Embed Size (px)
Citation preview
2013
Seminars in Ophthalmology, 2014; 29(1): 11–17! Informa Healthcare USA, Inc.
ISSN: 0882-0538 print / 1744-5205 online
DOI: 10.3109/08820538.2013.839813
Subfoveal Choroidal Thickness in Preeclampsia:Comparison with Normal Pregnant and
Nonpregnant Women
Nihat Sayin1, Necip Kara2, Dilara Pirhan1 , Asli Vural1, Hatice Bilge Araz Ersan1,Ali Ismet Tekirdag3, Ibrahim Polat3, Bekir Gulac3, and Gokce Yilmaz3
1Department of Ophthalmology, Kanuni Sultan Suleyman Education and Research Hospital, Istanbul, Turkey,2Department of Ophthalmology, Sehitkamil State Hospital, Gaziantep, Turkey, and 3Department of Obstetrics &
Gynecology, Kanuni Sultan Suleyman Education and Research Hospital, Istanbul, Turkey
ABSTRACT
Purpose: To compare the subfoveal choroidal thickness (SFCT) in preeclampsia, normal pregnancy, and non-pregnant women using enhanced depth imaging optical coherence tomography (EDI-OCT). Methods: Onehundred nineteen volunteers were enrolled in this prospective and comparative study. The participants weredivided into three groups: group 1 (33 preeclamptic women), group 2 (46 normal pregnant), and group 3 (40non-pregnant healthy women). The SFCT was measured by EDI-OCT. The refractive error, intraocular pressure(IOP), axial length (AL), central corneal thickness (CCT), systolic and diastolic blood pressure, and ocularperfusion pressure (OPP) were also measured. Medical records of pregnant women, including gestational age,maternal weight gain, weight, and proteinuria, were noted. Results: Mean SFCT of groups 1, 2, and 3 were333.8� 55.3 mm (range 235-440mm), 368.6� 67.6 mm (range 223-517 mm), and 334.8� 59.9 mm (range 197-432mm),respectively. The mean SFCT was thicker in group 2 than that in groups 1 and 3 (p = 0.045 and p = 0.038,respectively), whereas no significant difference was seen between groups 1 and 3 (p = 1.0). In group 1, SFCTshowed a negative correlation with the CCT (p = 0.009, r = -0.493). In group 2, SFCT showed a positivecorrelation with OPP (p = 0.030, r = 0.321) and a negative correlation with gestational age and fetal weight(p = 0.008, r = -0.387 and p = 0.011, r = -0.373, respectively). Conclusion: Our results suggested that SFCT wassignificantly thicker in normal pregnant women than non-pregnant women. However, SFCT values ofpreeclamptic women were similar to those of non-pregnant women.
Keywords: Preeclampsia, pregnancy, subfoveal choroidal thickness
INTRODUCTION
Preeclampsia is an obstetric disorder characterized byhypertension, peripheral edema, and proteinuria.1,2
It affects approximately 5% of pregnant women.3–7
Preeclampsia is a multisystem disorder that can causecardiovascular changes, hematologic abnormalities,hepatic and renal impairment, and neurologic orcerebral manifestations.8,9
Pregnancy may induce several ocular changes,including a decrease in corneal sensitivity, an increasein central corneal thickness (CCT) and curvature, a
decrease in intraocular pressure (IOP), and changes invision and ocular blood flow.10–14 Pregnancy compli-cated by preeclampsia may also lead to numerousocular alterations, including visual symptoms (e.g.,decreased vision, photopsia, and visual field defects)and abnormalities of the conjunctiva, retina andretinal vasculature, optic nerve, visual cortex, andchoroid.15–17
The choroid is the most vascular structure withinthe eye, 18 and the fovea, situated at the center of themacula, has the highest photoreceptor density andmetabolic activity. The choroid, being a vascular
Correspondence: Nihat Sayin, Atakent Mahallesi, 4, Cadde. C 2-7 Blok, Kat: 3 Daire: 13, Kucukcekmece, Istanbul, Turkey. E-mail:[email protected]
Received 26 May 2013; accepted 20 August 2013; published online 26 November 2013
11
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.
structure, is prone to being affected by systemicconditions such as hypertension. Chorioretinal find-ings in preeclampsia consist of acute changes, includ-ing serous retinal detachment and retinal pigmentepithelial lesions secondary to choroidal ischemia, aswell as occlusive retinal vascular disease. Latechanges include retinal vascular narrowing, opticatrophy, atrophic pigmentary changes, and Elschnigspots.19–21
Traditional imaging modalities, such as indocya-nine green angiography and B-scan ultrasonography,are limited in image resolution and measurementaccuracy. Also, the invasive nature of angiographylimits their potential diagnostic use in pregnantwomen because of the possible maternal and fetalcomplications.22 However, magnetic resonance ima-ging is non-invasive, yet differentiation betweenretina, choroid, and sclera is difficult.23
Until recently, choroidal thickness could not beaccurately measured by any imaging modality Arecent modification to the standard optical coherencetomography technique, called enhanced depth ima-ging optical coherence tomography (EDI-OCT), offersa non-invasive, rapid, objective, and reliable diagnos-tic modality for the imaging of choroidal alterationsand allows in-vivo examination and quantification ofthe choroid. Many previous studies have focused onmeasuring subfoveal choroidal thickness (SFCT) inhealthy participants as well as those with severalpathologies.24–30 However, there has been no qualita-tive and quantitative study on choroidal morphologyin preeclampsia. The purpose of the current study isto evaluate SFCT measured by EDI-OCT inpreeclampsia.
METHODS
Study Population and Design
This prospective and comparative study was per-formed at the Obstetrics and Gynecology andOphthalmology Departments of Istanbul KanuniSultan Suleyman Education and Research Hospital.The study followed the tenets of the Declaration ofHelsinki and was approved by the local ethicscommittee. All participants received oral and writteninformation about the study, and each participantprovided written informed consent.
The participants were divided into three groups.Group 1 consisted of pregnant women complicated bypreeclampsia. Group 2 consisted of healthy pregnantwomen. Group 3 consisted of non-pregnant healthywomen. Ocular exclusion criteria included the fol-lowing: a best-corrected visual acuity worse than 20/20, glaucomatous optic disc changes such as excava-tion, notching, or focal thinning of the neuroretinalrim, peripapillary hemorrhage, glaucomatous visual
field defects, IOP readings greater than 22 mmHg,more than 2 diopters of cylindrical and/or 5 dioptersof spherical refractive error, poor image quality, anyhistory of ocular diseases, and history of previousintraocular surgery or laser therapy. Extraocularexclusion criteria included a history of systemicdisease such as hypertension or diabetes mellitus,and the development of complications such aspreeclampsia (except group 1).
Examination Protocol and StudyMeasurements
All participants underwent a detailed ophthalmologicexamination, including medical history, refractiveerror, best-corrected visual acuity, slit lamp micros-copy, intraocular pressure, and funduscopic examin-ation. A complete medical history includinggestational age, fetal weight, and maternal weightgain was recorded. The quantification of 24-hourproteinuria and measured by dipstick values werealso noted. Study participants underwent centralcorneal thickness (CCT) and axial length (AL) meas-urements using ultrasonic scans. Systolic blood pres-sure (sBP) and diastolic blood pressure (dBP) weremeasured before the choroidal thickness measure-ment. Mean blood pressure (mBP) was calculated asthe dBP plus one-third of the difference between sBPand dBP. The ocular perfusion pressure (OPP) wascalculated by measuring the difference between twoout of three of the mBP and the IOP values.31,32
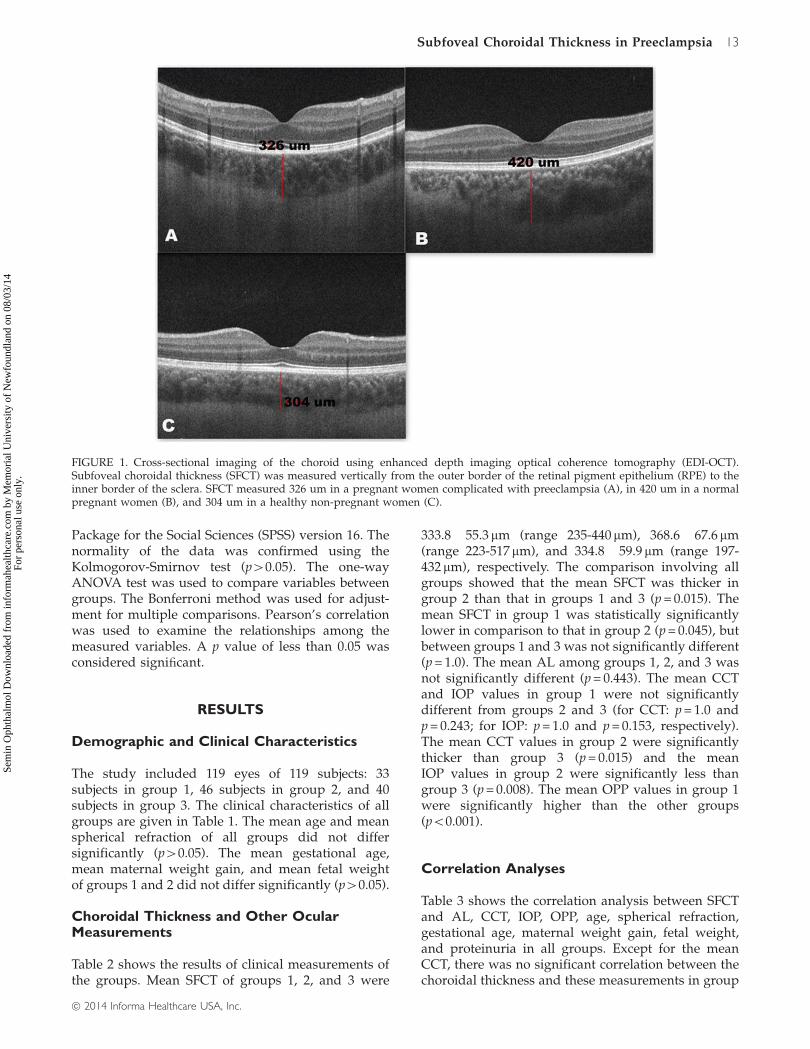
EDI-OCT Measurement: The SFCT was measuredusing spectral domain OCT (Cirrus-HD OCT, CarlZeiss Meditec, Inc., Dublin, CA). The scan patternused on Cirrus HD-OCT was HD 5 Line Raster spacedat 0.25 mm. It is a 6 mm line consisting of 1024 A-scan/B-scan and averaging 4 B-scans per image. To beincluded in this study, images had to be taken as closeto the fovea as possible by choosing to image thethinnest point of the macula, with the understandingthat slight differences in positioning could affect themeasured thickness. Only high-quality images withsignal-to-noise ratio 47 were selected for the study.SFCT was determined as the vertical distance from thehyperreflective line of the hyperreflective RPE to theline of the inner surface of the sclera centered on thefovea using a measuring tool with built-in linearmeasuring. The choroidal thickness measurementswere performed by one ophthalmologist (NS) andassessed by one ophthalmologist (DP) who weremasked in terms of groups (Figure 1).
Data Analyses
One eye per patient was selected for the analyses. Allstatistical analyses were performed using Statistical
12 N. Sayin et al.
Seminars in Ophthalmology
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.
Package for the Social Sciences (SPSS) version 16. Thenormality of the data was confirmed using theKolmogorov-Smirnov test (p40.05). The one-wayANOVA test was used to compare variables betweengroups. The Bonferroni method was used for adjust-ment for multiple comparisons. Pearson’s correlationwas used to examine the relationships among themeasured variables. A p value of less than 0.05 wasconsidered signiEcant.
RESULTS
Demographic and Clinical Characteristics
The study included 119 eyes of 119 subjects: 33subjects in group 1, 46 subjects in group 2, and 40subjects in group 3. The clinical characteristics of allgroups are given in Table 1. The mean age and meanspherical refraction of all groups did not differsignificantly (p40.05). The mean gestational age,mean maternal weight gain, and mean fetal weightof groups 1 and 2 did not differ significantly (p40.05).
Choroidal Thickness and Other OcularMeasurements
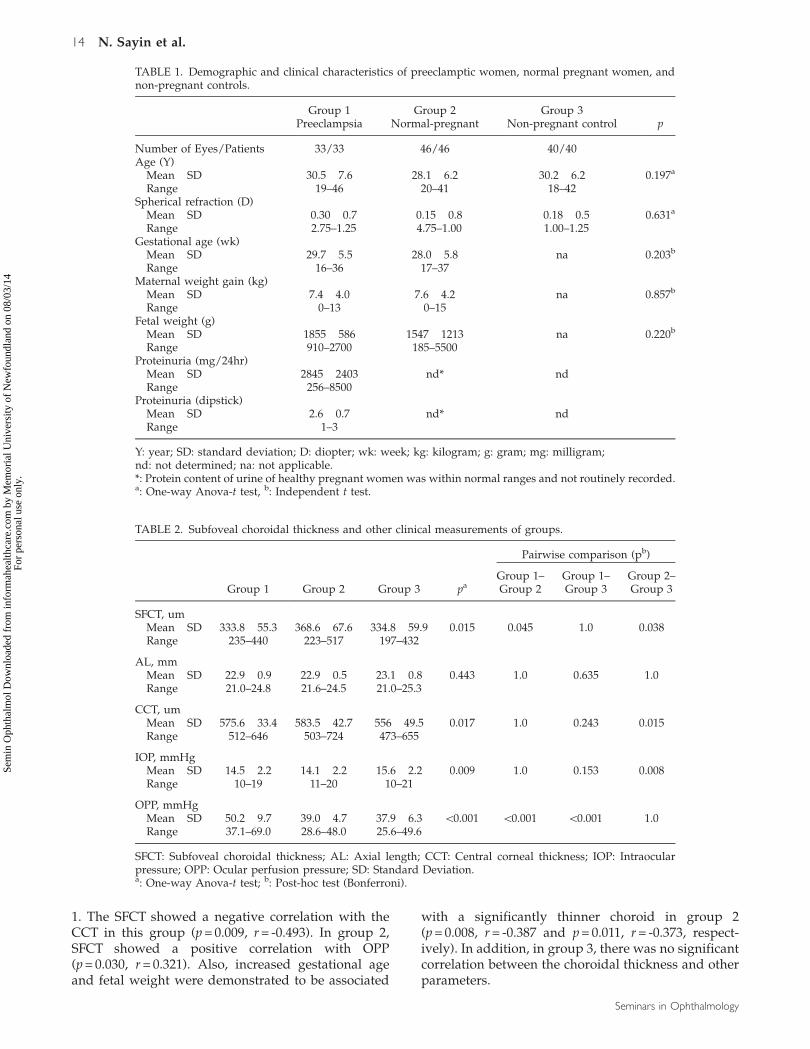
Table 2 shows the results of clinical measurements ofthe groups. Mean SFCT of groups 1, 2, and 3 were
333.8� 55.3 mm (range 235-440 mm), 368.6� 67.6 mm(range 223-517 mm), and 334.8� 59.9 mm (range 197-432 mm), respectively. The comparison involving allgroups showed that the mean SFCT was thicker ingroup 2 than that in groups 1 and 3 (p = 0.015). Themean SFCT in group 1 was statistically significantlylower in comparison to that in group 2 (p = 0.045), butbetween groups 1 and 3 was not significantly different(p = 1.0). The mean AL among groups 1, 2, and 3 wasnot significantly different (p = 0.443). The mean CCTand IOP values in group 1 were not significantlydifferent from groups 2 and 3 (for CCT: p = 1.0 andp = 0.243; for IOP: p = 1.0 and p = 0.153, respectively).The mean CCT values in group 2 were significantlythicker than group 3 (p = 0.015) and the meanIOP values in group 2 were significantly less thangroup 3 (p = 0.008). The mean OPP values in group 1were significantly higher than the other groups(p50.001).
Correlation Analyses
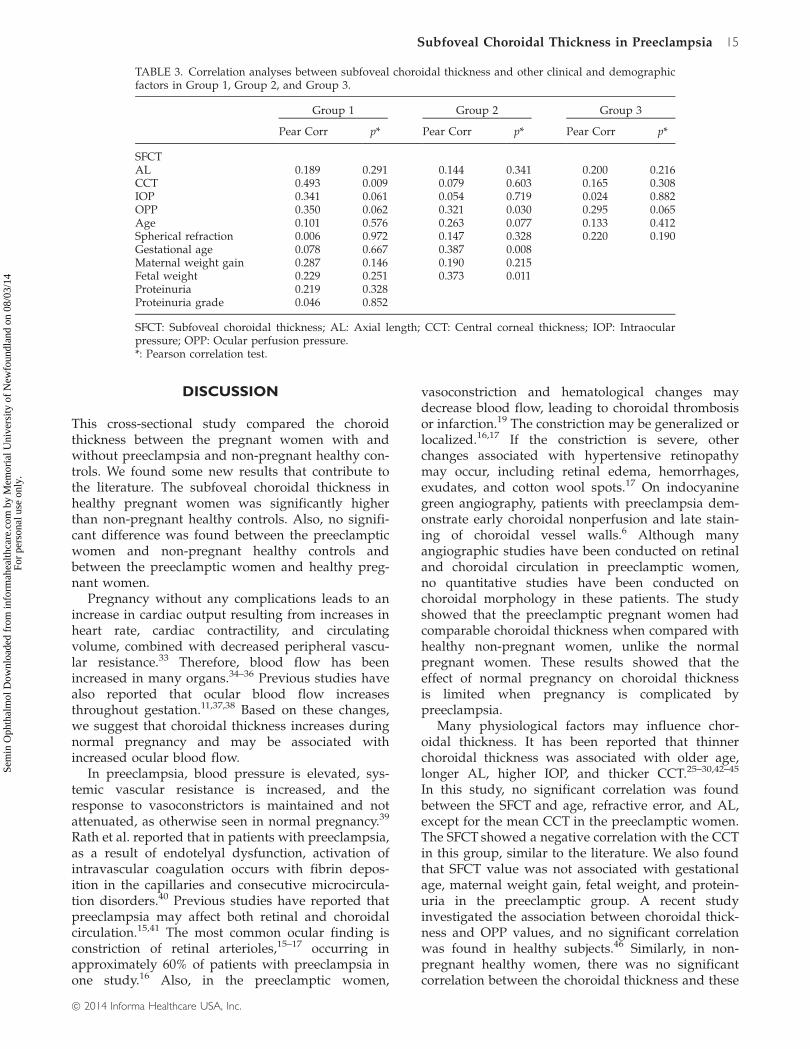
Table 3 shows the correlation analysis between SFCTand AL, CCT, IOP, OPP, age, spherical refraction,gestational age, maternal weight gain, fetal weight,and proteinuria in all groups. Except for the meanCCT, there was no significant correlation between thechoroidal thickness and these measurements in group
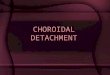
FIGURE 1. Cross-sectional imaging of the choroid using enhanced depth imaging optical coherence tomography (EDI-OCT).Subfoveal choroidal thickness (SFCT) was measured vertically from the outer border of the retinal pigment epithelium (RPE) to theinner border of the sclera. SFCT measured 326 um in a pregnant women complicated with preeclampsia (A), in 420 um in a normalpregnant women (B), and 304 um in a healthy non-pregnant women (C).
Subfoveal Choroidal Thickness in Preeclampsia 13
! 2014 Informa Healthcare USA, Inc.
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.
1. The SFCT showed a negative correlation with theCCT in this group (p = 0.009, r = -0.493). In group 2,SFCT showed a positive correlation with OPP(p = 0.030, r = 0.321). Also, increased gestational ageand fetal weight were demonstrated to be associated
with a significantly thinner choroid in group 2(p = 0.008, r = -0.387 and p = 0.011, r = -0.373, respect-ively). In addition, in group 3, there was no significantcorrelation between the choroidal thickness and otherparameters.
TABLE 1. Demographic and clinical characteristics of preeclamptic women, normal pregnant women, andnon-pregnant controls.
Group 1 Group 2 Group 3Preeclampsia Normal-pregnant Non-pregnant control p
Number of Eyes/Patients 33/33 46/46 40/40Age (Y)
Mean� SD 30.5� 7.6 28.1� 6.2 30.2� 6.2 0.197a
Range 19–46 20–41 18–42Spherical refraction (D)
Mean� SD �0.30� 0.7 �0.15� 0.8 �0.18� 0.5 0.631a
Range �2.75–1.25 �4.75–1.00 �1.00–1.25Gestational age (wk)
Mean� SD 29.7� 5.5 28.0� 5.8 na 0.203b
Range 16–36 17–37Maternal weight gain (kg)
Mean� SD 7.4� 4.0 7.6� 4.2 na 0.857b
Range 0–13 0–15Fetal weight (g)
Mean� SD 1855� 586 1547� 1213 na 0.220b
Range 910–2700 185–5500Proteinuria (mg/24hr)
Mean� SD 2845� 2403 nd* ndRange 256–8500
Proteinuria (dipstick)Mean� SD 2.6� 0.7 nd* ndRange 1–3
Y: year; SD: standard deviation; D: diopter; wk: week; kg: kilogram; g: gram; mg: milligram;nd: not determined; na: not applicable.*: Protein content of urine of healthy pregnant women was within normal ranges and not routinely recorded.a: One-way Anova-t test, b: Independent t test.
TABLE 2. Subfoveal choroidal thickness and other clinical measurements of groups.
Pairwise comparison (pb)
Group 1 Group 2 Group 3 paGroup 1–Group 2
Group 1–Group 3
Group 2–Group 3
SFCT, umMean� SD 333.8� 55.3 368.6� 67.6 334.8� 59.9 0.015 0.045 1.0 0.038Range 235–440 223–517 197–432
AL, mmMean� SD 22.9� 0.9 22.9� 0.5 23.1� 0.8 0.443 1.0 0.635 1.0Range 21.0–24.8 21.6–24.5 21.0–25.3
CCT, umMean� SD 575.6� 33.4 583.5� 42.7 556� 49.5 0.017 1.0 0.243 0.015Range 512–646 503–724 473–655
IOP, mmHgMean� SD 14.5� 2.2 14.1� 2.2 15.6� 2.2 0.009 1.0 0.153 0.008Range 10–19 11–20 10–21
OPP, mmHgMean� SD 50.2� 9.7 39.0� 4.7 37.9� 6.3 50.001 50.001 50.001 1.0Range 37.1–69.0 28.6–48.0 25.6–49.6
SFCT: Subfoveal choroidal thickness; AL: Axial length; CCT: Central corneal thickness; IOP: Intraocularpressure; OPP: Ocular perfusion pressure; SD: Standard Deviation.a: One-way Anova-t test; b: Post-hoc test (Bonferroni).
14 N. Sayin et al.
Seminars in Ophthalmology
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.
DISCUSSION
This cross-sectional study compared the choroidthickness between the pregnant women with andwithout preeclampsia and non-pregnant healthy con-trols. We found some new results that contribute tothe literature. The subfoveal choroidal thickness inhealthy pregnant women was significantly higherthan non-pregnant healthy controls. Also, no signifi-cant difference was found between the preeclampticwomen and non-pregnant healthy controls andbetween the preeclamptic women and healthy preg-nant women.
Pregnancy without any complications leads to anincrease in cardiac output resulting from increases inheart rate, cardiac contractility, and circulatingvolume, combined with decreased peripheral vascu-lar resistance.33 Therefore, blood flow has beenincreased in many organs.34–36 Previous studies havealso reported that ocular blood flow increasesthroughout gestation.11,37,38 Based on these changes,we suggest that choroidal thickness increases duringnormal pregnancy and may be associated withincreased ocular blood flow.
In preeclampsia, blood pressure is elevated, sys-temic vascular resistance is increased, and theresponse to vasoconstrictors is maintained and notattenuated, as otherwise seen in normal pregnancy.39
Rath et al. reported that in patients with preeclampsia,as a result of endotelyal dysfunction, activation ofintravascular coagulation occurs with fibrin depos-ition in the capillaries and consecutive microcircula-tion disorders.40 Previous studies have reported thatpreeclampsia may affect both retinal and choroidalcirculation.15,41 The most common ocular finding isconstriction of retinal arterioles,15–17 occurring inapproximately 60% of patients with preeclampsia inone study.16 Also, in the preeclamptic women,
vasoconstriction and hematological changes maydecrease blood flow, leading to choroidal thrombosisor infarction.19 The constriction may be generalized orlocalized.16,17 If the constriction is severe, otherchanges associated with hypertensive retinopathymay occur, including retinal edema, hemorrhages,exudates, and cotton wool spots.17 On indocyaninegreen angiography, patients with preeclampsia dem-onstrate early choroidal nonperfusion and late stain-ing of choroidal vessel walls.6 Although manyangiographic studies have been conducted on retinaland choroidal circulation in preeclamptic women,no quantitative studies have been conducted onchoroidal morphology in these patients. The studyshowed that the preeclamptic pregnant women hadcomparable choroidal thickness when compared withhealthy non-pregnant women, unlike the normalpregnant women. These results showed that theeffect of normal pregnancy on choroidal thicknessis limited when pregnancy is complicated bypreeclampsia.
Many physiological factors may influence chor-oidal thickness. It has been reported that thinnerchoroidal thickness was associated with older age,longer AL, higher IOP, and thicker CCT.25–30,42–45
In this study, no significant correlation was foundbetween the SFCT and age, refractive error, and AL,except for the mean CCT in the preeclamptic women.The SFCT showed a negative correlation with the CCTin this group, similar to the literature. We also foundthat SFCT value was not associated with gestationalage, maternal weight gain, fetal weight, and protein-uria in the preeclamptic group. A recent studyinvestigated the association between choroidal thick-ness and OPP values, and no significant correlationwas found in healthy subjects.46 Similarly, in non-pregnant healthy women, there was no significantcorrelation between the choroidal thickness and these
TABLE 3. Correlation analyses between subfoveal choroidal thickness and other clinical and demographicfactors in Group 1, Group 2, and Group 3.
Group 1 Group 2 Group 3
Pear Corr p* Pear Corr p* Pear Corr p*
SFCTAL �0.189 0.291 �0.144 0.341 0.200 0.216CCT �0.493 0.009 �0.079 0.603 �0.165 0.308IOP �0.341 0.061 0.054 0.719 �0.024 0.882OPP 0.350 0.062 0.321 0.030 0.295 0.065Age 0.101 0.576 �0.263 0.077 �0.133 0.412Spherical refraction 0.006 0.972 0.147 0.328 �0.220 0.190Gestational age �0.078 0.667 �0.387 0.008Maternal weight gain �0.287 0.146 �0.190 0.215Fetal weight 0.229 0.251 �0.373 0.011Proteinuria �0.219 0.328Proteinuria grade 0.046 0.852
SFCT: Subfoveal choroidal thickness; AL: Axial length; CCT: Central corneal thickness; IOP: Intraocularpressure; OPP: Ocular perfusion pressure.*: Pearson correlation test.
Subfoveal Choroidal Thickness in Preeclampsia 15
! 2014 Informa Healthcare USA, Inc.
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.
measurements. However, SFCT showed a positivecorrelation with OPP and negative correlation withgestational age and fetal weight in pregnant womenwithout preeclampsia.
To the best of our knowledge, our study is the firstwork that has assessed choroidal thickness in pre-eclamptic women and its association with ocularparameters and pregnancy-related factors. On theother hand, the present study had several limitations.Repeatability is critical when an imaging technique isto be implemented in practice. For EDI-OCT, there isno automated software to measure choroidal thick-ness. All measurements must be done manually. Thisraises concern regarding inter-observer and inter-session repeatability. Although good inter-observerrepeatability was produced with manual measure-ments, there are still some difficulties. The mainproblems are the relatively lower resolution in chor-oidal images than in conventional retinal scans andthe lack of eye-tracking in some models of OCT (onlythe Heidelberg Spectralis is currently able to performeye-tracking for EDI-OCT). To enhance repeatability,automated measurement software should be devel-oped for choroidal measurements and eye-trackingfunction should be ideally incorporated into everyOCT machine.
In summary, SFCT in normal pregnant womenwas significantly thicker than in non-pregnanthealthy women, whereas SFCT values of preeclamp-tic pregnant were similar to non-pregnant women.However, SFCT values showed a significant correl-ation with only central corneal thickness in thepreeclamptic women. This result should be takeninto consideration when choroidal thickness isevaluated for pregnancy-related disease or clinicalresearch. Improved in-vivo visualization of thechoroid and measurement of choroidal thicknessusing EDI-OCT could improve our understanding ofa variety of pregnancy-related disorders such aspreeclampsia in the future.
DECLARATION OF INTEREST
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing ofthe paper.
REFERENCES
1. Sunness JS. The pregnant woman’s eye. Surv Ophthalmol1988;32:219–238.
2. Schultz KL, Birnbaum AD, Goldstein DA. Ocular diseasein pregnancy. Curr Opin Ophthalmol 2005;6:308–314.
3. Correa MD, Correa JR MD. Doenca hipertensiva especıficada gravidez. In:Nocoes Praticas de Obstetrıcia. Correa MD,ed. Belo Horizonte: Editora Coopmed, 1999. pp 392–405.
4. Aburymra S. Doencas retinianas da gravidez. In:Retina e Vıtreo: Clınica e Cirurgia Sociedade Brasileirade Retina e Vıtreo e Conselho Brasileiro deOftalmologia, ed. Sao Paulo: Editora Roca, 2000. pp584–585.
5. Kahhale S, Zugaib M. Sındromes Hipertensivas naGravidez; Sao Paulo: Atheneu, 1995. pp 107–121.
6. Valluri S, Adelberg D, Curtis R, Olk RJ. Diagnosticindocyanine green angiography in preeclampsia. Am JOphthal 1996;122:672–677.
7. Ober RR. Pregnancy-induced hypertension (preeclampsia-eclampsia). In: Retina, 2nd ed., vol. 2 Ryan SJ, ed. Mosby:St. Louis, 1994. pp 1405–1411.
8. ACOG Practice Bulletin Committee. Diagnosis and man-agement of preeclampsia and eclampsia. Obstet Gynecol2002;99:159–167.
9. ACOG Practice Bulletin Committee. Diagnosis and man-agement of preeclampsia and eclampsia. Obstet Gynecol2002;99:159–167; Drife JO, Magowan, editors. Clinicalobstetrics and gynaecology. pp. 367–70 [chap. 39].
10. Weinreb RN, Lu A, Beeson C. Maternal cornealthickness during pregnancy. Am J Ophthalmol 1988;105:258–260.
11. Chen HC, Newsom RS, Patel V, et al. Retinal blood flowchanges during pregnancy in women with diabetes. InvestOphthalmol Vis Sci 1994;35:3199–3208.
12. Horven I, Gjonnaess H. Corneal indentation pulse andintraocular pressure in pregnancy. Arch Ophthalmol 1974;91:92–98.
13. Kass MA, Sears ML. Hormonal regulation of intraocularpressure. Surv Ophthalmol 1977;22:153–176.
14. Akar Y, Yucel I, Akar ME, et al. Effect of pregnancy onintra-observer and inter-technique agreement in intraocu-lar pressure measurements. Ophthalmologica 2005;219:43–48.
15. Jaffe G, Schatz H. Ocular manifestations of preeclampsia.Am J Ophthalmol 1987;103:309–315.
16. Hallum AV. Eye changes in hypertensive toxemia ofpregnancy: A study of three hundred cases. JAMA 1936;106:1649–1651.
17. Hallum AV. Changes in the retinal arterioles associatedwith the hypertensions of pregnancy. Arch Ophthalmol1947;37:472–490.
18. Huang D, Swanson EA, Lin CP, et al. Optical coherencetomography. Science 1991;254:1178–1181.
19. Saito Y, Tano Y. Retinal pigment epithelial lesionsassociated with choroidal ischemia in preeclampsia.Retina 1998;18:103–108.
20. Wang CL. Exudative retinal detachment in the pregnancy-induced hypertension syndrome. Chang Hua Yen Ko TsaChih 1992;2:77–79.
21. Bos AM, Van Loon AJ, Ameln JG. Serous retinal detach-ment in preeclampsia. Ned Tijdschr Geneeskd 1999;143:2430–2432.
22. Somfai GM, Mihaltz K, Tulassay E, Rigo Jr J. Diagnosis ofserous neuroretinal detachments of the macula in severepreeclamptic patients with optical coherence tomography.Hypertens Pregnancy 2006;25:11–20.
23. Weber AL, Mafee MF. Evaluation of the globe usingcomputed tomography and magnetic resonance imaging.Isr J Med Sci 1992;28:145–152.
24. Spaide RF, Koizumi H, Pozonni MC. Enhanced depthimaging spectral-domain optical coherence tomography.Am J Ophthalmol 2008;146:496–500.
25. Ikuno Y, Kawaguchi K, Nouchi T, Yasuno Y. Choroidalthickness in healthy Japanese subjects. Invest OphthalmolVis Sci 2010;51:2173–2176.
26. Brown JS, Flitcroft DI, Ying GS, et al. In vivohuman choroidal thickness measurements: Evidence
16 N. Sayin et al.
Seminars in Ophthalmology
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.

for diurnal Fuctuations. Invest Ophthalmol Vis Sci 2009;50:5–12.
27. Margolis R, Spaide RF. A pilot study of enhanced depthimaging optical coherence tomography of the choroid innormal eyes. Am J Ophthalmol 2009;147:811–815.
28. Fujiwara T, Imamura Y, Margolis R. Enhanced depthimaging optical coherence tomography of the choroid inhighly myopic eyes. Am J Ophthalmol 2009;148:445–450.
29. Esmaeelpour M, Povazay B, Herman B, et al. Three-dimensional 1060 nm OCT: Choroidal thickness maps innormal subjects and improved posterior segment visual-ization in cataract patients. Invest Ophthalmol Vis Sci 2010;51:5260–5266.
30. Manjunath V, Taha M, Fujimoto JG, Duker JS. Choroidalthickness in normal eyes measured using Cirrus HDoptical coherence tomography. Am J Ophthalmol 2010;150:325–329.
31. Barbosa CP, Stefanini FR, Penha F, et al. Intraocularpressure and ocular perfusion during hemodialysis. ArqBras Oftalmol 2011;74:106–109.
32. Schmidl D, Weigert G, Dorner GT, et al. Role of adenosinein the control of choroidal blood flow during changes inocular perfusion pressure. Invest Ophthalmol Vis Sci 2011;52:6035–6039.
33. de Swiet M. Physiology in relation to pregnancy andlabour. In: Scientific Foundations of Obstetrics andGynaecology. Philipp E, Setchell M, Ginsburg J, eds.Oxford: Butterworth-Heinemann, 1991. pp 208–219.
34. Ikeda T, Ikenoue T, Mori N, et al. Effect of early pregnancyon maternal regional cerebral blood flow. Amf ObstetGynecol 1993;168:1303–1308.
35. Katz M, Sokal MM. Skin perfusion in pregnancy. AmfObstet Gynecol 1980;137:30–33.
36. Dunlop W. Serial changes in renal hemodynamics duringnormal human pregnancy. Brf Obstet Gynaecol 1981;88:l–9.
37. Centofanti M, Migliardi R, Bonini S, et al. Pulsatile ocularblood flow during pregnancy. Eur J Ophthalmol 2002;12:276–280.
38. Vigander K, Takserman A, Kerty E. Color doppler imagingof maternal retrobulbar blood flow in normal pregnancyand postpartum (a longitudinal study). Invest OphthalmolVis Sci 2004;45:E-Abstract 2621.
39. Morris NH, Eaton BM, and Dekker G. Nitric oxide, theendothelium, pregnancy and pre-eclampsia. Br J ObstetGynaecol 1996;103:4–15.
40. Rath W, Faridi A, Dudenhausen JW. HELLP syndrome.J Perinat Med 2000;28:249–260.
41. Bosco JAS. Spontaneous nontraumatic retinal detachmentin pregnacy. Am J Obstet Gynecol 1981;82:208–212.
42. Wong IY, Wong RL, Zhao P, Lai WW. Choroidal thicknessin relation to hypercholesterolemia on enhanced depthimaging optical coherence tomography. Retina 2013;33:423–428.
43. Agawa T, Miura M, Ikuno Y, et al. Choroidal thicknessmeasurement in healthy Japanese subjects by three-dimensional high-penetration optical coherence tomog-raphy. Graefes Arch Clin Exp Ophthalmol 2011;249:1485–1492.
44. Maul EA, Friedman DS, Chang DS, et al. Choroidalthickness measured by spectral domain optical coherencetomography: factors affecting thickness in glaucomapatients. Ophthalmology 2011;118:1571–1579.
45. Mwanza JC, Hochberg JT, Banitt MR, et al. Lack ofassociation between glaucoma and macular choroidalthickness measured with enhanced depth-imaging opticalcoherence tomography. Investig Ophthalmol Vis Sci 2011;52:3430–3435.
46. Wei WB, Xu L, Jonas JB, et al. Choroidal thickness: theBeijing Eye Study. Ophthalmology 2013;120:175–180.
Subfoveal Choroidal Thickness in Preeclampsia 17
! 2014 Informa Healthcare USA, Inc.
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
08/
03/1
4Fo
r pe
rson
al u
se o
nly.