Embed Size (px)
DESCRIPTION
Agenesia de cuerpo calloso
Citation preview

PEDIATRIC
Structural connectivity analysis reveals abnormal brainconnections in agenesis of the corpus callosum in children
Avner Meoded & Rohan Katipally & Thangamadhan Bosemani &Thierry A. G. M. Huisman & Andrea Poretti
Received: 6 September 2014 /Revised: 20 October 2014 /Accepted: 21 November 2014# European Society of Radiology 2014
AbstractObjectives Structural connectivity analysis is an ideal tool tostudy connections in brain malformations. We aimed to char-acterize the topological network measures and study sub-networks in children with agenesis of the corpus callosum(AgCC). We hypothesized a more segregated structural net-work in children with AgCC.Methods Structural connectivity analysis including topologyanalysis and network-based-statistics was applied in childrenwith AgCC and age-matched controls. Probabilistic-tractography and brain segmentation into 108 regions wereperformed. For controls, structural connectivity has been an-alyzed after excluding the callosal connections (‘virtualcallosotomy’).Results Ten patients (six males, mean age 6.5 years, SD4.5 years) and ten controls (mean age 5.9 years, SD 4.7 years)were included. In patients, topology analysis revealed higherclustering coefficient and transitivity and lower small worldindex and assortativity compared to controls. The bilateralinsula were identified as hubs in patients, whereas the cere-bellum was detected as a hub only in controls. Three sub-networks of increased connectivity were identified in patients.
Conclusions We found reduced global and increased localconnectivity in children with AgCC compared to controls.Neural plasticity in AgCC may attempt to increase the inter-hemispheric connectivity through alternative decussatingpathways other than the corpus callosum.Key Points• The structural connectivity analysis quantifies white-matternetworks within the brain
• In callosal agenesis there is reduced global and increasedlocal connectivity
• In callosal agenesis, alternative decussating pathways areused for interhemispheric connectivity
Keywords Corpus callosum . Agenesis . Children .
Structural connectivity . Diffusion tensor imaging
AbbreviationsAgCC agenesis of the corpus callosumAC anterior commissureBCT brain connectivity toolboxCC corpus callosumFT fiber tractographyPT probabilistic tractographyNBS network based statistics
Introduction
The corpus callosum (CC) is the main forebrain commissureand comprises more than 190 million organized axons, whichform homo- or heterotopic connections between cerebral re-gions [1, 2].These connections are involved in cognitive func-tions and the integration of complex sensory informationbetween the cerebral hemispheres [3, 4]. Agenesis of the CC(AgCC) may result from disruption of multiple developmental
Electronic supplementary material The online version of this article(doi:10.1007/s00330-014-3541-y) contains supplementary material,which is available to authorized users.
A. Meoded (*) : T. Bosemani : T. A. G. M. Huisman :A. PorettiSection of Pediatric Neuroradiology, Division of PediatricRadiology, The Russell H. Morgan Department of Radiology andRadiological Science, The Johns Hopkins University School ofMedicine, Charlotte R. Bloomberg Children’s Center, Sheikh ZayedTower, Room 4174, 1800 Orleans Street, Baltimore,MD 21287-0842, USAe-mail: [email protected]
R. KatipallyDepartment of AppliedMathematics, Brown University, Providence,RI, USA
Eur RadiolDOI 10.1007/s00330-014-3541-y

steps during brain development [5]. Neurocognitive deficitsand behavioural issues are common in children with AgCC [6,7]. Patients with AgCC may provide us with a unique oppor-tunity to study the response of the brain to an underlyingdevelopmental abnormality.
Diffusion tensor imaging (DTI) is an advanced magneticresonance imaging (MRI) technique that allows in vivo eval-uation of the microstructure and integrity of white-matter(WM) tracts [8]. Fibre tractography (FT) uses the preponder-ant direction of diffusion in each voxel to reconstructconnecting pathways [9]. In AgCC, DTI and FT can demon-strate the Probst’s bundles pre- and postnatally [10–12]. TheProbst’s bundles are largeWM tracts that course parallel to theinterhemispheric fissure and contain fibres that would normal-ly cross the midline in the intact CC. The anatomical connec-tivity analysis is a further step in DTI post-processing whichenables quantification of WM networks within the brain [13,14]. Metrics can be defined to characterize the global andregional network organization [14, 15]. In addition, sub-networks may be identified that are strongly interconnectedand are likely to be functionally integrated [16]. In AgCC, thestructural connectivity analysis may better characterize WMabnormalities and discover subtle, yet functionally relevantabnormal connectivity. The majority of the available studieson WM connectivity in AgCC have been performed using FT[1, 17]. Only one study so far has applied the structuralconnectivity analysis, but included primarily adult patients[18]. Furthermore, this study did not assess cerebro-cerebellar connectivity patterns (the cerebellum was notincluded in the connectivity analysis) and did not applynetwork-based statistics (NBS) to quantify connectivitydifferences.
This current study combined topology analysis and NBS to(1) characterize the topological network measures and (2)study connected and disconnected sub-networks in childrenwith AgCC. We hypothesized a more segregated and lessintegrated structural network in children with AgCC com-pared to age-matched controls.
Materials and methods
This study was approved by the institutional research ethicsboard.
Subjects
The inclusion criteria for this study were: (1) isolated AgCC,(2) availability of DTI data without artefacts enabling a high-quality post-processing and (3) age at MRI less than 18 years.Eligible patients were collected through a search of our pae-diatric neuroradiology database covering the time period be-tween 1 September 2010 and 31 August 2013.
Age- and gender-matched controls were selected from ourpaediatric database using the following criteria: (1) normalbrain anatomy, (2) absence of neurological disorders and (3)availability of DTI raw data.
Image acquisition
All MRI studies were performed on a 1.5 T scanner (SiemensAvanto, Erlangen, Germany). 3D-T1-weighted images, axialT-weighted images, axial fluid attenuation inversion recovery(FLAIR) and a single-shot spin echo, echo planar axial DTIsequence with diffusion gradients along 20 non-collinear di-rections were acquired. For the acquisition of the 3D-T1-weighted images, the following parameters were used: repeti-tion time (TR)=1130 ms, echo time (TE)=3.99 ms, slicethickness=1.0 mm, field-of-view (FOV)=190×190 mm, ma-trix size=192×192. For DTI, an effective high b-value of1000 s/mm2 was used for each of the 20 diffusion-encodingdirections. We performed an additional measurement withoutdiffusion weighting (b=0 s/mm2). For the acquisition of theDTI data, the following parameters were used: TR=7100 ms,TE=84 ms, slice thickness=2.5 mm, FOV=240×240 mmand matrix size=192×192. Parallel imaging iPAT=2 withgeneralized auto-calibrating partial parallel acquisition(GRAPPA) reconstruction was used. The acquisition wasrepeated twice to enhance the signal-to-noise ratio.
Data pre-processing
Algorithms in the TORTOISE software package were used tocorrect DTI raw data for motion artefacts and eddy currentsdistortion and to calculate the tensor and DTI metrics maps[19]. Subsequently, the DTI raw data of each subject wasregistered to MNI space with dimensions of 91×109×91sampled at 2-mm intervals, corresponding to the SPM andFSL MNI templates (MNI 152).
We used the functional MRI of the brain (FMRIB)linear image registration tool to perform linear registra-tion between the reference b0 images and the structuralspace and FMRIB’s non-linear image registration tool toperform non-linear registration of T1-weighted images(FMRIB Software Library v5.0) [20].
Probabilistic tractography (PT) and connectivity matrixconstruction
To model the structural brain connectivity, we used the graphtheory that describes a neural network consisting of a collec-tion of nodes and connections/edges [21].
The brain was parcellated into 108 cortical regions usingthe automated anatomical labelling template (SupplementaryTable 1) [22]. The anatomical regions have been definedaccording to theWake Forest University (WFU) pickatlas tool
Eur Radiol

in SPM8 [23]. These 108 cortical regions represent the nodesof the neural network and were used as the seed points for thePT [13]. To compare the structural connectivity studies ofpatients and controls, in all controls we simulated the removalof all callosal connections by using an exclusion mask toexclude all callosal connections from PT as previously shownby Owen et al. [18] (in the remainder of the manuscript wewill refer to this post-processing step as ‘virtual callostomy’).
The edges were calculated using PT that was preformedwith probtrackx2 [24]. Each of the seed’s tracking results weremasked by each of the other 107 regions, referred to as targets,to obtain a connection strength between each seed and targetpair, effectively taking the total number of streamlinesconnecting two regions as the connection strength. Since PTcannot determine directionality due to the antipodal symmetryof DTI, edges were considered undirected and hence nodirectionality was assigned between nodes. The resulting108×108 connection matrix reflects the distribution of pair-wise WM connections between nodes. All matrices weresymmetrical about the diagonal and the individual matrixdiagonal was set to zero. Aweight conversion function (BrainConnectivity Toolbox (BCT), http://www.brain-connectivity-toolbox.net/) was used to binarize all connection matrices forNBS. For topological measures analysis, thresholding theconstructed association matrices at a range of networkdensities was performed for comparing the networktopologies across that range.
Network analysis
To evaluate the differences in network connectivity betweenpatients and controls, two different network analyses wereperformed: topology analysis and NBS.
Topology analysis was applied to evaluate differences inthe network measures between patients and controls [25].Individual network measures characterize one or several as-pects of global or local connectivity that describes aspects ofstructural integration and segregation, also characterizing pat-terns of local anatomical circuitry, and tests resilience ofnetworks to insult. Network measures are influenced by basicnetwork characteristics including number of nodes and linksand degree distribution. The significance of network statisticsis established by comparison with statistics calculated on null-hypothesis networks that have simple random or orderedtopologies, but preserve basic characteristics of the originalnetwork. We used a null-hypothesis network with a randomtopology that shared the size, density and binary degree dis-tribution of our connection network [25, 26]. The graphanalysis toolbox, which integrates functions from BCT, wasused for quantification of the individual network measures[25, 27]. The association matrix for each subject wasthresholded at a range of network densities for comparingthe network topologies across that range. Before performing
statistical testing, the density range in which the networkswere not fragmented was identified, and the final range ofdensities was set to [0.05:0.35], with 0.04 as the interval forincrements. The topology of the brain networks were com-pared to the corresponding mean values of 20 benchmarkrandom graphs. The following network measures have beencalculated: clustering coefficient (a measure of segregation,reflecting the density of connections between the node neigh-bours), transitivity (a variant of the clustering coefficient, thatis normalized collectively and hence is not disproportionatelyinfluenced by nodes with a low degree), local efficiency (ameasure related to the clustering coefficient and defined as theglobal efficiency computed on node neighbourhoods), modu-larity (a measure of segregation defined as the degree to whichthe network may be subdivided into clearly delineated andnon-overlapping groups), path length (a measure of integra-tion defined the sum of the edge lengths - short paths are likelyto be most effective for inter-node communication), globalefficiency (a measure of integration defined as the averageinverse shortest path length), small worldness (a combinationof high clustering and short characteristic path length; subse-quently also defined as the combination of high global andlocal efficiency of information transfer between nodes of anetwork), and assortativity (a measure of network resiliencedefining the correlation between the degrees of connectednode pairs; positive assortativity indicates that edges tend tolink nodes with matching degrees) [25]. A nonparametricpermutation test with 5,000 repetitions was used to test thestatistical significance of the between-group differences innetwork topology and regional network measures. A two-tailed p<0.05 value was used to determine significance. Inaddition to comparing global network measures at every den-sity, functional data analysis was performed to make thebetween-group comparison less sensitive to the thresholdingprocess. For the regional network measures comparison, thep-values are false discovery rate corrected for multiple com-parisons. In addition, we calculated Dmin as the minimumdensity and compared graphs at this density. Hubs have beendefined based on the between-ness centrality (2SD greaterthan network mean between-ness centrality), which is a mea-sure of node centrality in a network. Network modularityanalysis was also performed with optimization algorithmsimplemented in BCT, for quantification of modular structure[27]. In order to characterize the degeneracy of the modularitystructure adequately, the optimization algorithm was set to run100 iterations. The brain networks were visualized withBrainNet Viewer (www.nitrc.org/projects/bnv) [28]. Age andgender were included in the model as covariates of nuisance.
NBS was performed in order to evaluate the differences insub-networks between the patients and the controls [29].Withpermutation testing on topological clusters of connectionsNBS allows us to identify sub-networks of graphs that aredifferent between groups. The statistical model included the
Eur Radiol

following components: a design matrix of ten patients andten controls with contrast [1, -1] and [-1, 1]. The firstcontrast was applied to identify sub-networks that aremore interconnected in controls compared to patients,while the second contrast was used to test the opposite.A t-test was applied to assess the statistical significance ofbetween-group comparisons of the network metrics. Foreach metric, the data labels were randomly reassignedbetween the two groups and t-values were computed foreach relabeling. A total of 5,000 permutations were per-formed to estimate the null distribution and associationswith t>3 were analysed by NBS. A family wise error ratecorrected significance level of p<0.05 was used. In NBS,no individual connection can be declared significant, onlythe interconnected sub-network as a whole.
Results
Ten children with AgCC (six males, mean age 6.5 years, SD4.5 years) and ten age-matched controls (mean age 5.9 years,SD 4.7 years) were included in this study.
Topology analysis revealed a higher clustering coefficientand transitivity and lower small world index and assortativityacross the range of densities in patients compared to ‘virtualcallosotomy’, age-matched controls (Table 1). In patients,hubs were found in the bilateral insula and precuneus(Fig. 1b), whereas in controls, hubs were identified in thebilateral precuneus, right postcentral gyrus and right cerebellarlobule 8 (Fig. 1a). No significant difference in global networkmodularity was found between patients and controls. Howev-er, six modules were identified in the network of controls
Table 1 Differences (mean±SD) in network measures between patients with AgCC and controls with ‘virtual callosotomy’
Network measure Healthy controls (reference) ‘Virtual callosotomy’ Patients P values
Assortativity 0.1080±0.04 0.1110±0.04 0.0552±0.06 0.03
Global efficiency 0.5445±0.021 0.4640±0.02 0.4753±0.01 0.14
Clustering coefficient 0.6079±0.015 0.5570±0.008 0.5759±0.009 0.005
Local efficiency 0.7988±0.008 0.7440±0.006 0.7472±0.009 0.45
Modularity 0.4116±0.026 0.4900±0.02 0.4880±0.01 0.86
Path length 2.1350±0.09 2.6630±0.11 2.5720±0.05 0.11
Small worldness 2.1800±0.17 3.1890±0.3 2.8100±0.23 0.005
Transitivity 0.5265±0.01 0.4978±0.01 0.5187±0.01 0.003
SD, standard deviation. Bold numbers indicate statistically significant differences between patients and controls; Values for healthy controls (withoutvirtual callosotomy) are reported for reference
Fig. 1 Network hubs (nodes with nodal between-ness of 2SD greaterthan network mean between-ness) include bilateral precuneus, rightpostcentral gyrus and right eighth cerebellar lobule in ‘virtual
callosotomy’ controls (A) and bilateral precuneus, bilateral insula andright lingual gyrus in patients with AgCC (B)
Eur Radiol

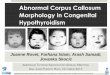
Fig. 3 Highly connected sub-networks in patients with AgCC compared to ‘virtual callosotomy’ controls as identified by network-based statistics.Networks 1 and 3 are left intrahemispheric and network 2 is interhemispheric and connects the left cerebral hemisphere with the contralateral cerebellum
Fig. 2 Topology analysis ofnetwork modules identified sixmodules for controls (A) and fivemodules for AgCC patients (B).The anatomical regions arecolour-coded according to thecorresponding colour-moduleassignment at the right of eachpanel. For the complete list of theregions included in each module,refer to Supplementary Tables 2(controls) and 3 (patients)
Eur Radiol

(Fig. 2a and Supplementary Table 2), while five modules werefound in the network of patients (Fig. 2b and SupplementaryTable 3). In both networks, the degree of distribution followedan exponentially truncated power-law. NBS identified threesub-networks of increased connectivity in patients comparedto controls (Fig. 3 and Table 2).
Discussion
Advances in neuroscience have revealed that neurocognitivefunctions and behaviour depend on the effective global com-munication within the brain and integration of informationacross the entire network. Recent progress in neuroimagingtechniques has allowed for a comprehensive mapping of thestructural and functional connectivities within the brain [13].Structural or anatomical connectivity describes a physical net-work of connections, which may correspond to fibre pathwaysor individual synapses, while functional connectivity character-izes interregional neural interactions during particular cognitiveor motor tasks or at rest [21, 30]. The connectivity analysis hasemerged as an ideal tool to study the structure, performance andplasticity of the normal and malformed brain [18, 31, 32].
In our study, topology analysis revealed higher cluster-ing coefficient in patients compared to controls. Thesefindings are in agreement with a structural connectivitystudy in adults with AgCC and represents increased localconnectivity [18]. Increase in local connectivity was con-firmed by higher transitivity values in AgCC compared to‘virtual callosotomy’. Additionally, in patients and controlswe found a small-world index higher than 1 demonstrating
that both groups follow a small-world organization across awide range of network densities. A small-world organiza-tion represents a highly-efficient network characterized byhigh clustering and short characteristic path length havinghigh global and local efficiency [33]. In patients, however,the small-world index was lower compared to controls.Although we did not find differences in global efficiencyand path length, a lower small-world index in our patientsmay suggest reduced global connectivity in AgCC. This isin agreement with the results of Owen et al. [18]. Finally,topology analysis showed reduced assortativity in patients.Assortativity represents the correlation between the de-grees of connected node pairs. Reduced assortativity sug-gests that network organization in patients tends to havedisconnected hubs [34]. In agreement with our hypothesis,topology analysis showed that patients have a more segre-gated structural connectivity with reduced global and in-creased local connectivity compared to controls.
In all subjects, the degree of network distribution followedan exponentially truncated power law distribution. This sug-gests that networks consist of a high number of regions with asmall number of connections and few regions with a highnumber of connections, the so-called hubs. Hubs are highly ordensely connected to the rest of the network, and facilitateglobal integrative processes. In all subjects, we found hubs inthe posterior medial and parietal cortical regions. These re-gions have a high metabolic activity and are key componentsof the human default mode network [35–37]. It may besurprising that we found only four hubs in controls. ‘Virtualcallosotomy’ most likely explains the low number of hubs inour controls. The cerebellum was identified as a hub only inthe control group. This supports a reduced global connectivityin patients. The insular regions, however, were identified ashubs only in patients. The bilateral insular regions are con-nected to each other by the anterior commissure (AC). In theabsence of the CC, the AC is the most important interhemi-spheric commissure. Moreover, in up to 50 % of AgCCpatients, the AC is thickened [2, 38].This may suggestthat interhemispheric connection in AgCC could be re-routed through the AC as a result of brain plasticity [6].The presence and thickening of the AC alone, however,is not sufficient to explain interhemispheric connectivityin AgCC.
NBS identified three sub-networks with higher connectionin AgCC compared to controls. Two sub-networks were lo-cated only in the left cerebral hemisphere including the fronto-parietal and temporo-occipital regions. The third highly con-nected sub-network included fronto-cerebellar interhemi-spheric connections. It is intriguing that in AgCC, one highlyconnected sub-network (interhemispheric fronto-cerebellarconnections) and two insular hubs, which are most likelyhighly connected to the rest of the network via the AC, arepointing to midline crossing. Evolutionary arguments suggest
Table 2 Sub-networks with increased connectivity in AgCC patientscompared to ‘virtual callosotomy’ controls
Network P values Region 1 Region 2 t test value
1 0.013 Precentral L Insula L 3.99
Olofactory L Insula L 3.16
Insula L Hippocampus L 3.01
Rolandic Oper L Postcentral L 3.22
Insula L Postcentral L 3.55
Insula L Parietal Inf L 3.57
Hippocampus L Angula L 3.12
2 0.021 Frontal Med Orb L Cingulum Ant R 3.06
Amygdala L Cerebelum 4_5 L 3.09
Cingulum Ant L Cerebelum 4_5 R 3.22
Cingulum Ant R Cerebelum 4_5 R 3.01
Amygdala L Cerebelum 4_5 R 3.34
3 0.048 Calcarine L Fusiform L 3.16
Fusiform L Heschl L 3.12
Heschl L Temporal Mid L 3.21
Eur Radiol

that midline crossing emerged in response to distinct physio-logical and anatomical constraints [39]. In the human braindecussation is essential to complex 3D somatotopic functions[40]. The disconnection syndrome is caused by injury ofcommissural pathways and occurs more often in older chil-dren or adults with commissurotomy compared to youngchildren with commissurotomy or patients with AgCC [41,42]. In the absence of the CC, neural plasticity in young brainsmay attempt to increase connectivity through alternative de-cussating pathways and improve the interhemispheric flow ofinformation [6]. It is arguable that the efficiency of alternativedecussating pathways may be responsible for the variableneurocognitive outcome in children with AgCC.
Highly efficient brain networks promote integrative pro-cessing and are composed of interconnected hubs that directglobal information flow. Hubs, however, come at a high costowing to the long-distance connections between differentbrain regions [37]. Brain network organization is the resultof an economical trade-off between the physical cost of thenetwork and the adaptive value of its topology. In AgCC wefound a lower number of modules, which by definition aremore intraconnected than interconnected with each other.These findings suggest that neural plasticity in AgCC reorga-nizes structural connectivity with a cost-efficient trade-off toreduce further connection cost at the expense of decreasingintegrative capacity. Although one sub-network includes thecontralateral cerebellum, the exclusion of the cerebellum as ahub and the lower modularity compared to controls representa trade-off between topology and the ‘wiring cost’ of neuralplasticity during the CNS development in AgCC.
We are aware of some limitations in our study. First, thesample size is rather small. In addition, the lack of correlationwith neurocognitive and behavioural functions does not allowthe investigation of the clinical significance of abnormal ana-tomical connectivity in AgCC. Finally, DTI raw data have beenacquired on a 1.5 T scanner with diffusion gradients along 20non-collinear directions. Although there is no consensus re-garding the ‘standard’ acquisition protocol for structural con-nectivity studies, in the majority of the studies DTI raw datahave been acquired on 3 T scanners with diffusion gradientsalong more than 30 non-collinear directions. However, a recentoutstanding article reported structural connectivity studiesbased on DTI raw data acquired on a 1.5 T scanner [43]. Inaddition, our findings acquired on a 1.5 T scanner with diffu-sion gradients along 20 non-collinear directions are consistentwith a previous study, which used a 3 T scanner and diffusiongradients along 55 non-collinear directions [18].
Conclusions
Our study shows that structural connectivity in AgCC is muchmore complex than may be explained by the absence of
transcallosal connectivity and presence of Probst’s bundles.Patients with AgCC have more segregated brain connectivitywith reduced global and increased local connectivity com-pared to controls. Two hubs in the insular regions close tothe AC and one highly connected sub-network including thecontralateral cerebellum suggest that neural plasticity inAgCC may attempt to increase the interhemispheric connec-tivity through alternative decussating pathways other than theCC. CNS development in AgCC, however, is following acost-efficient trade-off between topology and the ‘wiring cost’of neural plasticity resulting in a less efficient structural con-nectivity compared to controls.
Acknowledgements The scientific guarantor of this publication isAndrea Poretti. The authors of this manuscript declare no relationshipswith any companies whose products or services may be related to thesubject matter of the article. The authors state that this work has notreceived any funding. One of the authors (Avner Meoded) has significantstatistical expertise. Institutional Review Board approval was obtained.Written informed consent was waived by the Institutional Review Board.Methodology: retrospective.
References
1. Wahl M, Strominger Z, Jeremy RJ et al (2009) Variability ofhomotopic and heterotopic callosal connectivity in partial agenesisof the corpus callosum: a 3T diffusion tensor imaging and Q-balltractography study. AJNR Am J Neuroradiol 30:282–289
2. Raybaud C (2010) The corpus callosum, the other great forebraincommissures, and the septum pellucidum: anatomy, development,and malformation. Neuroradiology 52:447–477
3. Brown WS, Jeeves MA, Dietrich R, Burnison DS (1999) Bilateralfield advantage and evoked potential interhemispheric transmissionin commissurotomy and callosal agenesis. Neuropsychologia 37:1165–1180
4. Paul LK, Van Lancker-Sidtis D, Schieffer B, Dietrich R, Brown WS(2003) Communicative deficits in agenesis of the corpus callosum:nonliteral language and affective prosody. Brain Lang 85:313–324
5. Edwards TJ, Sherr EH, Barkovich AJ, Richards LJ (2014) Clinical,genetic and imaging findings identify new causes for corpuscallosum development syndromes. Brain
6. Paul LK, Brown WS, Adolphs R et al (2007) Agenesis of the corpuscallosum: genetic, developmental and functional aspects of connec-tivity. Nat Rev Neurosci 8:287–299
7. Sotiriadis A,Makrydimas G (2012) Neurodevelopment after prenataldiagnosis of isolated agenesis of the corpus callosum: an integrativereview. Am J Obstet Gynecol 206:e331–335
8. Basser PJ, Pierpaoli C (1996) Microstructural and physiologicalfeatures of tissues elucidated by quantitative-diffusion-tensor MRI.J Magn Reson B 111:209–219
9. Mori S, Crain BJ, Chacko VP, van Zijl PC (1999) Three-dimensionaltracking of axonal projections in the brain by magnetic resonanceimaging. Ann Neurol 45:265–269
10. Lee SK, Mori S, Kim DJ, Kim SY, Kim DI (2004) Diffusion tensorMR imaging visualizes the altered hemispheric fiber connection incallosal dysgenesis. AJNR Am J Neuroradiol 25:25–28
11. Meoded A, Poretti A, Tekes A, Flammang A, Pryde S, Huisman TA(2011) Prenatal MR diffusion tractography in a fetus with completecorpus callosum agenesis. Neuropediatrics 42:122–123
Eur Radiol

12. Kasprian G, Brugger PC, Schopf V et al (2013) Assessing prenatalwhite matter connectivity in commissural agenesis. Brain 136:168–179
13. Sporns O, Tononi G, Kotter R (2005) The human connectome: astructural description of the human brain. PLoS Comput Biol 1:e42
14. Bullmore E, Sporns O (2009) Complex brain networks: graph theo-retical analysis of structural and functional systems. Nat RevNeurosci 10:186–198
15. Bullmore ET, Bassett DS (2011) Brain graphs: graphical models ofthe human brain connectome. Annu Rev Clin Psychol 7:113–140
16. Zalesky A, Fornito A, Harding IH et al (2010) Whole-brainanatomical networks: does the choice of nodes matter?Neuroimage 50:970–983
17. Tovar-Moll F, Moll J, de Oliveira-Souza R, Bramati I, AndreiuoloPA, Lent R (2007) Neuroplasticity in human callosal dysgenesis: adiffusion tensor imaging study. Cereb Cortex 17:531–541
18. Owen JP, Li YO, Ziv E et al (2013) The structural connectome of thehuman brain in agenesis of the corpus callosum. Neuroimage 70:340–355
19. Pierpaoli C, Walker L, Irfanoglu MO et al (2010) TORTOISE: anintegrated software package for processing of diffusion MRI data18th Annual Meeting of the International Society of MagneticResonance in Medicine Stockholm, pp 1597
20. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM(2012) Fsl. Neuroimage 62:782–790
21. Filippi M, van den Heuvel MP, Fornito A et al (2013) Assessment ofsystem dysfunction in the brain through MRI-based connectomics.Lancet Neurol 12:1189–1199
22. Tzourio-Mazoyer N, Landeau B, Papathanassiou D et al (2002)Automated anatomical labeling of activations in SPM using a mac-roscopic anatomical parcellation of the MNI MRI single-subjectbrain. Neuroimage 15:273–289
23. Maldjian JA, Laurienti PJ, Kraft RA, Burdette JH (2003) Anautomated method for neuroanatomic and cytoarchitectonicatlas-based interrogation of fMRI data sets. Neuroimage 19:1233–1239
24. Behrens TE, Berg HJ, Jbabdi S, Rushworth MF, Woolrich MW(2007) Probabilistic diffusion tractography with multiple fibre orien-tations: what can we gain? Neuroimage 34:144–155
25. Rubinov M, Sporns O (2010) Complex network measures ofbrain connectivity: uses and interpretations. Neuroimage 52:1059–1069
26. Maslov S, Sneppen K (2002) Specificity and stability in topology ofprotein networks. Science 296:910–913
27. Hosseini SM, Hoeft F, Kesler SR (2012) GAT: a graph-theoreticalanalysis toolbox for analyzing between-group differences in large-scale structural and functional brain networks. PLoS One 7:e40709
28. Xia M, Wang J, He Y (2013) BrainNet Viewer: a network visualiza-tion tool for human brain connectomics. PLoS One 8:e68910
29. Zalesky A, Fornito A, Bullmore ET (2010) Network-based statistic:identifying differences in brain networks. Neuroimage 53:1197–1207
30. Smith SM, Fox PT, Miller KL et al (2009) Correspondence of thebrain’s functional architecture during activation and rest. Proc NatlAcad Sci U S A 106:13040–13045
31. Owen JP, Li YO, Yang FG et al (2013) Resting-state networks and thefunctional connectome of the human brain in agenesis of the corpuscallosum. Brain Connect 3:547–562
32. Tymofiyeva O, Hess CP, Ziv E et al (2013) A DTI-based template-free cortical connectome study of brain maturation. PLoS One 8:e63310
33. Sporns O (2006) Small-world connectivity, motif composition, adcomplexity of fractal neuronal connections. Biosystems 85:55–64
34. Newman ME (2002) Assortative mixing in networks. Phys Rev Lett89:208701
35. Hagmann P, Cammoun L, Gigandet X et al (2008) Mapping thestructural core of human cerebral cortex. PLoS Biol 6:e159
36. van den Heuvel MP, Sporns O (2011) Rich-club organization of thehuman connectome. J Neurosci 31:15775–15786
37. Bullmore E, Sporns O (2012) The economy of brain network orga-nization. Nat Rev Neurosci 13:336–349
38. Hetts SW, Sherr EH, Chao S, Gobuty S, Barkovich AJ (2006)Anomalies of the corpus callosum: anMR analysis of the phenotypicspectrum of associated malformations. AJR Am J Roentgenol 187:1343–1348
39. Vulliemoz S, Raineteau O, Jabaudon D (2005) Reaching beyond themidline: why are human brains cross wired? Lancet Neurol 4:87–99
40. Shinbrot T, YoungW (2008)Why decussate? Topological constraintson 3D wiring. Anat Rec (Hoboken) 291:1278–1292
41. Seymour SE, Reuter-Lorenz PA, Gazzaniga MS (1994) The discon-nection syndrome. Basic findings reaffirmed. Brain 117:105–115
42. Choudhri AF, Whitehead MT, McGregor AL, Einhaus SL, Boop FA,Wheless JW (2013) Diffusion tensor imaging to evaluate commis-sural disconnection after corpus callosotomy. Neuroradiology 55:1397–1403
43. Crossley NA, Mechelli A, Scott J et al (2014) The hubs of the humanconnectome are generally implicated in the anatomy of brain disor-ders. Brain 137:2382–2395
Eur Radiol