Embed Size (px)
Citation preview
Click to edit Master title style
Subarachnoid Hemorrhage (SAH)
William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program
Click to edit Master title style
Disclosures/Relationships
No conflicts of interest
SAH Objectives
• Recognize and appropriately evaluate suspected SAH
• Apply appropriate strategies to prevent re-bleeding
• Apply appropriate strategies to reduce intracranial pressure
• Use appropriate treatment for seizures or to prevent seizures
SS1280 Case 1
• 28 year old woman, presented to an outside ED • Sudden HA while doing kettlebell exercises
– Sharp right parietal pain, radiating down neck, with limited movement of head and neck due to pain
– Associated photophobia • Described as the worst headache of her life • PMH: Migraine
Questions
What evaluation should she have? Other than the history of migraine –
she had no significant PMH Neurological examination was
reportedly normal Non-contrast head CT was reportedly
normal A Spinal tap was not done
SS1280 Case 1
• Four days later she returned to the kettlebell class and again had sudden similar headache but even worse
• She returned to the ED with headache, lightheadedness, numbness and tingling, and nausea and vomiting
• She was treated with IV fluids and anti-emetics in the ED and discharged with a prescription for oxycodone
SS1280 Case 1
• Since then she continued to have severe headache, worse with valsalva (sneezing, coughing, etc.) and associated with – Nausea and vomiting – Severe lower back pain – Difficulty walking
• Twelve days after the initial headache she drove from New Mexico to her parents home in Aurora and was seen in the Neurology Outpatient clinic
SS1280 Case 1
• She reports a severe headache which is much different than she has ever experienced with migraine
• Examination: – Pain with eye movement and transient bilateral
horizontal nystagmus with lateral gaze – Intense pain with neck flexion – Normal sensory examination
SS1280
SS1280 Case 1
• Spinal tap – Non-traumatic – Cloudy, light pink fluid – Tube #1:
• Bloody, slight xanthochromia • 16 WBCs • 5184 RBCs
– Tube #4: • Bloody, slight xanthochromia • 26 WBCs • 3610 RBCs
SS1280
Symptoms suspicious for acute SAH
• “The worst headache of my life” is described by ~80% of patients who can give a history – A warning or sentinel headache is also described by 20% – Most intracranial aneurysms remain asymptomatic until they rupture
• Aneurismal SAH occurs frequently during physical exertion or stress but can occur at any time
• Other signs and symptoms are often associated with headache: – Nausea and/or vomiting (~77%) – Stiff neck (~35%) – Brief loss of consciousness (~53%) – Focal neurological deficits (including cranial nerve palsies)
• Up to 12% die before receiving medical attention
Risk Factors for SAH
• Hypertension • Smoking • Heavy alcohol use • Sympathomimetic drugs (especially in younger
patients) – Cocaine – Methylphenidate
• Diabetes does not appear to be a risk factor for SAH
Evaluation of suspected acute SAH
• SAH is a medical emergency and is frequently misdiagnosed
• A high level of suspicion for SAH should exist in patients with acute onset of severe headache
• CT scanning for suspected SAH should be performed – If the CT is negative lumbar puncture is strongly
recommended • Selective cerebral angiography should be performed in
patients with SAH to document the presence and anatomic features of aneurysms – MRA and/or CTA may be considered when conventional
angiography cannot be performed in a timely fashion
PZ1131 Case 2
• 78 year old woman presented to outside ED • Awoke with 10/10 bitemporal headache,
nausea, and vomiting • BP 156/79 (123-171/59-87), HR 122 (73-122) • Regular, unlabored, and protecting airway • Lethargic but follows directions, pupils
“pinpoint,” grip is weak on the right
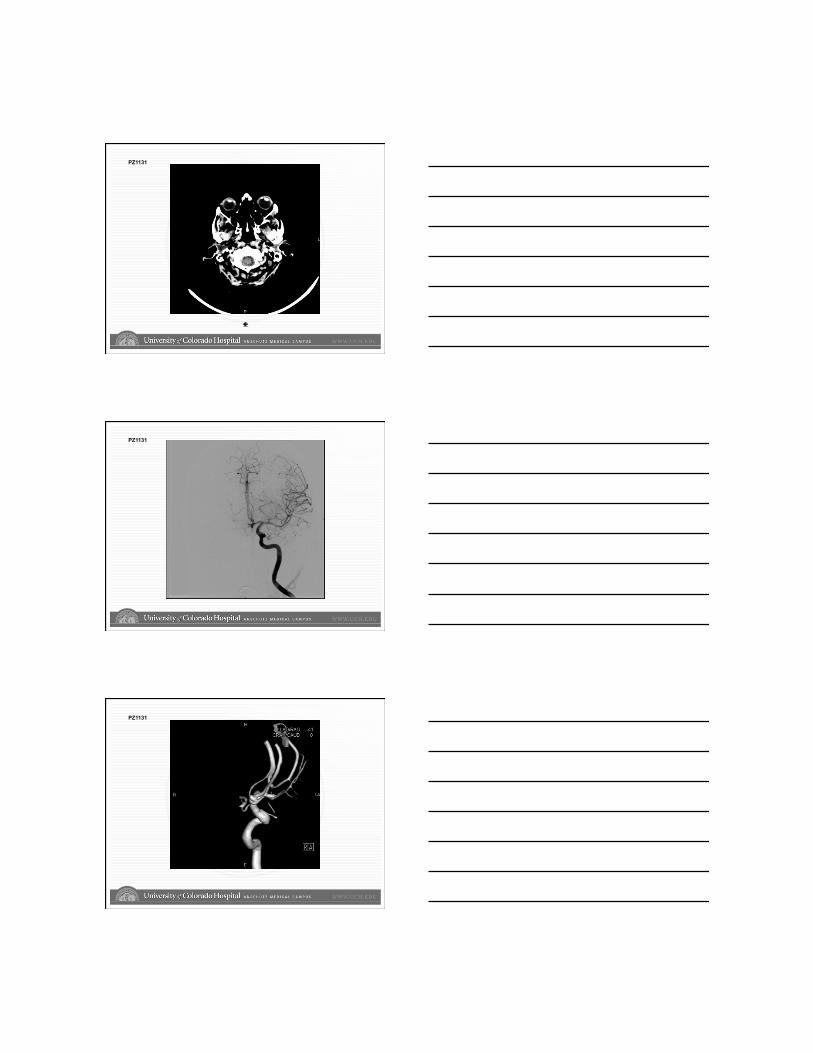
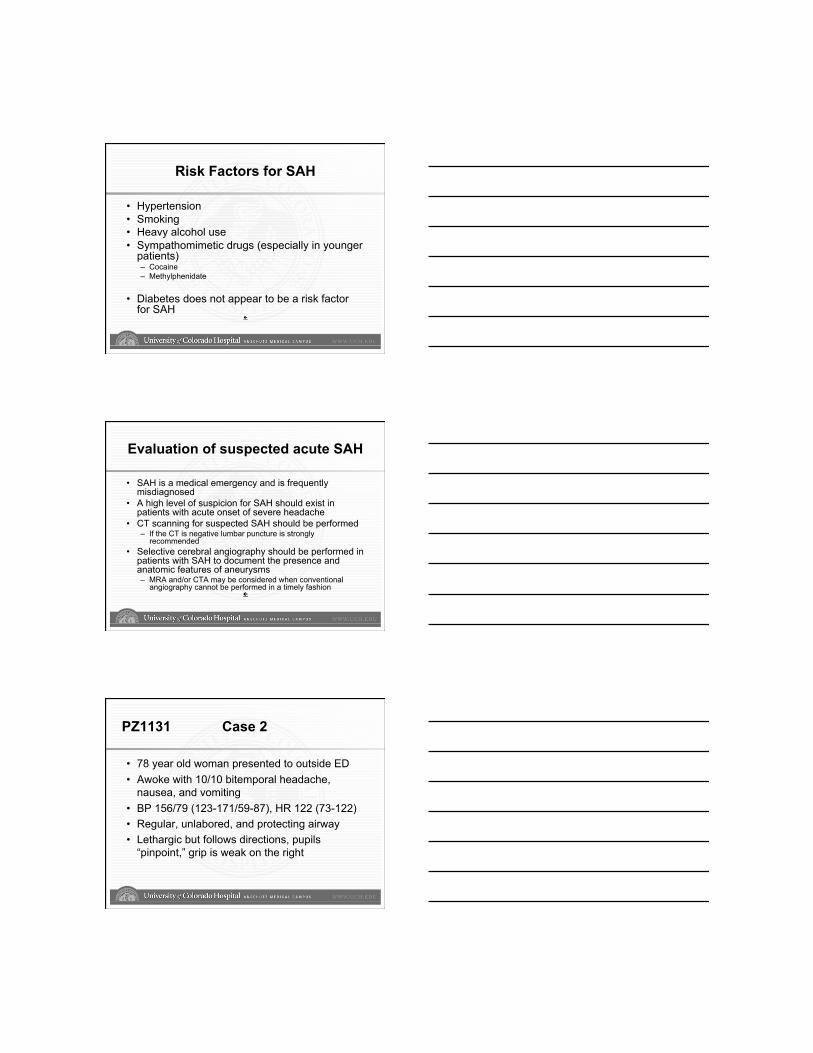
PZ1131
PZ1131
PZ1131
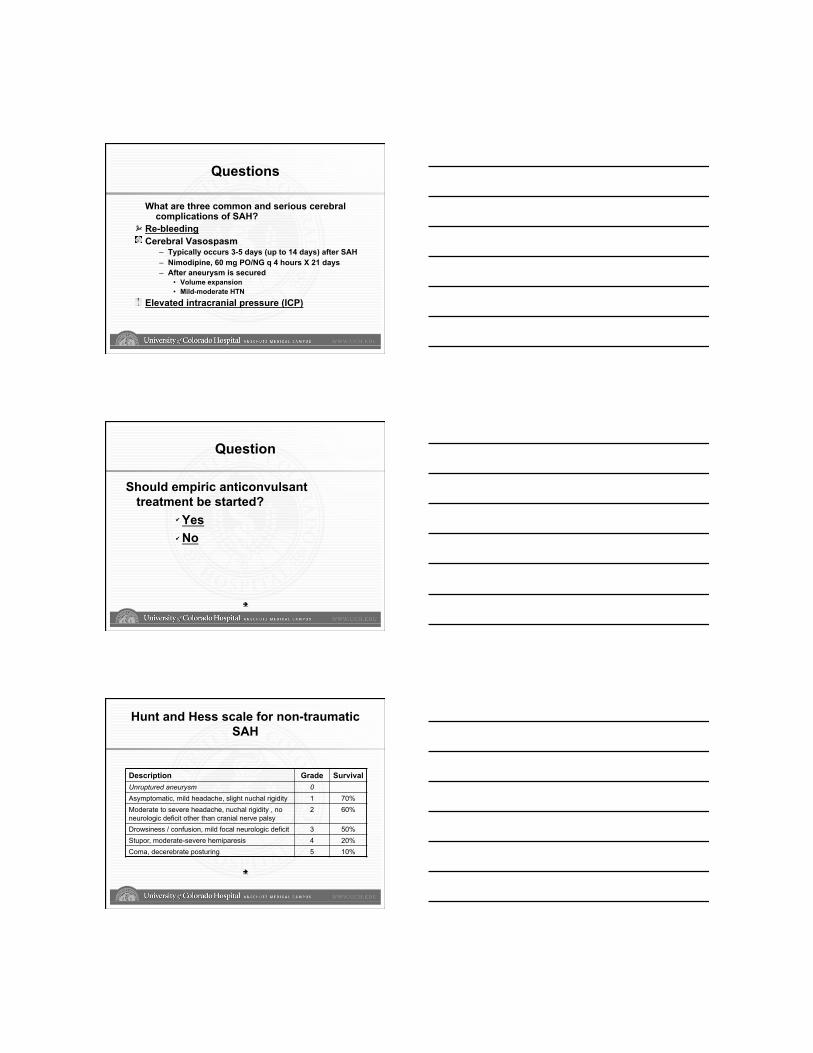
Questions
What are three common and serious cerebral complications of SAH?
Re-bleeding Cerebral Vasospasm
– Typically occurs 3-5 days (up to 14 days) after SAH – Nimodipine, 60 mg PO/NG q 4 hours X 21 days – After aneurysm is secured
• Volume expansion • Mild-moderate HTN
Elevated intracranial pressure (ICP)
Question
Should empiric anticonvulsant treatment be started? Yes No
Hunt and Hess scale for non-traumatic SAH
Description Grade Survival Unruptured aneurysm 0 Asymptomatic, mild headache, slight nuchal rigidity 1 70% Moderate to severe headache, nuchal rigidity , no neurologic deficit other than cranial nerve palsy
2 60%
Drowsiness / confusion, mild focal neurologic deficit 3 50% Stupor, moderate-severe hemiparesis 4 20% Coma, decerebrate posturing 5 10%
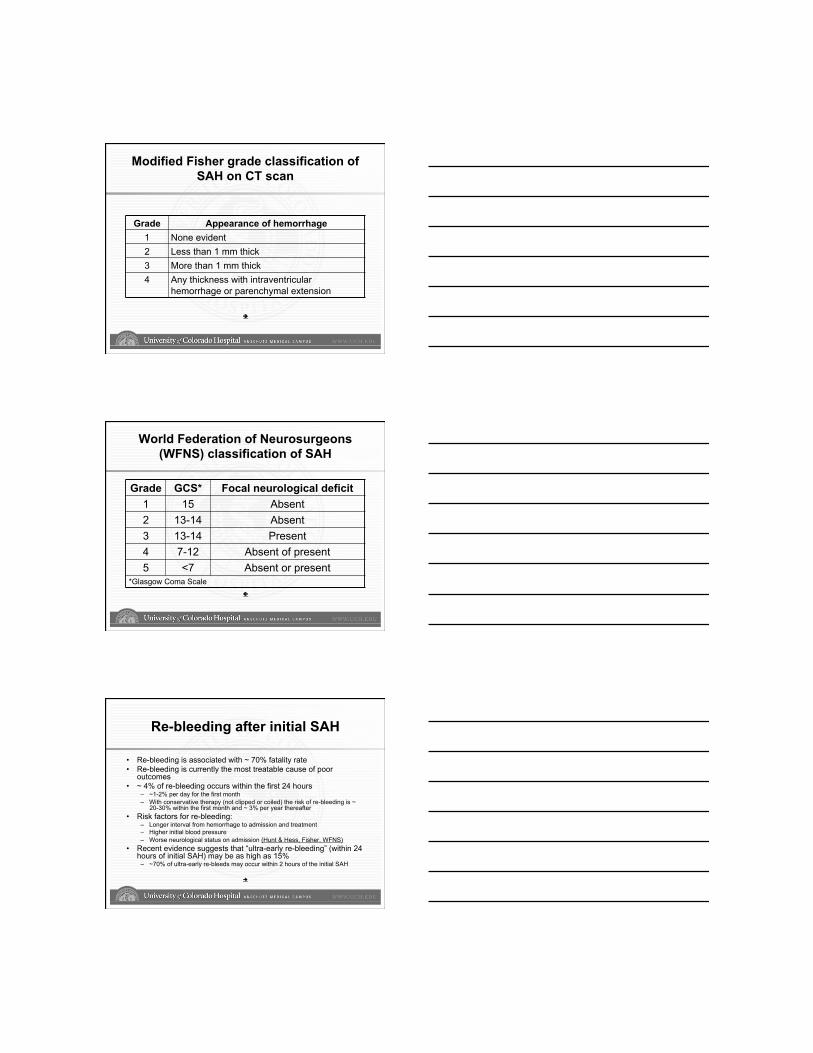
Modified Fisher grade classification of SAH on CT scan
Grade Appearance of hemorrhage 1 None evident 2 Less than 1 mm thick 3 More than 1 mm thick 4 Any thickness with intraventricular
hemorrhage or parenchymal extension
World Federation of Neurosurgeons (WFNS) classification of SAH
Grade GCS* Focal neurological deficit 1 15 Absent 2 13-14 Absent 3 13-14 Present 4 7-12 Absent of present 5 <7 Absent or present
*Glasgow Coma Scale
Re-bleeding after initial SAH
• Re-bleeding is associated with ~ 70% fatality rate • Re-bleeding is currently the most treatable cause of poor
outcomes • ~ 4% of re-bleeding occurs within the first 24 hours
– ~1-2% per day for the first month – With conservative therapy (not clipped or coiled) the risk of re-bleeding is ~
20-30% within the first month and ~ 3% per year thereafter • Risk factors for re-bleeding:
– Longer interval from hemorrhage to admission and treatment – Higher initial blood pressure – Worse neurological status on admission (Hunt & Hess, Fisher, WFNS)
• Recent evidence suggests that “ultra-early re-bleeding” (within 24 hours of initial SAH) may be as high as 15%
– ~70% of ultra-early re-bleeds may occur within 2 hours of the initial SAH
Prevention of re-bleeding
• Surgical clipping or endovascular coiling should be performed to reduce the rate of re-bleeding after aneurismal SAH – Early referral to high-volume centers that have both
experienced cerebrovascular surgeons and endovascular specialists is recommended
• Treat hypertension • Antithrombolytics (±)
Prevention of re-bleeding (elevated blood pressure)
• No well-controlled studies of blood pressure control on the rate of re-bleeding • Retrospective studies have shown:
– Re-bleeding is less frequent in patients treated with antihypertensive medication • Even though blood pressures were still higher in the treated than non-treated
patients – An increase in blood pressure immediately before re-bleeding – Re-bleeding associated with systolic blood pressure > 150 mm Hg – Re-bleeding associated with systolic blood pressure > 160 mm Hg – ~ 13.6% of re-bleeds in the ambulance or while still at the referring hospital with a peak
incidence within 2 hours of the initial hemorrhage
– Re-bleeding rate of only 6.9% with no relationship to blood pressure • When blood pressure is elevated, short-acting continuous-infusion
intravenous agents with a reliable dose-response relationship and favorable safety profile are desirable to reduce SBP <150 mm Hg:
– Nicardipine, labetalol, and esmolol reportedly best meet these criteria – However, sodium nitroprusside is more reliable at quickly and effectively lowering blood
pressure but may raise intracranial pressure and causes toxicity with prolonged infusion
Prevention of re-bleeding (antifibrinolytics)
• Antifibrinolytic agents (epsilon-aminocaproic acid, 36 gm/day; or tranexamic acid, 6 to 12 gm/day):
– 40-60% reduction in re-bleeding in treated versus control subjects • Nearly one third of treated patients in these trials were clinically worse at 14
days • Up to 43% increase in the rate of cerebral infarction
– No difference in re-bleeding between subjects receiving tranexamic acid versus control subjects
– Similar results have been found with either epsilon-aminocaproic acid (36 gm/d) or tranexamic acid (6 to 12 gm/d)
• More recently, a prospective, randomized trial of tranexamic acid administered immediately after the diagnosis of SAH followed by early clipping or coiling demonstrated reduced re-bleeding rates and adverse outcomes
Prevention of re-bleeding
• Quiet bed-rest may be helpful but is not sufficient to prevent re-bleeding without being combined with broader treatment strategies
• Blood pressure should be monitored and controlled to balance the risk of stroke, hypertension-related re-bleeding, and maintenance of cerebral perfusion pressure
– Within the first 24 hours when risk of vasospasm is low (typically occurs between 3-14 days) and the risk of re-bleeding is highest, SBP should be maintained < 150 mm Hg
• Recent evidence suggests that early treatment with a short course of antifibrinolytic agents combined with early aneurysm treatment followed by discontinuation of the antifibrinolytic may be reasonable
– avoid hypovolemia and vasospasm – (±) Aminocaproic acid 4-5 gm IV over one hour, then 1 gm IV per hour for 24
hours or until clipped or coiled
Increased intracranial pressure
• Increased ICP is common following SAH may be caused by one or more of: – Hydrocephalus
• May occur with or without intra-ventricular blood • Is associated with the amount of cisternal blood
when intra-ventricular blood is absent – Intra-parenchymal hemorrhage – Cerebral edema
Increased intracranial pressure
• Most patient require ICP monitoring – Intracranial pressure monitor (bolt) – Intra-ventricular drain (s) – can also be used
to treat hydrocephalus and elevated ICP • Mannitol 0.8-0.9 gm/kg will reduce ICP
– May cause hyponatremia – May cause volume depletion and thus
decreased cerebral perfusion • Hyperventilation temporarily reduces ICP
Anticonvulsant treatment
• The risk and implications of seizures associated with SAH are not well defined, and the need for and efficacy of routinely administered anticonvulsants after SAH are not well established
– “Seizure-like” episodes have been associated with aneurismal rupture – In retrospective reviews seizures frequency ranges from 6% to 18% – Most seizures occurred before medical presentation and in-hospital seizures
are rare in patients given prophylactic anticonvulsants – The relationship between seizures and outcome is not clear – In one series of patients who underwent continuous EEG monitoring found
19% of stuporous or comatose patients had non-convulsive seizures • All were receiving prophylactic anticonvulsants, and all died
– Risk factors for seizures after SAH include: • middle cerebral artery aneurysms • intraparenchymal hematoma • cerebral infarctions • history of hypertension
Anticonvulsant treatment
• Anticonvulsants should be administered in patients with seizures
• Prophylactic anticonvulsants may be considered in the immediate post-hemorrhagic period – Dilantin (phenytoin)
• Typically avoid phenytoin because cardiac rhythm disturbances are common with SAH and phenytoin may also cause arrhythmias
– Keppra (levetiracetam) – 500-1000 mg IV BID – Valproic acid – 10-15 mg/kg per day divided TID,
may increase up to 30-60 mg/kg per day
SAH recommendations
• Prevention of re-bleeding – Secure aneurysm ASAP – Maintain SBP < 150 mm Hg until aneurysm is secured
• Nicardipine, 3-15 mg per hour IV drip • Nipride (nitroprusside), 3-10 mcg/kg per minute IV drip
– ±Amicar (aminocaproic acid) immediately and for 24 hours or until aneurysm is secured
• Treatment of ICP – ICP monitor or intra-ventricular drain (s) – Mannitol 0.8-0.9 gm/kg
• Anticonvulsants – Keppra (levetiracetam), 500-1000 mg BID – Depacon (valproate), 10-60 mg/kg per day, divided TIA
Questions







![Inflammation in human cerebral aneurysms: pathogenesis ... · aneurysmal subarachnoid hemorrhage (SAH) is higher in hypertensive patients, smokers, heavy drinkers, and females. [2,4]](https://img.pdfslide.us/doc/110x75/5ed55ef36933f508e973f11f/inflammation-in-human-cerebral-aneurysms-pathogenesis-aneurysmal-subarachnoid.jpg)