Embed Size (px)
Citation preview
Billing and Coding in Neurology and Headache
Stuart B Black MD, FAAN
Chief of Neurology
Co-Medical Director: Neuroscience Center
Baylor University Medical Center at Dallas
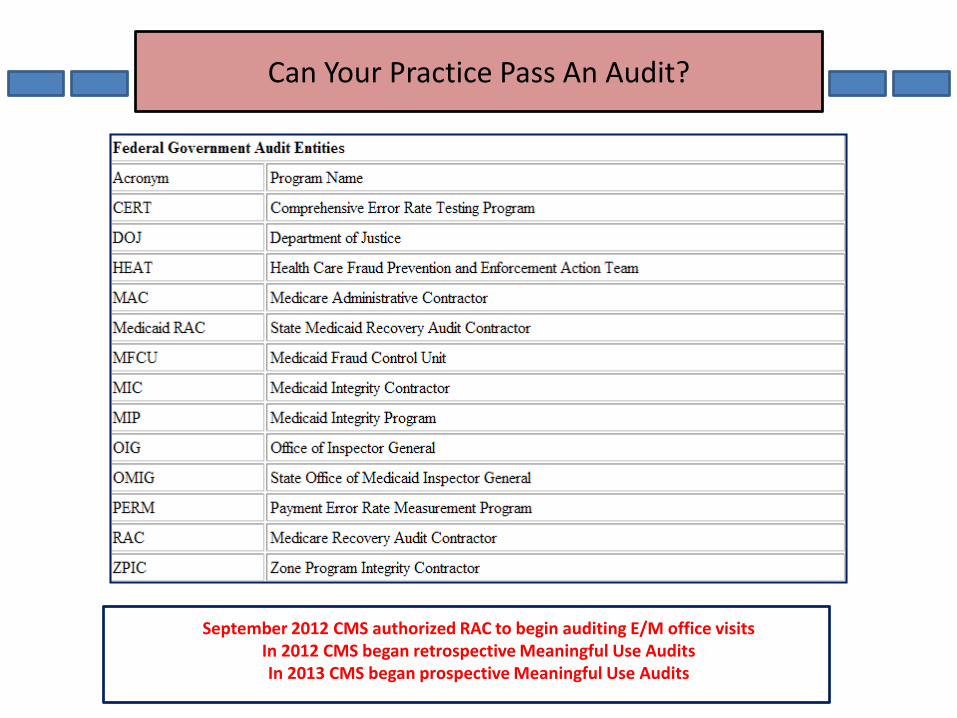
Can Your Practice Pass An Audit?
September 2012 CMS authorized RAC to begin auditing E/M office visitsIn 2012 CMS began retrospective Meaningful Use Audits In 2013 CMS began prospective Meaningful Use Audits
RAC Audits
Connolly Healthcare: Exclusive RA prime contractor for region C
Covers 35% of all claim volume from 17 states
Connolly has collected more than $3 billion in audit payments
Connolly is paid on a contingency fee of 9% of collections
E/M Codes make up 1.6% of all procedure codes
E/M Codes account for 20% of all approved services
E/M Codes account for 43% of Medicare B payments
CMS estimates up to $35 billion a year is paid “erroneously”
The CMS 2011 “Improper Payments Report” indicated an “erroneous”
payment rate of 8.6% representing $28.8 billion in “improper payments”
RAC AuditsQuestions Being Raised By CMS
2010: 370 Million E/M services were submitted to CMS by 442,000 physicians
2010: Payments for Medicare E/M increased from $22.7 to $33.5 Billion
Health and Human Services Office and The Department of Justice:
Are the increases in E/M services due to “Upcoding”?
Has upcoding occurred in tandem with increased use of EHRs?
Is Upcoding due to Cut and Pasting, Cloning, Macros, Templates and Prepopulated Data?
Will audits show Bulleted Lists which are not compliant with Medical Decision Making?
Do EHRs allow physicians enhanced capabilities to record their services?
Do EHRs provide physicians enhanced billing capabilities without ↑ services?
Do EHRs provide focused documentation to mainly justify coding and reimbursements?
Do EHRs focus on a traditional reason for record keeping or on a payer instigated process?
Do EHRs jeopardize the traditional record keeping process and safeguards?
Not All EHRs Are Created Equally
There are ±600 EHR vendors listed
The most widely used EHRs are:
Epic -22% Centricity – 6% Next Gen – 6%Allscripts -10% eClinicalWorks – 5% Greenway – 1%
▫ In 2011, the Dept. of Health and Human Services Office of the National Coordinator for Health Information Technology established EHR certification for Meaningful Use
There is no EHR certification or formal evaluation process for EHR E/M coding tools
All EHR users must upgrade their systems before attesting to meaningful use under Medicare for the 2014 payment year.
▫ It does not matter whether they attest to Stage 1 or Stage 2 of meaningful use
but
▫ Regardless of the stage of meaningful use being met, they must use a Stage 2 certified product in 2014
Some EHR venders have already released Stage 2 certified versions Check the Certified Health Product List (CHPL) to see if your vendor has upgraded
Is Your EHR 2014 Certified
During attestation CMS requires you give them an EHR Certification ID for the EHR technology you use to demonstrate meaningful use.
What Auditors Focus OnFocused Documentation to justify coding / reimbursements?
Documentation: Must have Narrative for HPI and Medical Decision Making
Must be information obtained “…during a particular encounter”
Must be relevant data “…for the specific visit”
A HPI and MDM “…unique for the designated patient encounter”
Red Flags: Especially for HPI and Medical Decision Making:
Cloning of data not relevant to the specific visit
Cut and Pasting of data not unique to the specific patient encounter
Data from Templates such as the same level 4 or 5 H&P for each visit
Prepopulated Data which may not be accurate for the specific visit
Bullets and macros
“Bullets without transcript/narrative do not define the physician’s decision making thought process”
Why Auditors Focus On Medical Decision Making“Cloning ICD From Prior Visit is Not MDM”
The MDM Elements Are The number of diagnosis or management options The amount of data reviewed or orderedThe complexity of data reviewedThe complexity of data orderedThe risk of the presenting problemThe risk of diagnostic procedures oThe risk of management options selected
“For a presenting problem without an established diagnosis, the assessment may be stated in the form of differential diagnosis or as a ‘possible‘, ‘probable‘, or ‘rule out‘ (R/O) diagnosis”
MDM does not ask for the final diagnosis. That is the ICD which also links the diagnosis code(s) with the
services provided (CPT)
MDM defines the physician’s actual cognitive process and intellectual process during the patient encounter
Red Flags
Repetitious data based reports that are embedded in templates
Overreliance on Templates and “check boxes” leads to the disappearing narrative
Array of patient data not conducive to critical thinking and treatment plan
MDM templated; not compliant with E/M Documentation Guidelines
Medical Decision Making bulleted lists; not specific for the designated encounter
Documentation does not reflect changes in the physical exam
Plans and recommendations are fragmented and hard to find
Copy forward notes with significant documentation errors
Office records for different patients all look the same with similar dialog
CMS requires narrative for HPI and MDM
EHR
For legal reasons, know what the printed copy of your EHR report looks like.
Develop a policy statement that defines what your practice considers to be a legal patient record.
□ When is the record considered complete for compliance purposes?
□ What data are disclosed upon request for medical records?
Record patient compliance, including missed/cancelled appointments
Record patient and related telephone conversations
Use the EHR for clinical alerts and reminders
□ Known or suspected allergies
□ Medication list/reconcillation
□ Therapeutic decision support via formularies
□ Patient education
□ Evidence-based diagnostic decision support
RBRVS and E/M CPT Codes
The Resource Based Relative Value System: Uniform policy for physician paymentsCPT: Codes for reporting and describing the medical services and proceduresICD: Codes used to describe diseases and other health problems
Each CPT code is assigned a total number of Relative Value Units (RVU) which represent the physician time, resources and expertise to perform a service
Each RVU has three components
1. Physician’s Work = 52% of the total relative value service2. Practice Expense = 44% of the total relative value service 3. Medical Liability Insurance = 4% of the total relative value service
A Geographical Practice Cost Index (GPCI) adjusts the RVU for regional differences
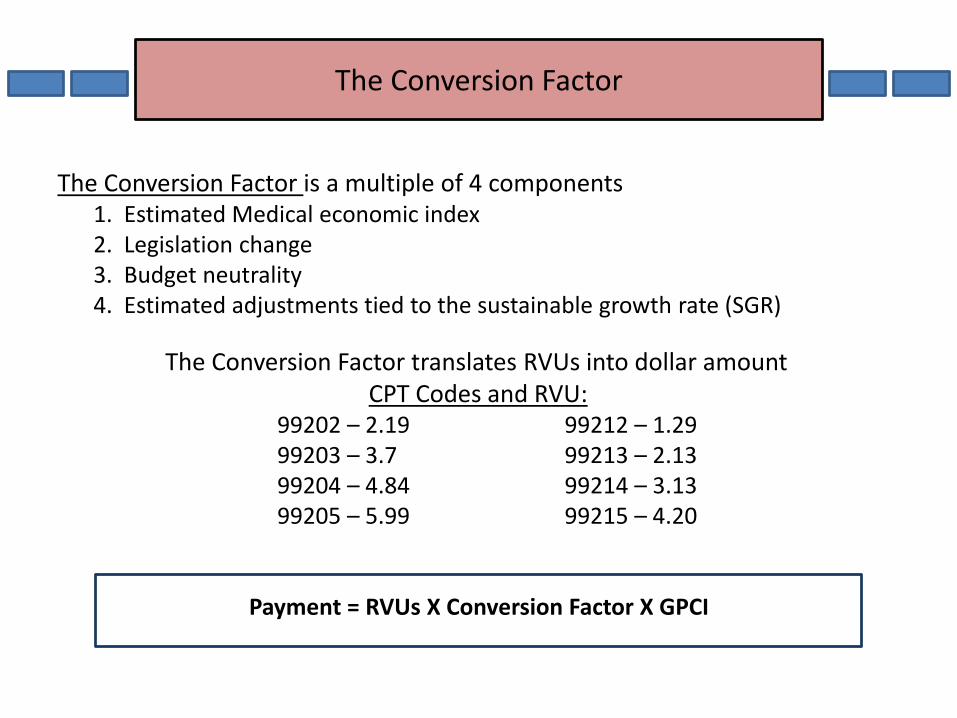
The Conversion Factor is a multiple of 4 components1. Estimated Medical economic index2. Legislation change3. Budget neutrality4. Estimated adjustments tied to the sustainable growth rate (SGR)
The Conversion Factor translates RVUs into dollar amountCPT Codes and RVU:
99202 – 2.19 99212 – 1.2999203 – 3.7 99213 – 2.1399204 – 4.84 99214 – 3.1399205 – 5.99 99215 – 4.20
Payment = RVUs X Conversion Factor X GPCI
The Conversion Factor
AAN Position StatementDefinition of Neurology Subspecialty
2012CPT Revision:“Guidelines for Evaluation and Management (E/M) Services define the use of new and established patient visits based on whether a patient has been seen by a provider of the exact same subspecialty who belongs to the same group practice within the previous three years”
“For the purposes of defining the subspecialties of neurology, the AAN looks to accreditation and certification programs from ABPN,ACGME,UCNS, and the Health Care Provider Taxonomy Code Set”
CMS January 1,2010: A new patient is “…a patient who has not received any professional services (E/M or other face-to-face service) within the previous 3 years”
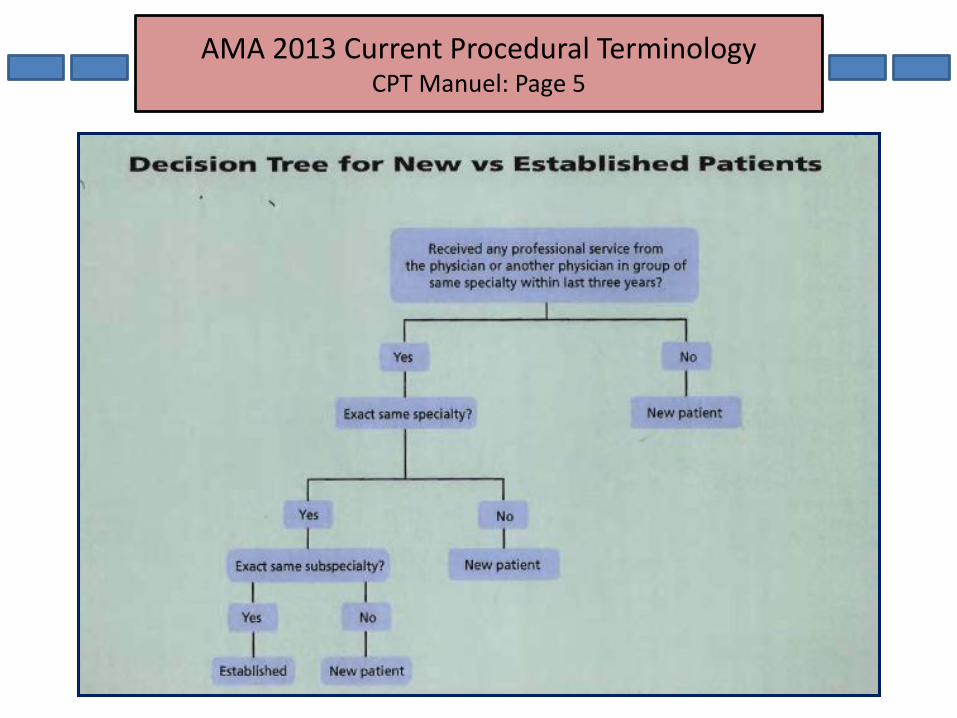
AMA 2013 Current Procedural TerminologyCPT Manuel: Page 5
New Patient or Established Patient
CPT 2012 states: “A new patient is one who has not received any professional services from the physician or another physician of the exact same specialty and subspecialty who belongs to the same group practice, within the past three years”
AAN Policy Aug 14, 2012: “Neurologists of a different subspecialty who see a patient within 3 years of another Neurologist in the same group should report the new patient E/M Code for that visit”
CMS 2012 states: “CMS claims processing systems do not recognize physician subspecialties’. “Therefore, CMSs instructions for billing new and established E/M codes has not changed for 2012”
If an on call physician is covering for another physician, the patient’s encounter will be classified as it would have been by the physician who
is not available; including an ED encounter.
Non-Medicare payers generally follow Medicare guidelines.
Three New Chronic Care Coordination Codes“CCCC” Codes 2013
99487
First hour of clinical staff time directed by a physician or other qualified health
care professional with no face-to-face visit, per calendar month
99488
First hour of clinical staff time directed by a physician or other qualified health
care professional with one face-to-face visit, per calendar month
99489
Each additional 30 minutes of clinical staff time directed by a physician or
other qualified health care professional, per calendar month
List separately in addition to code for primary procedure.
Created to coordinate different services and medical specialties to manage the
complex chronically ill patient
Medicare considers the new CPT CCCC codes Bundled Services and will not reimburse for these codes
Chronic Care Coordination Care Codes“CCCC” Codes 2013
Created to coordinate different services and medical specialties need to manage the complex nature of the patient’s medical condition, psychosocial needs and activities of daily living; e.g... Chronic Daily Headache and Alzheimer's patients.
If reimbursed by private carriers, these codes will typically require the coordination of a number of specialists and services, and will typically involve patients with one or more chronic conditions or episodic health conditions
Medicare considers the new CPT “CCCC” codes “…Bundled Services…” and will not reimburse for these codes
New Transition Care Management Service Codes“TCM’ Codes
99495
Communication (direct contact, telephone ,electronic) with the patient
and/or caregiver within 2 business days of discharge.
MDM of least moderate complexity during the service period.
Face-to-face visit, within 14 calendar days of discharge.
99496
Communication (direct contact, telephone, electronic) with the patient
and/or caregiver within 2 business days of discharge.
MDM of high complexity during the service period.
Face-to-face visit, within 7 calendar days of discharge.
Transitional Care Management Service Codes“TCM” Codes
TCM Codes created to report services for an established patient whose medical and/or psychosocial problems require moderate or high complexity MDM during transitions in care
Reimbursements: Based on 2013 Conversion Factor and RVUs
99495 performed in non-facility (e.g. doctor’s office): ±$164.00
Compared to 999214 (3.13 RVUs): $106.59
99495 performed in facility: ±$135.00
99496 performed in non- facility (e.g. doctor’s office): ±$231.12
99496 performed in facility: $197.76
Approved by CMS and available January 13
Chemodenervation for Chronic Migraine
CPT code 64615:
Available as of 1/1/13 for chemodenervation with Onabotulinumtoxin A to treat Chronic Migraine
Phase 3 Research Evaluating Migraine Prophylaxis Therapy (PREEMT)
▫ Defined appropriate patient selection, injection sites, dosages and technique
▫ A combination of 31 FSFD (fixed-site, fixed dose) and FTP (follow-the-pain) injection protocol was found to be most optimal
▫ Minimum dose of 155 U of Botox administered across 7 specific head/neck muscles
▫ An additional 40 U of Botox could be administered at physician’s discretion using FTP strategy up to max of 195 U administered to 39 sites
▫ Protocol was repeated q. 12 weeks up to 5 treatment cycles
Chemodenervation for Chronic Migraine
▫ The Physician/Practice expense for Botox:$5.25/Unit or $525 for a 100 U vial
▫ Currently Medicare allows $5.48/U or $548 per vial▫ In Dallas, private insurers pay as an average between $5.52/U to $7.00/U▫ The medication “J code” for Botox is J0585▫ PREEMT criterion defines bilateral injections▫ The injection fees vary but are often in the $445-$495 range
An average reimbursement from private carriers ranges ± $180-$280
OnabotulinumtoxinA Reimbursement Website: www.botgoxreimbursement.us
Additional onabotulinumtoxinA Codes64612: Cervical64613: Spinal61614: Extremity
Bundled Payments for Care Improvement InitiativeBPCII: Introduced by CMS April 23, 2011
Reimbursement model where fees of multiple providers are bundled into a single, comprehensive payment that covers all of
the services involved in the patient’s care
Fee-For-Service:
Puts the full insurance risk on the payer
Capitation:
Puts the full insurance risk on the provider
Bundled Payments:
Requires providers to bear more of the financial responsibility for outcomes
Bundled Payments
Bundled payments
Will need to have some type of integrated delivery system consisting of an administrative structure to determine the patient needs and how much each provider should be
reimbursed for care.
ACOs
Are being considered one such entity to manage bundled payments on behalf of its providers plus develop collaborative and contractual relationships with
facilities such as hospitals in providing patient
care coordination
Bundled Payments
CMS outlined 4 models of Bundled Payments:First 3 Models are retrospective; Model 4 is prospective
For Models 2 & 3, there is shared savings for profit beyond target price
Model 1:For inpatient stay in a general acute care hospital
Model 2:Inpatient stay & post hospital care, ending 30 to 90 days after discharge
Model 3: From discharge as a hospital inpatient, ending no sooner than 30 days after discharge
Model 4:CMS would make a bundled payment to the hospital, which would pay physicians
and other health care providers involved in the episode of care instead of them making individual Medicare claims.
Bundled Payments10 Concerns and Operational Design Issues for Neurologists
1. Are Neurologists willing to have a hospital be in charge of administering their reimbursements?
2. Are Neurologists willing to develop an equitable agreed upon fee for both the hospital and the physician group?
3. How will bundled payments be divided among various physicians? Who will make that decision?
4. Will Neurologists be willing to make an expensive investment in a new contracting and claims infrastructure to handle the new payment model?
5. Will bundling with hospitals require an integrated health care system?6. Will bundling with hospitals require having Neurohospitalists in the hospital?7. In the absence of Neurohospitalists, would a general Neurology practice be
expected to provide Neurohospitalists services?8. Would Neurology services be more consultative with the Medical Home physician
with less direct patient contact?9. Given the proposed shortage of Neurologists, would Neurology be subsidized?10. Would a Neurologists salary be tied to productivity?
Billing and Coding in Neurology and Headache
Aristotle (384 B.C—322B.C)
“Good decisions come from experience, and experience comes from bad decisions”.
Neurology 2013:
One bad decision which alters a physician’s existing practice organizational model could be catastrophic





























