a functional magnetic resonance imaging investigation. Archives ofGeneral Psychiatry 61, 781–792.
Christophe, V., Antoine, P., Leroy, T., Delelis, G., 2009. Évaluation de deux stratégiesde régulation émotionnelle: la suppression expressive et la réévaluationcognitive. Revue Européenne de Psychologie Appliquée/European Review ofApplied Psychology 59, 59–67.
Curran-Everett, D., 2000. Multiple comparisons: philosophies and illustrations.American Journal of Physiology - Regulatory, Integrative and ComparativePhysiology 279, R1–R8.
El-Mallakh, R.S., Hollifield, M., 2008. Comorbid anxiety in bipolar disorder alterstreatment and prognosis. Psychiatric Quarterly 79, 139–150.
El-Mallakh, R.S., Karippot, A., 2005. Antidepressant-associated chronic irritabledysphoria (acid) in bipolar disorder: a case series. Journal of Affective Disorders84, 267–272.
Favre, S., Aubry, J.-M., Gex-Fabry, M., Ragama-Pardos, E., McQuillan, A., Bertschy, G.,2003. Translation and validation of a French version of the Young Mania RatingScale (YMRS). Encephale 29, 499–505.
Franzen, P.L., Buysse, D.J., Dahl, R.E., Thompson, W., Siegle, G.J., 2009. Sleepdeprivation alters pupillary reactivity to emotional stimuli in healthy youngadults. Biological Psychology 80, 300–305.
Giakoumaki, S.G., Bitsios, P., Frangou, S., Roussos, P., Aasen, I., Galea, A., Kumari, V.,2010. Low baseline startle and deficient affective startle modulation in remittedbipolar disorder patients and their unaffected siblings. Psychophysiology 47,659–668.
Gross, J.J., 1998. Antecedent- and response-focused emotion regulation: divergentconsequences for experience, expression, and physiology. Journal of Personalityand Social Psychology 74, 224–237.
Gross, J.J., 2002. Emotion regulation: affective, cognitive, and social consequences.Psychophysiology 39, 281–291.
Gross, J.J., John, O.P., 2003. Individual differences in two emotion regulationprocesses: implications for affect, relationships, and well-being. Journal ofPersonality and Social Psychology 85, 348–362.
Grühn, D., Scheibe, S., 2008. Age-related differences in valence and arousal ratingsof pictures from the International Affective Picture System (IAPS): do ratingsbecome more extreme with age? Behavior Research Methods 40, 512–521.
Hassel, S., Almeida, J.R., Kerr, N., Nau, S., Ladouceur, C.D., Fissell, K., Kupfer, D.J.,Phillips, M.L., 2008. Elevated striatal and decreased dorsolateral prefrontalcortical activity in response to emotional stimuli in euthymic bipolar disorder:no associations with psychotropic medication load. Bipolar Disorders 10,916–927.
Havermans, R., Nicolson, N.A., Berkhof, J., deVries, M.W., 2010. Mood reactivity todaily events in patients with remitted bipolar disorder. Psychiatry Research179, 47–52.
Hawley, C.J., Gale, T.M., Sivakumaran, T., 2002. Defining remission by cut off scoreon the MADRS: selecting the optimal value. Journal of Affective Disorders 72,177–184.
Henry, C., M'Bailara, K., Mathieu, F., Poinsot, R., Falissard, B., 2008a. Constructionand validation of a dimensional scale exploring mood disorders: MAThyS(Multidimensional Assessment of Thymic States). BMC Psychiatry 8, 82.
Henry, C., Van den Bulke, D., Bellivier, F., Roy, I., Swendsen, J., M'Bailara, K., Siever, L.J.,Leboyer, M., 2008b. Affective lability and affect intensity as core dimensions ofbipolar disorders during euthymic period. Psychiatry Research 159, 1–6.
Holmes, T.H., Rahe, R.H., 1967. The social readjustment rating scale. Journal ofPsychosomatic Research 11, 213–218.
Hothorn, T., Bretz, F., Westfall, P., 2008. Simultaneous inference in general para-metric models. Biometrical Journal 50, 346–363.
Irtel, H., 2007. PXLab: The Psychological Experiments Laboratory. University ofMannheim, Mannheim (Germany).
Kleinginna, P.R., Kleinginna, A.M., 1981. A categorized list of emotion definitions, withsuggestions for a consensual definition. Motivation and Emotion 5, 345–379.
Lang, P.J., Bradley, M.M., Cuthbert, B.N., 2008. International affective picture system(IAPS): Affective ratings of pictures and instruction manual (Technical ReportA-8). University of Florida, Gainesville, FL.
Little, A.C., Jones, B.C., DeBruine, L.M., 2011. The many faces of research on faceperception. Philosophical Transactions of the Royal Society B: Biological Science366, 1634–1637.
Loewenfeld, I.E., 1999. The Pupil: Anatomy, Physiology, and Clinical Applications.Butterworth-Heinemann, Boston.
M'bailara, K., Demotes-Mainard, J., Swendsen, J., Mathieu, F., Leboyer, M., Henry, C.,2009. Emotional hyper-reactivity in normothymic bipolar patients. BipolarDisorders 11, 63–69.
Martineau, J., Hernandez, N., Hiebel, L., Roché, L., Metzger, A., Bonnet-Brilhault, F.,2011. Can pupil size and pupil responses during visual scanning contribute tothe diagnosis of autism spectrum disorder in children? Journal of PsychiatricResearch 45, 1077–1082.
Merikangas, K.R., Akiskal, H.S., Angst, J., Greenberg, P.E., Hirschfeld, R.M.A.,Petukhova, M., Kessler, R.C., 2007. Lifetime and 12-month prevalence of bipolarspectrum disorder in the National Comorbidity Survey replication. Archives ofGeneral Psychiatry 64, 543–552.
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 7
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i

Montgomery, S.A., Asberg, M., 1979. A new depression scale designed to besensitive to change. British Journal of Psychiatry 134, 382–389.
Myin-Germeys, I., Peeters, F., Havermans, R., Nicolson, N.A., DeVries, M.W.,Delespaul, P., Van Os, J., 2003. Emotional reactivity to daily life stress inpsychosis and affective disorder: an experience sampling study. Acta Psychia-trica Scandinavica 107, 124–131.
Perugi, G., Toni, C., Maremmani, I., Tusini, G., Ramacciotti, S., Madia, A., Fornaro, M.,Akiskal, H.S., 2010. The influence of affective temperaments and psychopatho-logical traits on the definition of bipolar disorder subtypes: a study on Bipolar IItalian National sample. Journal of Affective Disorders 136, 41–49.
Phillips, M.L., Travis, M.J., Fagiolini, A., Kupfer, D.J., 2008. Medication effects inneuroimaging studies of bipolar disorder. American Journal of Psychiatry 165,313–320.
Pinheiro, J., Bates, D., DebRoy, S., Sarkar, D., the R Development Core Team, 2013.nlme: Linear and Nonlinear Mixed Effects Models.
Pinheiro, J.C., Bates, D.M., 2009. Mixed-Effects Models in S and S-Plus, 1st ed. 2000.2nd printing. ed. Springer-Verlag, New York (Inc).
R Development Core Team, 2013. R: A Language and Environment for StatisticalComputing. R Foundation for Statistical Computing, Vienna, Austria.
Rosso, G., Albert, U., Bogetto, F., Maina, G., 2009. Axis II comorbidity in euthymicbipolar disorder patients: no differences between bipolar I and II subtypes.Journal of Affective Disorders 115, 257–261.
Samalin, L., Llorca, P.M., Giordana, B., Milhiet, V., Yon, L., El-Hage, W., Courtet, P.,Hacques, E., Bedira, N., Filipovics, A., Arnaud, R., Dillenschneider, A., Bellivier, F.,2014. Residual symptoms and functional performance in a large sample ofeuthymic bipolar patients in France (the OPTHYMUM study). Journal ofAffective Disorders 159, 94–102.
Sheehan, D.V., Lecrubier, Y., Sheehan, K.H., Amorim, P., Janavs, J., Weiller, E.,Hergueta, T., Baker, R., Dunbar, G.C., 1998. The Mini-International Neuropsy-chiatric Interview (M.I.N.I.): the development and validation of a structureddiagnostic psychiatric interview for DSM-IV and ICD-10. Journal of ClinicalPsychiatry 59 (Suppl 20), 22–33 (quiz 34–57).
Tempesta, D., Couyoumdjian, A., Curcio, G., Moroni, F., Marzano, C., De Gennaro, L.,Ferrara, M., 2010. Lack of sleep affects the evaluation of emotional stimuli. BrainResearch Bulletin 82, 104–108.
Tursky, B., Shapiro, D., Crider, A., Kahneman, D., 1969. Pupillary, heart rate, and skinresistance changes during a mental task. Journal of Experimental Psychology79, 164–167.
Versace, A., Thompson, W.K., Zhou, D., Almeida, J.R.C., Hassel, S., Klein, C.R., Kupfer,D.J., Phillips, M.L., 2010. Abnormal left and right amygdala-orbitofrontal corticalfunctional connectivity to emotional faces: state versus trait vulnerabilitymarkers of depression in bipolar disorder. Biological Psychiatry 67, 422–431.
Young, R.C., Biggs, J.T., Ziegler, V.E., Meyer, D.A., 1978. A rating scale for mania:reliability, validity and sensitivity. British Journal of Psychiatry 133, 429–435.
M. Lemaire et al. / Psychiatry Research ∎ (∎∎∎∎) ∎∎∎–∎∎∎8
Please cite this article as: Lemaire, M., et al., Subjective and physiological emotional response in euthymic bipolar patients: Apilot study. Psychiatry Research (2014), http://dx.doi.org/10.1016/j.psychres.2014.07.002i