Embed Size (px)
Citation preview
STRUCTURAL NEUROPATHOLOGY OF
CEREBRAL INJURY
Pathophysiology of Traumatic Brain Injury
Traumatic brain injury (TBI) is a nondegenerative, noncongenital insult to the brain from an external mechanical force, possibly leading to permanent or temporary impairment of cognitive, physical, and psychosocial functions, with an associated diminished or altered state of consciousness (Dawodu, 2009).
TBI can manifest clinically from concussion to coma and death.
Acute TBI is characterized by two injury phases, primary and secondary.

Phases of Injury
Tissue disruption from the primary injury is usually permanent, and does not respond to pharmacologic or physiologic manipulations.
Extensive primary injury presupposes a poor outcome, regardless of medical and rehabilitative therapy and frequently constitutes the limiting factor for the most idea recovery.
The series of biochemical processes associated with primary injury result in secondary brain injury.
The primary aim for the acute management of TBI is to limit the secondary injury.
Phases of Injury
The secondary brain injury is caused by a dynamic interplay between ischemic, inflammatory and cytotoxic processes (Veenith, Goon, & Burnstein, 2009).
There is a complex cascade of cellular inflammatory response following TBI which propagates secondary brain damage.
This inflammatory process lasts from hours to days contributing continuously to secondary brain damage.
The inflammatory response resulting from an acute TBI is not limited to the brain and multiple organ dysfunction syndromes are commonly seen.

Phase of Injury
The primary insult also results in an immediate disturbance of the cerebral circulation, resulting in cerebral ischemia.
Cerebral ischemia contributes significantly to about 90% of deaths after closed head injuries.
Ischemic brain damage is perpetuated by factors such as hypotension, hypoxia, raised intracranial pressure, edema, focal tissue compression, damage to the microvasculature, and in late phases, vasospasm in the remaining vessels.
Injury Sequence
The time sequence after TBI can be arbitrarily divided into three phases associated with marked regional variations in cerebral blood flow:o Phase 1--immediate, rupture of cellular and vascular
membranes, release of intracellular contents, shearing and stretching, hypoperfusion, and disrupted metabolism;
o Phase 2--intermediate (days 1-3), interplay between ischemia, inflammatory, and cytotoxic processes, promoting necrosis and apoptosis; and
o Phase 3--late (days 4-15), when vasospasm can be seen with a marked reduction in blood flow.

Mechanisms of Brain Injury
The physical mechanisms of brain injury result from dynamic or static loading.
Dynamic loading generally occurs in a much faster time frame (less than 50 ms) than static loading.
Static or quasi-static loading occurs when the effect of speed of occurrence is not significant.
Static loading is rare but can occur if a slow moving object traps the head against a rigid structure and slowly squeezes the skull to produce numerous comminuted fractures of the cranial vault which may be sufficient to deform the brain.

Mechanisms of Brain Injury
Dynamic loading is the mechanical force that is most commonly associated with the sequelae following TBI.
Dynamic loading can be further classified as either impact or impulsive (Graham et al., 2000; McIntosh et al., 1996).
Impact loading occurs when there is a collision of the head with a solid object at a tangible speed, e.g., skull versus a rigid surface; blunt object striking the head.
Impulsive or inertial loading occurs when there is sudden motion of the head without significant physical contact, e.g., whiplash, shaking baby.

Mechanisms of Brain Injury
Impulsive loading can occur when the head is set into motion as a result of impact to the body in another area (McIntosh et al., 1996), or when a moving head is suddenly stopped, either without it striking anything or by contact with an object.
Contact force occurs when there is physical interaction between the head and an object or between the head and the ground.
Inertial force occurs when the head is set in motion with or without any contact force, leading to acceleration of the head.

Mechanisms of Brain Injury
We can have a pure contact event with no resulting inertial event and we can have pure inertial events with no resulting contact force.
An example of a pure contact event is a person lying down with head constrained/supported by the ground and someone hits that person’s head with a baseball bat.
An example of a pure inertial event is the occupant of an automobile sustaining a whiplash of the head on the neck without contacting the seat or headrest.
Mechanical Force and Brain Tissue Injury
Most TBIs, however, are the result of a combination of contact and inertial forces: forces involving the head striking or being struck by something (impact loading) and movement of the brain within the skull (inertial loading).
For example, a bar patron is punched in the side of the head (contact force) and the head accelerates along the direction of the force (inertial force).
Contact and/or inertial forces may strain the brain tissue beyond its structural tolerance, leading to focal (contact force) or diffuse (inertial force) injury.

Mechanical Force and Brain Tissue Injury
Strain is the amount of tissue deformation caused by an applied mechanical force.
The three basic types of tissue deformation areo Compressive-tissue compressiono Tensile-tissue stretching ando Shear-tissue distortion produced when tissue
slides over other tissue The type, direction, intensity, and duration of
forces all contribute to the characteristics and severity TBI.
Motion and Brain Injury
Head injury typically results from either a direct impact to the head or from an indirect impact applied to the head and neck when the torso is stopped or accelerated rapidly.
Acceleration is a change in velocity over time. In the case of the head or body, it can speed
up, slow down, or merely change direction at a constant speed depending upon impact and/or inertial loading.

Motion and Brain Injury
Acceleration that passes through the body’s center of gravity resulting in linear motion is termed translational acceleration.
Acceleration that results in pivoting or angular motion of the body about its geometric or inertial center is termed angular acceleration.

Motion and Brain Injury
Most impact forces are unpaired and produce combined rotational and linear motions, or curvilinear motion.
The observed cranial movement is always a combination of both translation and rotation.
Some degree of rotation always occurs around the foramen magnum, because of the how the head is attached to the cervical spine.

Motion and Brain Injury
In either case, the head sustains combined linear and angular acceleration—the two major mechanisms of head injury.
Impact loading by head contact results in predominantly linear acceleration and inertial loading of the head results in predominantly rotational acceleration.
The traumatized brain always includes inseparable markings of both translational and rotational trauma.

Skull-Brain Interface
The frontal lobes sit in the anterior fossa of the cranial cavity region of the skull.
The anterior lateral aspects of the frontal bone swing around each of the frontal lobes, encapsulating them.
Skull-Brain Interface
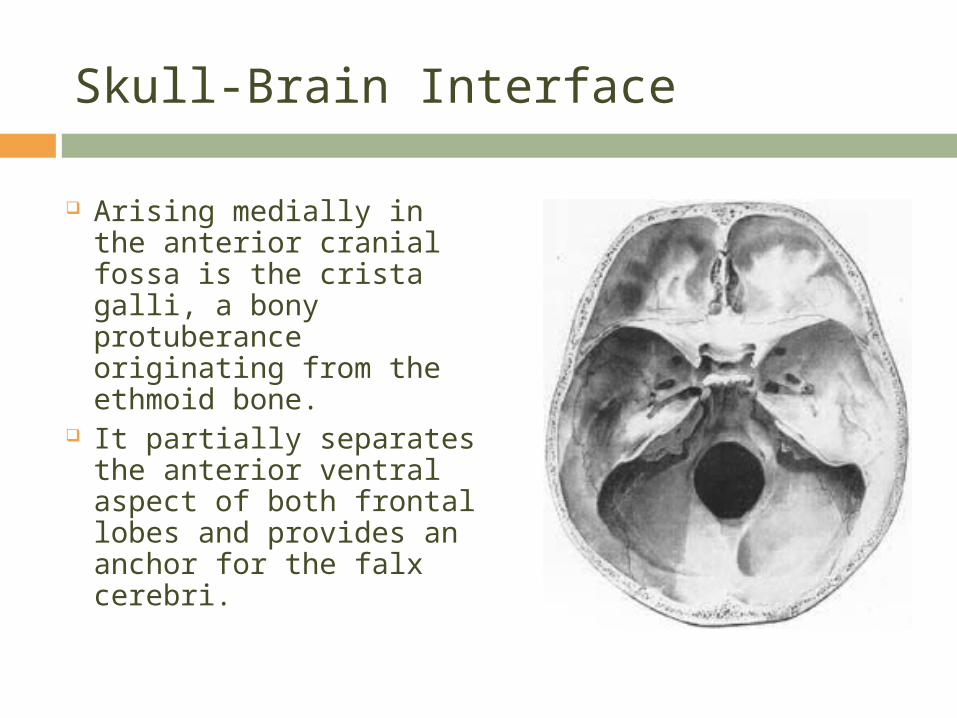
Arising medially in the anterior cranial fossa is the crista galli, a bony protuberance originating from the ethmoid bone.
It partially separates the anterior ventral aspect of both frontal lobes and provides an anchor for the falx cerebri.
Skull-Brain Interface
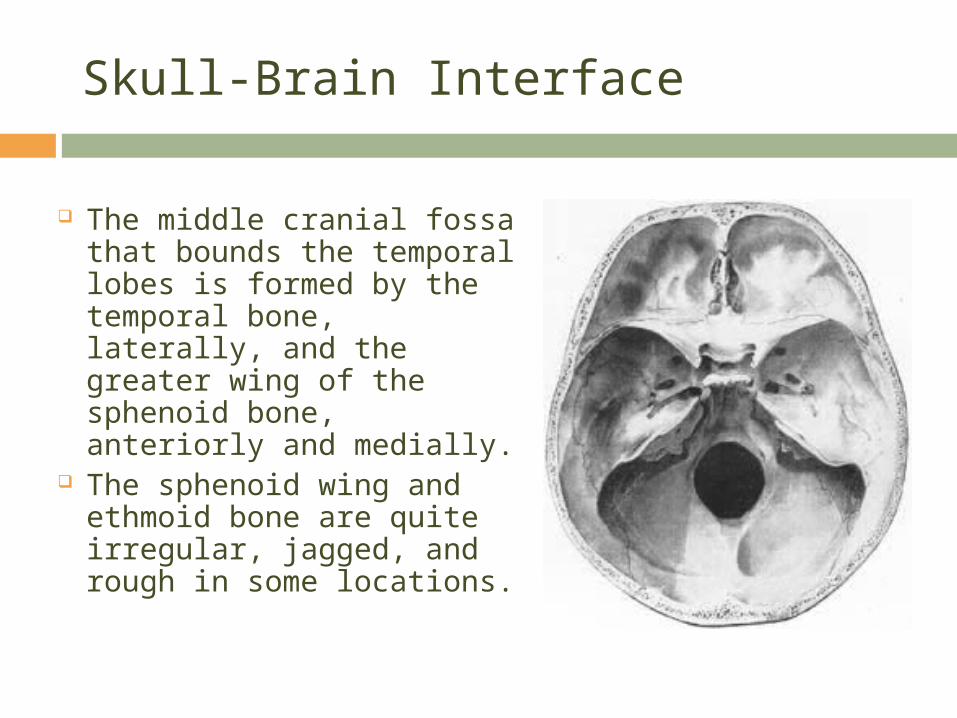
The middle cranial fossa that bounds the temporal lobes is formed by the temporal bone, laterally, and the greater wing of the sphenoid bone, anteriorly and medially.
The sphenoid wing and ethmoid bone are quite irregular, jagged, and rough in some locations.
Translational Trauma
The majority of CHIs involve acceleration dependent mechanisms.
Whether through impact or inertial loading, whenever the head accelerates rapidly forward, there is differential movement of the skull and brain.
The skull does not need to strike an object in order for the brain to get injured.
Take for example a rear-end motor vehicle collision in which the force is transmitted through the car and the occupants of the car begin to move forward.

Translational Trauma
The head accelerates, but movement of the brain lags behind that of the skull because the brain is buoyed by cerebrospinal fluid and remains fairly stationary due to the meninges attachment to the skull.
Even if the skull does not hit the dashboard, windshield, steering wheel, or window, the neck will reach the end point of moving forward (hyperflexion), and with that rapid deceleration of the head, the brain continues forward hitting into the interior structure of the skull.
Translational Trauma
Contact sports can also produce inertial loading with cervical acceleration/ deceleration injury, or CAD.
The unsupported head can be suddenly forced into hyperflexion and/or hyperextension.
During its movement transit, the delicate cortex is rubbed against the sharp dural edges of the falx, the sphenoid ridge, and the jagged floor of the anterior cranial fossa.
The surface of the soft brain, especially the crowns of gyri, is easily contused (bruised) and lacerated by these hard bony ridges.
Translational Trauma
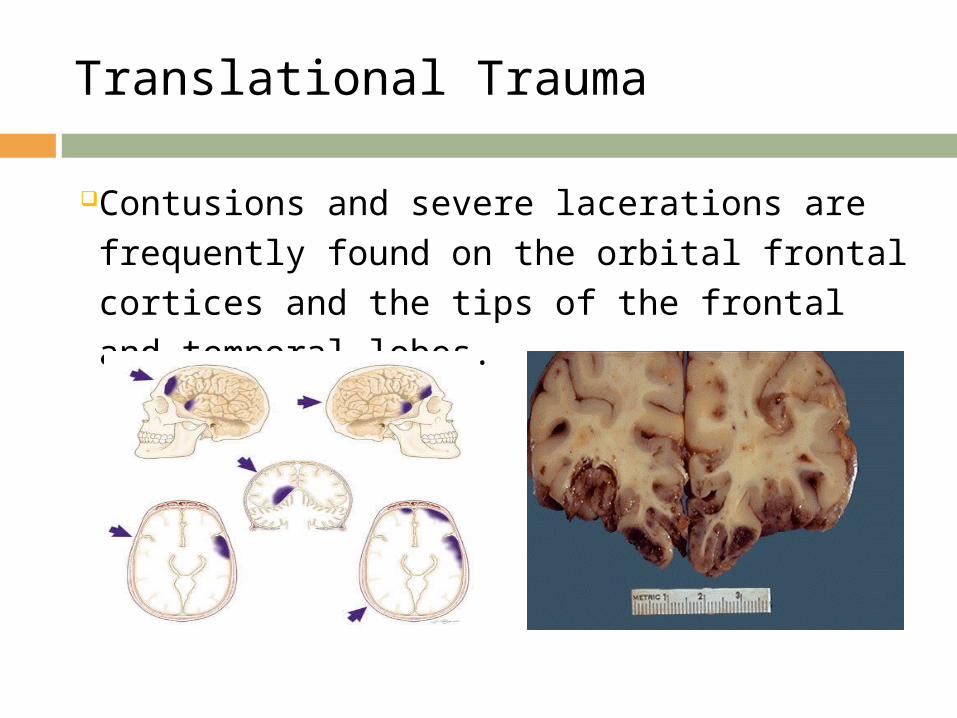
Contusions and severe lacerations are frequently found on the orbital frontal cortices and the tips of the frontal and temporal lobes.
Translational Trauma
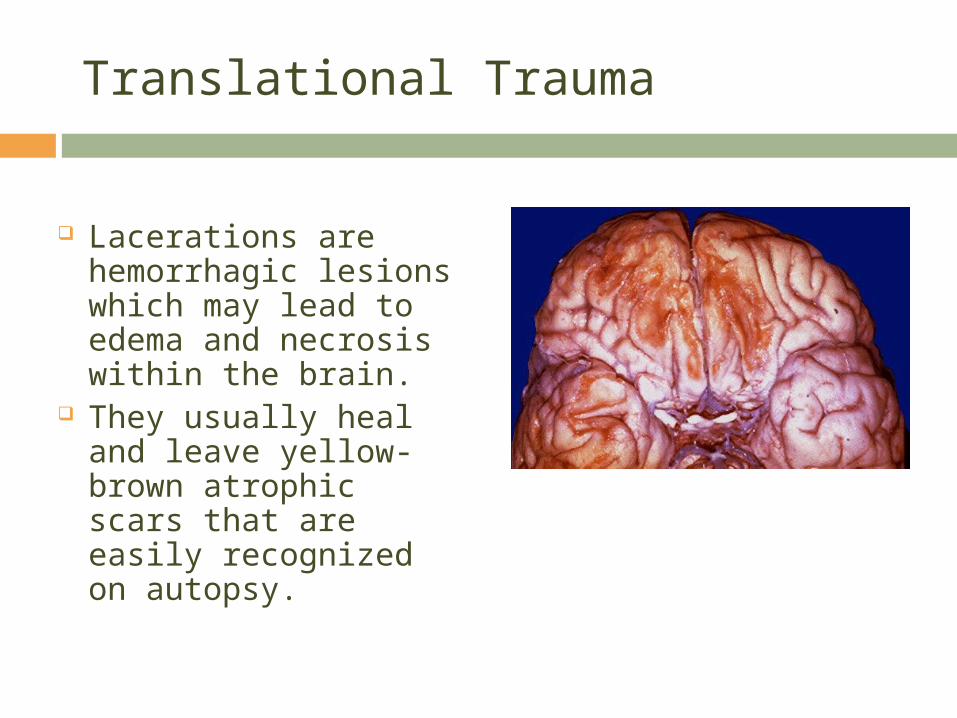
Lacerations are hemorrhagic lesions which may lead to edema and necrosis within the brain.
They usually heal and leave yellow-brown atrophic scars that are easily recognized on autopsy.
Translational Trauma
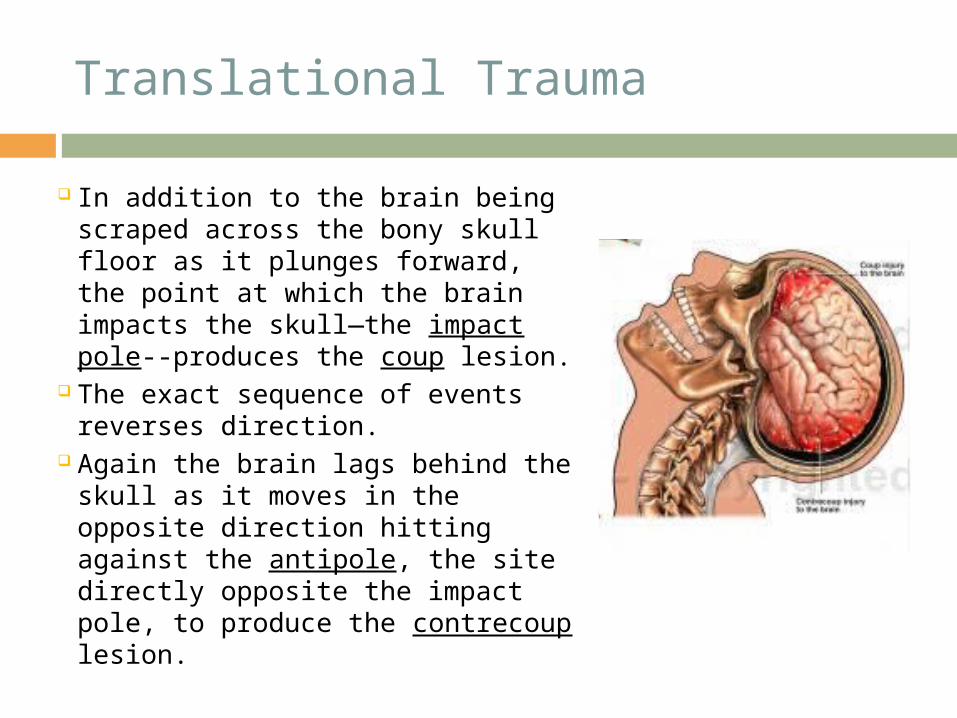
In addition to the brain being scraped across the bony skull floor as it plunges forward, the point at which the brain impacts the skull—the impact pole--produces the coup lesion.
The exact sequence of events reverses direction.
Again the brain lags behind the skull as it moves in the opposite direction hitting against the antipole, the site directly opposite the impact pole, to produce the contrecoup lesion.
Translational Trauma
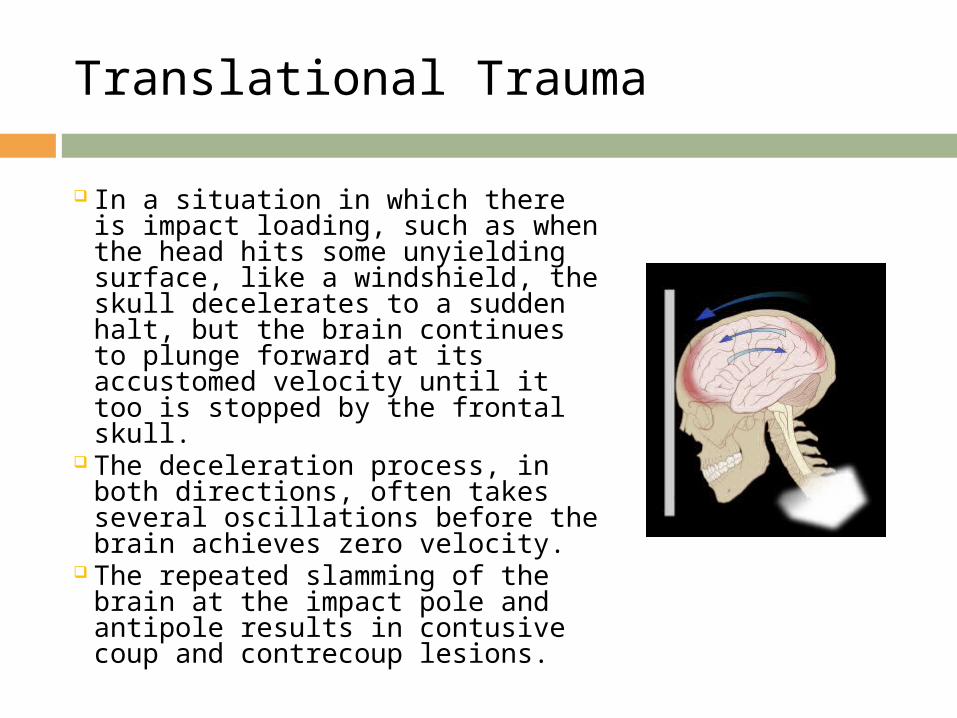
In a situation in which there is impact loading, such as when the head hits some unyielding surface, like a windshield, the skull decelerates to a sudden halt, but the brain continues to plunge forward at its accustomed velocity until it too is stopped by the frontal skull.
The deceleration process, in both directions, often takes several oscillations before the brain achieves zero velocity.
The repeated slamming of the brain at the impact pole and antipole results in contusive coup and contrecoup lesions.
Translational Trauma
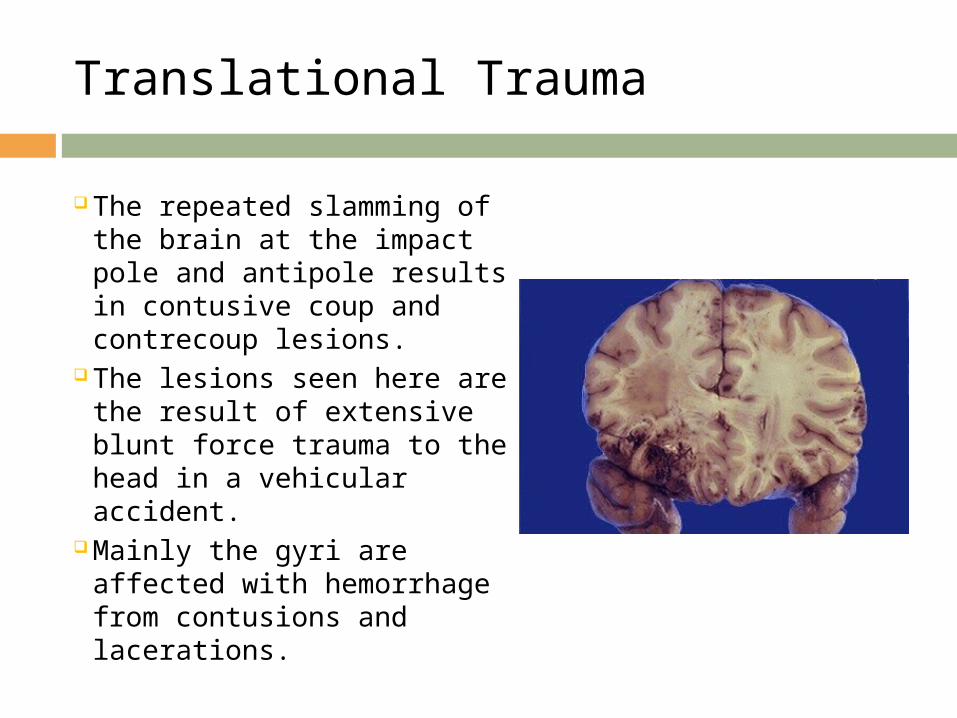
The repeated slamming of the brain at the impact pole and antipole results in contusive coup and contrecoup lesions.
The lesions seen here are the result of extensive blunt force trauma to the head in a vehicular accident.
Mainly the gyri are affected with hemorrhage from contusions and lacerations.
Translational Trauma
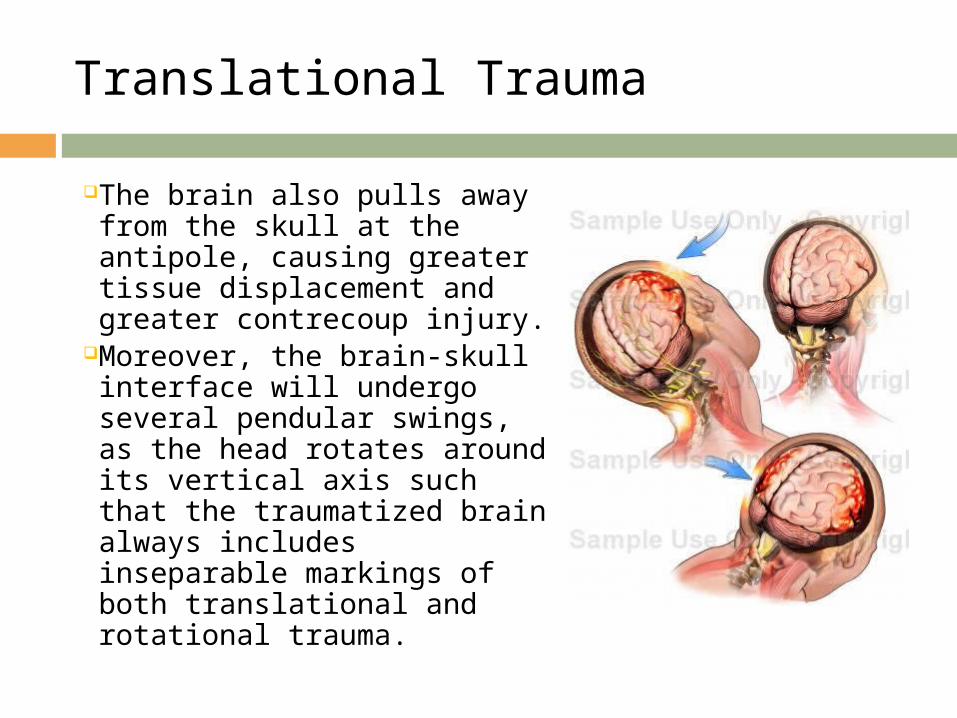
The brain also pulls away from the skull at the antipole, causing greater tissue displacement and greater contrecoup injury.
Moreover, the brain-skull interface will undergo several pendular swings, as the head rotates around its vertical axis such that the traumatized brain always includes inseparable markings of both translational and rotational trauma.

Rotational Trauma
Rotational trauma depends on shearing strain—the displacement of one point relative to another as a consequence of the stress per unit area.
During angular acceleration of the head, as the head rotates around its vertical axis, the brain will initially remain stationary while the skull rotates.
Eventually, the brain is dragged along by friction forces over the bony prominences of the anterior and middle fossa floors.
Rotational Trauma
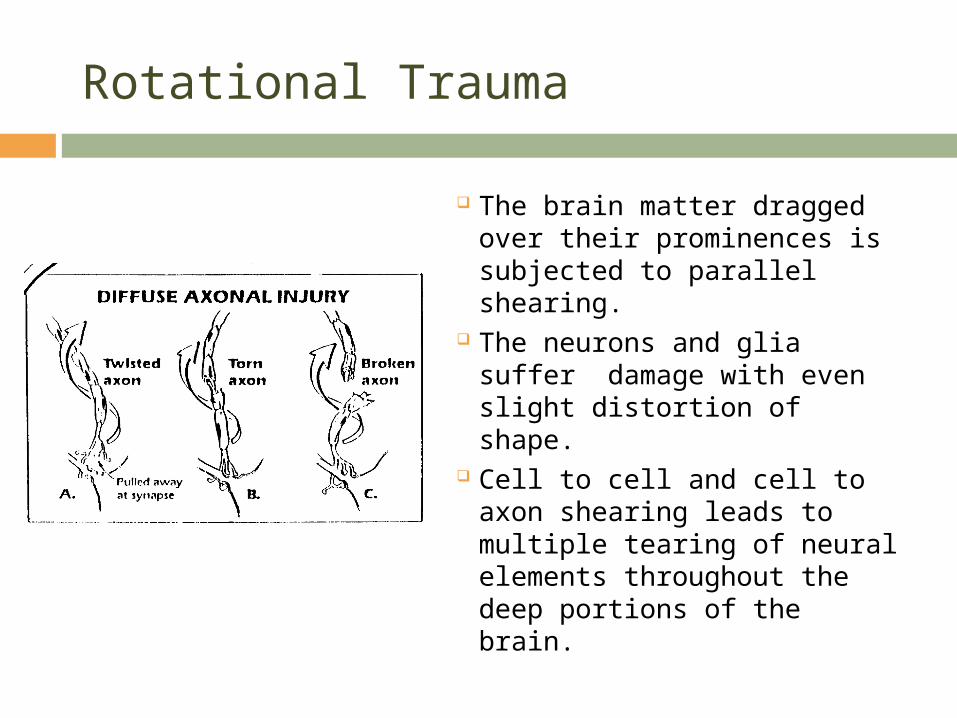
The brain matter dragged over their prominences is subjected to parallel shearing.
The neurons and glia suffer damage with even slight distortion of shape.
Cell to cell and cell to axon shearing leads to multiple tearing of neural elements throughout the deep portions of the brain.

Diffuse Axonal Injury
Diffuse axonal injuries
result when shearing, stretching, and/or angular forces pull on axons and small vessels.
Impaired axonal transport leads to focal axonal swelling and (after several hours) may result in axonal disconnection.

Shearing Lesions
Shearing lesions have a predilection for corticomedullary
(gray matter-white matter) junctions (particularly in the frontal and temporal areas), around the basal ganglia, deep gray matter, internal capsule, the ventricles, the superior cerebellar peduncles, the corpus callosum, and the fiber tracts of the brainstem.
The most common neuropathological consequence is damage to the hippocampus and other medial temporal lobe limbic structures, resulting in post-traumatic memory disorder and emotional behavior changes.

Non-Acceleration Dependent Mechanisms
Clinical head injuries not involving acceleration of the skull are rare.
A typical example is the car mechanic lying in the grease pit when the car falls on his supported head.
A less “pure” example is the individual whose head is hit directly on the vertex by a falling object.
In both cases, there is no head movement, and the energy is usually diffuse causing extensive fractures but little brain injury.
Impression Trauma
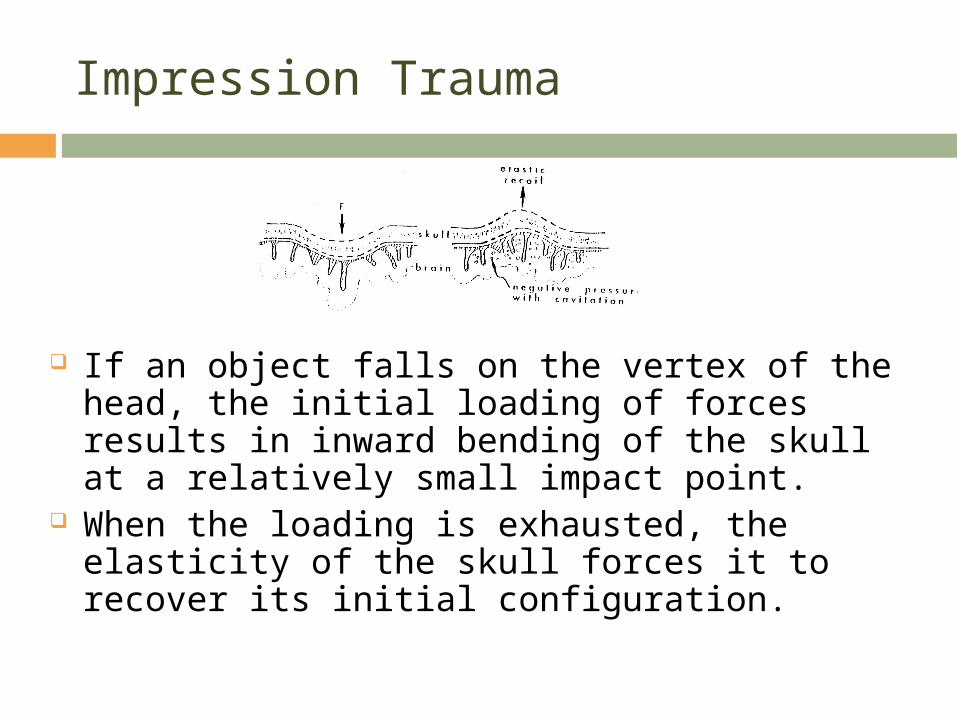
If an object falls on the vertex of the head, the initial loading of forces results in inward bending of the skull at a relatively small impact point.
When the loading is exhausted, the elasticity of the skull forces it to recover its initial configuration.
Impression Trauma
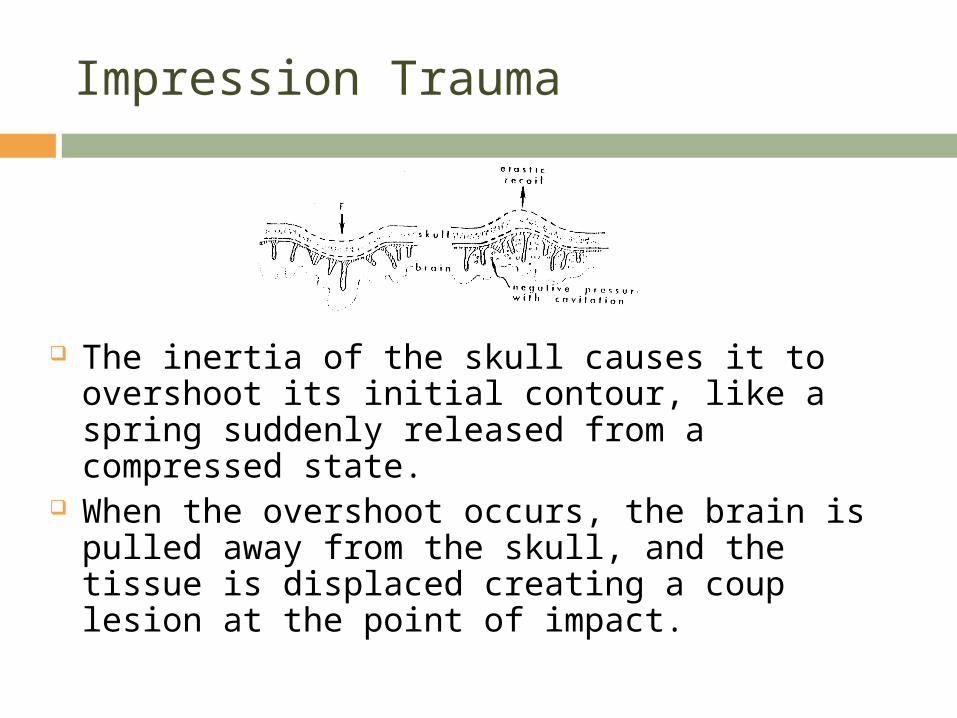
The inertia of the skull causes it to overshoot its initial contour, like a spring suddenly released from a compressed state.
When the overshoot occurs, the brain is pulled away from the skull, and the tissue is displaced creating a coup lesion at the point of impact.
Ellipsoidal Deformation
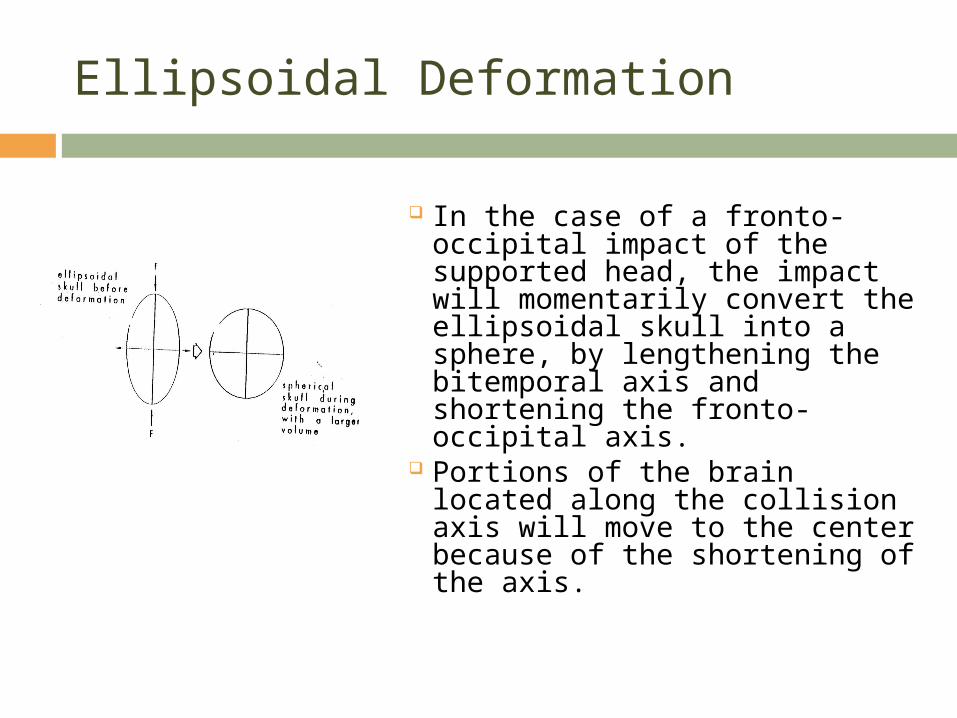
In the case of a fronto-occipital impact of the supported head, the impact will momentarily convert the ellipsoidal skull into a sphere, by lengthening the bitemporal axis and shortening the fronto-occipital axis.
Portions of the brain located along the collision axis will move to the center because of the shortening of the axis.
Ellipsoidal Deformation
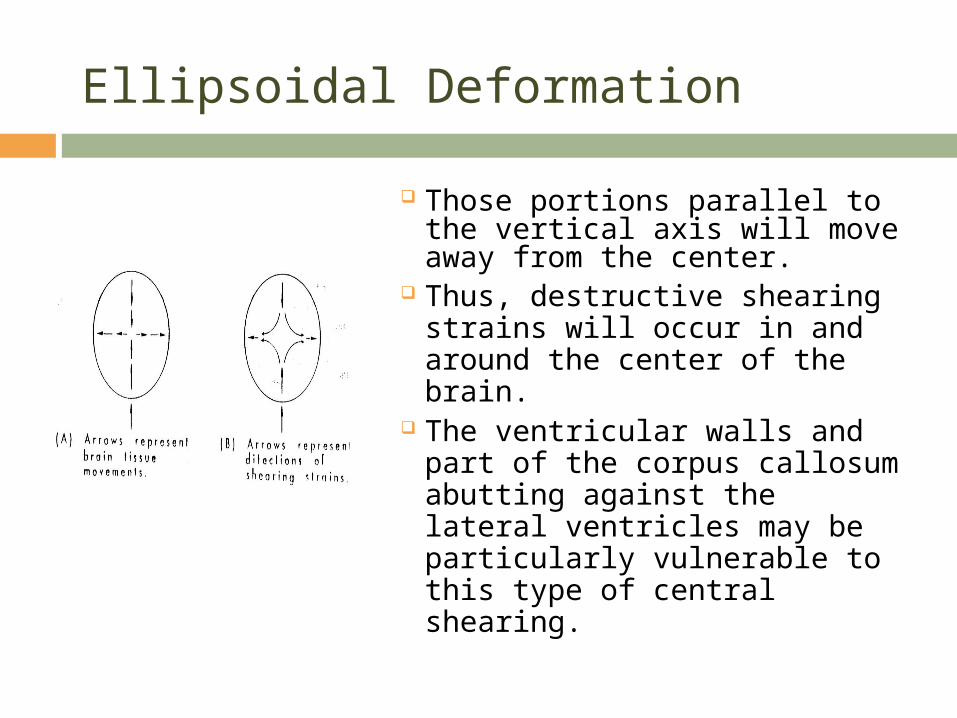
Those portions parallel to the vertical axis will move away from the center.
Thus, destructive shearing strains will occur in and around the center of the brain.
The ventricular walls and part of the corpus callosum abutting against the lateral ventricles may be particularly vulnerable to this type of central shearing.

Blast Injuries
As of October 2005, improvised explosive devices (IEDs) have accounted for one third of all American deaths in Iraq.
In 2005, the US military invested $3.3 billion in IED countermeasures, primarily through improved armor and other technologies.
Blast injuries result from multifactorial mechanisms.o primary effects—those resulting from the crushing
effects of blast overpressure, or direct exposure to an overpressurization wave with a velocity >/=300 m/sec (speed of sound in air);
Blast Injuries
o secondary effects—those resulting from the impact, penetrating and nonpenetrating, of debris accelerated by the blast wave;
o tertiary effects—those resulting from displacement of the person by the blast and impact with walls and the ground caused by accelerating the body itself; and
o quaternary effects--burns/inhalation of gases/toxic fumes and crush injuries.
Primary Effects
The changes in atmospheric pressure that cause primary blast injuries arise because a high-explosive detonation results from the nearly instantaneous conversion of a solid or liquid into gasses.
Momentarily these gasses occupy the same volume as the parent solid or liquid and thus they are under extremely high pressure.
Extreme pressure differences occur as the blast wave reaches the body, resulting in both stress and shear waves.

Blast Pressure Wave
At the instantaneous conversion of a solid/liquid into gasses, the gasses expand rapidly, causing compression in the surrounding air, forming a pulse of pressure (blast overpressure, positive phase of the blast wave).
As the gasses continue to expand, the pressure drops, creating a relative vacuum (blast underpressure, negative phase of the blast wave).
Blast Pressure Wave
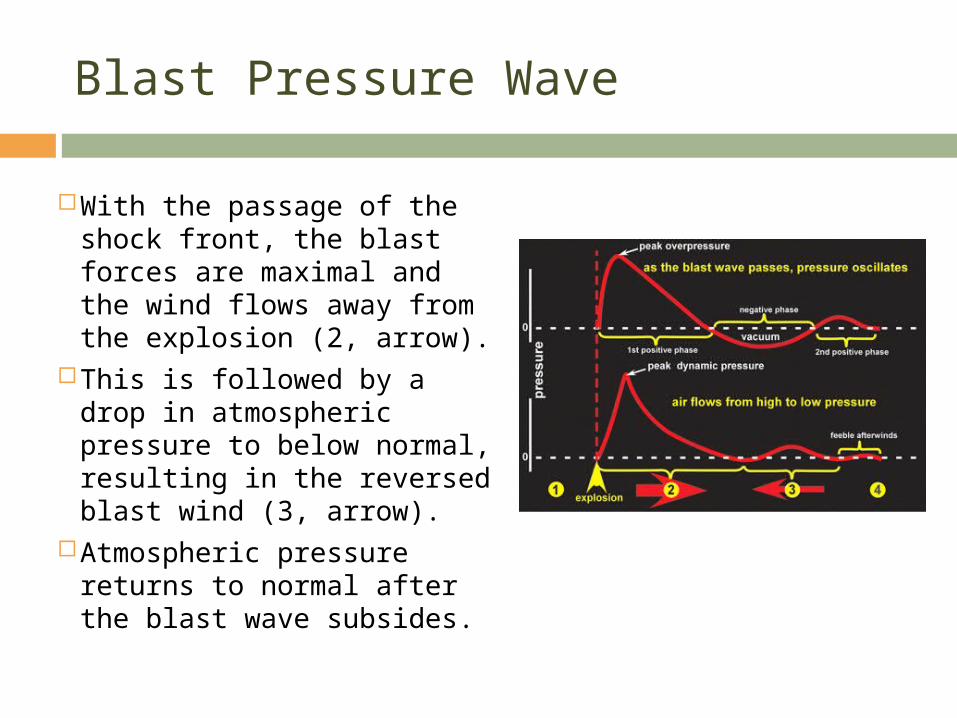
With the passage of the shock front, the blast forces are maximal and the wind flows away from the explosion (2, arrow).
This is followed by a drop in atmospheric pressure to below normal, resulting in the reversed blast wind (3, arrow).
Atmospheric pressure returns to normal after the blast wave subsides.

Barotrauma
The violent consequences of being near an explosion can produce a wide range of injuries.
Blast wave-induced changes in atmospheric pressure create barotrauma.
The high pressures of the blast can crush the body and cause internal injury.
Organs and tissues of different densities are accelerated at different relative rates, resulting in displacement, stretching and shearing forces.

Barotrauma
The most vulnerable parts of the body to primary blast injury are considered to be those with air-fluid interfaces, particularly the lungs, bowel, and middle ear.
Rupture of the tympanic membrane is the most frequent injury.
Injuries that result from crushing overpressure, however, are truly unique to blast.
These primary blast injuries occur because the body is not a solid, incompressible mass; it has air-containing organs that will crush under the external load.
Barotrauma
Crushing allows the outer shell of the body in those regions to move rapidly inward, thus distorting the air-containing tissue and producing local, large stresses.
Injuries to the lung, gastrointestinal (GI) tract, and upper respiratory tract (URT) are common manifestations of this effect.
Rapid distortion of the air-containing organs can transmit stress to neighboring solid organs as well.
Contusions to the heart, for example, arise in part from the strong stress waves that develop in the lung.
Barotrauma
Large deformations of the body can also lead to stresses in solid organs that result in damage (e.g., liver and spleen lacerations).
Finally, rapid volumetric changes outside the normal physiological range can disrupt systemic processes.
Creation of air emboli by forcing gas across the air–blood barrier of the lung and creation of large pressure transients in the vascular system may be responsible for brain injury and cell death.
Ballistic Trauma
Both the blast wave and blast wind can propel objects with considerable force, causing secondary and tertiary blast injuries.
Strong winds behind the blast front can hurl fragments and debris against the body and cause the same blunt trauma or penetration injuries that would occur if the material were propelled by other means.
Secondary blast injury, or ballistic trauma, results from objects put in motion by the blast wind impacting a person.

Tertiary and Quaternary Trauma
Tertiary blast injury results from a person being blown into solid objects by the blast wind.
The strong winds behind the blast front and the pressure gradient in the wave can exert significant forces that can accelerate the body and cause the same blunt trauma that would occur in a fall or a car crash.
The extreme heat and light released by the explosion can cause burning and blindness, whereas inhaling the toxic fire gases can lead to immediate incapacitation or delayed lethality.

Collateral Injury
Finally, any of these traumas can lead to subsequent effects caused by disruption of the body’s biochemical or neurological system.
Although blast provides a unique process by which projectiles are propelled, bodies are accelerated, and trauma is caused, the resulting secondary injuries and sequelae can also result from other traumatic events.
Categories of Brain Injury
You’ll recall that acute TBI is characterized by two injury phases, primary and secondary.
Primary injury in TBI results from local mechanical stresses in the brain that disrupt neural cells and tissues.
In animal models with impact trauma, primary tissue injury has been observed in endothelial cells, in axons, and in cortical astrocytes and neurons.
CHI typically gives rise to contusions and lacerations on or within the surface of the brain.
Lacerations are lesions that break the pia mater; contusions leave the pia mater intact.
Primary Impact Damage
Lacerations are usually found on the superficial crests of the gyri of the cerebral hemispheres, but they may penetrate the whole thickness of the cortex and extend into the subcortical white matter.
Potential sites for cerebral contusion following CHI include:o Site of impact;o Sites diametrically opposite site of impact;o Frontal and temporal lobe crests; ando Surface lesions of the upper borders of the
hemispheres.
Secondary Injury
Secondary injury occurs as a result of epiphenomena causally related to the primary injury.
Impact disruption of large dural or cortical vessels often lead to epidural or subdural hematomas.
Disruption of capillaries or disturbance of vascular endothelial membranes during the original impact may lead to vasogenic cerebral edema.
As both hematoma and edema constitute mass effect, they raise intracranial pressure and may result in brain shift and cerebral hypoperfusion.

Secondary Injury
Brain herniations represent shift of the normal brain through or across regions to another site due to mass effect.
Hypoperfusion and herniation lead to further brain damage in the form of pressure necrosis and infarction, often remote from the site of the primary injury.
Secondary lesions, unlike primary ones, are potentially avoidable if they are caught quickly and amenable to treatment, such as surgical evacuation of hematoma and edema therapy.
Herniation
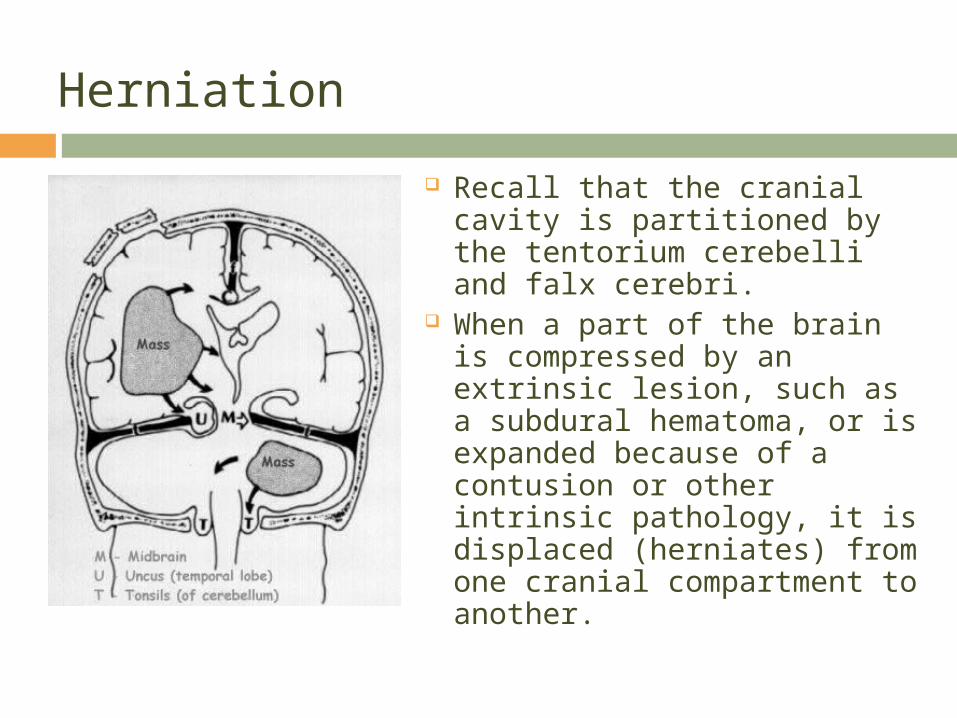
Recall that the cranial cavity is partitioned by the tentorium cerebelli and falx cerebri.
When a part of the brain is compressed by an extrinsic lesion, such as a subdural hematoma, or is expanded because of a contusion or other intrinsic pathology, it is displaced (herniates) from one cranial compartment to another.

Herniation
Three major herniations can occur, either alone or in combination.
Subfalcial herniation is displacement of the cingulate gyrus from one hemisphere to the other, under the falx cerebri.
The left cingulate gyrus has herniated under the falx.

Herniation
Uncal (transtentorial) herniation is herniation of the medial temporal lobe from the middle into the posterior fossa, across the tentorial notch.
The uncus of the temporal lobe is forced into the gap between the midbrain and the tentorium.
shift of the uncus into the suprasellar cistern as well as a subfalcine shift to the right.
Herniation
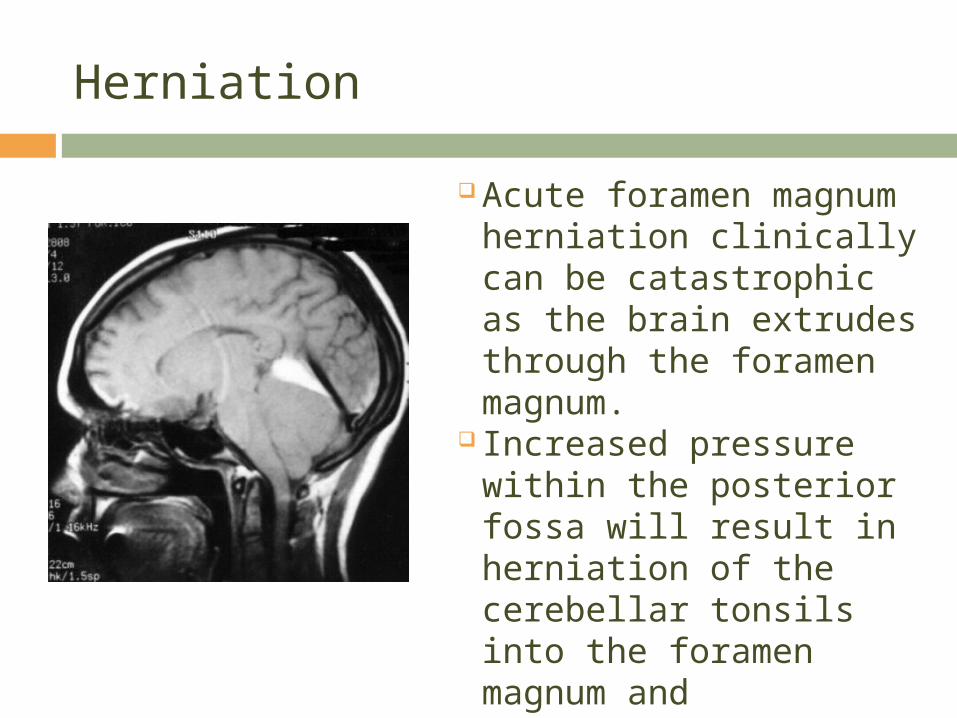
Acute foramen magnum
herniation clinically can be catastrophic as the brain extrudes through the foramen magnum.
Increased pressure within the posterior fossa will result in herniation of the cerebellar tonsils into the foramen magnum and compression of the medulla.

Secondary Injury
The structural disruption to the neural cells and tissues from primary injury creates a secondary cascade that may lead to functional disruption through metabolic and biochemical processes.
Following TBI, two different types of cells are visible; type 1cells, that show a classic necrotic pattern following the primary injury, and Type 2 cells, that show a classic apoptotic pattern on microscopy.
Apoptosis, also referred to as programmed cell death, is now recognized as an important factor in secondary brain injury.

Secondary Injury
Cells undergoing apoptosis die without membrane rupture and therefore elicit less inflammatory reactions in contrast to the cells undergoing necrosis.
Neuronal apoptosis after TBI is hypothesized to be a protective response by the brain to remove injured tissue cells while having little effect on remaining brain tissue.
Apoptotic cells have been identified within contusions in the acute post-traumatic period, and in regions remote from the site of injury days and weeks after trauma.

Secondary Effects of Blast Injury
Evidence of ultrastructural and functional changes following blast neurotrauma has also been observed.
In addition to tension and shear-induced cellular injury, there is also evidence of cellular damage from direct pressure effects.
The blast-induced primary mechanical damage to cellular structures starts a secondary cascade of effects, including ion channel disruption, apoptosis, and necrosis.
In blast animal models, astrocyte and micro-glial responses have been seen as well as changes in apoptotic mechanisms.
Histological studies have detected degenerating neurons in the cerebral cortex and hippocampus of rats 1 and 5 days after blast exposure.
Secondary Effects of Blast Injury
Acceleration of the brain from direct blast loading to the head or a surge of blood into the brain from blast loads to the torso can produce pressure excursions, flow pulses, and mechanical stress far outside the normal physiological range that can cause tissue and cellular damage.
Furthermore, temporary disruption of oxygen delivery from immediate neurological response and electrical disruption of cellular processes from the explosion-generated electromagnetic pulse may further compound these primary injuries.

Imaging and Trauma Lesions
Magnetic resonance imaging (MRI) is more sensitive than computed tomography (CT) in detecting diffuse axonal injury.
T2 weighted magnetic resonance (MR) images, especially fluid attenuated inversion recovery (FLAIR) images, are best for visualizing nonhemorrhagic lesions.
Edema has lower signal intensity than brain on CT. Edema appears bright on T2 weighted or FLAIR MRI. The imaging appearance of contusion is variable.

Imaging and Trauma Lesions
In the absence of hemorrhage, CT may initially be only minimally abnormal.
If hemorrhage is present, there are commonly multiple bright areas of variable size.
Progression is common, with 25% demonstrating delayed hemorrhage over the
initial 48 hours. Small areas of hemorrhage may be most
easily identified with gradient echo MR.

Imaging and Trauma Lesions
The usual imaging appearance of subdural hemorrhage is an extraaxial, crescent-shaped, homogeneous fluid collection that conforms to the cerebral surface.
Its spread is limited by the dural reflections, and it rarely crosses the midline.
Imaged Trauma Lesions
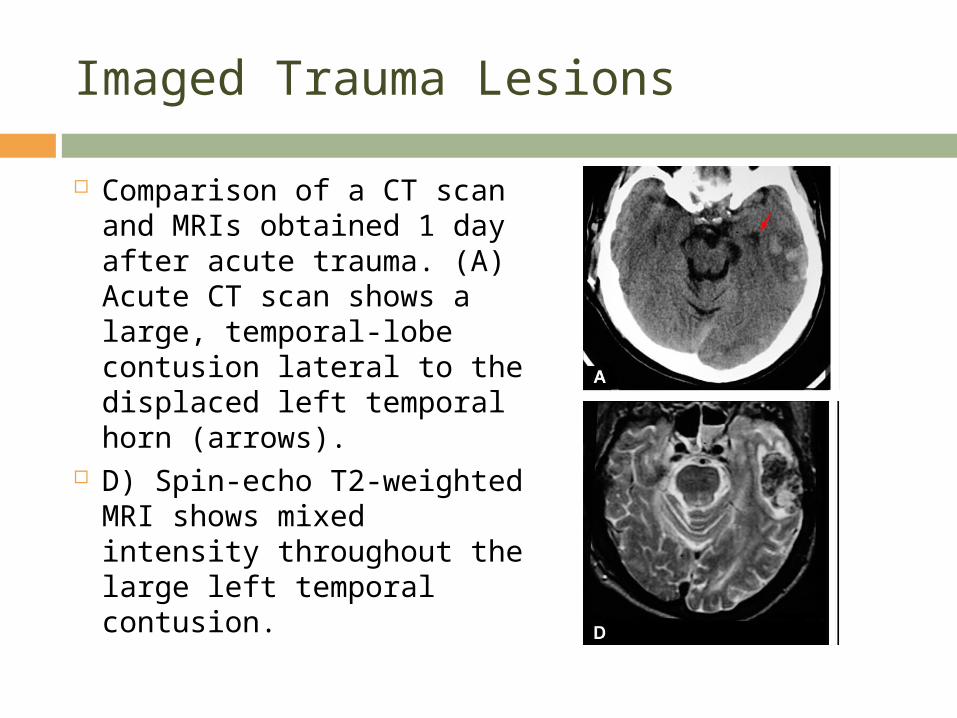
Comparison of a CT scan and MRIs obtained 1 day after acute trauma. (A) Acute CT scan shows a large, temporal-lobe contusion lateral to the displaced left temporal horn (arrows).
D) Spin-echo T2-weighted MRI shows mixed intensity throughout the large left temporal contusion.

Imaged Trauma Lesions
D) Spin-echo T2-weighted MRI shows mixed intensity throughout the large left temporal contusion.
(C) Fluid-attenuated inversion recovery (FLAIR) MRI demonstrates petechial hemorrhages that are isointense to the brain.
Note the accompanying abnormally bright signal in the left optic radiations (arrows); one of many small shearing injuries is seen at the right occipital cortex/gray matter junction (arrow).
Imaged Trauma Lesions
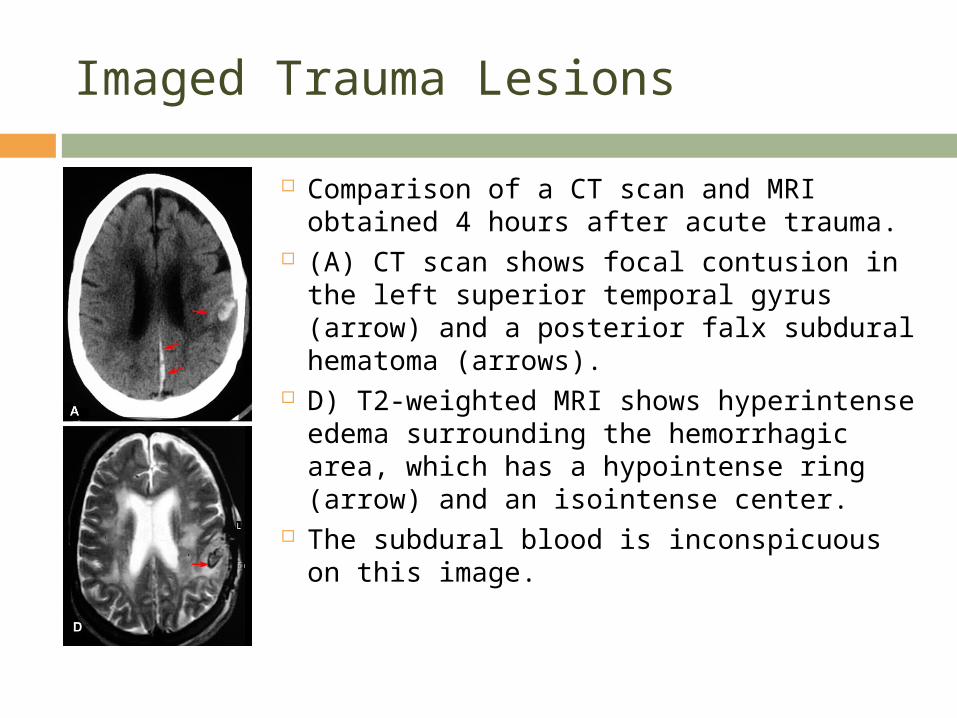
Comparison of a CT scan and MRI obtained 4 hours after acute trauma.
(A) CT scan shows focal contusion in the left superior temporal gyrus (arrow) and a posterior falx subdural hematoma (arrows).
D) T2-weighted MRI shows hyperintense edema surrounding the hemorrhagic area, which has a hypointense ring (arrow) and an isointense center.
The subdural blood is inconspicuous on this image.
Classification of Head Injury
The Mayo Head Injury Classification System (Malec, Brown, Leibson, Flaada, Mandrekar, Diehl, & Perkins, 2007) was developed to classify the severity of TBI based on commonly used TBI severity measures.
A moderate-severe (Definite) TBI (Criteria A) has one or more of the following characteristics: Death due to this TBI Loss of consciousness of 30 minutes or more Post-traumatic anterograde amnesia of 24 hours or
more

Classification of Head Injury
Worst Glasgow Coma Scale (GCS) full score in first 24 hours (unless invalidated upon review, e.g., attributable to intoxication, sedation, systemic shock)
One or more of the following present: • Subdural or epidural hematoma, • Cerebral contusion, • Hemorrhagic contusion, • Penetrating TBI (dura penetrated), • Subarachnoid hemorrhage, • Brain Stem Injury
Classification of Head Injury
If none of Criteria A apply, classify as a mild (Probable) TBI (Criteria B) if one or more of the following apply: Loss of consciousness of momentary to less than 30
minutes Post-traumatic anterograde amnesia of momentary to less
than 24 hours Depressed, basilar or linear skull fracture (dura intact) If none of Criteria A or B apply, classify as
Symptomatic (Possible) TBI if one or more of the following symptoms are present: Blurred vision Confusion (mental state changes)

Classification of Head Injury
Dazed Dizziness Focal neurologic symptoms Headache Nausea
Concussion
On of the continuing puzzles in head injury is the pathological basis for the phenomenon of concussion.
As per the 2008 Consensus Statement on Concussion in Sport (3rd International Conference on Concussion in Sport), concussion is defined as a complex pathophysiological process affecting the brain, induced by traumatic biomechanical forces.
Several common features utilized in defining the nature of a concussive head injury include:

Concussion
1. Concussion may be caused either by a direct blow to the head, face, neck or elsewhere on the body with an ‘‘impulsive’’ force transmitted to the head.
2. Concussion typically results in the rapid onset of short-lived impairment of neurologic function that resolves spontaneously.
3. Concussion may result in neuropathological changes but the acute clinical symptoms largely reflect a functional disturbance rather than a structural injury.
Concussion
4. Concussion results in a graded set of clinical symptoms that may or may not involve loss of consciousness. Resolution of the clinical and cognitive symptoms typically follows a sequential course however it is important to note that in a small percentage of cases however, post-concussive symptoms may be prolonged.
5. No abnormality on standard structural neuroimaging studies is seen in concussion.
The majority (80-90%) of concussions resolve in a short (7-10 day) period, although the recovery time frame may be longer in children and adolescents.
Concussion
The diagnosis of acute concussion usually involves the assessment of a range of domains including clinical symptoms, physical signs, behavior, balance, sleep and cognition.
The suspected diagnosis of concussion can include one or moreof the following clinical domains:
Symptoms – somatic (e.g. headache), cognitive (e.g. feeling like in a fog) and/or emotional symptoms (e.g. lability)
Physical signs (e.g. loss of consciousness, amnesia)
Concussion
Behavioral changes (e.g. irritablity) Cognitive impairment (e.g. slowed reaction times) Sleep disturbance (e.g. drowsiness) The appearance of symptoms might be delayed
several hours following a concussive episode. A range of additional investigations may be utilized
to assist in the diagnosis and/or exclusion of injury. Although conventional structural neuroimaging is
normal in concussive injury, a CT or MR brain scan should be employed whenever suspicion of an intra-cerebral structural lesion exists.

Concussion
Although in most case cognitive recovery largely overlaps with the time course of symptom recovery, it has been demonstrated that cognitive recovery may occasionally precede or more commonly follow clinical symptom resolution.
Although minor head injuries are generally considered benign, a significant number of people report persistent symptoms for weeks or months and some for years after injury despite a lack of evidence of brain abnormalities on MRI and CT scans.

Post Concussion Syndrome (PCS)
Post-concussion syndrome (post-concussional disorder in the DSM-IV) has been used to describe the range of residual symptoms that persist 12 months and beyond, sometimes years after the injury.
The most commonly reported symptoms of PCS are as follows: Attention deficits, difficulty sustaining mental effort. Fatigue and tiredness Impulsivity, irritability Low frustration threshold

Post Concussion Syndrome
Temper outbursts and changes in mood Learning and memory problems Impaired planning and problem solving Inflexibility, concrete thinking Lack of initiative Dissociation between thought and action Communication difficulties Socially inappropriate behaviors Self-centeredness and lack of insight Poor self-awareness

Post Concussion Syndrome
Impaired balance Dizziness and headaches Personality changes
Often despite several of these chronic symptoms, there is no evidence of brain abnormality from conventional structural neuroimaging tests, such as CT scans and MRIs.
The fact that these complaints seem to contradict the "negative" medical findings has often generated controversy as to whether PCS has an organic or psychological basis.
Post Concussion Syndrome
Over the past 30 years, evidence for an organic (brain based) etiology of post-concussion syndrome has accumulated through studies of cerebral blood flow, neuropsychological deficits, evoked potential recordings, PET, SPECT, MRI and quantitative EEG or QEEG.
Therefore, PCS can be considered a medically unexplained syndrome in which psychopathological processes are likely to be of considerable importance.
Post-Traumatic Complications
Residual disability or newly developing complications (e.g., seizure disorder; hydrocephalus) may be related to impact damage, to various early secondary pathological processes, or to later events, such as scarring or adhesions of brain tissue or blockage of CSF pathways.
Some of the post-traumatic complications are caused by diffuse (widespread) injury; other by focal (limited) injury.
The most severe form of diffuse damage is the chronic or persistive vegetative state, affecting about 5% of head injury survivors.

Post-Traumatic Complications
In cases where there is extensive neocortical necrosis, the cause is not so much the severity of the injury, but a consequence of resuscitation following cardio-respiratory arrest.
In cases where there is extensive subcortical white matter shearing, the cause is the severity of the initial impact damage.
In either case, the cortex has been rendered functionally inactive by widespread severe destruction of brain tissue.
Post-Traumatic Complications
Focal injuries, such as contusions or hematomas will often leave residual focal neurological deficits such as hemiplegia (paralysis of one half side of the body), hemiparesis (weakness of one half side of the body) hemianopsia (loss of one half of the visual field), and aphasia (disorders of language, both receptive and expressive).
Cranial nerve abnormalities often arise when cranial nerves are damaged when the skull is fractured or when the brain is thrown about during acceleration/deceleration injury.

Post-Traumatic Complications
Some common occurrences are damage to the olfactory (CN I) nerve after basilar skull fracture, resulting is anosmia, a partial or total loss of the sense of smell.
Damage to the optic nerve (CN II) may lead to transient loss of vision.
Damage to the facial (CN VII) nerve after temporal bone fracture may produce facial paralysis; and
Damage to the vestibulocochlear nerve (CN VIII) after basilar fracture in which otorrhea or hematotympanum is present, may affect hearing as well as vestibular function.
Post-Traumatic Complications
There is a definite risk of developing a chronic, recurring seizure disorder after significant head trauma.
The following factors significantly raise the probability of developing post-traumatic epilepsy:1.depressed skull fracture with dural tear
(>50%);2.penetrating wounds (>50%);3.Amnesia of > than 24 hours;4.Time after injury that first seizure occurs: a.
Immediate (little chance of becoming chronic); b. 1st week (33%); and c. 1st – 8th week (70%).

Post-Traumatic Complications
Seizures can first appear many years after an accident.
They are usually focal and more difficult to treat than idiopathic epilepsy.
Post-traumatic epilepsy is a chronic disorder, with only a 40% cure rate after 5 years.
Post-traumatic syndrome (PTS) is the most common and probably most complex sequelae of HI.
The basic elements of the syndromes are headache, dizziness, difficulty concentrating, and a host of vague behavioral symptoms such as anxiety, depression, and nervous instability.

Post-Traumatic Stress Disorder (PTSD)
Post-traumatic stress disorder (PTSD) is a common and complex sequelae of HI.
The basic elements of the syndromes are headache, dizziness, difficulty concentrating, and a host of vague behavioral symptoms such as anxiety, depression, and nervous instability.
This syndrome is more common with slight trauma than serious.
Biologic models posit that a fundamental mechanism underpinning PTSD involves an exaggerated response of the amygdala, resulting in impaired regulation by the medial prefrontal cortex.
Post-Traumatic Stress Disorder (PTSD)
The amygdala is central to the development and expression of conditioned fear reactions, and studies in humans and animals have shown that learning to inhibit these fear reactions involves inhibition by the medial prefrontal cortex.
Consistent with this model, patients with PTSD have diminished activation of the medial prefrontal cortex during the processing of fear.
Mild TBI often involves damage to the prefrontal cortex due to shearing forces of the frontal regions against the skull.
Post-Traumatic Stress Disorder
It is possible that a person’s capacity to regulate the fear reaction may be impaired after mild TBI because the neural networks involved in the regulation of anxiety may be damaged as a result of the mild TBI.
Cognitive models propose that PTSD is maintained when trauma survivors have inadequate cognitive resources to manage their trauma memories and to engage adaptive cognitive strategies to manage the traumatic experience (e.g., they are unable to appraise a distressing state as temporary and, therefore, have heightened anxiety).

Post-Traumatic Stress Disorder
Mild TBI can impair cognitive resources and may compromise the capacity to engage in cognitive strategies to manage the aftermath of a psychological trauma.
There is overwhelming evidence that maladaptive cognitive strategies (e.g., ruminating that one will never recover from the traumatic experience) after trauma are a major predictor of PTSD.
Therefore, it is possible that people with mild TBI have insufficient cognitive resources to engage appropriate cognitive strategies, which results in a greater incidence of PTSD.
Post-Traumatic Stress Disorder
The syndrome usually lasts a few weeks to a few months, with symptoms gradually disappearing only to be exacerbated by strenuous physical activity, emotional stress, or the use of alcohol.
Patients in highly physical or stressful jobs should be warned that symptoms might recur when they return to work.
Rest and symptomatic treatment are usually required.