Embed Size (px)
Citation preview

Original Research
Study of Focused Ultrasound Tissue Damage UsingMRI and Histology
Lili Chen, PhD,1* Donna Bouley, PhD,2 Esther Yuh, PhD,1 Helen D’Arceuil, PhD,1
and Kim Butts, PhD1
This paper reports on an experimental study of in vivotissue damage in the rabbit brain with focused ultrasound(FUS) using magnetic resonance imaging (MRI) and histo-pathological analysis. Ten ultrasonic lesions (tissue dam-age) were created in five rabbits using a focused ultrasoundbeam of 1.5 MHz, electrical power input to the transducerof 70–85 W, and an exposure duration of 15–20 seconds. T1-and T2-weighted fast spin-echo (FSE) and Fluid attenuatedinversion recovery (FLAIR) sequences were used to detectthe ultrasonic lesions after treatment. Imaging was per-formed for 4–8 hours after treatment, after which theanimals were immediately sacrificed. Ultrasonic lesiondiameter was measured on MRI and histological sectionsafter correction for tissue shrinkage during the histologi-cal processing. The T1-weighted images showed lesionspoorly, whereas both T2-weighted and FLAIR images showedlesions clearly. The lesion diameters on both T2 and FLAIRimaging correlated well with measurements from histol-ogy. The time delay before lesions appeared on T2-weighted imaging was 15 minutes to 1 hour, depending onthe exposure location in the brain. J. Magn. Reson. Imag-ing 1999;10:146–153. r 1999 Wiley-Liss, Inc.
Index terms: focused ultrasound surgery; tissue ablation;histopathology; MRI; rabbit brain; in vivo
FOCUSED ultrasound (FUS) has the potential to treatcancer noninvasively by selectively producing damagewithin a focal volume, with no known harm to overlyingor surrounding tissue. FUS has been investigated fornoninvasive treatment of hepatic metastasis (1–5), breastfibroadenoma (6), benign prostatic hyperplasia (7,8),prostatic carcinoma (9), bladder carcinoma (10), andrenal carcinoma (11,12). It has been demonstrated thatwith careful treatment planning, it is possible to dam-age all the tumor cells within the treatment volume inexteriorized rat liver with FUS (13).
An important factor contributing to the clinical appli-cation of noninvasive surgery is the use of high-qualitymethods of medical imaging to guide and monitor the
tissue damage. Theoretical and experimental evidenceindicated that the primary mechanism of ultrasoundtissue damage is thermal. Multiple MR parameters aresensitive to changes in temperature and in tissue micro-structure that occur with thermal coagulation fromheating (6,14–18). The feasibility of using MRI for guid-ing and monitoring thermal damage in tissue has beeninvestigated for ablation with FUS (6,14–17,19), radio-frequency (RF) (20), and laser interstitial probe (21,22).T2-weighted MRI appears to be especially promising forthe evaluation of thermal lesions. The purpose of thisstudy was to investigate the behavior of FUS lesionswith T2-weighted MRI and to compare lesion size mea-sured on MRI with the actual tissue damage zonemeasured on histological sections.
MATERIALS AND METHODS
Heating Apparatus and MR Scanner
A 1.5 MHz FUS field was generated by a bowl-shaped,10 cm diameter piezoelectric ceramic transducer (PZT4)with a focal length of 8 cm (GE Corporate Research andDevelopment). The transducer was electrically matched.An experiment on calibration of the transducer wascarried out on ex vivo bovine liver tissue. It providedvarying lesion sizes as a function of electrical inputvoltage to the transducer with given exposure duration.The transducer was mounted vertically in a plexiglaswater tank (83 3 14 3 13 cm) filled with degassed wa-ter at room temperature (25°C). The water tank wascovered with a plexiglas board (2.5 cm thick) with anacoustic window of 5 cm diameter. Electrical inputvalues to the transducer from 70 to 85 W and 15–20seconds of exposure duration were used. A three-dimensional coordinate system (GE Corporate Researchand Development) was used to move the transduceralong the beam axis and in both orthogonal directions(Fig. 1). The water tank was mounted on a standard MRimaging table of a 1.5 T MR scanner (GE MedicalSystems, Milwaukee, WI). The focal spot was observedby producing a water jet at the surface of the water bathwith low FUS intensity and registering it with the MRIplane.
1Department of Radiology, Stanford University, Stanford, California94305.2Department of Comparative Medicine, Stanford University, Stanford,California 94305.*Address reprint requests to: L.C., Radiological Sciences Laboratory,Department of Radiology, Stanford University, 1201 Welch Rd., Stan-ford, CA 94305-5488. E-mail: [email protected] January 15, 1999; Accepted May 14, 1999.
JOURNAL OF MAGNETIC RESONANCE IMAGING 10:146–153 (1999)
r 1999 Wiley-Liss, Inc. 146

Experimental Procedures
FUS Exposure on Rabbit Brains
Five New Zealand white rabbits (weight 3–4 kg) wereused for this study. The animal experiments were ap-proved by the Administrative Panel on Laboratory Ani-mal Care (APLAC) at Stanford University. Each rabbitwas anaesthetized using ketamine (35 mg/kg) andxylazine (5 mg/kg) subcutaneously. After induction, therabbit was intubated and anesthesia was maintainedwith isoflurane (2–3%) and oxygen (1%). An acousticwindow approximately 25 3 20 mm was created bysurgically removing a piece of skull, leaving the duramater intact. The rabbit was mounted on top of thewater tank in the supine position. A plastic blanket wasplaced between the rabbit and the water tank to aid inthermoregulation. The brain was set on the acousticwindow of the cover board and placed in contact withdegassed water. Care was taken to prevent the introduc-tion of air bubbles between the water and the brain. A5-inch surface coil was placed above the rabbit. Prior totreatment, a T1- or T2-weighted fast spin-echo (FSE)sequence was performed to visualize both the trans-ducer and the rabbit brain. A field of view (FOV) of 16 cmwas used to image both the transducer and the brainwithout phase wrap. The transducer was adjusted sothat its focal peak was set to the desired location,approximately 9 6 1 mm into the brain for the 10lesions. Care was taken to ensure that the skull boneedge did not block the focal beam. Two separatedultrasonic lesions were created on the same imagingplane (sagittal) in the brain. The separations betweenthe two individual lesions were from 6 to 12 mm. Thefirst FUS exposure was placed rostrally (close to theolfactory lobes) or caudally (close to the cerebellum) inrandom order. In two rabbits, the first FUS exposure
was placed rostrally whereas in three rabbits, the firstFUS exposure was placed caudally. The lesions werecreated in either the left or right cerebral hemisphere,approximately 3 mm lateral to the longitudinal fissure.
MR Imaging Parameters

were routinely processed and embedded in paraffin,and 10 µm thick sections, 150 µm apart, were mountedon glass slides, stained with hematoxylin and eosin(H&E), and coverslipped.
Data Analysis
To eliminate any possible bias in the lesion measure-ment, the MR measurements were performed by amedical physicist, and the histological measurementswere performed by a boarded Veterinary Pathologist,without the knowledge of each other’s measurementresults.
Defining Lesion Boundary and LesionMeasurement on MRI
The boundary between the bright ring and normal brainwas clearly distinguished on MR imaging. In this study,the exterior margin of the bright ring on T2-weightedMRI was defined as the FUS lesion boundary. Before thelesion measurement, the image was magnified 4 times(1024 3 1024 pixels) using a bilinear interpolation inorder to count accurately the number of pixels acrosseach of the thermal lesions. During the lesion measure-ment, the lesion boundary was manually traced on theMR image. The location of the maximum lesion diameterwas visually determined, and the diameter was mea-sured. The measurement was performed 3 times oneach lesion, and the lesion diameter was calculated asthe average value over the three measured values. Thestandard deviation of the three measurements per le-sion was calculated. The measurement was performedon images acquired just before the rabbit was sacrificed.
Determination of Maximum Lesion Diameter in MRI
The MR imaging plane was aligned with the focal peakas previously mentioned. In order to ensure further thatthe focal spot (corresponding to the maximum lesiondiameter) was registered accurately with the MR plane,additional MR images at 61 mm of the focal spot wereacquired at each time point.
Measurement of Lesion Diameter From Histology
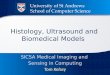
Using a Zeiss microscope attached to a video imagingsystem, the perimeter of each FUS-induced lesion wastraced using the Neuroleucida Imaging System andassociated software, creating closed contours. The le-sion boundary was identified by an outer rim of mildvacuolation of neuropil with decreased staining inten-sity, as indicated by the arrow in Fig. 2a. The closedcontour dimensions (including maximum lesion diam-eter) and distance between the centers of the twocontours (two lesions) were obtained and comparedwith MRI measurements. The maximum lesion diam-eter from each animal was determined from a series ofsections taken at 150 µm intervals.
To correct for the degree of shrinkage due to routineprocessing of brain tissue, the distance between the twolesion centers was measured from both MR and histol-ogy. The actual value of the lesion diameter correspond-ing to the FUS-induced histopathology was calculated
by the following formula,
D 5 DH · CF, (1)
where D is the lesion diameter after tissue shrinkagecorrection, DH is the lesion diameter measured onhistological section, and CF is the shrinkage correctionfactor, defined as
CF 5 SMR/SH, (2)
where SMR is the lesion separation distance measuredfrom center to center of the two lesions on MR, and SH isthe lesion separation distance measured from center tocenter of two lesions on histological section. This correc-tion assumes uniform shrinkage of the processed braintissue; thus the relationship between the lesion separa-tion (lesion center to lesion center distance) and thelesion diameter remains unchanged before and after thefixation process.
RESULTS
Observation of Ultrasonic Lesions on Histology byLight Microscopy
The FUS lesion was distinguished from untreated brainby light microscopy in all animals in this study. Thetypical lesion exhibits differential staining intensities,with two distinct zones: a central zone of the lesion ischaracterized by an overall increase in staining inten-sity with eosin, due to increased density of the neuropil.Within this central zone (labeled ‘‘C’’ in Fig. 2a), neuronshave uniformly dark-staining, smudged nuclear chro-matin, while the neuronal soma is faded and pale pink(Fig. 2b). This zone corresponds to the hypointense coreon T2-weighted and FLAIR imaging and is thought torepresent generalized coagulation due to high tempera-ture. The outer zone (labeled ‘‘I’’ in Fig. 2a) is character-ized by extensive vacuolation (spongiosis) of the neuro-pil. Within this zone, neurons have peripherally clumpedNissl substance, and there are increased, small, moredarkly staining cells, interpreted as glia, and also paren-chymal edema. We called this the intermediate zone.These cells within the intermediate zone are clearlydamaged, although it is unclear from this study which ifany these cells will ultimately die. This region corre-sponds to the hyperintense ring in T2-weighted andFLAIR images. In addition, a third zone measuringapproximately 0.3–0.8 mm wide immediately sur-rounds the intermediate zone, and histologically ismildly hypercellular with minimal spongiosis, but other-wise unaffected. We call this the transition zone. Thecells within this zone appear intact with H&E and areconsidered viable at the time. Since the cells in this zoneappear more normal than in the intermediate zone anddo not stain differently from normal tissue, the transi-tion zones have not been included in tissue damagezones for this study. Figure 2c shows untreated normalbrain.
148 Chen et al.

Observation of Ultrasonic Lesion on MRI WithDifferent MR Sequences
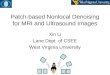
It was found that the ultrasonic lesion showed as aslightly hypointense region on T1-weighted MR, but thelesion boundary could not be clearly distinguished (Fig.3a). The lesion could be seen clearly on T2-weighted MRimaging as a slightly hypointense (dark) area in thecenter, surrounded by a hyperintense (bright) ring.These results are similar to those reported by otherinvestigators (eg, refs. 17 and 23–25). There were nosignificant differences in lesion contrast between T2-weighted and FLAIR imaging, as seen in Fig. 3b,c). Thelesion diameter measured by T2-weighted MRI andFLAIR were identical, as seen in Fig. 4.
Correlation of Lesion Diameter by T2-Weighted FSEMRI and Histology
Paired lesions created in five rabbits, which were appro-priate for histopathological analysis, were evaluated.
The values of lesion diameter, measured by histologyversus those measured on T2-weighted FSE MRI, aregiven in Table 1 and illustrated in Fig. 5. The tissueshrinkage correction factor was found to be between0.97 and 1.17 in this study. It is apparent that the lesionsize measured from MR correlated well with that fromhistology after tissue shrinkage correction. The correla-tion coefficient between lesion diameters measured onMR images and histological sections is 0.895. Thedifference of the magnitude between lesion diametermeasurement from MRI and histology is in the range of0.1–0.7 mm, which is approximately one MRI pixelvalue (0.625 mm).
Time Delay for FUS Lesion to Appear on MRImaging and Location Dependence
In some lesions, the lesion core appeared hypointenseon T2-weighted and FLAIR imaging before the brightring formation. However, the hypointensity was not
Figure 2. Histological sections a: The lesion boundary be-tween treated and untreated rabbit brain, (arrow 310). C,central zone of the lesion; I, intermediate zone. b: Coagulationnecrosis of neurons in the central zone (350) and c: Untreatednormal brain (350). The rabbit was sacrificed 4 hours afterFUS exposure and stained with H&E.
Study of FUS Tissue Damage by MRI and Histology 149

always appreciable immediately after FUS exposure.The time delay for the bright ring formation on T2-weighted imaging varied significantly. After FUS expo-sure, the shortest time for the bright ring to appear onT2-weighted (or FLAIR) imaging was 15 minutes. Thelongest delay for the appearance of the bright ring wasapproximately 1 hour.
It was observed that for all rabbits we used in thisstudy, the time delay for lesions to appear on MRimaging correlated with the exposure location. In allrabbits treated in two locations with the same FUSexposure parameters, the rostral-most lesions consis-tently took a longer time to appear. Figure 6 shows thetime delay for lesions to appear on T2-weighted imagingas a function of the distance from the olfactory lobe. Thebars represent the known time range for the first appear-ance of the lesion on T2-weighted MRI from each FUSexposure. The left ends of the bars represent the timepoint at which the lesion had not yet appeared when the
T2-weighted image was taken, and the right ends of thebars represent the first time point at which the lesiondid appear on a subsequent image. In addition, Fig. 6demonstrates that, in general, the lesion located furtheraway from the olfactory lobe (or close to the cerebellum)appeared earlier on T2-weighted MRI.
Figure 7 shows an example of the time delay for thebright ring to appear on T2-weighted images in oneanimal. The time after FUS exposure for the lesion isindicated, and the lesion is indicated by an arrow. It canbe seen that the lesion appears between 26 and 35minutes after FUS treatment.
Brain Edema After FUS Treatment
Brain edema after FUS treatment was observed in ourstudy. In three rabbits sacrificed immediately afterimaging 5, 6, and 8 hours post-treatment, the lesionsize on MR had increased significantly, and also thedistance between the two lesion centers had increased
Figure 3. a: A T1-weighted image. b: A T2-weighted image. c: A FLAIR image of the same plane. The focused lesion was poorlyseen on the T1-weighted imaging; it is well seen on the T2-weighted and FLAIR imaging. The images were taken approximately 2hours after FUS treatment.
Figure 4. Measurement of lesion diameters by T2-weightedand FLAIR imaging. The line of identity line is shown. Thelesion diameter measured by T2-weighted MRI and FLAIR wasidentical.
Table 1Measurement of Lesion Diameter by T2-Weighted MRI andHistology Using Light Microscopy
Rabbitno.
Lesionno.
CFa
SMR/SH
on
Before CFhistology
(mm)
After CFon histology
(mm)
T2-weightedMRI (mm)b
1 1 1.06 4.0 4.3 4.7 6 0.121 2 1.06 4.3 4.6 5.1 6 0.032 3 1.17 3.9 4.5 4.7 6 0.092 4 1.17 3.5 4.0 3.6 6 0.053 5 1.06 6.0 6.3 6.2 6 0.093 6 1.06 4.7 5.0 5.6 6 0.094 7 1.12 5.6 6.3 6.0 6 0.094 8 1.12 5.9 6.6 6.4 6 0.095 9 0.97 5.6 5.5 6.2 6 0.105 10 0.97 4.5 4.4 5.1 6 0.09
aCF 5 correction factor.bThese values represent the standard deviation of the three MRImeasurements per lesion.
150 Chen et al.

by 9 6 0.12% compared with the initial value. However,the brain edema has been taken into account with thecorrection factor, as described previously.
Lesion Growth With Time on MRI
Lesion growth with time after FUS was observed. Figure8 shows that lesion diameters increased approximately1 mm over the first 2 hours and continued growing byapproximately 1 mm after the 3 hour imaging interval.
DISCUSSION
Relationship Between the FUS Lesions on MRI andHistology
The results of this study demonstrated that T1-weightedimages showed FUS lesions in rabbit brain poorly, while
both T2-weighted and FLAIR images showed the lesionsclearly. On T2-weighted and FLAIR imaging, the lesionshowed as a slightly hypointense core surrounded by ahyperintense ring. This is consistent with the reports byother groups (17,23–25).
In our study, the appearance of the FUS lesions inbrain showing on histological sections is similar to theearly observations of Lele (26) and Vykhodtseva et al(27). There are reports on the correlation of lesion sizebetween MR images and necropsy. Hynynen et al (28,29)reported that FUS lesions were produced in dog andrabbit thigh muscle in vivo; the lesion sizes measuredfrom T2-weighted MR images and contrast-enhancedimages (proton density, T2-weighted, and GRASS) corre-lated well with those measured post mortem. However,they noted that these measurements were only approxi-mate owing to tissue deformation during the dissection.In our study we report on the correlation of lesion sizebetween MR images and histology.
In our study, both the hypointense core and hyperin-tense ring on both T2-weighted and FLAIR imaging werewithin the ultrasonic tissue damage zone seen on histo-logical sections. Given the nature of these studies,however, the reversibility of cell damage within thehyperintense ring (areas of spongiosis histologically)could not be determined. Lesion growth over time mightindicate an evolution of damage. Survival studies usingsimilar FUS techniques or studies using cell viabilitystains should be able to provide further informationregarding the degree of reversible vs irreversible celldamage within the hyperintense ring. These findingsare important in regard to treatment planning for can-cer therapy using MR-guided FUS, in which it is criticalto ensure destruction of all the tumor cells and to avoidleaving gaps between ultrasonic lesions.
Time Delay on MR and Location Dependence
Use of MRI as a guiding and monitoring system forthermal tissue ablation, including FUS, RF, and intersti-tial laser, requires that it be accurate and in real time.We have demonstrated that FUS lesions shown onT2-weighted and FLAIR images correlate well with theultrasonic lesion zone on histological sections. The timedelay for lesion onset on T2-weighted MR imaging isfrom 15 minutes to approximately 1 hour after FUStreatment, depending on the exposure location in thebrain. The time delay for thermal lesion formation onT2-weighted MRI was also observed by other investiga-tors. Farahani et al (20) reported that thermal lesionscreated in normal rabbit brain by an RF probe wereshown on T2-weighted MR imaging in approximately10–15 minutes. Morocz et al (24) reported that it took1–2 hours to detect MR signal intensity alterations inFUS lesions created in normal rabbit brains. Darkazanliet al (23) reported that lesions created in rabbit and dogmuscle showed up on T2-weighted images a few min-utes after FUS. Cline et al (14) also reported that thetime delay for FUS lesion shown on T2-weighted MRIwas approximately 15 minutes in rabbit muscle. Thesedata suggest that the time delay could vary significantlywith tissue type. We have carefully shown that it couldalso be significantly different within the same tissue
Figure 5. Measured values of lesion diameter by T2-weightedMR imaging and histology. The line of identity line is shown.The lesion size measured from MR correlated well with thatfrom histology after tissue shrinkage correction.
Figure 6. Time delay on T2-weighted MRI as a function of thedistance from olfactory lobe. The bars represent the knowntime range for the first appearance of the lesion on T2-weightedMRI from each FUS exposure. The left ends of the barsrepresent the time point at which the lesion had not yetappeared when the T2-weighted image was taken, and theright ends of the bars represent the first time point at which thelesion had appeared on a subsequent image. The lesion locatedfurther away from the olfactory lobe appeared earlier onT2-weighted MRI.
Study of FUS Tissue Damage by MRI and Histology 151

type at different locations. The mechanism behind thelocation dependence is poorly understood. Presumably,it relates to different anatomic structures and bloodperfusion rate. In clinical application of MR-guidedthermal therapy, the time delay effect should be consid-ered.
Lesion Growth After Thermal Ablation
Our results, demonstrating progressive growth of FUSlesions with time, are similar to those reported byFarahani et al (20) and Tracz et al (21). Farahani et al(20) showed that the lesion area in rabbit brain in-creased by 40% over the first 20 minutes after RFablation, and then reached a plateau. Schatz et al (20)showed that the histological lesion size in rabbit brainwas greatest at 48 hours after Nd.YAG laser ablation.However, this result was reported from a single measure-ment and compared with different rabbits at differenttimes of sacrifice after thermal ablation. Our studyshowed lesion growth at least over the first 2 hours after
treatment. However, from our study, it is not knownwhether the lesion plateau in size has been reachedwithin the 3 hour imaging interval (Fig. 8).
It is possible that the transition zone on histologymight be related to further lesion growth, although thecells looked normal at the time of animal sacrifice in thisstudy. In order to study FUS lesion growth in the brain,further investigation of long-term FUS tissue damageusing MR imaging is warranted.
ACKNOWLEDGMENTS
We would like to acknowledge GE Medical Systems andthe Lucas Foundation. We are grateful to Diane Howardfor her expert technical assistance.
REFERENCES1. ter Haar GR, Sinnett D, Rivens IH. High intensity focused ultra-
sound—a surgical technique for the treatment of discrete livertumors. Phys Med Biol 1989;34:1743–1750.
2. ter Haar GR, Rivens IH, Andrew V. Phase 1 clinical trial of the use offocused ultrasound surgery for the treatment of soft tissue tumors.SPIEs Int Symp Biomed Optics. 1998;3249–31:53–53.
3. Hill CR, Rivens I, Vaughan MG, ter Haar GR. Lesion development infocused ultrasound surgery: a general model. Ultrasound Med Biol1994;20:259–269.
4. Rivens IH. Quantitative studies of biological damage induced usinghigh-intensity focused ultrasound. PhD Thesis, University of Lon-don, 1992.
5. Yang R, Sanghvi NT, Rescola FJ, et al. Extracorpreal liver ablationusing sonography-guided high-intensity focused ultrasound. InvestRadiol 1992;27:796–803.
6. Hynynen K, Freund WR, Cline HE, et al. A clinical, noninvasive, MRimaging-monitored ultrasound surgery mothod. Radiographics1996;16:185–195.
7. Gelet A, Chapelon JY, Margonari J, et al. High intensity focusedultrasound experimentation on human benign prostatic hypertro-phy. Eur Urol 1993;23:44–47.
8. Madersbacher S, Kratzic C, Szabo N, et al. Tissue ablation in benignprotatic hyperplasia with high intensity focused ultrasound. EurUrol 1993;23:39–43.
9. Chapelon JY, Margonari F, Vernier F, et al. In vivo effects of highintensity ultrasound on prostatic adenocarcinoma Dunning R3327.Cancer Res 1992;52:6353–6357.
Figure 7. An example in one animal of time delay for bright ring to appear on T2-weighted MR images. The lesion appearedbetween 26 and 35 minutes after FUS exposure.
Figure 8. FUS lesions increased on T2-weighted MRI with timeafter FUS exposure. The connecting lines are drawn to indicatesame lesions. The lesion increases faster over the first 2 hours,and then slowly increases over the next 3 hours.
152 Chen et al.

10. Chartier-Kastler E, Chopin D, Vallancien G. The effects of focusedextracorporeal pyrotherapy on a human bladder tumor cell line(647V). J Urol 1993;149:643–647.
11. Capelon JY, Margonari J, Theillere Y, et al. Effect of high-energyultrasound on kidney tissue in the rat and dog. Eur Urol 1992;22:147–152.
12. Vaughan MG, ter Haar GR, Hill CR, Clarke RL, Hopewell JW.Minimally invasive cancer surgery using focused ultrasound: apre-clinical, normal study. Br J Radiol 1994;67:267–274.
13. Chen L, ter Haar GR, Hill CR, Eccles SA, Box G. Treatment ofimplanted rat liver tumors with focused ultrasound. UltrasoundMed Biol 1998;24:1475–1488.
14. Cline HE, Schenck JF, Watkins RD, Hynynen K, Jolesz FA, Mag-netic resonance-guided thermal surgery. Magn Reson Med 1993;30:98–106.
15. Cline HE, Hynynen K, Watkins RD, et al. Focused US system for MRimaging-guided tumor ablation. Radiology 1995;194:731–737.
16. Graham SJ, Chen L, Leitch M, et al. Quantifying tissue damage dueto focused ultrasound heating observed by Magn Reson Med1999;41:321–328.
17. Hynynen K, Damianou CA, Colucci V, et al. MR monitoring offocused ultrasonic surgery of renal cortex: experimental and simu-lation studies. J Magn Reson Imaging 1995;5:259–266.
18. McDannold N, Hynynen K, Wolf G, Jolesz F. MRI evaluation ofthermal ablation of tumors with focused ultrasound. J Magn ResonImaging 1998;8:93–100.
19. Rowland IJ, Rivens I, Chen L, et al. MRI study of rat liver tumorsfollowing high intensity focused ultrasound surgery. Br J Radiol1997;70:144–153.
20. Farahani K, Mischel PS, Black KL, et al. Hyperacute thermal
lesions: MR imaging evaluation of development in the brain. Radiol-ogy 1995;196:517–520.
21. Schatz SW, Bown SG, Wyman DR, Groves JT, Wilson BC. Lowpower interstitial ND-YAG laser photocoagulation in normal rabbitbrain. Laser Med Sci 1992;7:433–439.
22. Tracz RA, Wyman DR, Little PB, et al. Magnetic resonance imagingof interstitial laser photocoagulation in brain. Laser Surg Med1992;12:165–173.
23. Darkazanli A, Hynynen K, Unger E, Schenck JF. On-line monitoring ofultrasound surgery with MRI. J Magn Reson Imaging 1993;3:509–514.
24. Morocz IA, Hynynen K, Cudbjartsson H, et al. Brain edema develop-ment after MRI-guided focused ultrasound treatment. J MagnReson Imaging 1998;8:136–142.
25. Hynynen K, Vykhodtseva NI, Chung AH, et al. Thermal effects offocused ultrasound on the brain: determination with MR imaging.Radiology 1997;204:247–253.
26. Lele PP. A simple method for production of trackless focal lesionswith focused ultrasound: physical factors. J Physiol 1962;160:494–512.
27. Vykhodtseva NI, Hynynen K, Damianou C. Pulse duration and peakintensity during focused ultrasound surgery: theoretical and experi-mental effects in rabbit brain in vivo. Ultrasound Med Biol 1994;20:987–1000.
28. Hynynen K, Darkazanli A, Damianou CA, Unger E, Schenck JF. Theusefulness of a contrast agent and gradient-recalled acquisition in asteady-state imaging sequence for magnetic resonance imaging-guidednoninvasive ultrasound surgery. Invest Radiol 1994;29:897–903.
29. Hynynen K, Darkazanli A, Unger E, Schenck JF. MRI-guidednoninvasive ultrasound surgery. Med Phys 1993;20:107–115.
Study of FUS Tissue Damage by MRI and Histology 153