Embed Size (px)
Citation preview
—.. —
IndoorRadon:A Case
Study inDecisionmaking 6
w hen radon gas, which originates in the Earth’s crust,is emitted into the open air, it is rapidly diluted to thelow ‘background’ or ‘outside’ levels that are foundeverywhere and are inevitable. When it is emitted into
a home, school, or other building, dilution is slower, and theconcentrations of radon inside structures are usually higher thanthe concentrations outside. These higher levels raise healthconcerns because studies have shown higher levels of radon areassociated with higher rates of lung cancer in uranium miners andother workers exposed.
Responding to those concerns, Congress and the Environ-mental Protection Agency (EPA) have considered methods toreduce the risks posed by indoor radon. Most indoor radon entersbuildings directly from the soil, and efforts to reduce thoseexposures include EPA programs to inform homeowners aboutthe radon risks and how to reduce radon inflow into buildings.The private sector has also acted to reduce radon in homes byimposing requirements for measuring and, if deemed necessary,reducing indoor radon as a condition in real estate contracts.
EPA cannot, of course, regulate radon from soil because radonfrom that source enters homes directly without passage throughany entity that can be regulated. Some radon, however, entersbuildings through the water supply, and the agency can regulateradon in water just as it regulates other contaminants under theSafe Drinking Water Act (SDWA) (P.L. 93-523 and 99-339).
Some Members of Congress, including the Chairman of theHouse Committee on Science, Space, and Technology, asked the0ffice of Technology Assessment (OTA) to examine an ‘ ‘incon-sistency’ in EPA’s approach to radon. The request, which
145

146 ! Researching Health Risks
arrived after this study of health risk assessmentresearch had begun, resulted in an analysis ofissues related to radon, which is included in thisreport.
This chapter reviews and comments on thebases for assessing the risks posed by indoorradon and radon in water and discusses ongoingand possible future research projects. It alsodiscusses the policy issues surrounding the con-gressionally identified “inconsistency’ that arisesbecause of differences between the goal of theIndoor Radon Abatement Act (IRAA) (P.L. 100-551), EPA’s proposed level for the regulationof radon in drinking water under the SDWA,and the level of indoor radon at which EPAurges homeowners to take voluntary action toreduce radon infiltration (box 6-A). The inconsis-tency is quantitative: The IRAA sets the target forindoor air concentrations of radon as equal toconcentrations in outdoor air. The proposedregulation under the SDWA sets a stricter level,imposing regulations on water suppliers so thatemissions of radon from water to air would bereduced to about one-tenth of the level of radon inoutdoor air. The voluntary action level EPA urgesfor homeowners-about eight-times higher thanthe level of radon in out-door air-is higher thaneither the IRAA goal or the SDWA regulatorylimit. In response to the congressional request,this chapter also includes a rationale for “policyoptions for developing a consistent approach toreducing the risk from radon. ’
HOW LARGE IS THE WATERBORNERADON PROBLEM?
EPA (U.S. EPA, 1993b) estimates that about19 million people are served by water systemsthat exceed its proposed regulatory limit for radon
in water of 300 picoCuries per liter (pCi/L).l Toreduce current concentrations that exceed thathit, the agency has selected aeration as the BestAvailable Technology (BAT). A number ofaeration methods are available, which, accordingto EPA, will eliminate up to 99.9 percent of theradon as well as some fraction of other volatile,toxic contaminants from water (U.S. EPA, 1991).The volatility of radon, which makes aerationEPA’s treatment of choice, results in waterborneradon being a problem primarily in water suppliesthat depend on groundwater because radon insurface water volatilizes into the outdoor airbefore it enters buildings.
Some background information is necessary toput the proposed regulation of radon in water intoperspective. The proposed regulation dependsupon the interpretation of epidemiologic studies,congressional actions in response to the projectedregulation, some risk assessment models devel-oped by EPA, and a series of reviews by EPA’sScience Advisory Board (SAB).
RADON, MINING, AND INDOOREXPOSURES
Radon is a decay product of radium, whichitself is a decay product of the uranium foundubiquitously in the Earth’s crust. Radon alsoundergoes radioactive decay, and it is the prod-ucts of radon decay (called radioactive “prog-eny’ or “daughters”) that are associated withlung cancer. Radium and radon, of course, areespecially abundant in radioactive deposits, andthe Federal Government’s demand for uranium tomake atomic bombs during and after World WarII resulted in a rush to mine such deposits. As aconsequence, miners were exposed to high levelsof radon. Beginning in the 1950s, results from
1 A pico (p) Curie (Ci) is a measure of radioactivity. “Pico” means one-trilliont@ so a pico Curie (p@ is one-trillionth of a curie. OneCurie is equal to 3.7 X 1010 radioactive disintegrations per second and a pCi is then 3.7 X 10_2 per second or 2.2 disintegrations per minute.The measure 4 pCi/L means that the radioactivity in one liter (L) of air (or water) produces 4 X 2.2 disintegrations per minute = 8.8disintegrations per minute. Although pc,m is the unit of measure most often used in the United States to express concentrations of radioactivity,in other countries, “Bq/rn3’ is more commonly used. A becquerel (B@ is equal to 37 pCi, and one cubic meter (m3) is equal to one L. ‘1’kmforc,1 pCi/L is @ to 37 Bq/LU3. (Usually, when conversions between the two units of measure are made and no calculator is available, theconversion factor is @, that is, 1 pCi/L is about equal to 40 Bq/rn3.) Various detectors are available to measure radioactive disintegrations.

——
Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 147
Box 6-A--Reducing Exposures to Radon: A Goal, an Action Level,and a Regulatory Standard
Nazaroff and Teichman (1990)1 calculate that current exposures to radon are associated with about 15,700lung cancer deaths annually. They estimate that 97 percent of those deaths will occur in smokers, and 3 percentwill occur in nonsmokers. Indoor concentrations of radon are higher than those outdoors, and the FederalGovernment is directing several efforts at reducing indoor exposures. At present, there is a goal for reducing indoorradon concentrations, an action level to guide voluntary reductions, and a proposed regulation to reduceconcentrations of radon in water.
A Goal: The Indoor Radon Abatement Act sets the goal of reducing indoor radon concentrations to theconcentrations found outdoors-0.4 pCi/L. Currently, the average indoor concentration is about 1.5 pCi/L, withabout 6 percent of all houses having concentrations greater than 4 pCi/L. The Environmental Protection Agencystates that it is difficult to reduce indoor levels below 2 pCi/L (apparently for houses that have levels greater than4 pCi/L).
An Action Level: EPA recommends that indoor radon concentrations be reduced to 4 pCi/L or below, a levelconsidered technologically feasible for all houses. Reducing all indoor radon concentrations that are now greaterthan 4 to 2.7 pCi/L is expected to eliminate about 3,500 deaths (a reduction of about 17 percent). (The level of2.7 pCi/L is the mean between the national average of about 1.5 pCi/L and the action level of 4 pCi/L.)
A Regulatory Standard: Under provisions of the Safe Drinking Water Act, EPA proposes regulating radonin drinking water so t hat t he concentration of radon in air that results from the volatilization of radon from drinkingwater is no more than 0.03 pCi/L. According to EPA, reducing all higher concentrations of radon in water to thislevel would eliminate 80 radon-associated lung cancer deaths annually (a reduction of about one-hatf of 1 percent).
1 W,W, Nazaroff and K. Teichman, “Indoor Radon,” IEnvlrorvnenta/ S&nC61 and 7bchno@Y24(1990):774-782.
SOURCE: Office of Technology Assessment, 1993.
studies by the Atomic Energy Commission a result of studying human populations. Usually,showed that lung cancer was more common inU.S. uranium miners than in other men, andstudies of miners elsewhere—in Czechoslovakia,Sweden, and Canada—reported similar results(Brill, 1990).
Results from studies of miners identify radonas a hazard to human health, and assessing the riskthat radon poses to human health is free from theproblem of animal-to-human extrapolation thatbesets most health risk assessments. Those resultsidentify radon as a hazard, but they leave riskassessors and decisionmakers with the problem ofextrapolating from the effects seen at ‘‘highexposure levels’ in the miners to estimates ofexpected effects at the, generally, ‘‘low exposurelevels” found in houses, Such high-to-low ex-trapolations are a common issue with substancesthat are identified as a hazard to human health as
researchers accumulate the human data fromstudies of people exposed to high concentrationsof chemicals or radiation in the workplace or inmedical practice. Then those data must be used toextrapolate to the risks at lower ‘‘environmental’exposures (U.S. Congress, OTA, 198 1; U.S.DHHS, National Toxicology Program, 1991).
In the late 1970s, Congress recognized somerisks posed by nonoccupational exposures toradon and passed the Uranium Mill TailingsRadiation Control Act of 1978 (P.L. 95-604).That act directed EPA to set limits on radonemissions from inactive uranium processing sitesand to establish acceptable levels for indoor radonin buildings associated with those sites.
That narrow focus on occupational or residualexposures that remained from closed-down min-ing and refining operations disappeared in 1984.

148 I Researching Health Risks
As the story is commonly told, it ended whenStanley Watras, an engineer at the LimerickNuclear Power Plant in eastern Pennsylvania,passed through a radiation detector at the plant.He triggered the detector’s alarm every day foralmost 2 weeks in a row, which was surprisinggiven that his co-workers seldom triggered thealarm. Mr. Watras guessed that his radioactivecontamination might be coming from a sourceother than his work, and as an experiment onemorning, he went directly to the detector beforehe went to his job. The alarm sounded. Asubsequent inspection showed that Mr. Watraswas bringing in radon from his house on hisclothing and his person. Measurements in hishouse showed radon levels that resulted in aradiation dose well above those permitted inindustrial settings (Taylor, 1990). What is lesscommonly reported is that Mr. Watras’ house wasdirectly over the tunnel of a uranium mine andthat the house next door had only backgroundlevels of radon, about one-thousandth of thosedetected in his house (Moeller, 1989).
Although some scientists had identified indoorradon as a hazard by the late 1970s (Nero, 1990),Mr. Watras’s saga began the process that widelypublicized radon in homes as a health risk. Within2 years, EPA (1986) published A Citizen’s Guideto Radon, which” attributed between 5,000 and20,000 lung cancer deaths annually to exposure to
radon. A year later, when the agency (U.S. EPA,1987) cataloged sources of environmental cancerrisks, the numerical estimate for cancer mortalityfrom indoor radon (between 5,000 and 20,000annual deaths) was about the same as the estimatefor mortality from skin cancer (10,000) caused byexposure to sunlight. Both of those estimateswere much higher than risks of cancer associatedwith other sources (table 6-l). In the 1992revision of A Citizen’s Guide to Radon, EPA andthe Department of Health and Human Services(DHHS) estimated that radon causes about 14,000cancer deaths annually (U.S. EPA and DHHS,1992). Although EPA’s estimates have variedacross the years, they have consistently associ-
Table 6-1—Major Environmental Cancer Risksand Cancer Risks From Water
Estimated annualSource of risk cancer mortality
Indoor radon . . . . . . . . . . . . . . . . . . . . . 5,000-20,000’Sunlight . . . . . . . . . . . . . . . . . . . . . . . . 10,000All airborne cancer risks (excluding radon 2,267-3,294
and environmentaltobacco smoke) . . . . . . . . . . . . . . .
Pesticides . . . . . . . . . . . . . . . . . . . . . . . 3,075-6,150Radiation in drinking water. . . . . . . . . 37-730 b
All chemicals in drinking water . . . . . . 215-430
a ~her EPA estimates vary upwards from this range.b ~her EPA estimates vary within this range.
SOURCE: M. Gough. 1989. “Estimating Cancer Mortality.” l%timmrner?td Sdeme and T@no/ogy 23:925-930, based on U.S. Environ-mental Protection Agency. 1987. Unfkdshed Business.
ated several thousand cancer deaths with expo-sures to radon.
Smokers are much more likely than nonsmok-ers to develop lung cancer as a result of radonexposure. Nazaroff and Teichman (1990) esti-mate that only 3 percent of the projected mortalityfrom radon-associated lung cancer will occur innonsmokers; EPA (1992a) estimates that 70percent of deaths from radon-related lung cancerwill occur in smokers, 24 percent in formersmokers, and 6 percent in nonsmokers. In the1992 Citizen’s Guide (U.S. EPA and DHHS,1992), EPA and DHHS point out that, fo rsmokers, the most important step to reduce risksfrom radon is to quit smoking.
Currently, EPA recommends that homeownerstake action to reduce indoor radon concentrationsto 4 pCi/L, a level that can be reached in almostevery home. The agency also states that levels inmany homes can be reduced even more, to about2 pCi/L (U.S. EPA and DHHS, 1992). This goalof 2 pCi/L is a little higher than the average indoorconcentration in the United States (1.25 pCi/L),and it is from about 3 to 6 times higher than theoutdoor average concentration of 0.3 to 0.5 pCi/L.Remediation methods recommended by EPAinclude increasing ventilation below slabs andsealing basements and foundations to reduceentry of radon.

Chapter 6: Indoor Radon: A Case Study in Decisionmaking 1149
Interest in the health effects of indoor radon hasprompted more than a dozen epidemiologicstudies comparing the rates of lung cancer inpeople who live in homes with higher levels ofradon with those of people who live in homes withlower levels. Interpreting results from the variousstudies and attempting to reconcile conflictingresults require that some attention be given tohow the studies were designed and executed.
EPIDEMIOLOGIC STUDIES OFRADON-RELATED LUNG CANCER
Epidemiology is the study of the distributionsof diseases in populations and the conditions thatcontribute to the appearance or progression ofdiseases. The most basic epidemiologic infor-mation is provided in a case report, whichdescribes the occurrence of a disease (usually rareand therefore attracting attention) or a cluster ofcases of a disease. Such reports identify popula-tions for further investigation or study, but theyprovide no analysis of the putative links betweenexposure and disease, For example, a report of arare form of muscle disease in a worker in achemical plant would alert health professionals toa possible link between that disease and expo-sures to some toxic agent in the plant. But thedisease could have occurred completely bychance, and further investigation would be neces-sary to examine the worker’s exposures to spe-cific chemicals and other studies would be neededto see whether other exposed workers sufferedfrom the same disease or some precursor to it.
Beyond case reports, most epidemiologic re-search can be classified as one of three kinds:ecological studies, case-control studies, andcohort studies. Researchers have used all threetypes to investigate relationships between radonexposure and lung cancer. In general, ecologicaland case-control studies have been used toexamine questions about indoor radon and case-
control, and cohort studies have been employedfor investigations in occupational populations.
In ecological studies, scientists compare ratesof lung cancer in populations in geographicalareas that have different average levels of expo-sure to radon. Case-control studies involve locat-ing cases (persons who have lung cancer or therecords of people who have died from lungcancer) and comparing the exposures of the casesto the exposures of controls (people who do nothave lung cancer). In a cohort2 study, scientistscompare the rates of lung cancer in a group ofpeople, such as miners, who share types, times,and intensities of radon exposure that differ fromthose of other groups. In ecologic and cohortstudies of a disease as common as lung cancer,many cases of the disease will be expected in allthe studied populations. Finding that the rate ofthe disease is higher in a population exposed tohigher levels of radon is taken as evidence of aconnection between exposure and disease afterruling out other factors that might account for thedifference. For instance, if smoking was morecommon in the group with higher rates of lungcancer, a careful analysis would be necessary toascertain the separate and combined effects ofsmoking and radon.
Ecological studies provide no direct compari-sons between the exposures of individuals andtheir diseases. Such studies are relatively easy todo in areas in which records of disease incidenceor deaths are available and in which there havebeen enough measurements of indoor radon thatscientists can estimate average levels of exposurefor the area. When completed, however, ecologi-cal studies provide no information about whetherthe persons who developed the disease hadexposures near the average level or well above orbelow it.
Case-control studies are useful for studies ofboth indoor radon and exposures in theworkplace, and they can provide information
z As an epidemiologic teq a‘ ‘cohort’ is a group of people who share certain cha.racteristics (the word cohort originally identified on-tenthof a Roman legion).

150 I Researching Health Risks
about individual exposures and frequency ofdisease. One stumbling block for such studies isthe difficulty of determining all past exposures toradon. For instance, many people move severaltimes during their lifetimes, and a completeinventory of their exposures to indoor radonwould require measurements in each of theirhomes. A further complication in interpretingsuch studies is how to make allowances for‘‘competing risks’ that contribute to the risks ofdeveloping lung cancer. The most important issmoking; the second most important is probablyenvironmental tobacco smoke (Brownson et al.,1992).
Most of the available quantitative informationabout the risks posed by radon comes from cohortstudies of uranium miners that compare the ratesof lung cancer among the miners with ratesamong other workers. Because of the latent periodof 20 or more years between exposure to radonand the appearance of lung cancer, scientists whostudy rates of lung cancer among miners are mostinterested in their levels of exposure over twodecades ago and more. That need for a long-termview complicates interpretation of the studiesbecause accurate measurements are seldom avail-able for past exposures.
Ecological StudiesThe absence of direct ties between the exposure
of an individual and his or her health statuscomplicates interpreting the results of ecologicalstudies. Using average (or group) information toestimate exposures results in the “ecologicalfallacy,’ which links together specific healthconsequences among individuals and estimates ormeasures of average exposures. Only careful (andperhaps impossible) analysis would clarify whetherthe group measure was appropriate to describe theexposure of a person with a disease.
Although it may seem reasonable to concludethat people with an illness in a group exposed toa higher average level of radon were exposed tomore radon than people exposed (on average) to
lower levels of radon, there is no way to be certainof that. No single ecological study nor thecomplete set of such studies taken together willresolve the question of whether nonoccupationalexposure to radon increases the rate of lungcancer.
Samet (1989) reviewed 11 ecological studies:
In spite of crude exposure measures, most ofthese studies showed associations between expo-sure to radon decay products and the incidence ofor mortality from lung cancer. Two studies ofcounties in the Reading Prong [the area ofPennsylvania in which Mr. Watras lived] are ofparticular interest because of the high number ofhomes in this region with high radon concentra-tions.
Of particular interest in discussions of radon inwater and health risks are two studies reviewed bySamet (1989) that analyzed rates of lung cancer inrelation to levels of radioactivity in water sup-plies. One of the two studies found an increase inrates of lung cancer in both men and women as afunction of estimated greater exposures to radon;the other found an increase in men but not inwomen. The latter result would be an unexpectedone if radon in household water made a signifi-cant contribution to the risk of lung cancer.
Overall, Samet (1989) concluded that 5 of the11 studies were consistent with a correlationbetween exposure of higher levels of radonexposure and lung cancer, and one (one of the“water’ studies) found an increase in men butnot in women. Four of the 11 found no statisti-cally significant increase in rates of lung cancer;one study reported an inverse correlation betweenexposures to radon and rates of lung cancer. That‘‘negative study and others done by the samescientist and his colleagues have received a greatdeal of attention, perhaps because the associa-tions run counter to conventional ideas aboutradon and risk (Hanson, 1989).
Cohen (Cohen, 1990, 1992) investigated asso-ciations between rates of lung cancer and levels ofradon using tens of thousands of measurements in

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 151
living areas and basements in houses in the 48contiguous States of the United States. On the onehand, Cohen accepts that the ecological fallacymeans that such studies cannot shed light on thequestion whether radon causes lung cancer be-cause there is no way of knowing the levels ofexposure of the people who develop lung cancer.On the other hand, he argues that the ecologicalfallacy does not prevent such studies from an-swering the question of whether a linear, no-threshold relationship exists between exposure toradon and lung cancer (see the discussion in ch.2). According to Cohen, if that relationship iscorrect, cancer rates should vary directly withaverage countywide exposures. Cohen found thatrates went down as exposures increased.
Immediately, objections were raised to Cohen’sfinding. For instance, how does smoking varyfrom county to county? Cohen’s response was tocompare cigarette sales in different States, factorthat information into his analysis, and demon-strate that the negative correlation between levelsof radon and lung cancer persists. What kind ofcorrelation would be expected between currentrates of lung cancer and current householdexposures? Given the latent period betweenexposure and manifestation of disease, the expo-sures of interest occurred many years ago. Cohenhas adjusted his analysis to consider that fact andhas accumulated measurements of radon levels infar more houses than any other investigator.Nevertheless, other investigators have reportedno replications of Cohen’s results.
Taken together, the ecological studies presenta confusing picture. Each additional study, whetherit shows a positive association, no association, ora negative association, can be added to the tally,but no one study by itself nor all the ecologicalstudies taken altogether will convince everyoneabout whether low-level radon is associated withlung cancer. Moreover, calculating reliable, quan-titative estimates of risk from such studies isimpossible.
Case-Control StudiesCase-control studies provide more definitive
information about exposure than do ecologicalstudies. In case-control studies of indoor radon,scientists (Blot et al., 1990; Schoenberg et al.,1990; Svensson, Pershagen and Klominek, 1989)often focus on women because fewer womensmoke compared with men, and women typicallyspend more time at home.
Like the ecological studies, the case-controlstudies have yielded contradictory results. Forinstance, both Schoenberg et al. (1990) andSvensson et al. (1989) reported elevated levels oflung cancer among women who lived in houseswith higher levels of radon. As the authors ofthose papers pointed out, the numbers of womenincluded in the studies, especially the numbers ofwomen exposed to higher levels of radon, werequite small. Only 24 of 433 women with lungcancer in the Schoenberg et al. (1990) study hadlived in homes with concentrations of radongreater than 2 pCi/L. The small number of casesmakes it difficult to interpret those studies, andmany results showing excesses of cancer in themore highly exposed women were not statisti-cally significant; that is, the excesses that weredetected might have arisen by chance. Further-more, no consistent relationship was found be-tween smoking habits and lung cancer in theSchoenberg et al. (1990) and Svensson et al.(1989) studies, which introduces some uncer-tainty in interpretation because smoking and ratesof lung cancer rates usually vary directly witheach other.
Blot et al. (1990) studied women in a provinceof China and found that ‘No association betweenradon and lung cancer was observed regardless ofcigarette-smoking status, except for a nonsignifi-cant trend among heavy smokers. ’ Those authorsgo on to interpret their results as indicating that“projections (of cancer risk) from surveys ofminers exposed to high radon levels may haveoverestimated the overall risks of lung cancerassociated with levels typically seen in this

152 I Researching Health Risks
Chinese City. ” Letourneau et al. (1993) reportedcomparable results from a case-control study of750 people with lung cancer in Winnipeg, Can-ada. They found that ‘‘no increase in the relativerisk of any of the histologic types of lung cancerobserved among cases was detected in relation tocumulative exposure to radon. ’
Lubin et al. (1993) prepared an analysis andcomparison of the Blot, Schoenberg, and Svens-son studies and concluded that any link betweenexposure to radon and risk of lung cancer is onlyweakly demonstrated in the studies, if it is presentat all. Nevertheless, the fact that no increase wasdetected does not necessarily mean that none wasthere. It might have been present but undetectablebecause of the (small) size of the study.
Similarly, Ruosteenoja (1991) found “no sig-nificant correlation between the average radonexposure and incidence of male lung cancer.Yet, as the author pointed out, her study had littlechance to detect the level of risk predicted fromthe miner studies. As in other studies, the smallnumber of cases made it possible that any effectof radon that was present went undetected againstthe number of lung cancer cases expected regard-less of the presence or absence of radon.
So far, case-control studies leave open the twopossibilities that either the risk of developing lungcancer from exposures to indoor radon are zero(or at least below the limit of detection) or that itis compatible with the level of risk estimated fromthe miner studies. Additional case-control studiesof sufficient size and ‘‘power’ might provide theinformation needed to determine whether risksprojected from the miner studies are realized inpeople exposed to lower levels.
One alternative to a single large study is tocarry out a meta-analysis of the already com-pleted and soon to be completed studies and tocombine those results to produce a more defini-tive answer. Meta-analysis is not a panacea, but itis a developing subdiscipline with applications toepidemiology (Dickersin and Berlin, 1992) andrisk analysis (Society for Risk Analysis, 1993) aswell as in health and behavioral sciences in
general (Olkin, 1992). The Department of Energyhas begun preparations for conducting a meta-analysis of case-control studies to begin in about2 years when some ongoing studies will havebeen completed.
Researchers expect important findings fromtwo ongoing studies in the United States thatinvolve Midwesterners who tend to live in onehouse for long periods and who live in eitherMissouri or Iowa, States with relatively highradon concentrations. Of 524 homes examined inMissouri, 33(8 percent) had radon concentrationsof 4 pCi/L or greater, and 8 (2 percent) hadconcentrations more than 8 pCi/L. Results al-ready reported from that study verified predic-tions by Lubin et al. (1990) that people who movefrequently have lower exposures than people whoremain in a single home. Given the relative rarityof ‘hot homes, ’ a person who moves from sucha home is more likely than not to move to a housewith lower levels. Alavanja et al. (1992) reportthat 11 percent of Missouri women who lived ina single house for 30 years had been exposed toconcentrations greater than 4 pCi/L for that time;6 percent of women who lived in two houses hadexposures that high; and none of the women wholived in three or more houses had such exposures.Investigators expect to complete their analysis ofthe relationships between levels of radon andcancer incidence in the 600 nonsmoking womenwith lung cancer in the study by mid-1993 and topublish them by the end of the year.
A research team at the University of Iowa isconducting the second Midwestern study. Theinvestigators are studying women who smoke, toshed light on interactions between smoking andradon in cancer causation; studies of women whodo not smoke are expected to identify any directrelationships between radon and lung cancer(Lynch, 1993). Equal in size to the Missouristudy, the Iowa study includes a total of 600 casesof lung cancer and 1,400 controls. From theresults of the EPA survey of radon in homes, itappears that about 70 percent of Iowa homes haveradon concentrations greater than 4 pCi/L, and

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 153
those higher radon 1evels favor detecting associa-tions between exposures and lung cancer-if theyexist. The principal investigator of the studyexpects results to be published in late 1997.
Cohort StudiesSince the 1950s, scientists have studied the
health of miners (in particular, uranium miners,who were frost seen to be at risk) and determinedthat exposure to radon increases the incidence oflung cancers. Samet (Samet, 1989) reviewed 20studies of underground uranium miners andconcluded that the data show consistent relation-ships between exposure to radon and elevatedrates of lung cancer.
Exposure levels of the miners are expressed inworking-level months (WLM), which are anapproximation of the radiation exposure experi-enced by a uranium miner in 1 month’s work.Miners in the various epidemiologic studies ofradon had histories consistent with cumulativeoccupational exposures that ranged from 1 to10,000 WLM. The current occupational limit forexposure to radon is 4 WLM annually (NRC,1988), and a miner exposed at the current limit for40 years would accumulate 160 WLM from hisworkplace. In comparison, the 70 years lifetimecumulative exposure of residents of homes withaverage concentrations of indoor radon is about20 WLM (Samet, 1989).
As might be expected, cancer is far morefrequent in the miners exposed to hundreds orthousands of WLM than in those exposed to lowerlevels. However, Bodansky (1990), in a review ofthose data, stated “ . . . miner studies do seem tosuggest a statistically significant positive effect,for cumulative exposures as low as 20 to 50WLM. When the cumulative exposure is low,however, either due to low radon levels or shortduration of employment, the data is vulnerable toconfounding factors. ’ Despite the suggestedeffect at exposures below 100 WLM, correlationsbetween rates of lung cancer and higher levels ofexposure dominate the risk assessment.
A question is raised whether the relationshipsseen between cancer and radon at hundreds ofWLM, which are experienced in a few years,accurately predict cancer risks at levels of 10 or20 WLM accumulated over a lifetime. Somescientists in EPA’s Office of Science, Planningand Regulatory Support (Ulsamer, 1993) describethe problem this way: “The potential effects ofdifferences in dose rates between miners (whoare exposed for an average of 7 years to20+ WLM/yr) and home residents (who areexposed for an average of 72 years to 0.22WLM/yr from soil radon and 0.01 WLM/yrfrom water radon) . . . needs to be discussed.”In this respect, indoor radon is a prime example ofa problem in high-to-low-dose extrapolation.
Other CancersHenshaw and his colleagues (Henshaw et al.,
1990; 1992) reported associations between levelsof radon and the incidence of some cancers otherthan lung cancer in several countries. Thoseinvestigators relied upon ecological studies, mak-ing their results subject to the ecological fallacy,which reduces their value for decisionmaking.Although some scientists have treated the associ-ations as possibly indicating a role for radon inother cancers (Pete, 1990), Doll (1992) points outthat rates for none of the cancers that Henshaw etal. (1990) associate with radon exposure wereelevated among miners, and a recently publishedstudy of 4,000 Czech miners found no associationbetween radon exposure and leukemia (Anon,1993a). Moreover, Miller et al. (1993) directlyexamined the possibility of an association be-tween residential exposure to radon and theoccurrence of a form of leukemia that had beensuggested by Henshaw et al. (1990). They foundno evidence for the association. Currently, thereis little support for an association betweenexposures to radon and other cancers.

154 I Researching Health Risks
POLICYEPA divides its regulatory programs along
media lines-air, water, industrial wastes, and soforth. It has approached the issue of indoor radonas a media problem; thus, it has different policiestoward radon entering buildings in air and water.The agency has not proposed regulating radonthat is emitted directly from the soil, but it hasproposed regulation of water suppliers as amethod to reduce exposures to radon. Somescientists, Members of Congress, and other poli-cymakers have recognized that indoor radon isonly a single part of the larger issue of indoor airpollution, which presents assessment, remedia-tion, and regulatory difficulties different fromthose associated with pollutants in outside air.
Table 6-2-Comparison of Short-Term In-BasementMeasurements of Radon in Air and Estimated
Annual Exposures in Living Areas
If short-term Then estimated annualresult is: radon level is:
1 pCi/L 0.3 pCi/L2 0.73 1.04 1.3
5 1.76 2.07 2.38 2.7
9 3.010 3.311 3.712 4.0
A i rIn 1986, EPA estimated that 7 million U.S.
homes had concentrations of radon above 4pCi/L, the level at which the agency wouldrecommend remedial action. Subsequently, as aresult of its National Residential Radon Survey(EPA, 1992b) which involved measurements ofradon in houses around the country, the agencyreduced that estimate. Based on that survey, EPAnow estimates that between 60,000 and 100,000homes have concentrations of radon of 4 pCi/L ormore and that the average home has a concentra-tion of around 1.25 pCi/L.
The fact that EPA does not regulate airborneradon does not mean that those exposures havegone unaddressed. EPA distributed A Citizen’sGuide to Radon in 1988 and a revised documentin 1992 as part of an information program to alertcitizens about the risks from indoor radon. Someexperts have questioned whether the guidesprovide the appropriate information. In particular,Nero (1992) and others have criticized EPA forurging that all houses be tested because they seethat policy as distracting attention from homes inthe areas with the highest concentrations of radon.The critics have also faulted EPA for not focusingon persuading residents to mitigate concentra-
NOTE: pCi/L = pico Curies per liter.
SOURCE: Office of Technology Assessment, baeed on U.S. Environ-mental Protection Agency, F?eporthg on Radon (1989), pereonalcommunication from M. Reimer, U.S. Geological Survey.
tions of radon in houses with levels of 20 pCi/Lor higher. Those levels are higher than theexposures currently allowed for miners and otherworkers exposed to radon. According to thosecritics, EPA has dissipated the force of itsmessage by calling for remediation in any housewith levels greater than 4 pCi/L. Some expertshave also objected to EPA’s telling citizens to acton the basis of short tests of 2 to 7 days rather thantesting for a year to obtain more accurate results.
The data in table 6-2 demonstrate the impor-tance of appropriate testing techniques. Severalyears ago, EPA recommended that testing forradon be done with radiation detectors placed inthe basements of homes and that the homes bekept closed up during the measurement period. Asa result, the measurements were taken in the areaof the house with the highest level of radon,regardless of whether anyone spent any time inthat area, and under conditions that reduceddilution of indoor radon by outside air enteringthrough open doors and windows. As shown inthe table, measurements under those conditionswere three times higher than the year-round
Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 155
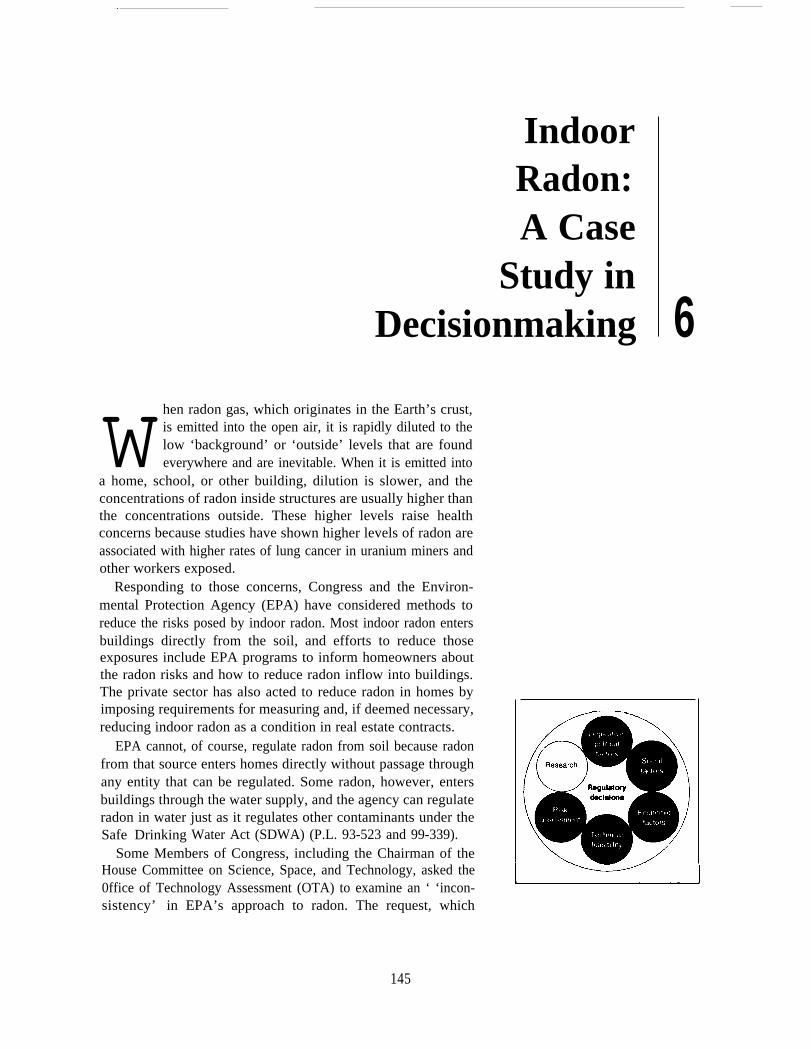
Table 6-3-Current Estimates of Radon-Associated Lung Cancer Deaths andReductions Expected From Reducing Indoor Exposures
Former Non-Source Smokers smokers smokers Total
Estimated number of annual radon-associated cancer deathsNazaroff and Teichman . . . . . . . . . . . . . . . . . . . . . 15,200’ 500 15,700Environmental Protection Agency . . . . . . . . . . . . 9,600 3,200 800 13,700
Estimated number of annual averted deaths at reduced exposuresExposures Former Non-reduced to Smokers smokers smokers Total
Nazaroff and Teichman . . . . . . . . . . . . . . . . . . . . . 2.7 pCi/L 2,300 200 2,500Environmental Protection Agency . . . . . . . . . . . . 4.0 1,500 500 100 2,200Environmental Protection Agency ., . . . . . . . . . . 3.0 1,800 600 200 2,600Environmental Protection Agency ... , . . . . . . . . 2.0 2,300 700 200 3,100Office of Technology Assessment . . . . . . . . . . . . 1.3b 5,000’
NOTE: pCi/L - pico Curies per liter.a Nazaroff and Tekhman combine current and former smokers in their CalCUktiOnS.b Average indoor mmetltratlon of radon in the Unitf3d states.c lnteTolat~ from figure 6-1.
SOURCES: W.W, Nazaroff and K. Teichman, “indoor Radon,” Erwionmentd Sckwwe and TAno/ogy 24(1990):774-782; U.S. EnvironmentalProtection Agency, Technical Support Dowment for the 1992 Citizen’s Guide to Radon, EPA 400-R-92-011 (Office of Technology Assessment,1993).
average measurement of radiation in the livingquarters of the house with ordinary ventilationand household traffic. EPA now recommends thatmeasurements be made in the lowest livingquarters of the house rather than in the basement.
Despite disagreements about the content ofEPA’s information materials, some people haveclearly heard the message that indoor radon is arisk that can be addressed. Indeed, in some Statesand counties, radon inspections, like inspectionsfor termites, are now part of real estate transac-tions. As a rule, inspecting for radon is notrequired by law or regulation but is part of theagreement between buyer and seller. For exam-ple, in Montgomery County, Maryland, mostsales contracts require a 2-day sampling forradon. If the concentration is 4 pCi/L or higher,the buyer may require the seller to take remedialaction to reduce the level.
Both Nazaroff and Teichman (1990) and EPA(1992a) have calculated the number of deathsfrom lung cancer that might be avoided byreducing exposures to indoor radon. Nazaroff and
Teichman (table 6-3) estimate that reducingconcentrations of radon to 2.7 pCi/L in all homesthat currently have concentrations above 4 pCi/Lwould prevent 200 deaths per year from lungcancer among nonsmokers and 2,300 deaths peryear among smokers (leaving about 12,000 radon-associated lung cancer deaths).
EPA’s (1992a) estimates are quite similar. EPAcurrently recommends that all homeowners takeaction to reduce any exposure in excess of4 pCi/L, and that level is often called the ‘‘actionlevel.’ Reductions of all current exposures abovethe action level to 4 pCi/L are calculated to reducethe lung cancer death rate by 2,200, with 100deaths being prevented in nonsmokers (table 6-3).The expected reductions in death rates increasewith further reductions in exposures to radon:reducing all indoor exposures now above 3 pCi/Lto 3 pCi/L would prevent about 2,400 deathsannually in smokers and former smokers and 200deaths among nonsmokers; reducing exposures to2 pCi/L, which EPA (1992a) considers near thepractical limit for mitigation efforts, is calculated
156 I Researching Health Risks
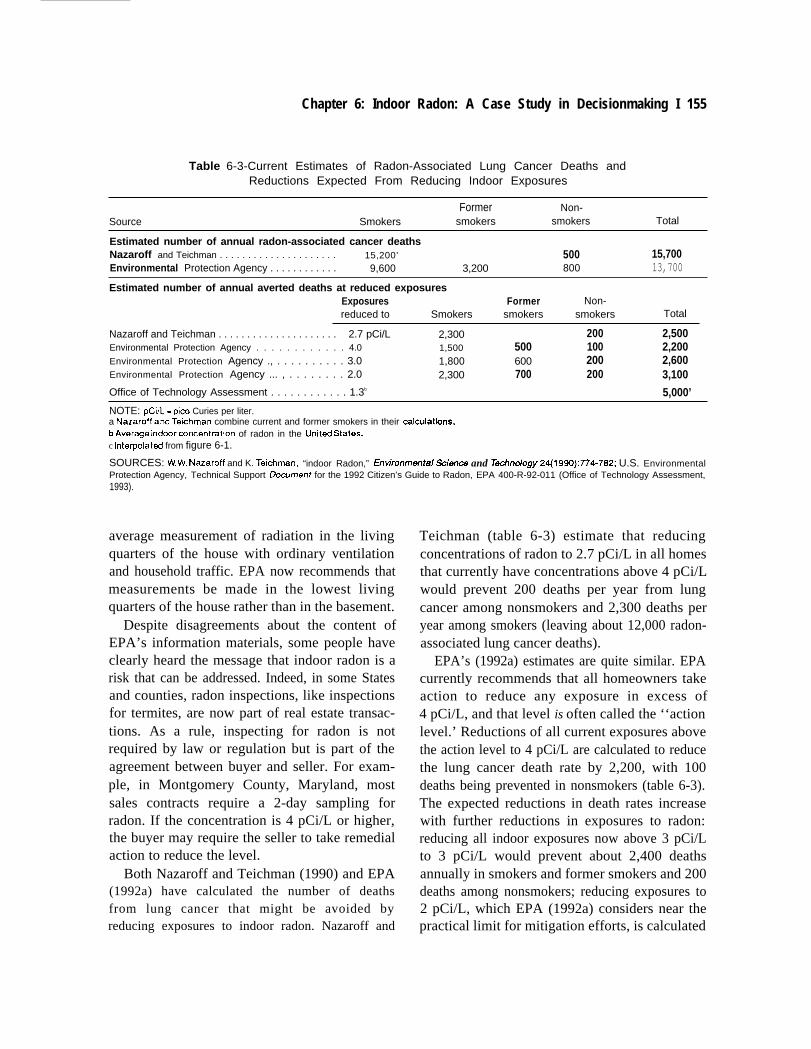
to lower the annual death rate from lung cancer byabout 3,100, leaving about 10,500 such deathsassociated with radon (figure 6-l).
As is apparent from figure 6-1, the bulk ofcancers associated with radon exposure occurs inthe population exposed to low levels, below 2pCi/L. The primary reason for that is that manymore people are exposed to those levels than tohigher levels. Given EPA’s conclusion that it isimpossible to reduce levels below 2 pCi/L insome houses, the practical lower limit on thenumber of deaths associated with radon maybe ashigh as 10,500. This estimate is based, of course,on extrapolations from the miners studies, andrefinement of those extrapolations might reduceor increase the estimate of the number of cancersassociated with radon.
Interpolating from the data on figure 6-1, OTAestimates that reducing all indoor exposures nowabove 1.25 pCi/L to that level, which is the U.S.average, would avert about 5,800 radon-associated lung cancer deaths annually (table6-3). That would leave 7,900, a little over half, ofradon-associated lung cancer deaths unabated.
Because radon is present in all air, both insideand outside, it is impossible to have zero radonexposures. Thus, some risk of death from radon-associated lung cancer is always present if it isassumed that there is no threshold for radon-associated lung cancer deaths, and as is shown onfigure 6-1, exposures to radon in outside air areassociated with about 500 lung cancer deathsannually.
The National Research Council’s (NRC, 1983)distinction between risk assessment and riskmanagement calls for deliberations at two levels:
1. Is there a risk?2. If there is one, what methods are most suited
for its control?
For radon in homes, EPA’s Technical SupportDocument for the 1992 Citizen’s Guide to Radon(EPA, 1992a) provides the agency’s reasoningbehind choosing 4 pCi/L as the level at which
Figure 6-1—Estimates of Deaths From Lung Cancerat Different Levels of Radon Exposure
14,000●
g 12,000-
s6 10,000-kn~ 8,000-ca2 6,000-
:
24,000-
.-fi 2 , 0 0 0 -
●
01 r 1 I [ I
o 4 8 12 16 20 24
Maximum exposure level (pCi/L)
SOURCE: Office of Thnology Assessment, 1993.
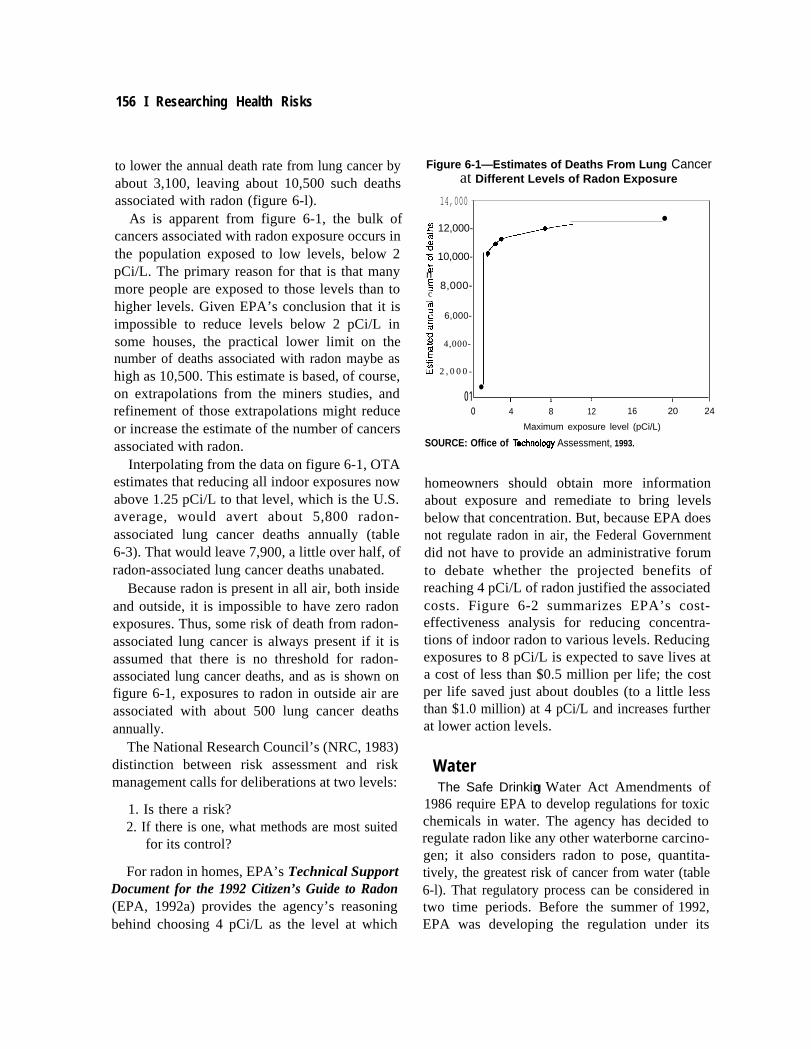
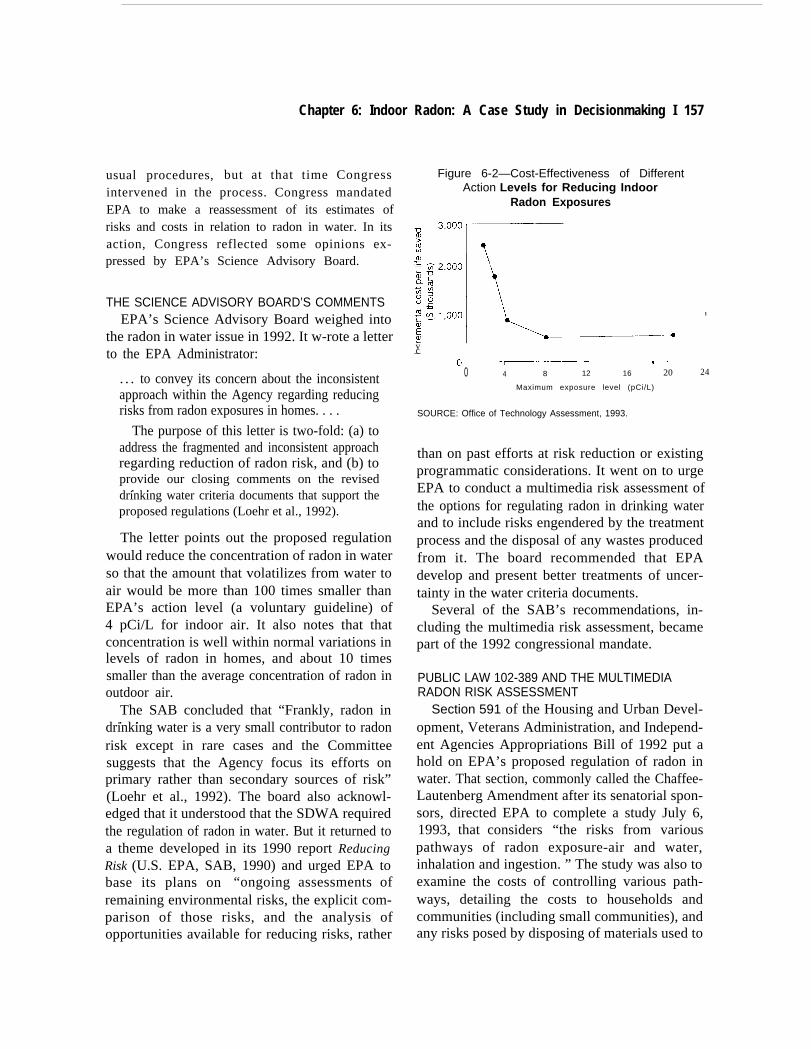
homeowners should obtain more informationabout exposure and remediate to bring levelsbelow that concentration. But, because EPA doesnot regulate radon in air, the Federal Governmentdid not have to provide an administrative forumto debate whether the projected benefits ofreaching 4 pCi/L of radon justified the associatedcosts. Figure 6-2 summarizes EPA’s cost-effectiveness analysis for reducing concentra-tions of indoor radon to various levels. Reducingexposures to 8 pCi/L is expected to save lives ata cost of less than $0.5 million per life; the costper life saved just about doubles (to a little lessthan $1.0 million) at 4 pCi/L and increases furtherat lower action levels.
WaterThe Safe Drinkin- g Water Act Amendments of
1986 require EPA to develop regulations for toxicchemicals in water. The agency has decided toregulate radon like any other waterborne carcino-gen; it also considers radon to pose, quantita-tively, the greatest risk of cancer from water (table6-l). That regulatory process can be considered intwo time periods. Before the summer of 1992,EPA was developing the regulation under its
Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 157
usual procedures, but at that time Congressintervened in the process. Congress mandatedEPA to make a reassessment of its estimates ofrisks and costs in relation to radon in water. In itsaction, Congress reflected some opinions ex-pressed by EPA’s Science Advisory Board.
THE SCIENCE ADVISORY BOARD’S COMMENTSEPA’s Science Advisory Board weighed into
the radon in water issue in 1992. It w-rote a letterto the EPA Administrator:
. . . to convey its concern about the inconsistentapproach within the Agency regarding reducingrisks from radon exposures in homes. . . .
The purpose of this letter is two-fold: (a) toaddress the fragmented and inconsistent approachregarding reduction of radon risk, and (b) toprovide our closing comments on the revised
. .drinking water criteria documents that support theproposed regulations (Loehr et al., 1992).
The letter points out the proposed regulationwould reduce the concentration of radon in waterso that the amount that volatilizes from water toair would be more than 100 times smaller thanEPA’s action level (a voluntary guideline) of4 pCi/L for indoor air. It also notes that thatconcentration is well within normal variations inlevels of radon in homes, and about 10 timessmaller than the average concentration of radon inoutdoor air.
The SAB concluded that “Frankly, radon in. .
drinking water is a very small contributor to radonrisk except in rare cases and the Committeesuggests that the Agency focus its efforts onprimary rather than secondary sources of risk”(Loehr et al., 1992). The board also acknowl-edged that it understood that the SDWA requiredthe regulation of radon in water. But it returned toa theme developed in its 1990 report ReducingRisk (U.S. EPA, SAB, 1990) and urged EPA tobase its plans on “ongoing assessments ofremaining environmental risks, the explicit com-parison of those risks, and the analysis ofopportunities available for reducing risks, rather
Figure 6-2—Cost-Effectiveness of DifferentAction Levels for Reducing Indoor
Radon Exposures
vc—0 —-—- —r-——.. ~. ,.
0 4 8 12 16 20
Maximum exposure level (pCi/L)
I
24
SOURCE: Office of Technology Assessment, 1993.
than on past efforts at risk reduction or existingprogrammatic considerations. It went on to urgeEPA to conduct a multimedia risk assessment ofthe options for regulating radon in drinking waterand to include risks engendered by the treatmentprocess and the disposal of any wastes producedfrom it. The board recommended that EPAdevelop and present better treatments of uncer-tainty in the water criteria documents.
Several of the SAB’s recommendations, in-cluding the multimedia risk assessment, becamepart of the 1992 congressional mandate.
PUBLIC LAW 102-389 AND THE MULTIMEDIARADON RISK ASSESSMENT
Section 591 of the Housing and Urban Devel-opment, Veterans Administration, and Independ-ent Agencies Appropriations Bill of 1992 put ahold on EPA’s proposed regulation of radon inwater. That section, commonly called the Chaffee-Lautenberg Amendment after its senatorial spon-sors, directed EPA to complete a study July 6,1993, that considers “the risks from variouspathways of radon exposure-air and water,inhalation and ingestion. ” The study was also toexamine the costs of controlling various path-ways, detailing the costs to households andcommunities (including small communities), andany risks posed by disposing of materials used to

158 I Researching Health Risks
remove radon from water. The study was to bereviewed by EPA’s Science Advisory Board, andthe board was to submit its recommendations tothe EPA Administrator, who would then report toCongress. After completing the analyses andreviews, EPA was to issue regulations for radonin water by October 1, 1993.
Congress adopted the Chaffee-Lautenberg Amend-ment after the Senate narrowly defeated thebroader Domenici Amendment that would haveplaced an outright moratorium on EPA’s capacityto promulgate drinking water standards. Accord-ing to Senator Chaffee's discussion of the amend-ment:
The dispute here is about the relative risk ofradon in drinking water. And since the FederalGovernment does not require that any steps betaken to correct the principal source of the risk,namely the gas that comes from the soil, the
. .drinking water suppliers, quite rightfully, wonderwhy they should be required to clean up drinkingwater at a great expense. In other words, yes,some radon comes up with the drinking water, butmore of it comes from infiltration through base-ment walls, et cetera.
So there is much to be said for the line ofreasoning for those who object to the testing of itin water. Thus our amendment delays promulga-tion of the radon standard until the end of 1993.During the interim, the EPA is asked to providebetter data on the relative risk of radon fromvarious sources, from water, from cellars, and soforth. So we can revisit that next year in 1993,because this postponement goes to the end of1993 (Chaffee, 1992).
Given the time the amendment allotted for therisk assessment, EPA could do Little more thanreview the existing literature about radon risksand address specifically some uncertainties in itsrisk assessment. Although the conclusions fromthe reassessment were very close to those inEPA’s (1991) water criteria document for radonin water, the multimedia risk assessment (orreassessment) did not answer all the questionsraised by the SAB and by the amendment.
PROPOSED REGULATIONThe SDWA imposes a goal of zero for concen-
trations of carcinogens in water. That goal isunattainable for radon (extensive aeration ofradon-bearing water would discharge the radoninto the air but there would always be radon atleast at the concentration found in outside air).EPA bases its proposed regulation on its determi-nation that the lowest ‘‘practical quantificationlevel” for radon in water is 150 pCi/L, and it setthe regulatory maximum-contaminant level atthat value in its proposed rule in 1991 (U.S. EPA,1991). The half-life of radon is 4 days; that is, halfof the radon decays in 4 days. Because EPAallows up to 4 days for transporting the water tothe testing lab, the agency decided that a measure-ment of 300 pCi/L was the lowest feasible levelfor its regulation. Differences in procedures formeasuring radon in air and water account for thefact that airborne measurements of 2 pCi/L of airare routinely obtained while EPA contends thatmeasurements below 150 pCi/L in water are notpractical.
There is general agreement that 10,000 pCi/Lof radon in groundwater results in 1 pCi/L ofradon in air from volatilization (U.S. EPA, 1991).Therefore, the 300-pCi/L limit on radon in water,if imposed, would mean that no more than0.03 pCi/L of radon in indoor air would resultfrom the waterborne radon. That concentration is10 percent or less of the radon in outdoor air, andit would contribute about 5 percent to total indoorexposures. Supplying a house with water thatcontains 1,000 pCi/L of radon does not increasethe airborne radon content by 1 pCi/L becausewhen no water is running, there is little transfer ofradon from water to air. EPA has carefullyexamined such things as how much radon isreleased into the air from water during showering,laundering, and flushing the toilet in order toestimate the contribution of radon from water toindoor air.
The Natural Resources Defense Council (NRDC)and the Friends of the Earth (FOE) dispute EPA’sclaim that 150 pCi/L in water is the lowest

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 159
practical quantification level (Olson et al., 1991)0
They point to published studies that show thatchanges in sampling and methods of analysis forradioactivity can lower the detection level to25 pCi/L, which makes it possible to set astandard 12 times more stringent than the oneEPA proposed. EPA’s own analysis of amounts ofradon in water casts doubt on 150 pCi/L being theminimal detection level because it reports on thenumber of water systems that exceed 100 pCi/Land presents some information about those be-tween 50 and 100 pCi/L (U.S. EPA, 1991).
NRDC and FOE also point out that EPAcalculates that the cancer risk at the proposedregulatory limit of 300 pCi/L is 2 X 10-4. Not onlyis that risk level twice as high as the 10-4 level thatis EPA’s usual upper limit on acceptable risk; itis also much higher than the risks from otherwaterborne carcinogens, which are often in therange of 10-6.
Arguing from the viewpoint that concentra-tions of radon in water below 300 pCi/L can bemeasured, NRDC and FOE also claim thatimposing regulations on water supplies withconcentrations below 300 pCi/L would greatlyreduce exposures and risks at little additionalcost. In particular, they calculate that such aregulation could avert twice as many cancers foran increase in cost of between 28 and 40 percent.
Water suppliers also disagree with EPA’sproposed standard. They question whether therisk assessment is accurate and whether theproposed standard will save 80 deaths annually asEPA calculates; they also draw attention to theestimate that about 90 percent of the risk of lungcancer risk is confined to smokers. Like NRDCand FOE, but for very different reasons and byreaching very different conclusions, water suppli-ers draw attention to the fact that the proposed
standard is based on a measurement level. Im-provements in the capacity to measure radon inwater (which NRDC and FOE contend are alreadyhere) could be translated into a constantly shift-ing, and constantly decreasing, standard. Thatkind of situation would leave the water suppliersfacing an uncertain future of tighter standards andhigher costs.
RISKIn 1991, EPA (1991) estimated that current
concentrations of radon in water were associatedwith about 200 deaths annually from cancer, andthe agency estimated that lowering all watersupplies that were then higher than 300 pCi/L to300 pCi/L would avert about 80 cancer deaths. Atthat time, EPA associated 80 percent of the riskfrom waterborne radon with radon that volatilizedfrom water and was inhaled. Because of aNational Research Council (1991) study that saidcertain adjustments were necessary to allow fordifferences between radon exposures in minesand in homes, EPA, in its reassessment, reducedits estimate of the number of cancer deathsassociated with volatilized radon. At the sametime, it increased its estimate of the number ofdeaths from cancer expected to result fromingested radon. When EPA (1993) added to-gether the number of deaths from cancer thatit associates with inhalation and ingestion ofradon from water, the total came to about 160annually, a number not different from theapproximately 200 deaths from cancer that itpreviously associated with inhaled radon fromwater.3
EPA predicts ingested radon will cause cancerof the stomach and other digestive system organs.However, unlike other estimates of radon risk, therisk from ingested radon is not based on directevidence of adverse effects in miners or other
s EPA calculates precise point estimates for risks along with a range of possible risks, For example, its estimate for annual deaths fromingested radon is 46, with a range of 11 to 212. Such precision is unwarranted because of uncertainties in measurement and models, and OTAprefers to present EPA results in less precise terms, such as ‘about 50.’ More importantly, the calculated range is not the same as the uncertaintythat surrounds the estimate. As the Science Advisory Board noted (behr and McClellan, 1993), the uncertainty of the risk from ingested radonis so great that them may be zero risk.

160 I Researching Health Risks
populations. Indeed, there is no evidence forincreases of those cancers in miners. Moreover,according to the Agency for Toxic Substancesand Disease Registry (1992), there is no evidencefor an association between groundwater radonand gastrointestinal cancers or leukemias. EPAbases its estimates of risk for ingested radon onmodeling of the distribution of xenon gas in thehuman body and on the observed increase ofstomach and other digestive system cancers insurvivors of atomic bomb blasts. The modeling,which is the basis for estimating doses of internalradiation from ingested radon, is taken from apaper that has not been peer-reviewed. And,although both radon and atomic bombs releaseradiation, they release different kinds of radiation—alpha particles are released from radon, andgamma rays and neutrons from atomic bombs.Moreover, the two sources deliver radiation quitedifferently: ingested radon is a long-term internalexposure, and atomic bombs produced an exter-nal, one-time exposure. Those differences pointto the problems involved in estimating the riskfrom ingested radon.
The upward revision of the number ofdeaths expected from ingested radon elicitedseveral negative comments. In particular, Harleyand Robbins (1993) estimated that the exposureof the stomach to radiation from ingested radon isabout 100 times less than did EPA. EPA scien-tists defended their process (Chiu, Puskin, andBarry, 1993), but Crawford-Brown (1993), theauthor of the paper on which EPA depends for itsestimate of radiation exposure to the stomach,agrees with Harley and Robbins that the estimateof exposure may be too high.
More fundamentally, Crawford-Brown (1993)objects to EPA’s assuming that the mathematicalequation it used to extrapolate risk is correct: "Ibelieve the USEPA is both philosophically andscientifically far from the mark in suggestingthat uncertainties in extrapolation equationsare to be characterized . . . (as if) . . . there is nouncertainty in these equations . . . ." Thiscomment questions the risk assessment based on
miner data that EPA has used to estimate thecancer risks from radon in water. Some scientistswithin EPA have made parallel comments aboutthe uncertainties in the dose-response equationthat is used in EPA’s risk assessment (Ulsamer,1993).
Scientists at Brookhaven National Laboratory(BNL) responded to a request from EPA’s Officeof Research and Development that the Depart-ment of Energy (DOE) review EPA’s risk assess-ment of radon in water. The resulting review wassent from DOE to EPA accompanied by a letter(Pelletier, 1993) that summarized the DOE posi-tion: “BNL concludes that the draft reportcontains significant flaws which seriously detractfrom its usefulness. ” The review itself is quitecritical of EPA’s risk analysis (Morris, Rowe, andBaxter, 1993). The BNL scientists agree withCrawford-Brown (1993) that EPA may haveoverestimated exposures from ingested radon bya factor of 100, and they point to a number ofcomputational errors that they found in the EPAreport. The EPA scientists who developed the riskassessment profoundly disagreed with the DOEreview (Chiu, Puskin, and Barry, 1993) andresponded to its summary comments.
In its review of the reassessment, EPA’sScience Advisory Board was quite critical of themethods used to estimate cancer rates fromingested radon. It characterized the methods asmore indirect than those used to estimate risksfrom airborne radon and concluded: “In theabsence of direct evidence, it is not possible toexclude the possibility of zero risk from ingestedradon” (Loehr and McClellan, 1993). As it did in1992, the SAB drew attention to the small riskassociated with radon in water as compared to theoverall risks from radon. The SAB also, as in1992, made comparisons between the number ofdeaths that might be associated with waterborneradon (about 160) and the 2,500 deaths that areexpected to occur annually from radioactivepotassium that occurs in the human body and the500 or so expected from outdoor radon.

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 161
COSTSThe three parties-EPA, NRDC, and FOE, and
the water suppliers-also disagree about ex-pected costs. In 1991, EPA estimated that thecosts to reduce radon to 300 pCi/L in all 25,907water supplies that exceeded that level would be$1.6 billion in capital costs and $0.18 billion inannualized costs (U.S. EPA, 1991). The cost ofaverting a case of radon-associated cancer wasestimated at $2.3 million. In February 1993, EPAincreased those estimates. Currently, its bestestimate is that 41,000 water supplies exceed300 pCi/L and that the best estimates for capitaland annualized costs are $1.8 billion and$0.26 billion, respectively (U.S. EPA, 1993a).
NRDC and FOE accept EPA’s cost estimatesfor reducing concentrations to 300 pCi/L and usethe agency’s estimates to project the additionalcost of reducing radon in water to lower levels(Olson et al., 1991). EPA’s proposed regulationwould reduce current levels by 80 percent.NRDC and FOE contend that reducing levelsto 1 percent of current levels, which mightdouble the expected health benefits, would costonly an additional 28 to 40 percent, and in fact,the greater reductions might be achieved ateven smaller cost increments. (Experts whowork for water suppliers have said that theywould expect costs to fall as more efficientaeration systems are developed to remove radonfrom water.)
The SAB (U.S. EPA, SAB 1993) did notendorse EPA’s proposal for wholesale adoptionof aeration to reduce radon concentrations inwater. EPA had considered and rejected granu-lated activated charcoal (GAC) as a controlmeasure, in part because of the problems raised bydisposing of the radioactive charcoal after its use.The SAB urged the agency to look again at GACbecause of its potential to hold down costs ascompared to the costs of aeration in someapplications. The Board made no projections ofthe costs. The board also urged EPA to revisit itsestimates of costs for water supplies of differentsizes and to consult with the water suppliers to
obtain more information. Whether aeration orGAC is used to remove radon, either techniqueallows the introduction of microbes into watersupplies, and SAB (U.S. EPA, SAB 1993) cau-tions that “costs of disinfection, especially insmall systems, needs to be reviewed thoroughly.
The Association of California Water Agenciescommissioned an engineering study of the costsof bringing public water suppliers in Californiainto compliance with the 300-pCi/L standard(Fensterheim, 1992). According to the associa-tion, the capital costs to bring 9,420 Californiawells into compliance would be $3.73 billion; theannualized costs would be $0.7 billion. Accord-ing to one projection from the associationsresults, total national capital costs are expected ofbetween $12 and $20 billion; those expendituresare expected to reduce total radon exposures byabout 1 percent (Abelson, 1993).
The SAB (U.S. EPA, SAB 1993) comparesEPA’s estimate of $3.2 million to avert a deathfrom lung cancer from waterborne radon to theEPA estimate that remediation to reduce airborneradon to 4 pCi/L will avert a death for about$700,000. The Association of California WaterAgencies calculates much higher costs; it esti-mates that the cost to avert a death from radon-associated lung cancer would range between $65and $87 million in California. The cost to avert adeath from lung cancer in a nonsmoker in thatState would be between $433 and $592 million.(The much higher cost for averting the deaths ofnonsmokers results from the fact that lung canceris so much rarer among them.)
Part of the reason for the California Associa-tion’s much higher cost estimate is its survey thatshows many more water supplies exceed theproposed 300-pCi/L regulatory limit than isestimated by EPA. The SAB (Loehr and McClel-lan, 1993) also points to uncertainty in theestimates of how many water supplies would besubject to regulation (’‘may seriously underesti-mate the number of community water systemsimpacted . . . “) and states that “this uncertainty

162 I Researching Health Risks
in exposure estimates ultimately impacts the costsof mitigation.
EPA has estimated that the average annual costfor radon reduction for houses served by thesmallest water utilities would be $120; mosthouses are served by larger systems and wouldpay about $50 per year (Wilcher, 1991). Based onAssociation of California Water Agencies esti-mates, former Senator William E. Dannemeyerwrote to EPA that every household that has to payfor radon reduction would pay an extra $340 peryear (Dannemeyer, 1991). The town of Hastings,Nebraska, has a population of 23,000 and waterthat exceeds EPA’s proposed limit for radon inwater. According to an analysis that the town con-ducted, a water treatment plant to remove theradon would cost $65 million and be the singlelargest drain on the town’s treasury (Schneider,1993).
NRDC and FOE do not accept that small watersuppliers will bear sizable new costs as a result ofsetting a standard of 300 pCi/L or lower for radonin water (Olson et al., 1991). They argue thatsmaller suppliers could tie into larger suppliers togain economies of scale or look for water thatcontains less radioactivity. Moreover, Olson et al.(1991) cite experts who state that technologies areavailable that are much less costly than those EPAconsidered in its 1991 cost estimates. In EPA’s1993 recalculation of estimated costs, total capitalcosts increased by 20 percent and annual costsincreased by 44 percent, whereas the number ofwater suppliers increased by 60 percent, indicat-ing that EPA had found some savings in costs persupplier.
The costs of the proposed regulation on radonin water regulation can also be compared with thecosts of a public health measure that has becomemore expensive in recent years and that hasproduced public outcries for reducing the profitsof pharmaceutical companies. The cost of child-hood immunizations has increased from between$7 and $23 in 1982 to between $129 and $244 in1992 (Orenstein, 1993). Even so, the annual costof the radon-in-water regulation-estimated by
EPA to be about $50 per family served byaveraged-sized systems and $120 per familyserved by small systems-ranges from between afifth to a little less than half the one-time cost ofimmunization. The estimate of the Association ofCalifornia’s Water Agencies of $340 per familyper year for the radon-in-water regulation exceedsthe one-time cost of immunization.
The continuing, annual estimated family costof the regulation, which will affect about 1percent of all exposures to radon, of between $50and $340 can also be compared with EPA’sestimate of the one-time cost of bringing indoorradon concentrations down to 4 pCi/L or lower.EPA (1992a) estimates for the one-time cost forremediation of a house ranges from $500 to$2,500 with an average of $1,200 and averageoperating expenses of $68.
SCIENCE ADVISORY BOARD COMMENTS,JULY 1993
The Science Advisory Board review gave EPAhigh marks for its general approach to themultimedia risk assessment, but it focused onareas such as estimates of the population exposedto concentrations of radon greater than 300 pCi/Lin water, calculated risks from ingested radon,and capital cost estimates in which it thought theagency could make efforts to refine its approachesand calculations. A letter from the chair of theSAB Executive Committee and the chair of theSAB Chafee-Lautenberg Study Review Commit-tee (Loehr and McClellan, 1993) returned to theBoard’s 1992 position that EPA should applyrelative risk approaches in its consideration ofrisks from radon. The relative risk approach‘‘caLls for giving the highest priority to mitigatingthe largest sources of risks first, especially whenthe cost-effectiveness of risk reduction of suchsources is high. ’
As part of that approach, Loehr and McClellan(1993) encourage EPA to continue its efforts “toencourage voluntary actions to reduce indoor airradon in view of the cost effectiveness of thisapproach for reducing risks. ” About radon in

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 163
water, they conclude that the proposed regulatorylimit of 300 pCi/L is “the most costly in terms ofcosts per cancer death avoided. ” They suggestthat EPA also consider setting limits for radon inwater at either 1,000 or 3,000 pCi/L. Even thehigher numbers would result in water contribut-ing no more radon to indoor air than is present inoutdoor air.
Nero (1993) has also suggested alternatives tothe 300-pCi/L limit on radon in water. Like theSAB, he suggests setting the water limit so thatradon from water would make no more of acontribution to indoor air than does the radon inoutside air, which would be in the range of 1,000to 3,000 pCi/L in water. An EPA official alsoreported to a newspaper that agency staff wereforwarding at least three options for a radon-in-water rule to the EPA Administrator: 300, 1,000,and 2,000 pCi/L (Anon, 1993 b).
Should a limit of 1,000 to 3,000 pCi/L in waterbe set, EPA could continue to accumulate infor-mation about the levels of radon in water, thenumber of water supplies with various concentra-tions, and the risks from ingestion of radon. Theadditional information would reduce the uncer-tainties in the estimates of risks, costs, and costper life saved, and pave the way for alterations inthe regulation if needed.
“Inconsistency” in EPA’sApproach to Radon
The letter that requested this OTA examinationof indoor radon cited the SAB 1992 concernsabout inconsistencies in EPA’s approach to re-ducing risks from radon. It contrasted the goals ofthe IRAA both with EPA’s action level for indoorradon and with its proposed level for regulatingradon in water under the SDWA: The IRAA goalis to bring indoor radon level down to thosecommonly found outdoors (0.1 to 0.5 pCi/L),whereas EPA urges that remediation be under-taken to reduce concentrations of radon in homesto 4 pCi/L or lower. In contrast, EPA’s proposedregulation would set 300 pCi/L of radon in
. .drinking water as the highest permitted level,limiting radon in indoor air to 0.03 pCi/L fromthis source (given the assumption that 10,000pCi/L of radon in water produces 1 pCi/L of radonin air because of volitalization). Clearly, the goal,the action level, and the proposed regulation setdifferent exposures as acceptable (box 6-A).
These inconsistencies are no surprise given theway that the goal, the action level, and theregulation were derived. Congress, in the IRAA,acknowledged that the outdoor level of radon inair is unavoidable and that concentrations cannotbe reduced below that level. At the same time,reducing concentrations to that level would be ashealth protective as possible.
EPA, in setting the 4-pCi/L action level,accepts a risk of cancer from radon that is farhigher than the 1 X 10_6 (one excess cancer permillion people) exposed for a lifetime that theagency routinely uses as a goal in regulatingexposures to toxic chemicals. The Citizen’s Guideto Radon (U.S. EPA and U.S. DHHS, 1992)provides some examples of comparative risk; forinstance, the risk that a nonsmoker bears fromconstant exposure to radon at 4 pCi/L is roughlythe same as that person’s risk of drowning.
The proposed radon-in-water standard underthe SDWA is risk- and measurement-based. Thelevel of 300 pCi/L of radon in water, set at whatEPA had determined is the practical limit onquantification, was projected to reduce risks toabout 2 X IN. In its preamble to the proposedrule, EPA raised the question of the significanceof waterborne radon to the total radon issue: ‘‘Inevaluating the various alternatives for proposinga radon MCL [maximum contaminant level; theregulatory standard], EPA considered the criticalpolicy questions of whether radon in water shouldbe regulated like other drinking water contami-nants, or whether it should be regulated more inaccord with its importance compared to overallradon exposure. EPA decided to regulate radonas other waterborne contaminants, and the SAB(Loehr et al., 1992) criticized that action because

164 I Researching Health Risks
of the small contribution that waterborne radonmakes to overall exposure to radon.
Congress’s mandating of the multimedia riskassessment produced some refinements in EPA’srisk and cost assessment, but whether it will makea difference in regulation remains to be seen. Therisk estimate hardly changed at all, and, accord-ing to EPA% assessment, radon in waterremains associated with a risk greater than10-4, which is the usual upper limit on the riskthat EPA finds tolerable.
Indoor AirRisks to health from contaminants in indoor
air-lead paint, asbestos in buildings, environ-mental tobacco smoke (ETS), and other sub-stances—have spotlighted the indoor environ-ment as a source of hazards. In the 102d Congress,Representative Joseph Kennedy and SenatorGeorge Mitchell introduced the Indoor Air Qual-ity Act of 1991 in the House and Senate,respectively (H.R. 1066 and S. 455). Had eitherbill passed, it would have authorized research,development, and demonstration projects con-cerned with improving air quality; the House billwould have imposed some regulations. BothKennedy and Mitchell have introduced bills in the103d Congress that focus on research and devel-opment.
The contents of the bills demonstrate thecomplexity of the issues arising in legislationregarding the quality of indoor air. In addition tothe agents mentioned above, indoor air cancontain hazardous chemicals that are carriedhome in clothes and on the skin from theworkplace; any number of volatile organic com-pounds from common household chemicals suchas paints and soaps; and allergens that arise frompets, insects, molds, and mildews. The billsaddressed indoor air quality in homes, which areprobably the setting that is most often consideredwhen thinking about indoor air, but they alsotreated air in educational facilities and commer-cial and Federal buildings. Clearly, legislation
dealing with indoor air would apply to manysubstances and various kinds of buildings.
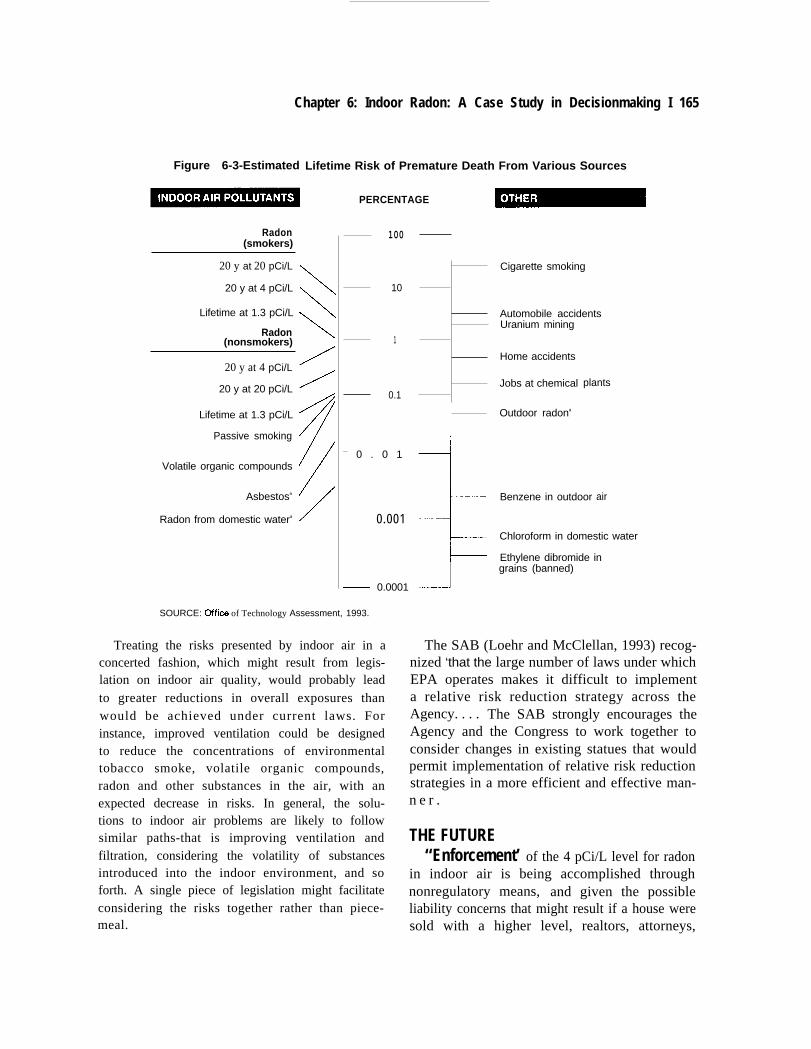
A decade ago, Spengler and Sexton (1983)discussed the special problems of indoor airpollution; more recently, Nero (1992) has arguedthat indoor air problems merit approaches differ-ent from other environmental issues. As shown onfigure 6-3, risks from substances in indoor air fallover a wide range, with the radon-related risk ofdeath for smokers as high as 8 percent and the riskfrom waterborne radon about 0.006 percent (morethan 1,000 times lower). [Because of computa-tional differences, figure 6-3 shows that the riskof death from waterborne radon is less that 0.01percent, which is less than the approximately 0.02percent (2 X l@) risk that EPA associates withwaterborne radon.] The highest risk shown on thefigure is for smoking, which increases the risk ofpremature death by about 25 percent. Accidentsand certain occupations are associated with levelsof risk around the level associated with radon.
EPA has concluded that the risks associatedwith indoor radon are greater than any other thatit contends with (with the exception of risks ofcancer posed by sunlight). The agency thus arguesthat indoor radon and waterborne radon requireimmediate attention. Nero (1993) counters thatthe risks from indoor radon are not put in theproper context when compared with outdoorrisks. Instead, he maintains that indoor radonshould be considered in the context of indoor risksthat are typically higher than outdoor risks.
Considering the risks posed by indoor radon inthe context of indoor risks would create monu-mental obstacles to setting the SDWA’s limit of10-4 (0.01 percent) on cancer risks as a consistentgoal for risk reduction. As shown in figure 6-3,many indoor risks are far above the proposedregulatory limit for radon in water. It is veryunlikely that the risks from radon in indoor air canbe lowered from the nearly 1 percent associatedwith the average concentration in U.S. homes of1.3 pCi/L or that the risk of fatal home accidentscan be lowered from about 0.8 to 0.01 percent.
Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 165
Figure 6-3-Estimated
Radon(smokers)
20 y at 20 pCi/L
20 y at 4 pCi/L
Lifetime at 1.3 pCi/L
Radon(nonsmokers)
20 y at 4 pCi/L
20 y at 20 pCi/L
Lifetime at 1.3 pCi/L
Passive smoking
Volatile organic compounds
Asbestosa
Radon from domestic watera
Lifetime Risk of Premature Death From Various Sources
\
\
\
/
/
/
f
/
/
PERCENTAGE
100
10
1
0.1
— 0 . 0 1
— 0.001
— 0.0001J
Cigarette smoking
Automobile accidentsUranium mining
Home accidents
Jobs at chemical
Outdoor radona
plants
Benzene in outdoor air
Chloroform in domestic water
Ethylene dibromide ingrains (banned)
SOURCE: Offics of Technology Assessment, 1993.
Treating the risks presented by indoor air in aconcerted fashion, which might result from legis-lation on indoor air quality, would probably leadto greater reductions in overall exposures thanwould be achieved under current laws. Forinstance, improved ventilation could be designedto reduce the concentrations of environmentaltobacco smoke, volatile organic compounds,radon and other substances in the air, with anexpected decrease in risks. In general, the solu-tions to indoor air problems are likely to followsimilar paths-that is improving ventilation andfiltration, considering the volatility of substancesintroduced into the indoor environment, and soforth. A single piece of legislation might facilitateconsidering the risks together rather than piece-meal.
The SAB (Loehr and McClellan, 1993) recog-nized ‘that the large number of laws under whichEPA operates makes it difficult to implementa relative risk reduction strategy across theAgency. . . . The SAB strongly encourages theAgency and the Congress to work together toconsider changes in existing statues that wouldpermit implementation of relative risk reductionstrategies in a more efficient and effective man-n e r .
THE FUTURE‘‘Enforcement’ of the 4 pCi/L level for radon
in indoor air is being accomplished throughnonregulatory means, and given the possibleliability concerns that might result if a house weresold with a higher level, realtors, attorneys,

166 I Researching Health Risks
buyers, and sellers probably will not alter theirpractices even if research findings show that risksat that level are smaller than is now believed. Onthe other hand, an increase in the estimate of riskwould probably be quickly reflected in real estatetransactions because of reasons of liability.
EPA’s proposed regulation of radon has beendelayed beyond October 1, 1993. The Agency is,reportedly, still deciding on its response to theScience Advisory Board’s comments on its multi-media risk assessment. It is expected that work onthe proposed regulation will follow that response.The regulation may be delayed for 1 year byCongress, if an amendment passed by the Senateis also approved by the House. Whenever EPAwrites the regulation, the Science Advisory Boardhas offered alternatives to its proposed limit of300 pCi/L radon in water. It is possible that theagency could set a higher limit that would, ineffect, apply only to water systems that contributea significant fraction of overall radon exposures.Setting a limit higher than 300 pCi/L would beexpected to engender lawsuits from citizens andorganizations concerned about risks from water-borne radon.
In contrast, if NRDC’s and FOE’s petition toset a stricter standard were successful, it wouldrequire that EPA reduce concentrations of water-borne radon, tightening the standard. Alterna-tively, Congress could relieve EPA of the respon-sibility for regulating radon in water, or shift itfrom the SDWA to the IRAA, or enact a new lawon indoor air. Any shift might result in a standarddifferent from 300 pCi/L.
No regulatory agenda requires a new studyabout the level of risk presented by indoor radon.The current risk assessment, based on theminer studies, is sufficient for regulatory ac-tion and indeed, being based on studies ofhumans, is more certain than animal-basedrisk assessments that form the basis for manyregulations. Nevertheless, a convincing studyof the risks associated with indoor radonwould provide a great deal of information aswell as a technical foundation for future policy
decisions. A study that answered the question ofwhether the risks predicted from the minersstudies were accurate would do more than informthe radon debate. It would also provide the firsttest of the accuracy of any extrapolated estimateof an environmental risk. Moreover, because itwould provide more certain information aboutrisks from radon in air at low levels, it wouldreduce the uncertainty of the risk assessment forradon in water because the major part of that riskis associated with inhalation.
Such a study would make a real contribution toscientific understanding and, depending on whatit reveals, could have different effects on debatesabout regulatory levels. If the study revealed thatthe current levels were about right, it wouldconfirm the appropriateness of the methods usedto generate current risk estimates. If the studyshowed that current risk estimates were too low,EPA could tighten up the regulations. If, however,the results of the study indicated that the riskswere lower than are now estimated, EPA might beconfronted with the problem of backing off onsome of its regulations and guidelines.
Doll (1992) is confident that studies now beingperformed will produce valid data about relation-ships between indoor radon and cancer within thenext few years. In anticipation of the completionof those studies, both EPA and DOE are planningto carry out meta-analyses of the findings fromthose studies. Yet, despite Doll’s optimism, thereis no guarantee that the ongoing studies willproduce a clear-cut answer about cancer risksfrom indoor radon. In that case, the governmentcould assemble a group of experts to decidewhether it is possible to design such a study, anddesign it, if it is feasible. A study of that kindwould probably have to be larger than any doneto date, and it would have to be carried out in areas(such as Missouri and Iowa) in which radonexposures are higher than average. To havescientific and political credibility, the studywould have to be planned in an open process withexplicit discussions of what results would beexpected under different planning assumptions.

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 167
Furthermore, the planning would have to deter-mine the study’s chances of resolving the issue. Ifthe chances were low, policymakers could decidenot to go ahead with the study. Still anothernonconvincing, nonconclusive study would notjustify the expenditure of resources necessary forits completion.
At quite a different level of research, studies ofmolecular mechanisms of radon-caused carcino-genesis and of movements of radon in buildings(for examples, see DOE, 1993) and of carcino-genesis in general (see chs. 3 and 4) may providemore information about risks from radon. Scien-tists can design epidemiologic studies and decide,in advance of doing them, whether the studieshave sufficient power to answer questions impor-tant for policymaking and how long the studieswill take---certainly they will take years. But,advances in molecular studies, which may pro-vide better estimates of exposure, pre-diseaseconditions, or mechanisms of action, cannot beput on a timetable. They may come in months, orthey may take years.
The specific questions raised by radon maybeanswered by congressional or EPA decisions thatimpose new regulations or that leave the currentapproaches intact. New epidemiologic resultsmay inform those decisions by revealing morecertain evidence of the level of risk posed byradon at environmental levels. And it is possiblethat research into mechanisms of carcinogenesismay shed some light on such risks. More gener-ally, radon is a case that illustrates the difficultiesposed by an environmental risk of uncertain sizethat reaches human beings through differentmedia.
As of mid-October 1993, Senator Baucus hadintroduced a bill that would direct EPA toregulate radon in water by a method differentfrom that now being considered. In addition,Senator Chaffee was considering introduction oflegislation as was Representative Slattery. Thislegislative action indicates that policy on radon inwater may well be set by legislative modificationsto the SDWA.
CHAPTER 6 REFERENCESAbelson, P.H. 1993, Regulatory costs (editorial).Science 259:159.
Agency for Toxic Substances and Disease Registry.1992. ATSDR Case Studies in Environmental Medi-cine; 14, Radon Toxicity. Atlanta, GA: U.S. Depart-ment of Health and Human Services, p. 9.
Alavanja, M. C. R., Brownson, R., Wood, M. et al.1992. Radon dosimetry for a lung cancer study inMissouri. In: F.T Cross (cd.) Indoor Radon and LungCancer: Reality or Myth. Columbus, OH; Richland,WA: Battelle Press, pp. 871-887.
Anon. 1993a. No radon-leukemia link [a description ofa study published in Lancet], Environmental HeaZth&tter. Apr. 16, p. 72.
Anon. 1993b. Final rule to control radionuclides willbe issued by October, Environrnenta.l protection Agencysays, Daily Report for Executives (Washington, DC:Bureau of National Affairs), June 3, p. A-6.
Blot, W.J,, Xu, Z-Y., Boice, J, D., Jr. et al. 1990. Indoorradon and lung cancer in China. Journal of theNational Cancer Institute 82: 1025-1030.
Bodans@, D. 1990. Radon induced lung cancer andmortality. In: S.K. Majumdar, R.F. Schrnalz, and E.W.Miller (eds.) Environmental Radon: Occurrence, Con-troZ and Health Hazards (Phillipsburg, NJ: Typehouseof Easton).
Brill, D.R. 1990. Radon and health. In: S.K. Majum-dar, R.F. Schmalz, and E.W. Miller (eds.) Environ-mental Radon: Occurrence, Control, and HealthHazards (Phillipsburg, NJ: Typehouse of Easton,1990).
Brownson, R. C., Alavanja, M. C. R., Hock. T.T. et al.1992. Passive smoking and lung cancer in nonsmokingwomen. American Journal of Public Health 82:1525-1530.
Chaffee, J. 1992. Remarks. Congressional Record138:13033, Sept. 9.
Chiu, N., Puskin, J., and Barry, T. 1993. Response toS.C. Morris, M.D. Rowe, S.J. Baxter on their com-ments on EPA draft Jan. 29, ‘‘Uncertainty Analysis ofRisks Associated with Exposure to Radon in DrinkingWater. ” Photocopied memo. May 3.

168 I Researching Health Risks
Cohen, B.L. 1990. Experimental tests of the linear-nothreshold thmry of radiation carcinogenesis. In: C.R.Cothern and P.A. Rebers (eds.) 1990. Racibn, Radiumand Uranium in Drinking Water. Cheka, Ml LewisPublishers, pp. 69-82.
Cohen, B.L. 1992. Multi-stratified multiple regressiontests of the linear/ncxthreshold theory of radon-induced lung cancer. In: F.T. Cross (cd.) ]nakxw Radbnand Lung Cancer: Reali~ or Myth? Columbus, OH;Richland, WA: Battelle Press, pp. 959-975.
Crawford-Brown, D.J. 1993. Utter to GenevieveMatanoski, chairman of the EPA Science AdvisoryBoard Committee on Radon. Mar. 27.
Damemeyer, W.E. 1991. U.S. Senator. Letter to theHonorable William E. Reilly, Administrator, U.S.Environmental Protection Agency. November 14.
Dickersin, K., and Berlin, J.A. 1992. Meta-analysis:State-of-the-science. Epi&miologic Reviews 14:154-176.
Doll, R. 1992. Risks from radon. Radiation ProtectionDosimetry 42:149-153.
Fensterheim, R.J. 1992. Demands to regulate radon indrinking water in an environment of evolving riskestimates. Paper presented at Annual Meeting of theAmerican Association for the Advancement of Sci-ence, Chicago, Feb. 11.
Hanson, D.J. 1989. Radon tagged as cancer hazard bymost studies. Chemical Engineering News 67:7-13.
Harley, N. H., and Robbins, E.S. 1993. A biogeneticmodel for the distribution of ‘% gas in the bodyfollowing ingestion. Submitted to the Science Advi-sory Board, Environmental Protection Agency, Mar.17.
Henshaw, D. L., Eatough, J.P., and Richardson, R.B.1990. Radon as a causative factor in induction ofmyeloid leukemia and other cancers. The Lancet335:1008-1012.
Henshaw, D.L., Eatough, J.P., and Richardson, R.B.1992. Is radon a causative factor in inducing myeloidleukemia and other cancers in adults and children? In:F.T. Cross (cd.) Indoor Radon and Lung Cancer:Reality or Myth? Columbus, OH; Richland, WA:Battelle Press, pp. 935-958.
htoumeau, E. G., Krewski, D., and Choi, J. 1993. Acase-control study of residential radon and lung cancer
in Winnipeg, Manitoba. In press, American JournaZ ofEpidemiology.
Lo&r, R.C., Nygaard, O.F., and Voilleque, P.G. 1992.Letter to W.M. Reilly, Administrator. U.S. Emiron-mental Protection Agency. Subject: Reducing Risksfrom Radon: Drinkm“ g Water Criteria Documents. Jan.29.
Loehr, R. C., and McClellan, R.O. 1993. Letter toHonorable Carol M. Browner, Administrator, U.S.Environmental Protection Agency. Re: SAB Reviewof Multimedia Risk and Cost Assessment of Radon in
. .Drmkmg Water. July 30.
Lubin, J.H., Sarnet, J. M., and Weinberg, C. 1990.Design issues in epidemiologic studies of indoorexposure to radon and lung cancer. Health Physics59:8070817.Lubin, J.H., Lang, Z., Hrubec, Z. et al. 1993. Radonexposure in residences and lung cancer among women:Combined analysis of three studies. Cancer Cause andControZ (in press).
Lynch, C. 1993. University of Iowa, Iowa City. 1993.Personal communication.
Miller, D., Morrison, H., Semenciw, R. et al. 1993.Leukemia and residential exposure to radon. CanadianJournal of Public Health (in press).
Moeller, D.W. 1989. Controlling levels of airborneradon. Forum for Applied Research Public Policy4:5-11.
Morris, S. C., Rowe, M.D., and Baxter, S.L. 1993.Comments on EPA draft Jan. 29, 1993, “UncertaintyAnalysis of Risks Associated with Exposure to Radonin Drinkul“ g Water. ” Photocopied typescript.
Nazaroff, W. W., and Teichman, K. 1990. IndoorRadon. Environmental Science and Technology 34:774-782.
Nero, A.V., Jr. Lawrence Berkeley Laboratory. 1990.Letter to M.L. Oge, U.S. Environmental ProtectionAgency, Sept. 20.
Nero, A.V., Jr. 1992. A national strategy for indoorradon. Issues in Science and Technology IX:334.Nero, A. V., Jr. 1993. Developing a conceptual fiarne-work for evaluating environmental risks and controlstrategies: The case of indoor air. Paper presented atthe meeting Indoor Air 1993. Helsinki, FinlanL July4-8.

Chapter 6: Indoor Radon: A Case Study in Decisionmaking I 169
NRC (National Research Council). 1983. Risk Assess-ment in the Federal Government: Managing theProcess. Washington, DC: National Academy Press.
NRC. 1988. Health Risks of Radon and other Inter-nally Deposited Alpha-Emitters. BEIR IV (Washing-ton, DC: National Academy Press),
NRC. 1991. Comparative Dosimetry in Mines andHomes. Washington, DC: National Academy Press.
Olkin, I. 1992. Reconcilable differences. The Sciences,July/August, pp. 30-36.
Olson, E.E., Guth, J., and Hu, D. 1991. Comments ofthe Natural Resources Defense Council and theFriends of the Earth on EPA’s Proposed National* D*g Water Regulations for Radionu-elides. photocopied typescript. Nov. 15 (correctedNOV. 25, 1991).
Orenstein, W.A. 1993. Director of Immunization.Centers for Disease Control and Prevention. Quoted inR. Pear, 1993. Clinton considers plan to vaccinate allU.S. children. New York Times, Feb. 1, pp. Al andA16.
Pelletier, R,F. 1993. Mter to Peter W. Preuss, Of13ceof Science, Plaming and Regulatory Evaluation, U.S.Environmental Protection Agency. Apr. 22.
Pete, J, 1990. Radon and the risk of cancer. Nature345:389-390.
Ruosteenoja, E. 1991. Indoor radon and risk of lungcancer: An epidemiological study in Finland. FinnishCentre for Radiation and Nuclear Safety: Helsinki.
Samet, J.M. 1989. Review: Radon and Lung Cancer.Journal of the National Cancer Institute 81 ;745-757.
Schneider, K. 1993. How a rebellion over environ-mental rules grew from a patch of weeds. New YorkTimes, Mar. 24, p. A16.
Schoenberg, J. B., Klotz, J. B., Wilcox, H.B. et al. 1990.Case-control study of residential radon and lung canceramong New Jersey women. Cancer Research 50:6520-6524.
Society for Risk Analysis. 1993. Panel Report on theUse of Meta-Analysis in the Assessment of HumanData for Cancer Risk Assessment. Photocopied type-script.
Spengler, J. D., and Sexton, K. 1983. Indoor airpollution: A pubhc health perspective. Science 221:9-17.
Svensson, C., Pershagen, G., and Klorninek, J. 1989.Lung cancer in women and type of dwelling in relationto radon exposure. Cancer Research 49:1861-1865.
Taylor, R. 1990. Facts on Radon and Asbestos. NewYork: Franklin Watts,
U.S. Congress, OTA (Office of Technology Assess-ment). 1981. Assessment of Technologies for Deter-mining Cancer Risks From the Environment. OTA-H-138. Washington, DC: U.S. Government PrintingOffice, June 1981.
U.S. DOE (Department of Energy). 1993. RadonResearch Program, Fiscal Year 1992. DOE/ER-0588.Washington, DC: U.S. Department of Energy.
U.S. DHHS (Department of Health and HumanSemices). 1991. National Toxicology Program. SixthAnnual Report on Carcinogens. Summary. Rockville,MD: Technical Resources, Inc., 1991.
U.S. EPA (Environmental Protection Agency) andU.S. DHHS (Department of Health and HumanSemices). 1992. A Citizen’s Guide to Radon (2d cd.).EPA/ANR44. Washington, DC: Environmental Pro-tection Agency.
U.S. EPA (Environmental Protection Agency). 1986.A Citizen’s Guide to Radon: What Is It and What DoesIt Do? Washington, DC: Environmental ProtectionAgency.
U.S. EPA. 1987. Unfinished Business: A ComparativeAssessment of Environmental Problems: Appendix I.Cancer Risk Work Group. Washington, DC: Erwiron-mental Protection Agency.
U.S. EPA. 1991. National primary drinking waterregulations; radionuclides. Fed2ra/ Register 56:33050-33127.
U.S. EPA. 1992b. Technical Support Document forthe 1992 Citizen’s Guide to Radon. EPA 400-R-92-011.
US. EPA. 1992a. National Residential Radon Survey:Summary Report. EPA 402-R-92-01 1.
U.S. EPA. 1993a. Draft national cost estimates forradon table. Feb. 7,
U.S. EPA. 1993b. Report to the United States Con-gress on Radionuclides in Drinkz”ng Water. Multime-dia and Cost Assessment of Raabn in Drinking Water.Prepared for P.L. 102-389. EPA-SAB-RAC-93-014.

170 I Researching Health Risks
U.S. EPA, SAB (Science Advisory Board). 1990.Reducing Risk: Setting Priorities and Strategies forEnvironmental Protection. SAB-EC-90-021. Washing-ton, DC: U.S. Environmental Protection Agency.
U.S. ERA, SAB. 1993. An SAB Report: Review ofIssues Related to the Cost of Mitigating Indoor RadonResulting from Drinkm“ g Water. EI?A-SAB-DWC-93-015. Washington, DC: lhinmrnentalPmtectionAgency.
Ulsamer, A.G. 1993, Memorandum to P.W. Preuss.Director. OffIce of Science, Plaming, and Regulatory
Support, Environmental Protection Agency. Reviewof the draft uncertainty analysis of risks associatedwith exposure to mdon in -drinking water. Office ofScience, Planning and Regulatory Support. Environ-mental Protection Agency. May 11.
Wilcher, L.S. 1991. Assistant Administrator. U.S.Environmental Protection Agency. Letter to the Hon-orable William E. Damemeyer. Dec. 11.