-
8/8/2019 Student Respiratory
1/15
1
THE RESPIRATORY SYSTEM
I. Definitions
A. Respiration - O2/CO 2 exchange between the body and the
environment.
1. Pulmonary ventilation
2. Diffusion of O2 and CO2
3. Transport of gases to and from tissue
B. Breathing - The movement of gas in and out of the lungs.
C. Lungs - air/blood flow for O2 and CO2 exchange. Maintaining
correct CO2partial pressure (PCO 2) is more important than PO2
because of pH.
D. Perfusion (Q) - cardiac output
EF. Partial pressure- How gases are measured.
II. Structural Basis of Breathing
A. Airways - structural/functional characteristics
Trachea cartilaginous support Have smooth muscle.
9 Can constrict airways
Bronchi esp. term. bronchioles
9 Have cilia; secrete mucus
Bronchioles conducting zone
9
Terminal
bronchioles
9
Respiratory
bronchioles
9 Diameter depends on
Alveolar ducts "terminal respiratory lung volume
9 unit"; primary areas of
Alveoli gas exchange
-
8/8/2019 Student Respiratory
2/15
2
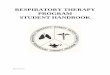
Alveoli have thin walls and a large
surface area.
B.Pulmonary capillaries - cover 70-80% of alveolar walls.
Capillary volume can
increase through recruitment and distension.
-
8/8/2019 Student Respiratory
3/15
3
C. Definitions
1. Inspiration - active phase of
breathing. Diaphragm and
external intercostal muscles.
2. Expiration - usually a passive
process. Abdominal muscles andinternal intercostal muscles
can
participate.
D. Lung expansion and contraction -
1. Transpulmonary pressure - pressure difference between
thoracic cavity and
alveoli.
2. Compliance - how easily lung expands.
Determined by:
a. elasticity of tissue
b. surface tension
Lung compliance measures the force that is needed toexpand the
lungs, or the ease of expansion. A lung with ahigh compliance is
easy to expand, whereas a lung with alow compliance is stiff and
hard to expand. The opposing orcompressive forces are the lung
elasticity and surfacetension.
Emphysema - loss of elastic fibers, so itincreases compliance
and decreases
elastance.
Fibrosis decreases compliance, so lung is
harder to expand and collapses further when
exhaling.
Asthma - Increase in airway resistance due to
constriction of smooth muscles.
3. Surface tension - attraction of water molecules for each
other at the
interface with air. This collapses alveoli.
4. Surfactant - Mixture of phospholipids, apoproteins and Ca2+
secreted by
type II alveolar cells. Decreases surface tension.
Neonatal respiratory distress syndrome
-
8/8/2019 Student Respiratory
4/15
4
III. Alveolar Ventilation -
A. Typical volumes and capacities:
VT = tidal volume = vol. of air in each breath.
-
8/8/2019 Student Respiratory
5/15
5
C. Relationship between
-
8/8/2019 Student Respiratory
6/15
6
E. Alveolar Gas Equation - predicts PAO2 based on PACO2.
PAO2. PO2 (air) - PACO2/R (R = Respiratory exchange ratio=
CO2production/O 2 consumpt ion) Ideally, R = 0.8
R is related to metabolic rate, energy sources, activity,
etc.
Use PACO2 to estimate PAO2:
During exercise, R can decrease to 0.53. PAO2 and PACO2 dont
change because
of the ventilation/perfusion ratio (
-
8/8/2019 Student Respiratory
7/15
7
IV. Ventilation/Perfusion Ratios (
-
8/8/2019 Student Respiratory
8/15
8
Smoking leads to:
1) small bronchioles become obstructed, causing excessive
physiological
shunt
2) alveolar walls become damaged causing excessive physiological
dead
space. (wasted ventilation)
3) incr. compliance of lungs4) increases in allergies and
asthma
Matching Q and
-
8/8/2019 Student Respiratory
9/15
9
V. Neural/Central regulation of
-
8/8/2019 Student Respiratory
10/15
10
B. Spinal integration - mechanoreceptors in muscles stimulate
spinal motor
neurons to inhibit their activity
C. Chemoreceptors - responsive to [H+] and [CO2].
i CO 2 + H2O W H2CO 3W H+ + HCO3- (bicarbonate) i
carbonic anhydrase
1. Central chemoreceptors - along surface of medulla; sensitive
to[H+].
2. Peripheral chemoreceptors - carotid bodies; sense PCO2 and
PO2
D.
-
8/8/2019 Student Respiratory
11/15
11
Change in Va in responseto a change in PCO2
Change in PCO2 inresponse to a change in Va
Likewise, reduced PaO 268
-
8/8/2019 Student Respiratory
12/15
12
VI O2 and CO2 Transportation
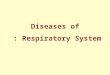
A. O 2 Transportation - Reversible binding
of O 2 to Hb:
O2-Hemoglobin Equilibrium Curve:
1. O2 is picked up in the lungs and
released in tissues
2. Hb buffers blood PO2 from major
changes.
B. Factors affecting HbO2 equilibrium curve
1. [H+], PCO 2 - Bohr effect.
2. Incr. temp. or 2,3-diphosphoglycerate3. CO - decreases O2
binding capacity
C. CO2 Transport
In the blood, CO2 is transported as:6 HCO3
- (ionic form; 90% of CO2 in blood)
6 protein bound (carbamino-CO2; HbCO2)
6 40 ml/L dissolved in plasma as a gas
CO 2 + H2O W H2CO 3W H+ + HCO3
-
8
Carbonic anhydrase
-
8/8/2019 Student Respiratory
13/15
13
In red blood cells this goes very rapidly. End products are
eliminated by:
1. H + combining with Hb 6 HHb
2. HCO3- diffuses into plasma in exchange for Cl-.
3. HCO3- attaching to Hb 6 HbHCO3
D. Modulation of CO2 binding to Hb - Haldane effect
PO2 decreasesCO2 binding to Hb. This nearly doubles the CO2
exchange in
the lungs.
= tissue conditions
= alveolar capillaries CO2-
bound
= change going from Hb
tissue to alveoli
E. [H+] Regulation - maintain pH 7 .4, range 7.2-7.6; damaging
beyond 6.7
and 7.8.
pH - log[HCO3-]
PCO 2
-
8/8/2019 Student Respiratory
14/15
14
1. pH - PCO 2 - HCO3- relationship Bicarbonate is potent
buffer;
8acids cause HCO3- to be converted to CO2 and H2O:
carbonic anhydrase
H+
+ HCO3-
6 H2CO 3W CO 2 + H2O
and CO2 is eliminated in lungs. Hb acts as an additional
buffer
if8CO 268H+
if8HCO3-69H+
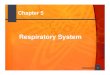
2. pH - bicarbonate diagram
At a given PCO 2, as you increase
pH, [HCO3-] goes up. If you
increase PCO 2, the curve shifts to
the left. The Buffer slope line
represents the buffering
capacity of the blood, especially available Hb.
During exercise, you get an8in acids.
i. Hb buffers some H+, so buffer slope line drops.
ii. HCO3- buffers some, so get 9[HCO3-].iii. 8PCO 2 causes 8
ventilation; with over compensation you get 9PCO 2.
3. Physiologic factors controlling pH
a. respiratory control mechanisms:
b. renal mechanisms (discussed in upcoming lectures on Renal
system)
-
8/8/2019 Student Respiratory
15/15
15
Nicotine in urine of smokers' babiesBy LEE BOWMAN, Scripps
Howard News Service
May 14, 2006
Scientists have found cancer-causing chemicals from tobacco
smoke in the urine of nearly half the babies ofsmoking parents they
tested in a new study.
The study found "substantial uptake" of nicotine and the
chemical NNAL in 67 of 144 infants, or 47 percent, and the
levels were directly related to how much their parents smoked
around them in the home or car. NNAL is a byproductof a toxin in
tobacco that's known to cause lung cancer.
"The take-home message is: Don't smoke around your kids," said
Stephen Hecht, a cancer-prevention researcher atthe University of
Minnesota Cancer Center who led the study, published Friday in the
journal Cancer Epidemiology,Biomarkers and Prevention.
Hecht and his team collected urine samples from the infants,
3-12 months, and interviewed parents about smokinghabits.
Eighty-two percent of the babies' mothers were daily smokers and 72
percent had other family members,including fathers, who smoked.
Parents or other family members of babies who had detectable
levels of NNAL smoked an average of 76 cigarettesa week in the home
or car with the infants present. Children with undetectable levels
of the chemical had familymembers who smoked an average of 27
cigarettes near the babies each week. Nearly all the babies had
detectablelevels of nicotine, as well as cotinine, the byproduct
that's left as the body metabolizes nicotine.
However, Hecht said that the difference likely reflects the
limits of the equipment used by the researchers. "Withmore
sensitive analytical equipment, the NNAL from urine of babies in
lower-frequency smoking households wouldmost likely be
detectable."
The infants' NNAL levels were higher than those seen in studies
of adults exposed to secondhand smoke in thehome.



















![Respiratory disorders(student)[1]](https://img.pdfslide.us/doc/110x75/55655061d8b42a77078b48de/respiratory-disordersstudent1.jpg)






