Embed Size (px)
Citation preview

Journal of Clinical InvestigationVol. 46, No. 8, 1967
Studies of the Mechanism by Which Chronic MetabolicAcidosis Augments Urinary Calcium Excretion in
Man *JACOBLEMANN, JR.,t JOHNR. LITZOW, ANDEDWARDJ. LENNONWITH THE
TECHNICAL ASSISTANCE OF OPAL A. KELLY(From the Department of Medicine and the Clinical Research Center, Marquette University
School of Medicine and Milwaukee County General Hospital, Milwaukee, Wis.)
Summary. Wecarried out clearance studies in nine healthy adults and fourpatients with hypoparathyroidism before and after inducing stable metabolicacidosis with either NHCl or acetazolamide. Clearances were repeated inseven normal subjects and three of the patients 3 days after stopping theseagents.
During acidosis in the normal subjects, serum ultrafilterable calcium con-centration rose significantly, but inulin clearance fell to a greater extent, sothat the calculated filtered load of calcium fell significantly. Despite this,urinary calcium excretion rose. Urinary calcium excretion remained ele-vated in the recovery studies when the serum ultrafilterable calcium con-centration and filtered load of calcium had returned to control levels. Evi-dence is presented indicating that the increased calcium excretion whichoccurred during acidosis and recovery clearances was not due to natriuresisor to increased excretion of complexing anions. The comparable results inthe four patients with hypoparathyroidism, two of whom also had hypo-thyroidism, suggest that the capacity to alter secretion rates of parathyroidhormone, thyrocalcitonin or both is not a critical determinant of the aug-mented rates of calcium excretion during acidosis.
Weconclude that metabolic acidosis produces increased urinary calciumexcretion by causing decreased renal tubular calcium reabsorption. Evi-dence is presented which suggests that this is a direct effect of metabolicacidosis on metabolic processes within renal tubular cells.
Introduction
A number of studies have shown that urinarycalcium excretion is increased during induced(1-3) or spontaneous (4) metabolic acidosis. Inthe dog, acute metabolic acidosis appears to causeincreased urinary calcium excretion as a result of
*Submitted for publication January 5, 1967; acceptedApril 20, 1967.
This investigation was supported in part by U. S.Public Health Service research grant 5 M01 FR-00058and in part by U. S. Public Health Service researchgrant 2 R01 AM-08924.
tAddress requests for reprints to Dr. Jacob Lemann,Jr., Dept. of Medicine, Marquette University School ofMedicine, Milwaukee County General Hospital, 8700West Wisconsin Ave., Milwaukee, Wis. 53226.
a rise in serum filterable calcium concentration andof the filtered calcium load (5). The mechanismof augmentation of urinary calcium excretion dur-ing sustained metabolic acidosis in man has notbeen elucidated.
To examine this problem, we carried out renalclearance studies in the same healthy adult sub-jects and in patients with hypoparathyroidism dur-ing control conditions, after stable metabolic acido-sis was induced with NH4Cl .or acetazolamide, andon the 3rd recovery day after stopping theseagents.
We found that urinary calcium excretion wassignificantly increased in the normal subjects dur-ing stable acidosis despite a significant fall in the
1318

ACIDOSIS AND CALCIUM EXCRETION 1319
>
o d m +_
.O O cdbc cd
0. 0 >00 r
00 cd o0 V 0~WC0 -d5 - 0m
d0 O c
~~~~~ If~~~~.- UU) if
>00~~~~~~~0 0
~ 00E =0 00-
00~~~~~~~~~~\
04~~~~~6 -
,~~00 00'000
?Nc
vCill

JACOB LEMANN, JR., JOHN R. LITZOW, AND EDWARDJ. LENNON
TABLE II
Experimental data for normal subject J. Br.*
Metabolic Clearance Blood Serum Serum Serumperiod period LH+] [HCOa-] total [Cal UFca Cinulin Filtered Ca UcaV
nEqIL mEqIL mmoles/L mmoles/L ml/min pumoles/min jumoles/minControl 1 38.9 24.3 2.40 1.42 124 176 1.30
2 2.38 1.38 117 161 0.883 2.36 1.44 113 163 1.034 38.9 24.5 2.37 1.42 111 158 0.82
Mean 38.9 24.4 2.38 1.41 116 164 1.01
NH4Cl 1 49.0 16.4 2.28 1.42 107 152 5.10acidosis 2 2.34 1.37 123 169 6.55
3 2.33 1.48 108 160 6.404 52.5 15.6 2.35 1.41 115 162 5.80
Mean 50.8 16.0 2.32 1.42 113 161 5.96
Recovery 1 38.0 26.5 2.32 1.41 118 166 2.452 2.32 1.46 131 191 2.303 2.34 1.46 128 187 2.454 35.5 27.0 2.31 1.46 131 191 2.15
Mean 36.8 26.8 2.32 1.45 127 184 2.34
* Abbreviations: UFca = ultrafilterable calcium concentration; Ci~ulii = inulin clearance; UcaV = urinary calciumexcretion.
filtered load of calcium. Augmented urinary cal-cium excretion persisted in the normal subjectsduring the recovery studies when the filtered loadof calcium was at control levels. These resultsclearly indicate that the augmentation of urinarycalcium excretion during experimental chronicmetabolic acidosis in normal man is due to de-creased tubular calcium reabsorption. This couldnot be explained by the known effects of sodiumexcretion (6) or the excretion of poorly reab-sorbable complexing anions (7) on urinary calciumexcretion. Comparable results in the patientswith hypoparathyroidism, two of whom were alsohypothyroid, suggest that alterations in the ratesof Aecretion of parathyroid hormone or thyrocal-citonin are not the cause of the augmented urinarycalcium excretion.
Methods
Studies were carried out in nine healthy adults, twopatients with hypoparathyroidism, and two patients withboth hypoparathyroidism and hypothyroidism. The sig-nificant clinical details concerning these patients areshown in Table I. All were receiving adequate replace-ment therapy when studied. All subjects were hospital-ized in the Marquette University School of MedicineClinical Research Center and received constant normaldiets. All clearance studies were begun at 8:00 a.m. afterovernight fasting. The subjects drank a liter of waterat 7:00 a.m. to induce diuresis and thereafter were given
water at intervals in amounts equivalent to urinary losses.After obtaining blood and urine samples for blank deter-minations, an appropriate priming dose of inulin wasinjected and thereafter a sustaining infusion of inulin inisotonic saline was given at 3 ml per minute with an infu-sion pump. After a 45-minute equilibration period, fourclearance periods were collected. Blood samples weredrawn at the midpoint of each period. The subjects wereallowed to stand or sit to void spontaneously, but other-wise remained recumbent during the studies.
After control clearances, metabolic acidosis was inducedin six of the normal subj ects and in each of the fourpatients by the daily oral administration of gradually in-creasing doses of NH4Cl for 3 to 4 days, and thereafterof a constant daily dose of NH4Cl. Clearances were re-peated 7 to 11 days after NH4Cl was begun when a stablestate of acidosis was present as indicated by no furtherfall in serum bicarbonate concentration during the 2 to3 days before study. In the other three normal subjects,metabolic acidosis was induced by giving 250 mg of aceta-zolamide four times a day. In these subjects, clearanceswere repeated 4 to 6 days after the drug was started.Recovery clearances were carried out in seven of the nor-mal subjects and in three of the patients on the morningof the 3rd day after stopping NH4Cl or acetazolamide.No significant symptoms occurred in any of the subjects.
Inulin in deproteinized filtrates of plasma and urine wasmeasured with the autoanalyzer by Earley and Friedler'sadaptation (8) of the method of Davidson and Sackner(9). Serum ultrafiltrates were prepared by the methodof Toribara, Terepka, and Dewey (10). Since the quan-tity of calcium which is ultrafilterable varies significantlywith the pH at which the ultrafiltrate is separated (10),we modified their method slightly. Wehandled the blood
1320

ACIDOSIS AND CALCIUM EXCRETION
t-o.o0
co c040 -H-Ho 0 0 4
+2- 4C@i 44- 4 -+
C, .
C o
o In
.0.
04H
Il-44-44i-44-44 ni iHNNN C4
4-40
0
00co 0 0o °N -H
c E S-4 4 44
0 0
-H -H -Hl-4
_. o; z "
(I
0 0 .
4-40 (44C4 o; C1
f-H
0;to.
0
0In
coC) vC;
0- -4
0o No 0 0
C4 C4 C4- 0 C%
INliNC4 C4
INvo m ~o co *40 In MC4 C4 N " "-. 1 4
+4C4-+
. ~~~ ~ ~
C4 Z
-H-H1
R n OR C~t "d! > l
0. -. ). .04.4
-H-Hc
co raos 0e
o~~~
0,0tN0 Oo a
csN" N > " o~40~ ~ ~~~~v
sro
~ ~ ~ ~ _c
-H -H r
C-4 1 (4-
0o 0co._V U4 _
-H -H -H
INel
H"!ooZ
0
C4-
coyZ
0 -I
N 04 N -do4-.- t4-
_; .4 1
0 .oHI-H 4
to m4(@m m "Z -.
mI
't40
-Hco
'o_.
0 0%2"-
41 c;
el , t_
W) (4
n 0co Tlm M 'd %n 00
06 06
o -o
o0
I_
4-4
oo o4I
C4-
0q el CS t
co
C4
14 t- co0- v
i
_4)
_ +06S6)eNC4Xouar0
4-4oco
.4
m) +2+o0u
O 0~0 m " mf VWoaa )
e240o04mo 0 0 co6 t-adCm m en
44
0
e i..
'0 .0o
cis~ ~ ~ ~ ~~~~wci ~~~~~~~~~~~~c44. s._ B _
£ £4 ---_ a.* 0*ol 1
0%-H
(@4
4)
C*ro
0
-I.-
~0.
0
o
co
.0
.0
@2)
o.04
0.
4)
04
Cd
0+
oo
04.
4)4.0 c
.0
co
0
1321
08rI-
8U
00
m
~2
4)
0)~0
10
0._
81 u
4)
0
0Go
0C
0
0
u
4)
0
4)
0*0
4i0
U
4.)
0
06
-.~
A20
4)4
4)4
0
.
.
.2
.44
42
0
4).0
4.)
0
0
.2

JACOB LEMANN, JR., JOHN R. LITZOW, ANDEDWARDJ. LENNON
0 r.q R
.t 0
2D00 V
0~~ ~ ~ ~~- -20++
00
(9000 02
.:) _~oq
C4o o 00
00 r--1 -00 - zH-U00
0~~~oo
~ 0%~0r-4r-4~ -H -H--~4 - - 00 Z0
(7o o ~o ON oo
.-0-
oo +~~~~~~~~~~~~~~~00%U,0200 -H -H n
_ _^ zoo Z
00
coN ICIoC00-
1 -H- + -
- -00 00 00*
ecln
001
o U, °.j2UUX ----0(900O-0
00' 9 ~ (~ -H0 > 1
Ch\0- S e - I0
.03
Ew zO
4
0Cd
0 * +-= 1-0 a0
0
0(N 20
-H -- -f(9Xos++0 +
0(0 -H -H -e+
00 %0 -HclH -H
-+
O.bo0 U)
UN
0~~~0%~~-H
- +
00-H-Hcn,
00002 Z 'n00U
z- -H -Hz
\00 + 1 HZ( 0%
0%(('20 -H -H -H
- -
r~ 0
_ U,
-- U) 11-
b u) (-
-s -z
- 9- (9ez
-H -H
_ 0U20oi
00 0 c
- 0 -o o
00 0
\0 -
00 0
_6)N ;oe -H~ O 2_
0-
H O!
00
UH, V
+
m uo
+ O
- V
0
eq Z
+0-Hl1100
+
O.)
0.v0
+
00
0
U) +U,
6n
Uo0 0%U,H200
200
+
U)U, HU)H-H
00-H-
0020O0
-H -Hu
00
U-4
(9(9U, -Hr-00 - U
0000 0-U -H
-4 0%
0%
20
-0
200
U -
0000000 0z
-00 - 00T
1.
060r0,0
0
oA 3I-C
1 E
¢ 0)g
co
0)
06 * 4-I0 1'0 a0
1322
>20)
0
0
0
0O
>2
0
00u
>2
0
tj
0
0
Q
>1I..
v
o08)
04,
¢!
0
0U
>2
0
0
r.
0
0
0
Q)
b
V0
Cd
u.0U)
Cd
Cdr.
r.0-
r-I'P.
.0Cdlu
a

ACIDOSIS AND CALCIUM EXCRETION
specimens with anaerobic precautions and used a varietyof CO2 in air mixtures for gassing the Toribara tubes,allowing a very close approximation to each subject'scalculated in vivo CO2 pressure (Pco2). With thesemodifications, it was possible to separate the ultrafiltrateat a pH within ±0.04 U of that prevailing in vivo.
The remaining methods used in our laboratory havebeen described in a previous publication (11). The re-sults for each subject are presented as the mean of thefour clearance periods in each phase of the studies. Re-sults were evaluated by Student's t test using the equa-tion: t = (d - 0)/(s/Vn), where d and s are the meanand standard deviation of the individual changes fromcontrol for the group (12). Thus, each subject served'as his own control. All group data are presented as themean ± one standard deviation.
Results
Table II shows in detail the effect of NH4Clacidosis on blood [H+], serum [HCO3-], and theparameters of renal calcium filtration and excre-tion in one normal subject (J. Br.). Table IIIpresents the average results of the four clearanceperiods in each phase of the study of all normalsubjects and patients. As illustrated in Table II,the agreement between replicate clearance periodswas satisfactory. For all subjects, the coefficientof variation between clearance periods for thoseparameters required in calculating renal tubularcalcium reabsorption averaged the following: inu-lin clearance ±9.3%o, serum ultrafilterable calciumconcentration ±2.5%c, filtered calcium ±9.5%, andurinary calcium excretion ±9.8%o.
All subjects lost weight for a few days becauseof diuresis after NH4Cl or acetazolamide wasbegun and gained weight for a few days whenthese agents were stopped. In the control studies.the average body weight of the nine normal sub-jects was 63.11 ± 6.05 kg and of the four patients,63.34 + 11.16 kg. The changes in body weightfrom control at the time of subsequent clearancesfor the normal subjects and patients averaged thefollowing: during acidosis, -1.03 ± 1.13 kg and-1.52 ± 0.68 kg; during recovery, -0.05 ± 1.35kg and -0.79 ± 1.03 kg, respectively. Duringthe clearances urine flow rates were always above8 ml per minute and were comparable in the samesubject in each phase of the studies.
In Tables III, IV, and V, few important differ-ences in the responses to acidosis produced byNH4Cl or acetazolamide in the normal subjectswere noted. The differences that seem signifi-
cant will be described, but otherwise the responsesof all normal subjects will be considered together.
As shown in Table III, the expected rise in blood[H+] and fall in serum [HCO3-] occurred in eachsubject during the administration of NH4Cl oracetazolamide, and these parameters had returnedto control values by the time of the recovery clear-ances. The severity of the acidosis was compara-ble between groups.
During acidosis, the serum total calcium con-centration fell in eight of the nine normal subjects(d = - 0.08 + 0.05 mmoles per L; p < 0.005),whereas serum ultrafilterable calcium concentra-tion (UFca) rose in each normal subject (d =+ 0.05 + 0.05 mmoles per L; p < 0.025). How-ever, because inulin clearance was reduced duringacidosis in eight of the nine normal subjects (d =- 13 + 12 ml per minute; p < 0.025), the calcu-lated rate of calcium filtration fell significantly(d =-13 + 16 pmoles per minute; p < 0.05).Nevertheless, urinary calcium excretion (UcaV)rose in each normal subject (d = + 3.18 ± 2.01umoles per minute; p < 0.005).
During acidosis, the patients on the average hada small increase in serum total calcium concentra-tion, and in three of the four, UFca rose (d = +0.10 + 0.10 mmoles per L).' The average fall infiltration rate for the patients (d = - 3 + 4 mlper minute) was smaller than that noted in thenormal subjects. Consequently, the calculated rateof filtration of calcium rose in two of the fourpatients. UcaV rose in each patient (d = + 4.63± 4.30 pmoles per minute). The increase inUCaV occurred despite a fall in calcium filtrationrate in S. C. and M. L. and exceeded the smallrise in calcium filtration rate in J. G. The strik-ing and equivalent increases in calcium filtrationrate and UcaV in L. K., who had severe idio-pathic hypoparathyroidism, differed from the find-ings in all other subjects studied.
During the recovery clearances, UcaV remainedsignificantly elevated above control values in theseven normal subjects (d = + 1.47 + 0.96 4molesper minute; p < 0.01) despite the return of bloodacid-base measurements to normal. In four ofthese seven studies, because of either a persistentelevation in UFca or a rise in filtration rate, the
1 The lack of statistical significance for many of thechanges observed in the patients clearly results from thesmall size of the group available for study.
1323

JACOB LEMANN, JR., JOHN R. LITZOW, ANDEDWARDJ. LENNON
C14 -It 00 0%
-t O 00N + +:: o qw m + + ""
)U) (Iooooo
- ,,t v 00r 0oo+o t v
4O
Sr~~~~rY0 C+ .d0WIU) QO °00t- - T-4- 0r ; \ -
+
20
inV 00'- 0\ - I t00 \0CO4i n
4O
CmC9 0 N0C'4 \
WU)00 \%0~)t V*.^ N ~~~U)U) 0
-I
U \0
..4 -t q00 0+ w U-0o 00 -4 \0 -47 -
-4 e--- d ) --_
04)
2I
C 0s r-00
E +r0~~~
z z~~
00
00 0%Zm +
U)
to1C1 CN _.4
+ HO
e m
%0 %Oto
-Hl -H OT-
U)xo
CO.
mf 0%
-HIld
00mto
e# U)
I
to
-.to)ZU) e4
en~
+
4Oo, _o6m to V
"o mV
U)
m moH -H
00 0%
-.4 0%
U)
_ I
000z0 I1
U) 0
t- U)
41i -H
I-
-HU)
00
~o
oZ
N 0%
I00 U)
00
1- T-
r do-oU)
U)
O%)-H -HO
%00o U) 0co V
+
C1400 4 -Ho
00v0
11 m0
Z -i -
00~o to 0
tQ~o U))4\0 -H0+ v
\0
eO °Ou
6
00 q4 -Om l-H T
oO4 d- 1 \0 Z
-
t-
WU4 in oo Ul) -Wo-1
Cd.0
r. 'o M
C34-1
w 0 cu~~
Cd
@~~~~~~~~~~~~4g O 023
01 Y l Ul-
._
u
blD0
0
4)
O
._
lo
C21
U)
.0
60'._
4)J
4Q
2t
0
4)-
0
so
4)0I
0C
._
Co
4)0
O .-
0cd0d.0
02bO.0
C.) ,V
4)4.
._
*
1324
204)
0
v
aaP4
0
>2
0
a)0
o0r
U
4)
04
42
wo15u
% 0
:D u.!402
-o
00
U
C)
.0
(n
C;:z
2-
U
.0
*0e
O)U ?
2-:),0
$ .-2
O
.^O
0=U
U<
0b
:0

ACIDOSIS AND CALCIUM EXCRETION
0 00s4 C
CE)00%%0 0 0
0%U) 0001% m- -- ~~4 -HCE)
.4 -
t _~
-I
0000-d4 000%r
%000%cCE)0
.X ~~~~~~+41ri
eO-etd 6o
V" V-° ° ds4 010 °
C4o
oq ID tn 0% mo 01
00 -40000- NH
O -
*1 z~4'U
oo C5 C 00 -.d z
00
0 - --\ U)%0
CEI- CE) If) 00
00 0 0ofOCEteq
Cl i CE) 4 eq4 -U
01% 0 m 00 0, ( e 0_6
oov-66O-S .i00
0%0+eq~eeq)006
00
o u)*in
I- 00t. 41 -Hc~i o6 o~
- I
0%.
X-o.m -H+ cnU) 0o eq
o(Ci ooC14 +
00 N0
0, C-4 Z~*-
- 00
e +0
eq4 t
00 eq4- .41 41
0h Cs 00 % 0lsi Ili - -T
-4
000eCE)
eq
-H-lto
V--4 0U)Z_ uo,o _--
.14 0Y%-o
-H -HY)ot I
U) tU)
-V
-4t
NeO 0-4 0 -H -H
_-_ U) 00
V- -4
00 -
O -
66600%000 -
0
"46++
Ul)-i -!Co 0
(
00 -
6; 6
6o
1
0 8el. .
0 0
oON
00
U) I- C4C
C-.4 co 41C 0 eq1
0 0
'IO eq40NV.4j4 Zq H4
- eq-Il
o6scA4. Z00 Cen
oo+
c;o\cli
CE)
U)H40-6) 00 Qf
U)00en
.+
-- +
-0
U)%0' oqot-eqS
mt '-o00
00 000 eq4_oo
00
-H
0%0%
000
0 eq
66t o I -H+
-
-V4 ci
*0
%ONOCo-C)Oqv- HO,_64owc
-I i
00 00 00
14- 14 14
1.
Cd
U) .Cd
, 04 or044E
4) .- 4.2)° ¢
Z;0 <v4Zzz~~~~~~~~~~~~4
-e
4100
d41.
a * -1--
10D
1325
>2>40
0
0
0
1
>20F.)
0
ra.
0
0
o
>2
0
0
0
0
0
.O
o0
0
o
ow
b.
4n
0
10
o0
w0
0
10
sco
.0w
0
06
to)
4-)
x
At
0
4-
04--$~0
0
r.0* 0
cn
4>
Cd
*-.4)
U)
cd
.00
4)
4-)
la
06
-0
bO.
4).0
00 C
C6
4)J
0Cd
.cd0
u4)
X4-)
o .o
o -
4)4

JACOB LEMANN, JR., JOHN R. LITZOW, AND EDWARDJ. LENNON
filtered load of calcium was sufficiently above con-trol values to account for the continued increase inUcaV. In the other three normal subjects, UcaVremained above control despite a reduction in therate of calcium filtration.
UcaV also remained elevated in the three pa-tients studied during recovery from acidosis, de-spite correction of blood [H+] and serum[HCO3-] to normal. In each of these patients,the filtered load of calcium had returned to orbelow control levels by this time.
Table IV gives the changes in UNaV, UKV, andUNH4+V during acidosis and during recovery forall studies. Serum sodium concentration remainednormal and steady in all groups. Serum potas-sium concentration fell during acidosis and re-mained low during the recovery clearances in allstudies. UNaV was below control rates in six ofthe nine normal subjects during acidosis and inall seven of the studies during recovery. Therewas no correlation between the variable changesin UNaVand the consistent increases in UcaV dur-ing acidosis. UKV fell in seven of the normalsubjects during acidosis and in each of the sevenrecovery studies. As expected, UNH4+V rose sig-nificantly in each normal subject given NH4Cl,whereas smaller rises occurred in the three normalsubjects made acidotic by carbonic anhydrase inhi-bition (acetazolamide). UNH4+V fell, but re-mained above control when NH4C1 administration
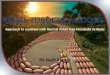
A UCAV,uM/min.
AUcAV M/min -0.23 +0.032 ALUNH4 V xEq/minr +0.89
p<O.001
+50 +100
LAUNH4V ,uEq/min.
FIG. 1. CORRELATIONBETWEENCHANGESIN URINARY
CALCIUM EXCRETION (A UcaV) ANDCHANGESIN URINARY
AMMONIUMEXCRETION (A UNH4+V) IN NORMALSUBJECTS.
* = NH4Cl acidosis, 0 = recovery from NH4Cl acidosis,A = acetazolamide acidosis, A = recovery from aceta-
zolamide acidosis.
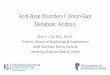
+1
A UCAVtM/min.
0 + 50 +100
AUNH+V jEq/min.
FIG. 2. RELATIONSHIP BETWEEN (A UcaV) AND
(A UNH4+V) IN PATIENTS WITH HYPOPARATHYROIDISM.* = NH4Cl acidosis, 0 = recovery from NH4Cl acidosis.The solid line is the regression line for the normalsubjects, which is included in this figure for comparison.
was stopped, and exceeded the values duringacidosis when acetazolamide was stopped. Thechanges in UNaV, UKV, and UNH4+V in the pa-tients were comparable to those of the normal sub-jects given NH4Cl.
Figure 1 shows a striking correlation betweenthe increments in renal ammonium and calciumexcretion above control during the acidosis andrecovery clearances in the normal subjects.
Figure 2 shows the same relationship in thepatients with hypoparathyroidism.
Table V presents the effects of induced acidosison serum phosphorus concentration and renalphosphorus excretion. Serum phosphorus concen-tration fell during acidosis in six of the sevennormal subjects given NH4C1 and rose slightlyin each of the three normal subjects given aceta-zolamide. Because of the reductions in glomeru-lar filtration rate, the filtered phosphorus load fellin seven of the nine normal subjects during acido-sis. Despite this, UpV rose in all of the normalsubjects. In the recovery studies in normal sub-jects, none of the parameters of renal phosphorusturnover differed from control observations. Theresults in the patients with hypoparathyroidismagain closely resembled those of the normal sub-jects given NH4Cl.
Discussion
In the present renal clearance studies, each ofnine normal subjects demonstrated an increase in
1326
Z=f=
.

ACIDOSIS AND CALCIUM EXCRETION
UCaV above control rates when metabolic acidosiswas induced by either increasing acid productionby NH4Cl administration (six subjects) or in-hibiting renal acid excretion by acetazolamide ad-ministration (three subjects). In eight of the ninenormal subjects, the observed increases in UCaVoccurred despite reduction in the rates of filtrationof calcium. Whereas UFca rose during acidosisin each of the nine subjects, presumably becauseof decreased binding of calcium by serum proteinsand a net increase in the rate of release of calciumfrom bone, inulin clearance fell to a greater ex-tent and, thus, the calculated rate of filtration ofcalcium was reduced. Weassume that the fall inglomerular filtration rate was due to extracellularfluid (ECF) volume depletion resulting from theinitial diuretic effect of both NH4Cl and aceta-zolamide. Clearly, the increases in UcaV ob-served during acidosis in these subjects must havebeen due to decreased renal tubular calciumreabsorption.
UcaV remained elevated above control rates ineach of the seven normal subjects studied againthree days after NH4Cl or acetazolamide adminis-tration was stopped. Since blood [H+] and serum[HCO3-] had returned to control values in eachsubject by this time, it is clear that ECF acidosiscould no longer be invoked as the cause of theaugmented renal calcium excretion. However,we have shown previously (3) that during therecovery from induced metabolic acidosis blood[H+] and serum [HCO3-] return to control levelsbefore all of the retained acid has been eliminatedfrom the body. Thus, it is quite conceivable thathydrogen ion concentration within cells (includ-ing those of the renal tubules) remained elevatedat the time of the recovery clearances. In four ofthese seven recovery studies, the calculated rateof filtration of calcium had risen sufficiently toaccount for the persisting increase in UcaV. Thisoccurred because of increases in inulin clearancesand, in some subjects, continued slight elevationof UFea. In the remaining three studies, how-ever, UCaV remained elevated despite rates ofcalcium filtration less than those of their controlstudies.
Although these results in normal subjects do notallow precise identification of the cause of de-creased tubular calcium reabsorption during in-
duced metabolic acidosis, we have considered sev-eral possibilities.
Walser (6) has shown that urinary calciumexcretion rises when sodium excretion is aug-mented. This could not account for the resultsof our experiments, since, on the average, urinarysodium excretion was unchanged from controlvalues during acidosis and somewhat below controlvalues during the recovery studies. Furthermore,there was no correlation between the variable di-rectional changes in UNaVduring acidosis and theconsistent increases in UcaV.
It is also unlikely that UcaV increased becauseof an increase in the rate of excretion of poorlyreabsorbable anions capable of complexing calcium(7). Whereas urinary phosphorus excretion wasincreased during acidosis, it was not elevated abovecontrol rates during the recovery clearances, whenUcaV remained elevated. Urinary sulfate andorganic acid excretion did not increase signifi-cantly in our earlier balance studies in which acido-sis was induced in a similar manner (3). Inaddition, the high urine flow rates maintained inall of the present clearance studies would haveminimized, by dilution, any effects of complexinganions.
Wecarried out the studies in the four patientswith hypoparathyroidism, two of whom were alsohypothyroid, to determine whether the capacity toalter the secretion rate of parathyroid hormone,thyrocalcitonin, or both, was required for aug-mentation of UCaV during metabolic acidosis.Weconsidered this possibility because the rise inultrafilterable (and presumably ionized) calciumin the blood of the normal patients during acidosiscould have altered the rates of secretion of thesehormones. Parathyroid extract has been shownto augment directly calcium reabsorption at adistal tubular site in the dog (13), and thyro-calcitonin, while not yet known to alter tubularcalcium reabsorption, produces phosphaturia inthe rat (14). Since the response to metabolicacidosis in the normal subjects included both de-creased tubular calcium reabsorption and de-creased tubular phosphorus reabsorption, it seemedpossible that these effects were mediated, respec-tively, by a decreased secretion of parathyroid hor-mone and an increased secretion of thyrocalci-tonin in response to the rise in ultrafilterable (andionized) calcium. The results in the four patients
1327

JACOB LEMANN, JR., JOHN R. LITZOW, ANDEDWARDJ. LENNON
suggest that this was not the case. With the ex-ception of the study during acidosis in patientL. K. (where the rate of calcium filtration rosesufficiently to account for the increase in UcaV),the responses of the patients closely resembledthose of the normal subjects.
Finally, since metabolic acidosis alters metabolicprocesses in renal tubular cells in other ways (15),it is possible that the observed decrease in calciumreabsorption during acidosis is also a direct effecton the tubule cells. A correlation between theincrements in urinary ammonium and calcium ex-cretion in response to induced acidosis was notedin both the normal subjects (Figure 1) and thepatients (Figure 2).
Although in two of the three normal subjectsgiven acetazolamide maximal UcaV occurred dur-ing the acidosis clearances while UNH4+V washigher during the recovery clearances, it is knownthat urinary ammonium excretion may underesti-mate total renal tubular ammonia production dur-ing carbonic anhydrase inhibition (16). Thus,stimulation of the metabolic processes involvedin the tubular production of ammonia rather thanurinary ammonium excretion per se may somehowimpair renal tubular calcium reabsorption. Farqu-harson, Salter, Tibbetts, and Aub (1) also notedthat changes in calcium and ammonium excretionwere related in induced metabolic acidosis. Al-though they felt that calcium and ammonium ex-cretion during acidosis were not directly inter-dependent, this will require further study.
References
1. Farquharson, R. F., W. T. Salter, D. M. Tibbetts,and J. C. Aub. Studies of calcium and phosphorusmetabolism. XII. The effect of the ingestion ofacid-producing substances. J. clin. Invest. 1931,10, 221.
2. Sartorius, 0. W., J. C. Roemmelt, and R. F. Pitts.The renal regulation of acid-base balance in man.IV. The nature of the renal compensations in am-monium chloride acidosis. J. clin. Invest. 1949,28, 423.
3. Lemann, J., Jr., J. R. Litzow, and E. J. Lennon.The effects of chronic acid loads in normal man:
further evidence for the participation of bone min-eral in the defense against chronic metabolic acido-sis. J. clin. Invest. 1966, 45, 1608.
4. Atchley, D. W., R. F. Loeb, D. W. Richards, Jr., E.M. Benedict, and M. E. Driscoll. On diabeticacidosis. A detailed study of electrolyte balancesfollowing the withdrawal and reestablishment ofinsulin therapy. J. clin. Invest. 1933, 12, 297.
5. Williamson, B. J., and S. Freeman. Effects of acutechanges in acid-base balance on renal calcium ex-cretion in dogs. Amer. J. Physiol. 1957, 191, 384.
6. Walser, M. Calcium clearance as a function of so-dium clearance in the dog. Amer. J. Physiol.1961, 200, 1099.
7. Walser, M. Ion association. VII. Dependence ofcalciuresis on natriuresis during sulfate infusion.Amer. J. Physiol. 1961, 201, 769.
8. Earley, L. E., and R. M. Friedler. Studies on themechanism of natriuresis accompanying increasedrenal blood flow and its role in the renal responseto extracellular volume expansion. J. clin. Invest.1965, 44, 1857.
9. Davidson, W. D., and M. A. Sackner. Simplifica-tion of the anthrone method for the determinationof inulin in clearance studies. J. Lab. clin. Med.1963, 62, 351.
10. Toribara, T. Y., R. Terepka, and P. Dewey. Theultrafilterable calcium of human serum. I. Ultra-filtration methods and normal values. J. clin. In-vest. 1957, 36, 738.
11. Lennon, E. J., J. Lemann, Jr., and J. R. Litzow. Theeffect of diet and stool composition on the net ex-ternal acid balance of normal subj ects. J. clin.Invest. 1966, 45, 1601.
12. Snedecor, G. W. Statistical Methods, 5th ed. Ames,Iowa, Iowa State College Press, 1956, p. 45.
13. Widrow, S. H., and N. G. Levinsky. The effect ofparathyroid extract on renal tubular calcium re-absorption in the dog. J. clin. Invest. 1962, 41,2151.
14. Robinson, C. J., T. J. Martin, and I. MacIntyre.Phosphaturic effect of thyrocalcitonin. Lancet1966, 2, 83.
15. Goodman, A. D., R. E. Fuisz, and G. F. Cahill, Jr.Renal gluconeogenesis in acidosis, alkalosis andpotassium deficiency: its possible role in regulationof renal ammonia production. J. clin. Invest. 1966,45, 612.
16. Owen, E. E., M. P. Tyor, J. F. Flanagan, and J. N.Berry. The kidney as a source of blood ammoniain patients with liver disease: the effect of ace-tazolamide. J. clin. Invest. 1960, 39, 288.
1328