Embed Size (px)
Citation preview

Subclinical thyroid disordersMario Skugor M.D. FACEAssociate Professor of MedicineCCLCM of CWRUCleveland Clinic

Definitions:
Individuals with elevation of TSH but normal thyroid hormone levels have sub-clinical hypothyroidism*.
*Some authors consider patients with high-normal TSH and abnormal response to TRH as having SCH.
Gharib H. et al. J Clin Endocrinol Metab 2005;90:581-585

Definitions:
Individuals with TSH lower than normal but with normal thyroid hormone levels have sub-clinical hyperthyroidism.
Gharib H. et al. J Clin Endocrinol Metab 2005;90:581-585

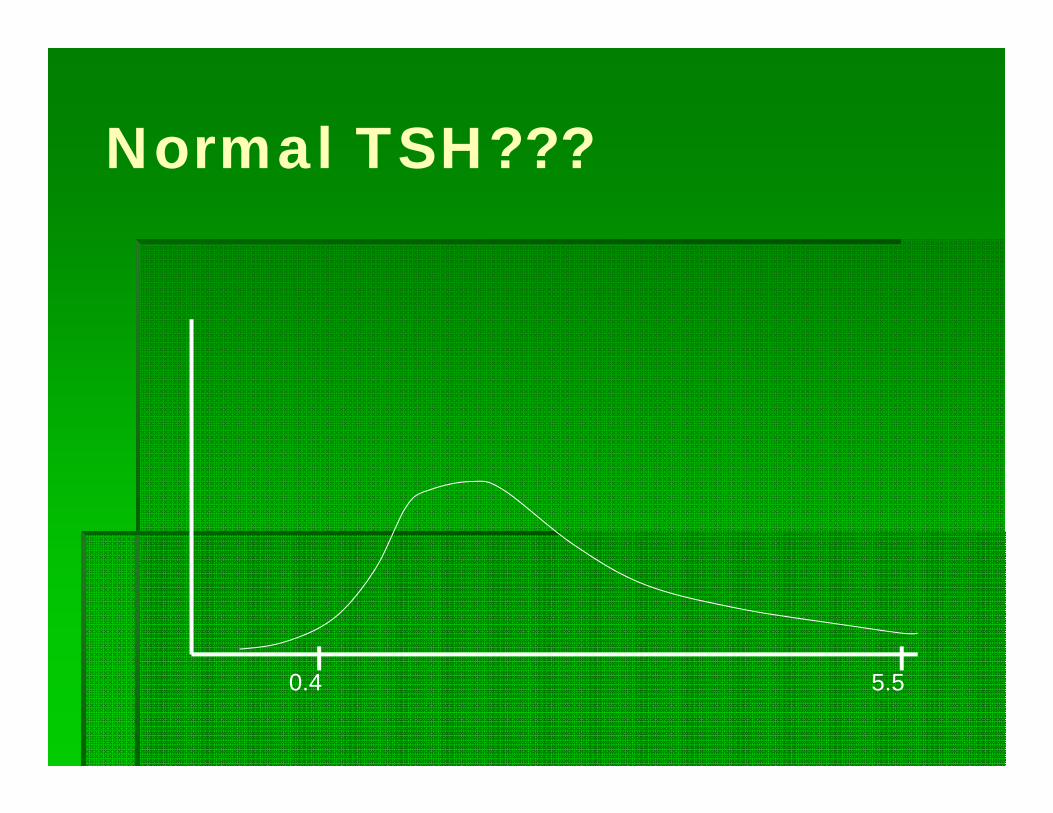
Normal TSH???
Normal TSH range Most common assays in U.S.A. 0.4-5.5 uU/mL 0.27-4.2 uU/mL

Normal TSH???
Lower limit of the normal range is somewhat variable but relatively well established.

Normal TSH???
Upper level of normal range is controversial.
Normal TSH???
0.4 5.5

NHANES III
0.45 4.121.39
median
N = 13,344Healthy, antibody negative subjects

Normal TSH???
Consensus conference (ATA, AACE, Endo Soc) accepted NHANES III derived normal range.
National Academy of Clinical Biochemistry proposed 0.4-2.5 uU/mL for normal range.
AACE proposed 0.3-3.0 uU/mL

Practical considerations
Results of lowering upper limit of normal range from 5 to 2.5 uU/mL changes prevalence of sub-clinical hypothyroidism:
4.6% to 20%
Fatourechi V. et al. JAMA 2003;290:3195-3196

Practical considerations
TSH varies with time. Mildly abnormal TSH should be rechecked in
3-4 months to confirm persistent elevation. Transient elevations are not uncommon.

Practical considerations
TSH elevations NOT associated with SC hypothyroidism: Recovery from non-thyroidal illness. Adrenal insufficiency. Treatment with metoclopramide and domperidone TSH secreting adenomas Thyroid hormone resistance Assay variability Late evening pulse in TSH secretion

Practical considerations
Decreased TSH also could be seen with conditions that are not associated with hyperthyroidism.

Practical considerations
Decreased TSH NOT associated with SC hyperthyroidism:
Central hypothyroidism Non-thyroidal Illness Glucocorticoid and dopamine use Recovery from hyperthyroidism Early pregnancy

Practical considerations
Even TSH over 20 uU/mL can be associated with normal TH levels.
Practical considerations
Attempts to identify individuals with mild thyroid disorders based on search for thyroid specific symptoms have not been successful.

Sub-clinical hypothyroidism
Should be diagnosed in patients who do NOT complain of symptoms associated with hypothyroidism.
In patients who are screened for presence of thyroid disorder because of increased risk.
Elevated TSH normal TH
If patient complains of symptoms and elevated TSH with normal TH is found, than disorder cannot be considered to be sub-clinical.

Mild hypothyroidism
In my opinion, after rechecking to confirm TSH elevation, treatment should be seriously considered in such patients. TSH should be corrected to below 2.0
uU/mL and therapeutic effects assessed after 2-3 months. If benefit is derived treatment should be
continued.

Sub-clinical hypothyroidism
Individuals with TSH from upper limit of normal to 10 uU/mL With normal TH levels With no symptoms that could be explained
by hypothyroidism
Have “Sub-clinical hypothyroidism”

Epidemiology
Whickham survey Prevalence Men 2.8% Women 7.5% Women >60 y 11.6%
Vanderpump MP. Et al. Clin endocrinol (Oxf) 1991;43:55-69

Epidemiology
NHANES III Prevalence in 16,533 individuals Patients with known thyroid disease were
excluded. SCH found in 4.3%
Hollowell JG, et al. J Clin Endocrinol Metab 2002;87:489.

Epidemiology
Colorado Thyroid Disease Prevalence Study N – 25,862 Prevalence Overall 9.5% 18-24 y 4.0% Women >74 22% Men >74 y 16%
Canaris GJ. Et al. Arch Intern Med 2000:160:526-534/

Epidemiology
Increased prevalence is reported in patients with: Diabetes mellitus type 1 (1) Schmidt’s syndrome (2) Celiac disease (3)
Due to presence of Hashimoto’s thyroiditis1. Vondra K. et al. J Endocrinol Invest 2004: 27:728-732.2. Betterie C. et al. Endocr rev 2002;23:327-364.3. Sategna-Guidetti C. et al. Am J Gastroenterol 2001:96:751-757.

Etiology–SC hypothyroidism
Common causes Iatrogenic In patients with coexisting heart disease In patients with malignant diseases In patients with poor compliance In patients taking medications inappropriately
Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Most common cause 54% of SCH patients in U.S. are abs positive (1) UK study found abs in 67% of women and 40%
of men with SCH (2)
1. Hamburger JI, et al. NEJM 1985;313:267.2. Tonbridge WM. Et al. Br Med J 1974;3:89.

Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Postpartum thyroiditis

Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Postpartum thyroiditis Medications Amiodarone Lithium Interferon Sunitinib Sorafenib

Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Postpartum thyroiditis Medications Partial thyroidectomy

Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Postpartum thyroiditis Medications Partial thyroidectomy Head and neck radiation

Etiology–SC hypothyroidism
Common causes Iatrogenic Hashimoto’s thyroiditis Postpartum thyroiditis Medications Partial thyroidectomy Head and neck radiation RAI ablation of Graves’ disease

Clinical consequences
Progression to overt hypothyroidism 2-5% yearly 10% may eventually normalize Higher initial TSH – higher the risk of
progression Positive AMA-s – higher risk of progression
Huber G. et al. J Clin Endocrinol Metab 2002;87:3221-3226.Diez JJ. et al. J Clin Endocrinol Metab 1991:72:209-213.

Clinical consequences
Development of hypothyroidism, 20 year follow up – Whickham survey 27% if abs positive 33% if TSH higher than normal 55% if TSH higher and abs positive 4% if TSH was normal and abs negative
Vanderpump MP. Et al. Clin endocrinol (Oxf) 1991;43:55-69

Clinical consequences
Vanderpump MP. Et al. Clin endocrinol (Oxf) 1991;43:55-69

Clinical consequences
Risk of CV disease Diastolic dysfunction Diastolic hypertension Increase in LDL-C Increased hsCRP Alteration in coagulation parameters Endothelial dysfunction
Alber CP. et al. Am Heart J 1964Diez JJ. et al. J Clin Endocrinol Metab 1991:72:209-213.

Clinical consequences
Risk of CV disease Whickham survey showed no association
over 20 years with: Coronary heart disease Dyslipidemia Mortality
Vanderpump MP, et al. Clin Endocrinol (Oxf) 1991:43:55-69.

Clinical consequences
Risk of CV disease Rotterdam study showed increased
prevalence of atherosclerosis (odds ratio 1.7) and MI (odds ratio 2.3) in women with SCH.
Hak AE, et al. Ann Intern Med 2000;132:270-278.

Clinical consequences
Risk of CV disease Studies show mixed results but population
studied are different and number of patients are usually small (total number of subjects is high but patients with SCH are not many).
Example – 4331 subjects but 281 with SCH (1)
Pearce EN, et al. Endo Soc, Boston MA abstract 42-1.

Controversy
McDermott MT, Ridgway EC 2001 Subclinical hypothyroidism is mild thyroid failure and should be treated. J Clin Endocrinol Metab 86:4585–4590.
Chu JW, Crapo LM 2001 The treatment of subclinical hypothyroidism is seldom necessary. J Clin Endocrinol Metab 86: 4591–4599.

Clinical Consequences
Fertility 17% of Tg and AM antibodies positive had
spontaneous miscarriage, compared to 8.4% of antibody negative women (1) 2.3% of 25,756 pregnant women had SCH,
and their risk for placental abruption and preterm delivery was 2 times normal (2)
1. Stagnaro-Green A, et al. JAMA 1990;264:1422-1425.2. Casey BM, et al.Obstet Gynecol 2005;105:239-245.

Clinical Consequences
Fertility The 16 and 11 recurrent aborters with
positive TPO-abs were treated with T4 and IV immunoglobulins respectively. T4 treated patients had 81.2% delivery rate
and IV Immunoglobulin treated 54.5%.
Vaquero E, et al. Am J Reprod Immunol 2000;43:204-208

Clinical Consequences Neuropsychiatric disorders SCH patients with depression have poorer
response to antidepressant medications (1) SCH patient have increased lifetime
prevalence of depression (2) Women with SCH and goiter have increased
rate of anxiety and depressive features (3)
1. Joffe RT, Levitt AJ. Psychoneuroendocrinology 1992;17:2152. Haggerty JJ, et al. Am J Psychiatry 1993:150:508.3. Monzani F, et al. Clin Invest 1993;71:367.

Clinical Consequences Mortality CV health study (N = 3,233) showed NO
increase (1) Meta-analysis showed increased risk in
those older than 65 (2) Several studies showed increase in CV and
all-cause mortality (3-5)1. Cappola AR, et al. JAMA 2006;295:1033.2. Razvi S, et al. J Clin Endocrinol Metab 2008;93:2998.3. Imaizumi M, at al. J Clin Endocrinol Metab 2004:89:3365.4. Iervasi G, et al. Arch Intern Med 2007;167:1526.5. Walsh JP, et al. Arch Intern Med 2005;165:2467.

Our experienceWe examined cohort of 6,408 patients at HIGH
RISK for cardiovascular disease.Patients were enrolled in cardiovascular
disease prevention program of Cleveland Clinic between January 16, 1995 and June 25, 2008.Data about patients were entered in the
Preventive Cardiology Information System (PreCIS) database.
McQuade C, et al. ATA meeting, Chicago IL, 2008 abstract 311.

MethodsPatients:Secondary prevention ~ 50%Primary prevention ~ 50% Hypercholesterolemia Strong family history of CVD
The CVD risk factors are aggressively treated.

Methods (cont)
Five TSH intervals predefined:
<0.4 µU/ml (hyperthyroid) 0.4-3.0 µU/ml (normal) 3.0-6.0 µU/ml (mild SCH) 6.0-10.0 µU/ml ( moderate SCH) >10.0 µU/ml (hypothyroid)

Methods (cont)Number of patients:
<0.4 µU/ml 168 patients0.4-3.0 µU/ml 4,755 patients3.0-6.0 µU/ml 1,214 patients6.0-10.0 µU/ml 178 patients>10.0 µU/ml 79 patientsNo TSH available 14 patients

Patients characteristics: There was no difference between groups: Framingham risk score Diabetes mellitus LDL Lp(a) Microalbuminuria Body mass index Diastolic blood pressure

Results
Adjustment was made for:AgeSexSmokingHDL LDLSystolic blood pressureDiastolic blood pressureDiabetes

Results
After adjusting for common risk factors there were no increased risk for the group of patients with TSH less than 0.4.

Source: Arial 9pt, left-aligned with slide title
All cause mortality - adjustedAll Patients
Time in Years
876543210
Cum
Sur
viva
l1.0
.9
.8
.7
.6
TSH Category
0.4-3.0
3.0-6.0
6.0-10.0
>10.0
All Patients (n = 6,394)
p<0.001P<0.001

Source: Arial 9pt, left-aligned with slide title
All cause mortality - adjustedAll Patients
Time in Years
876543210
Cum
Sur
viva
l1.0
.9
.8
.7
.6
TSH Category
0.4-3.0
3.0-6.0
6.0-10.0
>10.0
All Patients (n = 6,394)
P=0.021

Limitations Thyroid status based only on elevated TSH
values as L-T4 and T3 values are not consistently available The PreCIS database consists of exclusively
preventive cardiology patients at the Cleveland Clinic. The cohort is highly selected for patients with or at risk for CHD. Results may not be generalizable Cause of death cannot be determined from the
SS death index.

Effect of treatment
Psychometric outcomes and hypothyroid symptoms scores in double blind randomized trials: Improvement is seen consistently in those
with TSH >10 uU/mL.
Cooper DS, et al. Ann Intern Med 1984;101:18.Nystrom E, et al. Clin Endocrinol 1988;29:63.Jaeschke R, et al. J Gen Intern Med 1996;11:744.Meier C, et al. J Clin Endocrinol Metab 2001;86:4860.

Effect of treatment
Cholesterol T4 treatment decreases: Total Cholesterol in those with initial level over
240 mmol/L (meta-analysis) LDL – C Apolipoprotein B-100
Danese MD, et al. J Clin Endocrinol Metab 2000;85:2993.Mikhail GS, et al. Endocr Pract 2008;14:570.Iqbal A, et al. J Intern Med 2006;260:53.

Effect of treatment Cardiac function, blood pressure Cardiac output increases (1) Vascular resistance decreases (1) Mean arterial pressure decreases (1) Carotid intimal-media thickness decreases
(2) Diastolic and systolic function improve (3)
1. Faber J, et al. Thyroid 2002;12:319.2. Adress M, et al. Clin Endocrinol 2008.3. Turhan S, et al. J CLin Endocrinol Metab. 2006;91:3490.

Bottom line:
I treat individuals with SCH if there are associated clinical symptoms or positive thyroid autoantibodies. A 2-6 months later clinical and laboratory
response is assessed. Decision to treat or not to treat further is
made in discussion with patient.

SC hyperthyroidism
Etiology Iatrogenic 25% of patients taking T4 may have low TSH.
Some of these are intentional Thyroid carcinoma History of head and neck radiation Presence of nodules and goiters
De Whalley P. Br J Gen Pract 1995;45:93.

SC hyperthyroidism
Etiology Iatrogenic Autonomous nodules (solitary and in MNG) A 22% of patient with MNG found to have SC
hyperthyroidism (1) In hyperthyroid patients over 55 years of age with
MNG 57% were sub-clinical (2)
Diaz JJ. Gerontology 2003;49:316Rieu M, et al. Clin Endocrinol 1993;39:67

SC hyperthyroidism
Etiology Iatrogenic Autonomous nodules (solitary and in MNG) Graves’ disease About 6% of patients with Graves’ disease are
sub-clinical.
Diaz JJ. Gerontology 2003;49:316.

SC hyperthyroidism
Etiology Iatrogenic Autonomous nodules (solitary and in MNG) Graves’ disease Thyroiditis Graves’ disease in remission High hCG

SC hyperthyroidism
Epidemiology Reports vary from 0.7% to 12.4% NHANES III showed 0.7% (1)
Smokers two times higher prevalence.
Another study found 1.8% with TSH <0.1 uU/mL in U.S. (2) In England 6% had TSH <0.5 uU/mL (3)
1. Hollowell JG, et al. J Clin endocrinol Metab 2002;87:4892. Sawin CT, et al. Arch Intern Med 1991;151:165.3. Parle JV, et al. Clin Endocrinol (Oxf) 1991;34:77.

SC hyperthyroidism
Natural course 40-60% normalize (1-3) About 4% progresses to overt
hyperthyroidism (4,5)
1. Eggersten R, et al. BMJ 1988;297:15862. Parle JV, et al. Clin Endocrinol (Oxf) 1991;34:77.3. Meyerovitch J et al. Arch Intern Med 2007;167:1533.4. Sawin Ct, et al. Arch Intern Med 1991;151:1655. Sandrock D, et al. Acta endocrinol (Copenh) 1993;128:51

Clinical consequences Bone metabolism No good data on fracture rates. A meta-analysis found decreased BMD, but
only in postmenopausal women (1). In those taking T4 low BMD was found only
if dose was higher than 1.6 mcg/kg/d (2). Markers of bone turnover have been
reported to be increased (3)
Faber J, Galloe AM. Eur J Endocrinol 1994;130:350Schneider DL, et al. JAMA 1994;271:1245Loviselli A, etr al. Thyroid 1997;7:561

Clinical consequences CV effects Atrial fibrillation Prospective study- 2,000 adults over 60 followed
for 10 years TSH <0.1 uU/mL - 28% cumulative incidence TSH 0.1-0.4 uU/mL - 16% cumulative incidence TSH >0.4 uU/mL - 11% cumulative incidence
Cappola AR, et al. JAMA 2006;295:1033.

Clinical consequences CV effects Atrial fibrillation A cross-sectional study, 24,000 hospitalized
patients. 14% prevalence if overtly hyperthyroid 13% prevalence in SC hyperthyroidism 2% prevalence in euthyroid controls
Auer J, et al. Am Heart J 2001;142:838

Clinical consequences CV effects Other described effects Increased heart rate and atrial premature beats Reduced exercise tolerance Increased cardiac contractility Increase in LV mass index Lower LDL-C and total cholesterol Systolic hypertension

Clinical consequences Mortality In 3,121 cardiac patients SC
hyperthyroidism was associated with 2.32 increased risk for cardiac death (1) Meta-analysis of 290 subjects over 60 found
41% increase in all cause mortality (2) Cardiovascular Health Study (3,233 subjects
over 65 y) found no increase in mortality (3)
1. Iervasi G, et al. Arch Intern Med 2007;167:15262. Haentjens P, et al. Eur J Endocrinol 2008;159:329.3. Cappola AR, et al. JAMA2006;295:1033

SC Hyperthyroidism
Most individuals with TSH of 0.1 um/mL or higher do not experience any symptoms.

Management High risk patients TSH <0.1 uU/mL evaluate and treat. TSH 0.1-0.4 uU/mL evaluate and treat if
BMD low, a-fibb or symptoms of hyperthyroidism are present.
Low risk patients TSH <0.1 uU/mL evaluate and treat if BMD
low or symptoms present. TSH 0.1-0.4 uU/mL observe.

Questions
What is the appropriate normal range for TSH? Answer will require more studies that will
need to include antibody determination and more than one determination of TSH over period of time to avoid transient elevations to creep into the normal ranges.

Questions Should we screen for SC thyroid
dysfunction? Population screening is probably not cost
effective. Testing patients with mild symptoms
suggestive of hypothyroidism is NOT screening.

Questions Who should we screen for SC thyroid
dysfunction? High risk groups should be screened. History of neck irradiation Pituitary surgery or irradiation Use of medications known to affect thyroid Presence of thyroid nodule or MNG

Questions Should we screen for SC thyroid
dysfunction? Studies needed about Patients with autoimmune disorders Unexplained infertility Previous postpartum thyroiditis Refractory depression Turner’s and Down’s syndrome Obesity

Questions
Is there a treatment benefit? Studies are inconclusive. Patients with mild laboratory abnormalities
should not be treated automatically. These should be followed in 3-6 months and
reassessed. If even mild symptoms are present treatment
should be offered. Long term outcomes need studies





























