Embed Size (px)
Citation preview
Stroke SelfStroke Self--management: management: Outcomes of a Randomized Outcomes of a Randomized Controlled Pilot Trial Controlled Pilot Trial
Teresa M. Damush, Ph.D., Gloria Nicholas, RN, Lauri e Teresa M. Damush, Ph.D., Gloria Nicholas, RN, Lauri e Plue MA,, Susan Ofner, MS, Rebecca Beyth MD, Plue MA,, Susan Ofner, MS, Rebecca Beyth MD, Zhangsheng Yu, Ph.D., & Linda S. Williams, MDZhangsheng Yu, Ph.D., & Linda S. Williams, MD
VA Stroke QUERI Center, HSRD Center of Excellence o n ImplementinVA Stroke QUERI Center, HSRD Center of Excellence o n Implementin g g EvidenceEvidence --Based Practices, Roudebush VAMC, Indiana Universit y Based Practices, Roudebush VAMC, Indiana Universit y
School of Medicine, Regenstrief Institute, Inc., I ndianapolis, School of Medicine, Regenstrief Institute, Inc., I ndianapolis, ININ
Support from HSR&D IIR Grant #IMV 04Support from HSR&D IIR Grant #IMV 04 --096 and VA HSR&D STR096 and VA HSR&D STR --0303--168.168.
ObjectivesObjectives
•• Describe the Elements of our Describe the Elements of our Stroke SelfStroke Self --Management ProgramManagement Program
•• Present Preliminary Results from a Present Preliminary Results from a randomized controlled pilot studyrandomized controlled pilot study
BackgroundBackground•• Veterans with Stroke are at Risk for Veterans with Stroke are at Risk for
secondary strokessecondary strokes•• Secondary stroke prevention Secondary stroke prevention
promoted as guideline carepromoted as guideline care•• Lack of behavioral change Lack of behavioral change
strategies implemented to promote strategies implemented to promote secondary stroke preventionsecondary stroke prevention
•• Lack of clinical provider trainingLack of clinical provider training•• Lack of designated responsibility Lack of designated responsibility
for clinical staff for clinical staff

Development of Stroke Development of Stroke SelfSelf--Management ProgramManagement Program
•• Formative Developmental EvaluationFormative Developmental Evaluation–– Began with the Stanford Arthritis and Began with the Stanford Arthritis and
Chronic Disease SelfChronic Disease Self --Management Management format (Lorig et al)format (Lorig et al)
–– Key informant survey of structure of Key informant survey of structure of patient education and selfpatient education and self --management management resourcesresources
–– Received stakeholder input and Received stakeholder input and preferencespreferences�� Stroke SurvivorsStroke Survivors�� CaregiversCaregivers�� Neurologists & General InternistsNeurologists & General Internists�� NursesNurses
SelfSelf--Efficacy Theoretical Efficacy Theoretical Concepts & Program Concepts & Program ApplicationApplication
•• 1. Verbal 1. Verbal PersuasionsPersuasions–– Staff explanationsStaff explanations–– Promotion of physician and Promotion of physician and
therapeutic therapeutic recommendationsrecommendations
•• 2. Social Modeling/ 2. Social Modeling/ Vicarious Vicarious ExperiencesExperiences–– Staff demonstration of all Staff demonstration of all
strategies and new strategies and new behaviorsbehaviors
–– Peers practice behavior in Peers practice behavior in group meetings and share group meetings and share experiences vicariously (we experiences vicariously (we learn by watching the learn by watching the outcomes of othersoutcomes of others ’’behaviors)behaviors)
–– View material of stroke View material of stroke patients similar to thempatients similar to them
33. Past Achievements. Past Achievements–– Past failures may influence Past failures may influence
your current effortsyour current efforts–– Set realistic, achievable goalsSet realistic, achievable goals–– Gain an understanding of the Gain an understanding of the
course of stroke course of stroke rehabilitation and realistic rehabilitation and realistic expectationsexpectations
–– Tackle one stroke risk factor Tackle one stroke risk factor at a time at a time
•• 4. Reinterpretation of 4. Reinterpretation of Sensations/physical Sensations/physical statestate–– Discuss symptoms and how Discuss symptoms and how
to diminishto diminish–– Distraction Distraction –– Mental ImageryMental Imagery–– RelaxationRelaxation

SelfSelf--ManagementManagementMenu Menu ––6 sessions6 sessions
•• Expectations after Expectations after stroke stroke –– What is What is normal?normal?
•• Negative/Positive Negative/Positive thinkingthinking
•• Addressing FearsAddressing Fears•• Having Something to Having Something to
dodo•• Follow Follow –– Up Medical Up Medical
VisitsVisits•• CommunicationCommunication
–– ProviderProvider–– caregiverscaregivers
•• Adapting/coping Adapting/coping with disabilitieswith disabilities
•• Finding a buddyFinding a buddy•• Meds for MoodMeds for Mood•• Move to improve Move to improve
Mood & EnergyMood & Energy•• Community Community
ResourcesResources•• Stroke Risk Stroke Risk
Factor Factor ModificationModification

Build SelfBuild Self--EfficacyEfficacy--Each SessionEach Session
•• Goal SettingGoal Setting•• Behavioral ContractingBehavioral Contracting•• ProblemProblem --solvingsolving•• FeedbackFeedback•• Social SupportSocial Support
Goal Setting/Making a PlanGoal Setting/Making a PlanParts of a PlanParts of a Plan
•• Something the stroke survivor wants to doSomething the stroke survivor wants to do•• Something the stroke survivor can accomplish Something the stroke survivor can accomplish
over a few weeksover a few weeks•• Is behavior specificIs behavior specific•• Answers the questionsAnswers the questions
–– What?What?–– How long?How long?–– When?When?–– How often?How often?•• Survivor has the confidence level of 7 or Survivor has the confidence level of 7 or
more more (where 0 means not confident at all & 10 means (where 0 means not confident at all & 10 means totally confident)totally confident)
8
Secondary Stroke Prevention Secondary Stroke Prevention and Patient Selfand Patient Self--ManagementManagement•• Many Risk FactorsMany Risk Factors
–– Multiple behavior change is Multiple behavior change is challengingchallenging
–– We assess stroke risk factors in We assess stroke risk factors in session 1 session 1
–– Try to help the patient negotiate with Try to help the patient negotiate with self to start with one risk factor self to start with one risk factor �� ChallengeChallenge�� Focus on one before moving on to Focus on one before moving on to
anotheranother�� When to move onto next behaviorWhen to move onto next behavior�� Simultaneous preferencesSimultaneous preferences
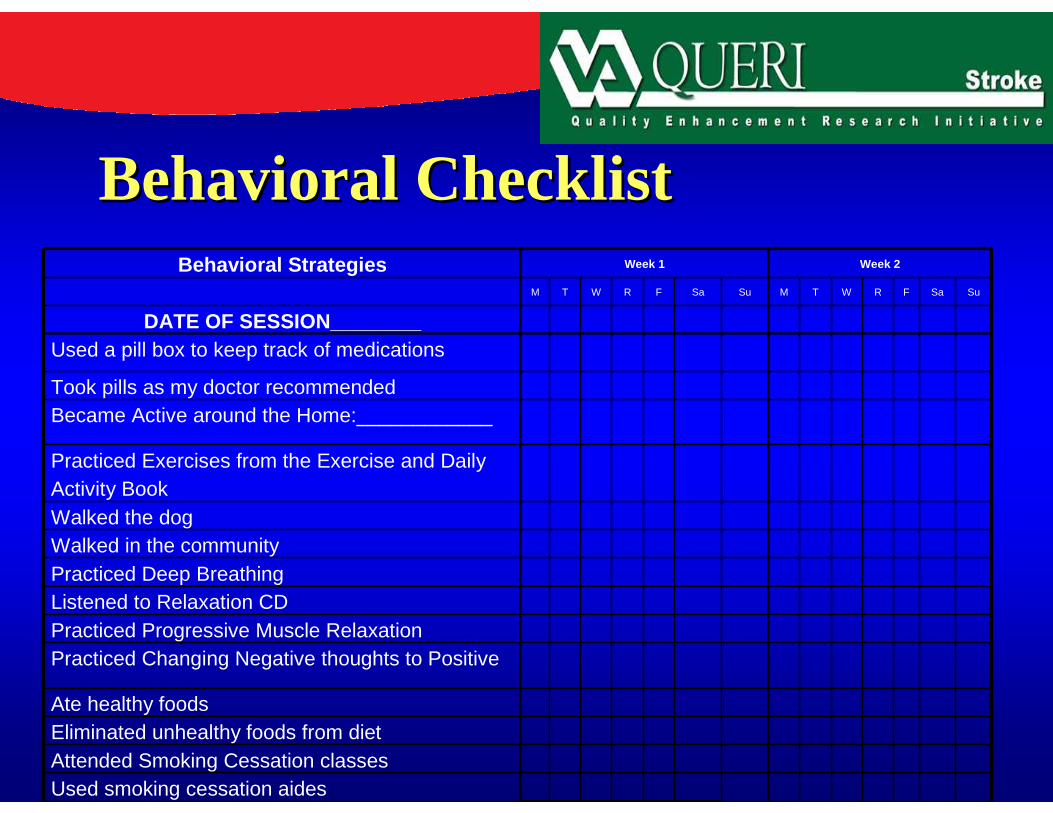
Behavioral ChecklistBehavioral ChecklistBehavioral Strategies Week 1 Week 2
M T W R F Sa Su M T W R F Sa Su
DATE OF SESSION________Used a pill box to keep track of medications
Took pills as my doctor recommended Became Active around the Home:____________
Practiced Exercises from the Exercise and Daily Activity BookWalked the dogWalked in the communityPracticed Deep BreathingListened to Relaxation CDPracticed Progressive Muscle RelaxationPracticed Changing Negative thoughts to Positive
Ate healthy foodsEliminated unhealthy foods from dietAttended Smoking Cessation classesUsed smoking cessation aides

Examples of Stroke Survivor Examples of Stroke Survivor plan plan –– Specific and Small StepsSpecific and Small Steps
•• I will walk 30 minutes after I will walk 30 minutes after breakfast around my neighborhood breakfast around my neighborhood or in the mall 3 days a weekor in the mall 3 days a week
•• I will measure my blood glucose I will measure my blood glucose once a day before breakfast in the once a day before breakfast in the bathroom.bathroom.
•• I will check my blood pressure I will check my blood pressure once a week at 4 p.m. in my living once a week at 4 p.m. in my living room easy chair.room easy chair.
•• I have a confidence level of 9 I have a confidence level of 9 11

Pilot:Patient Eligibility Pilot:Patient Eligibility CriteriaCriteria
•• Hospitalized for ischemic stroke at Hospitalized for ischemic stroke at 2 VA facilities: Indy and Gainsville2 VA facilities: Indy and Gainsville
•• No evidence of current substance No evidence of current substance abuseabuse
•• Not deemed terminally ill by Not deemed terminally ill by physicianphysician
•• Ability to speak English prior to Ability to speak English prior to dischargedischarge
•• Ability to selfAbility to self --care prior to care prior to dischargedischarge
•• Must have access to a telephoneMust have access to a telephone

FunctioningFunctioning•• Physical Physical –– must be able to selfmust be able to self --carecare•• Cognitive Cognitive --Screen with Short Screen with Short
Portable Mental Status Portable Mental Status Questionnaire (SPMSQ)Questionnaire (SPMSQ)
•• Dx of Dementia Dx of Dementia –– pass SPMSQ pass SPMSQ then eligiblethen eligible
•• Language FunctioningLanguage Functioning–– National Institutes of Health (NIH) National Institutes of Health (NIH)
Stroke Scale Stroke Scale –– Retrospective NIHSSRetrospective NIHSS

Design Design –– PILOT RCTPILOT RCTIndianapolis VAMCIndianapolis VAMC•• Recruited 41 veterans Recruited 41 veterans
hospitalized with hospitalized with ischemic stroke ischemic stroke
•• 19 Intervention19 Intervention
•• 22 Attention Control22 Attention Control
Gainesville VAMCGainesville VAMC•• Recruited 22 veterans Recruited 22 veterans
hospitalized with hospitalized with ischemic stroke ischemic stroke
•• 10 Intervention10 Intervention
•• 11 Attention Control11 Attention Control
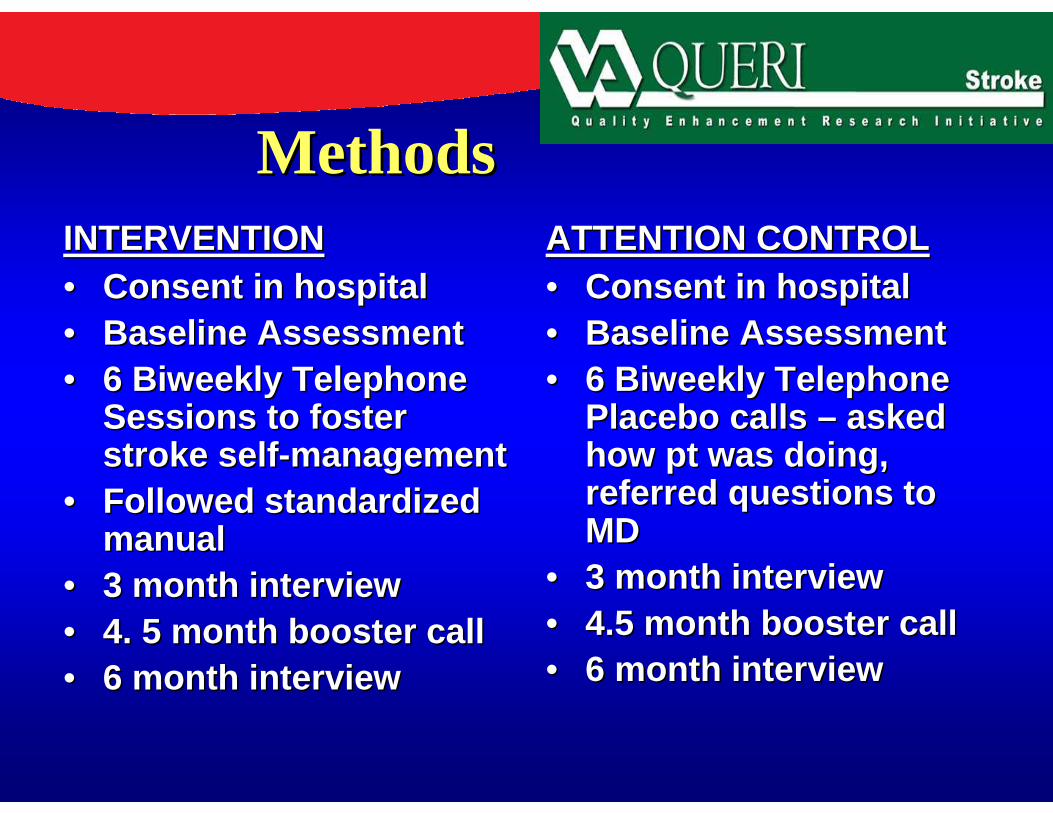
MethodsMethodsINTERVENTIONINTERVENTION•• Consent in hospitalConsent in hospital•• Baseline AssessmentBaseline Assessment•• 6 Biweekly Telephone 6 Biweekly Telephone
Sessions to foster Sessions to foster stroke selfstroke self --managementmanagement
•• Followed standardized Followed standardized manualmanual
•• 3 month interview3 month interview•• 4. 5 month booster call4. 5 month booster call•• 6 month interview6 month interview
ATTENTION CONTROLATTENTION CONTROL•• Consent in hospitalConsent in hospital•• Baseline AssessmentBaseline Assessment•• 6 Biweekly Telephone 6 Biweekly Telephone
Placebo calls Placebo calls –– asked asked how pt was doing, how pt was doing, referred questions to referred questions to MDMD
•• 3 month interview3 month interview•• 4.5 month booster call4.5 month booster call•• 6 month interview6 month interview
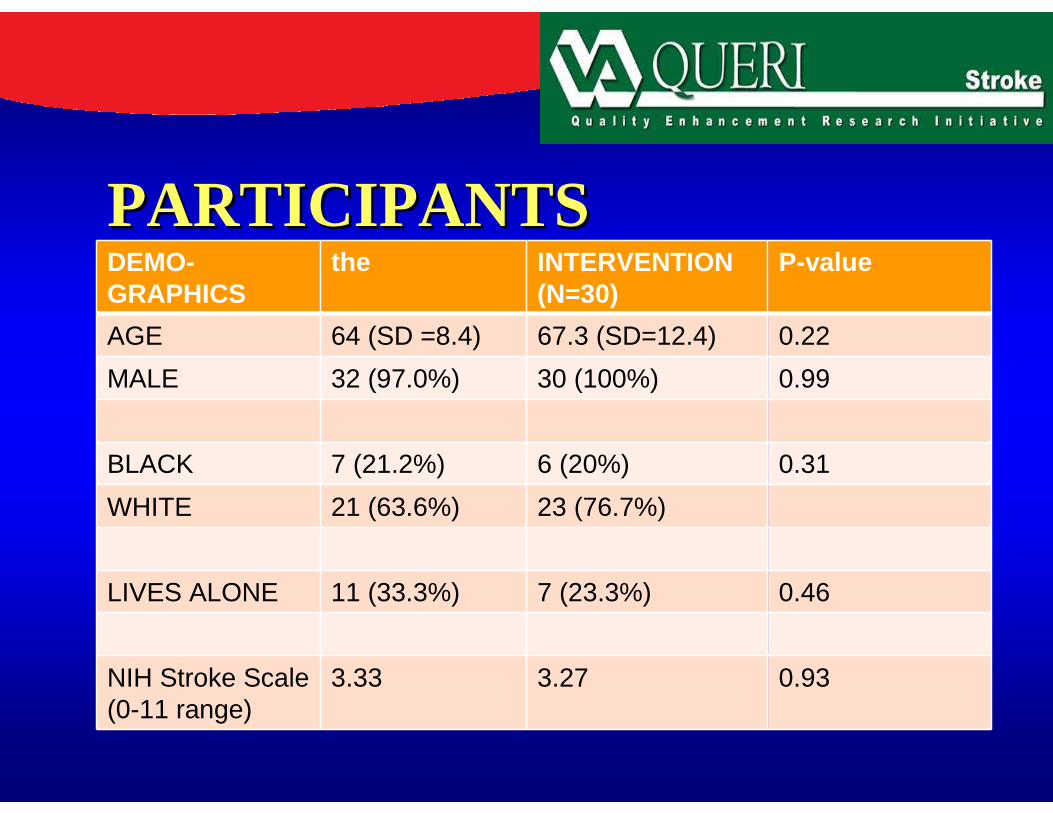
PARTICIPANTSPARTICIPANTSDEMO-GRAPHICS
the INTERVENTION (N=30)
P-value
AGE 64 (SD =8.4) 67.3 (SD=12.4) 0.22
MALE 32 (97.0%) 30 (100%) 0.99
BLACK 7 (21.2%) 6 (20%) 0.31
WHITE 21 (63.6%) 23 (76.7%)
LIVES ALONE 11 (33.3%) 7 (23.3%) 0.46
NIH Stroke Scale (0-11 range)
3.33 3.27 0.93

SESSIONS DELIVEREDSESSIONS DELIVERED
INTERVENTION (N=29)INTERVENTION (N=29)
•• Mean # (SD) Sessions Mean # (SD) Sessions delivered = 5.0 (1.8) delivered = 5.0 (1.8)
ATTENTION CONTROL (N=33)ATTENTION CONTROL (N=33)
•• Mean #(SD) Sessions Mean #(SD) Sessions delivered = 5.7 (0.98)delivered = 5.7 (0.98)

% Developed Behavior Plan % Developed Behavior Plan Per SelfPer Self--Management SessionManagement Session
•• Session 1 = 100% Session 1 = 100% •• Session 2 = 89.6%Session 2 = 89.6%•• Session 3 = 86.2%Session 3 = 86.2%•• Session 4 = 75.8%Session 4 = 75.8%•• Session 5 = 72.4%Session 5 = 72.4%•• Session 6 = 72.4%Session 6 = 72.4%

Frequently Reported Frequently Reported Activities in Behavior PlansActivities in Behavior Plans
•• 31% 31% -- Became Became active around the active around the homehome
•• 21.3% Walked in 21.3% Walked in the communitythe community
•• recommendedrecommended•• 14.1% Ate healthy 14.1% Ate healthy
foods foods •• 14% Eliminated 14% Eliminated
unhealthy foodsunhealthy foods
•• 13.7%Practiced 13.7%Practiced other physical other physical activityactivity
•• 10 % Listened to 10 % Listened to relaxation CDrelaxation CD
•• 8% Practiced 8% Practiced Rehab exercisesRehab exercises
•• 7.3% Took pills as7.3% Took pills asprescribedprescribed

Measurement OutcomesMeasurement Outcomes
–– SelfSelf --efficacy to perform self efficacy to perform self management behaviors (Lorig et al 96)management behaviors (Lorig et al 96)�� Present time perceptionPresent time perception
–– SelfSelf --management behaviors (Lorig et management behaviors (Lorig et al 96) during past weekal 96) during past week
–– Stroke Specific QOL (Williams LS)Stroke Specific QOL (Williams LS)�� Ask about activities and feelings during Ask about activities and feelings during
past week.past week.

Measurement Outcomes Measurement Outcomes (Cont)(Cont)
•• Process of SelfProcess of Self --ManagementManagement–– Behavioral checklists from 6 sessionsBehavioral checklists from 6 sessions–– Fidelity checklist of session contentsFidelity checklist of session contents–– Chart reviews of secondary stroke Chart reviews of secondary stroke
management clinical values during 6 management clinical values during 6 months postdischarge months postdischarge ––( eg, bp, ( eg, bp, smoking cessation)smoking cessation)

Analysis PlanAnalysis Plan•• Change from baseline to 3 and 6 Change from baseline to 3 and 6
months was modeled by a linear months was modeled by a linear model with fixed effects for model with fixed effects for treatment, visit, and treatment x treatment, visit, and treatment x visit interaction, a random subject visit interaction, a random subject for repeated measurement, and for repeated measurement, and adjustment for baseline score.adjustment for baseline score.
•• Response at 3 months was carried Response at 3 months was carried forward for missing 6 month forward for missing 6 month responsesresponses
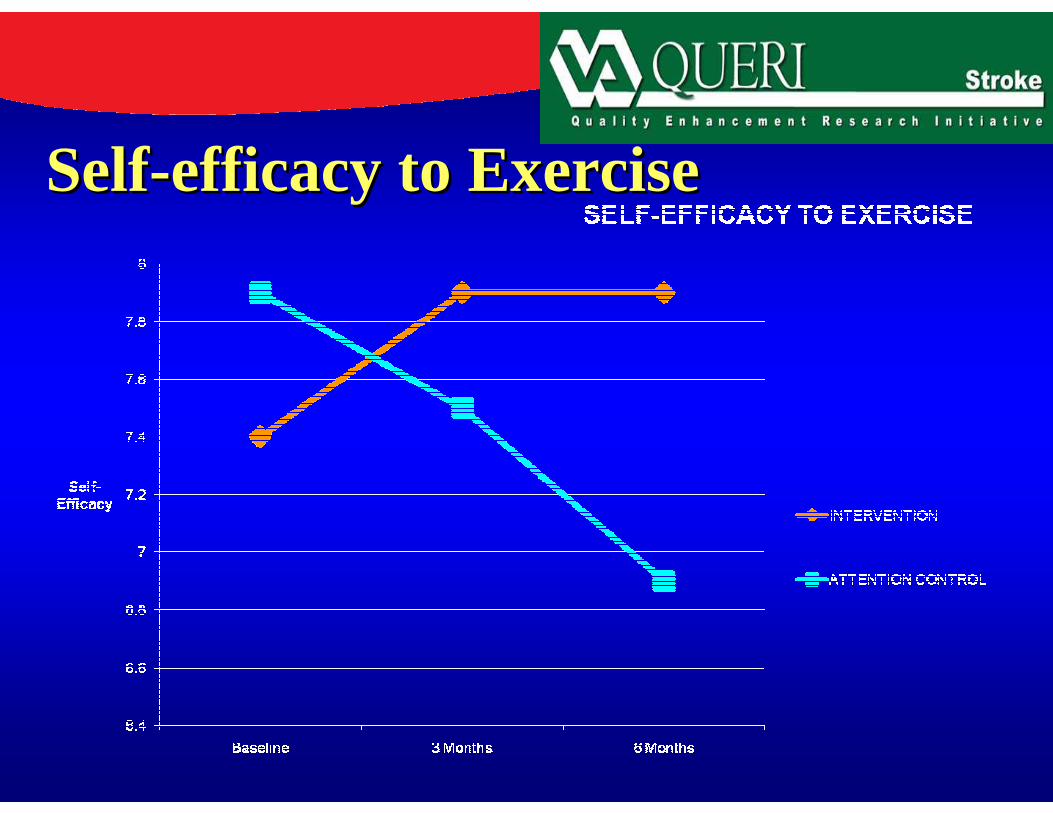
SelfSelf--efficacy to Exercise efficacy to Exercise

SelfSelf--Efficacy: MD CommunicationEfficacy: MD Communication
Self Efficacy: Communicate with Physician

Minutes Spent in Aerobic ActivitiesMinutes Spent in Aerobic Activities
Self Management: Past Week Minutes Spent in Aerobics

SSQOL: Family RolesSSQOL: Family Roles
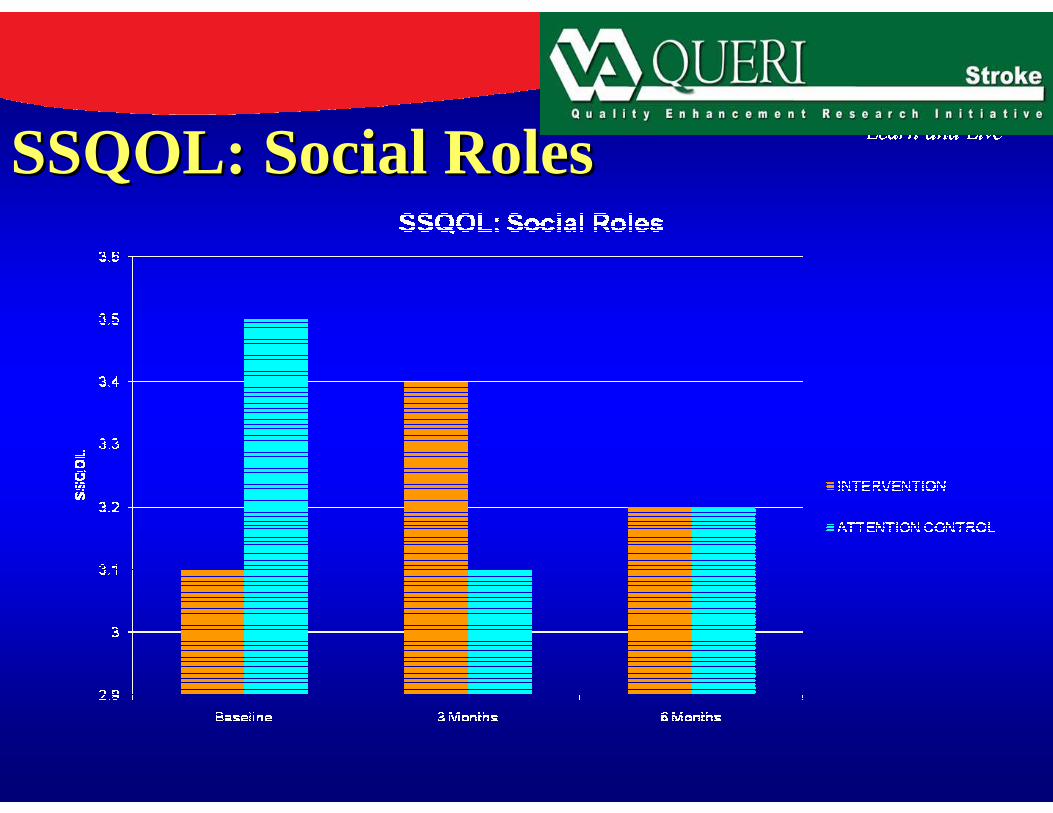
SSQOL: Social RolesSSQOL: Social Roles

LimitationsLimitations•• Small Sample Small Sample --Limited statistical Limited statistical
powerpower•• Multicomponent intervention Multicomponent intervention ––
difficult to untangle effects of each difficult to untangle effects of each componentcomponent
•• Participants targeted different Participants targeted different behaviors and risk factorsbehaviors and risk factors
•• Results are limited to veteran Results are limited to veteran stroke survivors with the ability to stroke survivors with the ability to selfself --carecare

SummarySummary
��A Telephone based stroke self A Telephone based stroke self management program is feasible for management program is feasible for recently discharged patients with recently discharged patients with ischemic stroke. ischemic stroke.
��A selfA self --management format may be a management format may be a venue for secondary stroke venue for secondary stroke prevention.prevention.
��We are reviewing postdischarge We are reviewing postdischarge clinical data to evaluate reduction in clinical data to evaluate reduction in risk factors.risk factors.
��Programs longer in duration may Programs longer in duration may sustain initial changes.sustain initial changes.



![Arm rehabilitation in post stroke subjects: A randomized ...€¦ · hemiparetic forearm of selected stroke patients [26]. Motor learning principles required for CNS-activity-dependent](https://img.pdfslide.us/doc/110x75/5edf184bad6a402d666a7229/arm-rehabilitation-in-post-stroke-subjects-a-randomized-hemiparetic-forearm.jpg)
























