Embed Size (px)
DESCRIPTION
Article
Citation preview

Stroke in Women: What is Different?
Dara G. Jamieson & Maryna Skliut
Published online: 21 May 2010# Springer Science+Business Media, LLC 2010
Abstract Stroke, a major cause of morbidity and mortality inthe general population, varies in incidence in men and womenof different age groups: more boys than girls have strokes; theincidence of stroke is greater in men in their 60s and 70s; andstroke is more common in women after age 80 years. Thesedifferences are attributed to hormonal (sex-related) changesand variable risk factors in women, as well as lifestyle andenvironmental (gender-related) co-morbid conditions. Awoman, who is more likely to have a stroke in her lifetimethan a myocardial infarction, has a different response toprimary and secondary prevention as compared with a man.Although response to thrombolysis is similar, older age andmore severe strokes in women lead to poorer outcomes infemale stroke survivors.
Keywords Stroke . Gender . Sex .Women .
Stroke treatment . Stroke risk factors . Pregnancy
Introduction
According to 2010 report from American Heart Association(AHA), each year about 795,000 people in the United
States have new or recurrent stroke [1••]. The same reportstates that approximately 55,000 more women than menhave a stroke each year. Community-based data on a groupof North Americans of European descent indicate that thelifetime risk of stroke for a middle-aged woman is 1 in 5and for a middle-aged man the risk is 1 in 6 [2]. The femalepredominance is not present in all ages and is expressedmostly in older women. Boys have more strokes than girls.In the age group of 65 to 74 years, the male-to-female-predominance-of-stroke ratio is 1.5. This ratio goes down to0.76 in the age group of ≥85 years. Women ages 45 to 54have a likelihood of developing a stroke twice as high asman in the same age group. The risk of stroke in womenincreases with age: there is a fourfold increase in thelikelihood of stroke in women ages 45 to 54 years comparedwith the ages of 35 to 44 years [3]. More women than men dieof stroke each year. In the United States, 60.6% of strokedeaths in 2006 were women. The decline in stroke-relateddeath is greater in women than in men, with the age adjustedmale-to-female ratio decreasing from 1.1 to 1.03. Commonrisk factors for stroke are applied to women as they are tomen, but women carry a significant number of specific riskfactors, including hormonal states like pregnancy andmenopause, predisposition to particular female predominantdiseases with increased stroke risk (such as migraine), andlongevity (resulting in higher risk of atrial fibrillation andassociated stroke risk) [4••]. Age is also an independentand the strongest risk factor for stroke. It is also a negativepredictive factor for poor outcomes after stroke [2].
Sex Versus Gender Influences on Stroke Risk in Women
Risk of stroke and response to treatment in women can bedivided into sex (hormonal) and gender (environmental)
D. G. Jamieson (*)Department of Neurology and Neuroscience,New York Presbyterian Hospital,Weill Cornell Medical College of Cornell University,525 E 68 St., F610,New York, NY 10065, USAe-mail: [email protected]
M. SkliutDepartment of Neurology, Beth Israel Medical Center,10 Union Square East, 5D,New York, NY 10003, USAe-mail: [email protected]
Curr Atheroscler Rep (2010) 12:236–243DOI 10.1007/s11883-010-0118-3

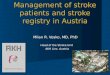
influences, as noted in Table 1. Hormonal fluctuations thatwomen experience through their lifetime and conditionsthat have higher prevalence in females, such as migraineheadache, exogenous estrogen, and pregnancy, increase awoman’s risk of stroke. In 2006, the National Institute ofNeurological Disorders and Stroke (NINDS) sponsored amultidisciplinary working group who published an overviewof our current understanding of the role of estrogen, bothendogenous and exogenous, in stroke risk, as well asrecommendations for future investigation [5]. Multipleepidemiologic studies, including the Women’s Health Study(WHS) [6–9, 10•], the Women’s Health Initiative (WHI) [11,12•, 13, 14], and the Northern Manhattan Stroke Study(NOMAS) [15, 16] have revealed vascular risk factorsrelevant to women.
Sex-Related Influences in Stroke Risk
Estrogen properties, as related to stroke risk, are paradoxical,with inconsistent translation from laboratory to clinicalobservations. Pretreatment with estradiol protects the cortexfrom cell death in a middle cerebral artery occlusion in arodent model, yet no clinical benefit is conferred by estradioltreatment of acute ischemic stroke. Although endogenousestradiol appears to be neuroprotective and may decrease a
woman’s risk of cardiovascular disease, exogenous estrogen(hormone replacement therapy) actually increases the risk ofcoronary heart disease or stroke in older postmenopausalwomen. Circulating endogenous estradiol is associated withincreased stroke risk in older postmenopausal women. Aprospective case-control study found that endogenous estradiollevel is an indicator of stroke risk in older postmenopausalwomen, especially in those with greater central adiposity.Potential mediators included atherogenic dyslipidemia, insulinresistance, and inflammation [17].
Multiple mechanisms of action may explain the compli-cated and contradictory effects of endogenous and exogenousestrogen in stroke risk. Nitric oxide synthase, which isexpressed within the vascular wall, is a target of estrogenaction, with different effects as a function of age. In youngerwomen estrogen produces a beneficial effect (production ofnitric oxide), but a deleterious product (superoxide) is formedin older women [18]. Although variations in the estrogenalpha receptor (ESR1) gene appear to be strongly associatedwith risk of ischemic heart disease, an association betweenvariations in the ESR1 gene and risk of stroke has not beenreplicated [19].
The role of serum and radiologic markers to predictvascular risk is unclear and controversial irrespective oftheir specificity and patient’s sex. Whether markers, proven
Sex: biological attributes of men or women
Estrogen
Possible neuroprotective effect
Decreased stroke size in animal MCA stroke models
Low premenopausal stroke rates
Antioxidant, antiapoptotic, antiglutamate, increased cGMP
Possible proinflammatory effect
Increased CRP (dose dependent)
Possible increase in cerebral blood flow
Increased eNO, increased prostacyclin, stimulation of angiogenesis
Possible prothrombotic effect
Venous thrombosis
Inherited predisposition for Factor V Leiden and prothrombin gene mutation
Effect on platelet activation
Female conditions with increased stroke risk
Exogenous estrogen treatment
Pregnancy
Migraines
Gender: the behavioral, cultural, or psychological attributes of men or women
Women
Lifestyle
Increased life expectancy
Care-giver vs care-receiver
Access to appropriate health care
Social isolation
Table 1 Women: effect of sexand gender on stroke
cGMP cyclic guanosinemonophosphate, CRP C-reactiveprotein, eNO endothelial nitricoxide, MCA middle cerebralartery
Curr Atheroscler Rep (2010) 12:236–243 237

or putative, can predict cerebrovascular, as distinct fromgeneral vascular or cardiovascular, risk is uncertain. Althoughdyslipidemia is more closely linked to cardiovascular than tocerebrovascular risk, elevations in total cholesterol, low-density lipoprotein (LDL) cholesterol, the total cholesterol tohigh-density lipoprotein (HDL) cholesterol ratio, and non-HDL cholesterol were significantly associated with anincreased risk of ischemic stroke in the WHS [6].
A study following 250 healthy postmenopausal womenfound that fibrinogen, carotid lesions, and high-sensitivityC-reactive protein (hs-CRP) were predictors of vascularevents [20]. However, although there was a correlation withrisk of myocardial infarction (MI), there was no correlationwith ischemic stroke risk. Fibrinogen, along with LDL, hasbeen correlated with the progression of carotid intima-mediathickness (IMT) in women. The Tromso Study, which usedultrasonography, showed sex-dependent differences in associ-ations between measures of carotid atherosclerosis, MI, andinflammatory markers. Carotid atherosclerosis predicted first-ever MI in women (absolute risk reduction=3.95; 95% CI,2.16–7.19) compared with men (absolute risk reduction=1.56;95% CI, 1.04–2.36). Women and men with carotid plaque hadsignificantly elevated levels of white blood cells (WBC) andfibrinogen, but not CRP, with a significant association betweenWBC and plaque echogenicity in women [21, 22]. Estrogenand sex hormone binding globulin have been associated witha reduction in carotid IMT in healthy postmenopausalwomen, indicating a potential marker for reduced vascularrisk, mediated through beneficial effects on lipids.
More specific markers of risk of stroke are being identified.Hepatocyte growth factor (HGF), a potent angiogenic factor,plays a role in the development and progression of athero-sclerotic lesions. Circulating levels of HGF are associatedwith an increased risk of incident ischemic stroke, independentof obesity and other risk factors for cardiovascular disease,among postmenopausal women aged 50 to 79 years in theWHI [11].
Lipoprotein-associated phospholipase A2 (Lp-PLA2)appears to be a reliable marker of risk for cardiovascularevents, including ischemic stroke. In the Northern Manhattanstudy, stroke patients with Lp-PLA2 activity levels in thehighest quartile compared with those in the lowest quartilehad an increased risk of recurrence after first ischemic stroke[16]. Investigators in the WHI found that among postmen-opausal women not using hormone replacement therapy,levels of the biomarker Lp-PLA2 in the highest quartilecompared with those in the lowest was independentlyassociated with a 64% increased risk of ischemic stroke[23]. The increased risk persisted after adjustment fortraditional cardiovascular risk factors (odds ratio=1.55;95% CI, 1.05–2.28). There was no association of Lp-PLA2
with stroke risk among women using hormone replacementtherapy. Among nonusers of hormone replacement therapy,
the association of Lp-PLA2 with stroke risk was strongest inwomen who also had elevated hs-CRP. In healthy postmen-opausal women, hs-CRP also appears to be a strong predictorof the risk of cardiovascular events [13].
Intracranial stenosis appears to be a marker for vascularrisk that is especially prescient in women [24]. TheWarfarin-Aspirin Symptomatic Intracranial Disease(WASID) trial found that women with intracranial stenosiswere at greater risk of stroke or vascular death (28.4% forwomen; 16.6% for men) [25]. After accounting fortraditional vascular risk factors and stroke severity, womenhad almost a twofold increased risk of stroke comparedwith men, and a 1.6-fold increased risk of combinedoutcome (stroke or vascular death).
Gender-Related Influences in Stroke Risk
Gender-specific risk factors for women relate to theirlifestyle and environment. Lifestyle issues are recognizedfor their important role in risk of cerebrovascular disease[26]. Kurth et al. [9] used data from the WHS of almost38,000 healthy female health professionals aged 45 yearsand older to look at lifestyle and weight as risk factors forstroke. Healthy lifestyle in the WHS was defined as 1)abstinence for smoking, 2) body mass index (BMI) lessthan 22 kg/m2, 3) exercise ≥4 times/week, 4) alcoholconsumption of 4 to 10.5 drinks per week, and 5) diet highin cereal fiber, folate, omega-3 fatty acids; high polyunsat-urated to saturated fat ratio; low in trans fat; low inglycemic load. A composite healthy lifestyle was associatedwith a significantly reduced total and ischemic stroke risk,but not with reduced hemorrhagic stroke risk. Theassociation was apparent even after controlling for hyper-tension, diabetes, and elevated cholesterol. Analysis of theindividual components of the healthy life style showedsubstantial reduction of stroke risk in nonsmokers andwomen with lower BMI. The associations with alcoholconsumption and physical activity were weaker. The healthierdiet paradoxically increased risk of ischemic and hemorrhagicstroke, but the overall risk outcomes were unchanged withexclusion of diet data. Data from the Northern Manhattanstudy suggest that increased daily total fat intake, especiallyabove 65 g, significantly increases risk of ischemic stroke in apredominantly female population [27].
Obesity is a strong risk factor for ischemic stroke, with aless clear relationship with hemorrhagic stroke. Markers ofabdominal adiposity are strongly associated with the risk ofischemic stroke or transient ischemic attack [28]. In the WHS,there was a statistically significant trend for increased risk ofischemic stroke with BMI greater than 30 kg/m2 but theassociation was highly mediated by hypertension, diabetes,and elevated cholesterol [8]. Women who were currentcigarette smokers had increased risk of stroke irrespective of
238 Curr Atheroscler Rep (2010) 12:236–243

BMI. The association between BMI and hemorrhagic strokein women was inconsistent. Physical activity reduces the riskof stroke. A study of combined work and leisure activity inmen and women confirmed this data, showing about 40%risk reduction for stroke in the most active group [29].
Female-Predominant Stroke-Related Conditions
Women’s Lifetime Risk of Stroke
Hormonal influences dictate a woman’s stroke risk throughouther life. Menarche before age 12 years is associated withincreased vascular risk, cardiac disease events, and overallmortality, with the association only partly mediated byincreased adiposity. However, the risk of stroke is notinfluenced by age of menarche [30].
Pregnancy
Pregnancy increases the immediate and future risk ofischemic and hemorrhagic stroke. Past pregnancies canalso increase future stroke risk. Multiple deliveries havebeen shown to increase a woman’s risk of hemorrhagicstroke, both intracerebral hemorrhage (ICH) and subarach-noid hemorrhage (SAH) [31]. The risk of cerebral infarc-tion or hemorrhagic stroke is greater in the postpartumperiod compared with during pregnancy [32]. The excessrisk for either type of stroke during or within 6 weeks afterpregnancy is 8.1 strokes per 100,000 pregnancies (95% CI,6.4–9.7). In pregnancy, the rate of ICH is equal to or greaterthan the rate of ischemic stroke, whereas the incidence ofischemic stroke is much greater than that of hemorrhagicstroke in nonpregnant women in the same age range [33].
Pregnancy-associated ischemic strokes are usually due toembolism (venous or cardiac thrombus, fat, amniotic fluid,air, or choriocarcinoma). Cerebral venous thrombosis orleakage from a vascular malformation can cause peri-partumICH. Subarachnoid hemorrhage due to aneurysmal rupture isa major cause of maternal mortality during pregnancy, withhigh fetal mortality as well. Preeclampsia and eclampsiacomplicate about 5% to 8% of pregnancies and are importantrisk factors for both hemorrhagic and ischemic stroke.Preeclampsia or eclampsia was found in 24% of women withcerebral infarction and 14% of women with intracerebralhemorrhage [32]. Risk of ischemic stroke after pregnancyand the puerperium is increased in women with a history ofpreeclampsia [33].
Oral Contraception
Although the correlation between oral contraceptives andstroke risk has been debated for decades, the evidence for
an association, independent of traditional vascular riskfactors, is not clear. Meta-analyses of studies published upto 2002 (with patient data collection up to 1995) reportedvariable risk depending on study design [34]. Doses ofestrogen greater than 50 μg were associated with greaterrisk than lower doses. The absolute risk was noted to below, with only an additional 4.1 ischemic strokes per100,000 nonsmoking, normotensive women using low-doseestrogen oral contraceptives. A population based cohortstudy in the Netherlands, the Risk of Arterial Thrombosis inRelation to Oral Contraceptives (RATIO) study, reportedthat current oral contraceptive use was associated with arisk of stroke twice that of nonusers; smoking, hyperten-sion, hypercholesterolemia, diabetes, and obesity conferredsignificantly increased risk in combination with oralcontraception [35]. Thrombophilias, specifically Factor VLeiden and the G20210A prothrombin gene mutation,increase the risk of cerebral venous thrombosis in users oforal contraceptives. Ischemic stroke risk, in associationwith oral contraceptives, has also been shown to beincreased in women with Factor V Leiden or methylenete-trahydrofolate reductase (MTHFR) 677TT polymorphism[36].
Menopause
The increased stroke risk in postmenopausal womanappears to be due to a combination of age and hormonalchanges caused by decreasing estrogen levels. Althoughestrogen has been shown to be neuroprotective in animalischemic stroke models, a neuroprotective effect of humanestrogen supplementation has not been confirmed in clinicaltrials. Observational cohort studies of the use of hormonereplacement therapy on stroke risk in postmenopausalwomen have shown mixed results [37]. The conflictingresults of these studies could be secondary to the differences inthe age of participants, dose of estrogen used, time ofadministration (pre/postmenopausal), preparation form, pre-morbid conditions, and genetic predisposition [38]. The WHIshowed a 44% increased incidence in ischemic stroke withestrogen plus progestin treatment of healthy women whowere on average a decade into menopause [14]. The Heartand Estrogen/Progestin Replacement Study found that inwomen with increased risk of vascular events due tocoronary heart disease, hormone replacement therapy offeredno primary protection against ischemic stroke [39]. A studyfound that there is an increased risk for the combination oftransient ischemic attack (TIA), ischemic stroke, andhemorrhagic stroke associated with the use of hormonereplacement therapy, with the greatest increase in risk duringthe first year of treatment [40]. Estrogen supplementation hasalso not been shown to be of benefit in secondary strokeprevention [41].
Curr Atheroscler Rep (2010) 12:236–243 239

Migraine
Approximately 21 million American women have migraineheadaches, making it a female-predominant disorder. In theWHS, migraine with aura was found to increase the risk ofischemic stroke as well as MI, coronary revascularization,and angina [7]. Migraines without aura and non-migraineheadaches were not associated with increased vascular risk.Although migraine with aura appears to confer an increasedvascular risk, migraine without aura may also be associatedwith some degree of vascular risk [42].
Stroke Prevention in Women
Women have different degrees of risk reduction with medicaland surgical therapy for stroke prevention compared withmen. The reasons for this differential response to therapy arepoorly understood.
Antiplatelet Therapy
Multiple clinical trials verify the benefit of long-termantiplatelet therapy in the reduction of recurrent ischemicstroke in both men and women. However, women mayrespond differently to aspirin therapy than men, in primaryprevention. Women appear to benefit from aspirin forprevention of a first stroke, an effect not as striking in men[12•, 43, 44]. The pathophysiologic mechanisms for theperceived clinical difference is not clear, but may reflectdifferences in aspirin metabolism or aspirin resistance, aswell as the gender difference in incidence of stroke and MI.The WHS showed that in women (mean age, 54.6 years),low-dose aspirin (100 mg every other day) had a protectiveeffect against a first stroke, but generally offered noprotection against MI and cardiovascular death except inwomen aged 65 years and older [43]. Among women in theplacebo group, there was a stroke to MI ratio of 1.4:1compared with a ratio of 0.4:1 among men in the Physicians’Health Study [44]. A sex-specific meta-analysis of aspirintherapy for the primary prevention of cardiovascular eventsfound that aspirin therapy was associated with a 24%reduced rate of ischemic stroke, with no apparent effect onhemorrhagic stroke in women [45]. Analysis of data frompostmenopausal women with stable cardiovascular diseaseenrolled in the WHI found aspirin use (with no differencebetween 81 mg and 325 mg) was associated with signifi-cantly lower risk of all-cause mortality [12•]12.
Carotid Endarterectomy and Carotid Angioplasty with Stenting
Although women with ischemic stroke or TIA are less likelythan men to undergo carotid screening and revascularization,
this difference is largely explained by potential contraindica-tions to surgery and by sex differences in the severity ofcarotid disease [46]. Carotid revascularization is widely usedfor primary and secondary stroke prevention in both men andwomen. Although data from older studies suggested thatcarotid endarterectomy (CEA) for prevention of initial andrecurrent stroke risk reduction in women may have lessbenefit than in men, this conclusion has been challenged[47]. Recent analysis of data from the Oxford VascularStudy found that lower rates of surgical intervention for50% to 99% symptomatic carotid stenosis in women couldbe explained by sex differences in population-basedincidence [48]. Restenosis rates after carotid surgery areincreased in women compared with men [49]. Smaller vesselsize and increased vessel redundancy in women maycontribute to their increased restenosis risk. Carotid angio-plasty with stenting is an alternative for CEA. Recent reportsindicate that there are no substantial gender influences onclinical outcomes or durability of carotid artery revasculari-zation following CEA or carotid angioplasty with stenting[47, 50–52].
Acute Stroke Treatment and Outcome
Presentation and outcomes of acute stroke in women aredifferent compared with men. Women, especially elderlywomen, may be less likely to be evaluated within the first 3hours after symptom onset [53]. Significantly fewer women(62%) receive imaging within 1 hour of emergencydepartment arrival than men [54]. Women have moresevere strokes and higher National Institutes of HealthStroke Scale (NIHSS) scores on presentation [55, 56]. Arecent study of gender differences in acute care showed thatwomen arrived in the emergency department at equivalenttimes and had similar baseline functional status. In thisstudy, women had similar NIHSS scores as men. Despitesimilar baseline characteristics, women had worse out-comes at 3 and 12 months, leading to the conclusion thatthe female sex, or gender-related lack of support systems,predisposes to poorer outcomes after acute ischemic stroke[57].
Women have worse functional outcome after having astroke, possibly related to advanced age and more frequentco-morbid conditions [58]. Quality of life, in particularmental health and physical function, has been found to belower in women after stroke. This difference persists evenafter correction for age and stroke severity. Treatmentdifferences may also play a role in this gender disparity infunctional outcome. Women are less likely to be giventhrombolytic therapy for acute ischemic stroke, perhaps dueto advanced age at the time of stroke or delay until strokesymptoms are recognized and treated [59].
240 Curr Atheroscler Rep (2010) 12:236–243

There does not seen to be a consistent difference inbenefit from thrombolysis based on sex. The recanalizationrate may be higher in women than in men, and women maybe more likely to benefit from the treatment compared withmen [60]. Good functional outcome, as measured by afavorable Barthel Index and modified Rankin Scale (mRS),may be more likely for men than women, but women maybe more likely to survive for 3 months [61•]. Equallyfavorable clinical outcome (mRS 0–2) and recanalizationrate were seen in both men and women after intra-arterialtissue plasminogen activator treatment of middle cerebralartery and internal carotid artery occlusion [62].
Although men and women may have comparable outcomesafter treatment with tissue plasminogen activator, if untreated,women have poorer outcomes after acute stroke than men [63,64]. Women have a higher rate of cardioembolic strokes thanthrombotic and lacunar strokes, with a higher frequency ofatrial fibrillation as the etiology of their ischemic strokes.Greater mortality due to stroke may occur because womenare older, with more co-morbid medical conditions, at thetime they suffer a more severe stroke [55, 56]. Quality of life,in particular mental health and physical functioning, has beenfound to be lower in women after stroke. This difference wasfound to persist even after correction for age and strokeseverity.
Conclusions
Stroke is common in women because they have unique riskfactors and they outlive men. The incidence of stroke variesin men and women of different age groups. The male/female differences are attributed to hormonal (sex-related)changes and variable risk factors in women, as well aswomen’s lifestyle and environmental (gender-related) co-morbid conditions. The risk of ischemic and hemorrhagicstroke is increased in the post-partum period. Women canreduce ischemic stroke risk by not smoking and stayingthin. A woman is more likely to have a stroke in herlifetime than an MI, a differential vascular risk that shoulddirect her life-style modification and medications to reducestroke risk. She has a different response to primary andsecondary prevention compared with a man. Aspirin offersprimary prevention against ischemic stroke in women butnot in men. Hormone replacement therapy does not offereither primary or secondary cerebrovascular protection.Although response to thrombolysis is similar, older age andmore severe strokes in women lead to poorer outcomes infemale stroke survivors, who may lack a post-stroke supportnetwork.
Disclosure No potential conflicts of interest relevant to this articlewere reported other than both authors are women.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. •• Lloyd-Jones D, Adams RJ, Brown TM, et al.: Heart disease andstroke statistics–2010 update: a report from the American HeartAssociation. Circulation 2010, 121:e46–e215. This comprehensiveupdated report outlines the incidence and prevalence of vasculardisease in different populations.
2. Seshadri S, Wolf PA: Lifetime risk of stroke and dementia: currentconcepts, and estimates from the Framingham Study. LancetNeurol 2007, 6:1106–1114.
3. Towfighi A, Saver JL, Engelhardt R, Ovbiagele B: A midlifestroke surge among women in the United States. Neurology 2007,69:1898–1904.
4. •• Bushnell CD: Stroke and the female brain. Nat Clin PractNeurol 2008, 4:22–33. This review summarizes the sex differencesrelated to stroke, and the effect of endogenous and exogenoushormones on the vasculature of the female brain.
5. Bushnell CD, Hurn P, Colton C, et al.: Advancing the study ofstroke in women: summary and recommendations for futureresearch from an NINDS-Sponsored Multidisciplinary WorkingGroup. Stroke 2006, 37:2387–2399.
6. Kurth T, Everett BM, Buring JE, et al.: Lipid levels and the riskof ischemic stroke in women. Neurology 2007, 68:556–562.
7. Kurth T, Gaziano JM, Cook NR, et al.: Migraine and risk ofcardiovascular disease in women. JAMA 2006, 296:283–291.
8. Kurth T, Gaziano JM, Rexrode KM, et al.: Prospective study ofbody mass index and risk of stroke in apparently healthy women.Circulation 2005, 111:1992–1998.
9. Kurth T, Moore SC, Gaziano JM, et al.: Healthy lifestyle andthe risk of stroke in women. Arch Intern Med 2006, 166:1403–1409.
10. • Kurth T, Schurks M, Logroscino G, Buring JE: Migrainefrequency and risk of cardiovascular disease in women. Neurology2009, 73:581–588. The association between migraine and cardio-vascular disease varies by migraine frequency. Ischemic stroke isassociated with a high frequency of migraine with aura in women.
11. Rajpathak SN, Wang T, Wassertheil-Smoller S, et al.: Hepatocytegrowth factor and the risk of ischemic stroke developing amongpostmenopausal women. Results from the Women's HealthInitiative. Stroke 2010 (in press).
12. • Berger JS, Brown DL, Burke GL, et al.: Aspirin use, dose, andclinical outcomes in postmenopausal women with stable cardio-vascular disease: the Women's Health Initiative ObservationalStudy. Circ Cardiovasc Qual Outcomes 2009, 2:78–87. Aspirinuse (81 mg) was associated with significantly lower risk of all-cause mortality, specifically cardiovascular mortality, amongpostmenopausal women with stable vascular disease.
13. Kaplan RC, McGinn AP, Baird AE, et al.: Inflammation andhemostasis biomarkers for predicting stroke in postmenopausalwomen: the Women's Health Initiative Observational Study. JStroke Cerebrovasc Dis 2008, 17:344–355.
14. Rossouw JE, Anderson GL, Prentice RL, et al.: Risks and benefitsof estrogen plus progestin in healthy postmenopausal women:principal results From the Women's Health Initiative randomizedcontrolled trial. JAMA 2002, 288:321–333.
15. Elkind MS, Leon V, Moon YP, et al.: High-sensitivity C-reactiveprotein and lipoprotein-associated phospholipase A2 stabilitybefore and after stroke and myocardial infarction. Stroke 2009,40:3233–3237.
Curr Atheroscler Rep (2010) 12:236–243 241

16. Elkind MS, Tai W, Coates K, et al.: Lipoprotein-associatedphospholipase A2 activity and risk of recurrent stroke. CerebrovascDis 2009, 27:42–50.
17. Lee JS, Yaffe K, Lui LY, et al.: Prospective study of endogenouscirculating estradiol and risk of stroke in older women. ArchNeurol 2010, 67:195–201.
18. White RE, Gerrity R, Barman SA, Han G: Estrogen and oxidativestress: a novel mechanism that may increase the risk forcardiovascular disease in women. Steroids 2010 (in press).
19. Bos MJ, Schuit SC, Koudstaal PJ, et al.: Variation in the estrogenreceptor alpha gene and risk of stroke: the Rotterdam Study.Stroke 2008, 39:1324–1326.
20. Corrado E, Rizzo M, Muratori I, et al.: Older age and markers ofinflammation are strong predictors of clinical events in womenwith asymptomatic carotid lesions. Menopause 2008, 15:240–247.
21. Johnsen SH, Mathiesen EB, Joakimsen O, et al.: Carotidatherosclerosis is a stronger predictor of myocardial infarction inwomen than in men: a 6-year follow-up study of 6226 persons:the Tromso Study. Stroke 2007, 38:2873–2880.
22. Halvorsen DS, Johnsen SH, Mathiesen EB, Njolstad I: Theassociation between inflammatorymarkers and carotid atherosclerosisis sex dependent: the Tromso Study. Cerebrovasc Dis 2009, 27:392–397.
23. Wassertheil-Smoller S, Kooperberg C, McGinn AP, et al.:Lipoprotein-associated phospholipase A2, hormone use, and therisk of ischemic stroke in postmenopausal women. Hypertension2008, 51:1115–1122.
24. Williams JE, Chimowitz MI, Cotsonis GA, et al.: Genderdifferences in outcomes among patients with symptomaticintracranial arterial stenosis. Stroke 2007, 38:2055–2062.
25. Chimowitz MI, Lynn MJ, Howlett-Smith H, et al.: Comparison ofwarfarin and aspirin for symptomatic intracranial arterial stenosis.N Engl J Med 2005, 352:1305–1316.
26. Galimanis A, Mono ML, Arnold M, et al.: Lifestyle and strokerisk: a review. Curr Opin Neurol 2009, 22:60–68.
27. Boden-Albala B, Elkind MS, White H, et al.: Dietary total fatintake and ischemic stroke risk: the Northern Manhattan Study.Neuroepidemiology 2009, 32:296–301.
28. Winter Y, Rohrmann S, Linseisen J, et al.: Contribution of obesityand abdominal fat mass to risk of stroke and transient ischemicattacks. Stroke 2008, 39:3145–3151.
29. Myint PK, Luben RN, Wareham NJ, et al.: Combined work andleisure physical activity and risk of stroke in men and women in theEuropean prospective investigation into Cancer-Norfolk ProspectivePopulation Study. Neuroepidemiology 2006, 27:122–129.
30. Lakshman R, Forouhi NG, Sharp SJ, et al.: Early age at menarcheassociated with cardiovascular disease and mortality. J ClinEndocrinol Metab 2009, 94:4953–4960.
31. Jung SY, Bae HJ, Park BJ, Yoon BW: Parity and risk ofhemorrhagic strokes. Neurology 2010 (in press).
32. Kittner SJ, Stern BJ, Feeser BR, et al.: Pregnancy and the risk ofstroke. N Engl J Med 1996, 335:768–774.
33. Bateman BT, Schumacher HC, Bushnell CD, et al.: Intracerebralhemorrhage in pregnancy: frequency, risk factors, and outcome.Neurology 2006, 67:424–429.
34. Baillargeon JP, McClish DK, Essah PA, Nestler JE: Associationbetween the current use of low-dose oral contraceptives andcardiovascular arterial disease: a meta-analysis. J Clin EndocrinolMetab 2005, 90:3863–3870.
35. Kemmeren JM, Tanis BC, van den Bosch MA, et al.: Risk ofArterial Thrombosis in Relation to Oral Contraceptives (RATIO)study: oral contraceptives and the risk of ischemic stroke. Stroke2002, 33:1202–1208.
36. Slooter AJ, Rosendaal FR, Tanis BC, et al.: Prothromboticconditions, oral contraceptives, and the risk of ischemic stroke. JThromb Haemost 2005, 3:1213–1217.
37. Grodstein F, Stampfer MJ, Manson JE, et al.: Postmenopausalestrogen and progestin use and the risk of cardiovascular disease.N Engl J Med 1996, 335:453–461.
38. Ouyang P, Michos ED, Karas RH: Hormone replacement therapyand the cardiovascular system lessons learned and unansweredquestions. J Am Coll Cardiol 2006, 47:1741–1753.
39. Grady D, Herrington D, Bittner V, et al.: Cardiovascular diseaseoutcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA 2002,288:49–57.
40. Arana A, Varas C, Gonzalez-Perez A, et al.: Hormone therapy andcerebrovascular events: a population-based nested case-controlstudy. Menopause 2006, 13:730–736.
41. Viscoli CM, Brass LM, Kernan WN, et al.: A clinical trial ofestrogen-replacement therapy after ischemic stroke. N Engl J Med2001, 345:1243–1249.
42. Bigal ME, Kurth T, Santanello N, et al.: Migraine and cardiovasculardisease: a population-based study. Neurology 2010, 74:628–635.
43. Ridker PM, Cook NR, Lee IM, et al.: A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease inwomen. N Engl J Med 2005, 352:1293–1304.
44. Final report on the aspirin component of the ongoing Physicians’Health Study. Steering Committee of the Physicians’ Health StudyResearch Group. N Engl J Med 1989, 321:129–135.
45. Berger JS, Roncaglioni MC, Avanzini F, et al.: Aspirin for theprimary prevention of cardiovascular events in women and men: asex-specific meta-analysis of randomized controlled trials. JAMA2006, 295:306–313.
46. Kapral MK, Ben-Yakov M, Fang J, et al.: Gender differences incarotid imaging and revascularization following stroke. Neurology2009, 73:1969–1974.
47. Dorigo W, Pulli R, Marek J, et al.: Carotid endarterectomy infemale patients. J Vasc Surg 2009, 50:1301–1306, discussion 1306–1307.
48. Marquardt L, Fairhead JF, Rothwell PM: Lower rates of interventionfor symptomatic carotid stenosis in women than in men reflectdifferences in disease incidence: a population-based study. Stroke2010, 41:16–20.
49. Hugl B, Oldenburg WA, Neuhauser B, Hakaim AG: Effect of ageand gender on restenosis after carotid endarterectomy. Ann VascSurg 2006, 20:602–608.
50. De Rango P, Parlani G, Caso V, et al.: A comparative analysis ofthe outcomes of carotid stenting and carotid endarterectomy inwomen. J Vasc Surg 2010, 51:337–44, discussion 344.
51. Goldstein LJ, Khan HU, Sambol EB, et al.: Carotid artery stentingis safe and associated with comparable outcomes in men andwomen. J Vasc Surg 2009, 49:315–323, discussion 323–324.
52. Park B, Aiello F, Dahn MS, et al.: No gender influences on clinicaloutcomes or durability of repair following carotid angioplasty withstenting and carotid endarterectomy. Vasc Endovascular Surg 2008,42:321–328.
53. Foerch C, Misselwitz B, Humpich M, et al.: Sex disparity in theaccess of elderly patients to acute stroke care. Stroke 2007, 38:2123–2126.
54. Prehospital and hospital delays after stroke onset–United States,2005-2006. MMWR Morb Mortal Wkly Rep 2007, 56:474–478.
55. Caso V, Paciaroni M, Agnelli G, et al.: Gender differences inpatients with acute ischemic stroke. Womens Health (Lond Engl)2010, 6:51–57.
56. Gall SL, Donnan G, Dewey HM, et al.: Sex differences inpresentation, severity, and management of stroke in a population-based study. Neurology 2010, 74:975–981.
57. Knauft W, Chhabra J, McCullough LD: Emergency departmentarrival times, treatment, and functional recovery in women with acuteischemic stroke. J Womens Health (Larchmt) 2010 (in press).
242 Curr Atheroscler Rep (2010) 12:236–243

58. Gray LJ, Sprigg N, Bath PM, et al.: Sex differences in quality oflife in stroke survivors: data from the Tinzaparin in AcuteIschaemic Stroke Trial (TAIST). Stroke 2007, 38:2960–2964.
59. Lisabeth LD, Brown DL, Morgenstern LB: Barriers to intravenoustissue plasminogen activator for acute stroke therapy in women.Gend Med 2006, 3:270–278.
60. Kent DM, Price LL, Ringleb P, et al.: Sex-based differences inresponse to recombinant tissue plasminogen activator in acuteischemic stroke: a pooled analysis of randomized clinical trials.Stroke 2005, 36:62–65.
61. • Elkind MS, Prabhakaran S, Pittman J, et al.: Sex as a predictor ofoutcomes in patients treated with thrombolysis for acute stroke.Neurology 2007, 68:842–848. Men were approximately three
times as likely to have good functional outcomes after tissueplasminogen activator treatment, despite elevated mortality. Evenafter receiving thrombolytic treatment, women were found to haveworse functional outcomes after stroke than men.
62. Arnold M, Kappeler L, Nedeltchev K, et al.: Recanalization andoutcome after intra-arterial thrombolysis in middle cerebral arteryand internal carotid artery occlusion: does sex matter? Stroke2007, 38:1281–1285.
63. Shobha N, Sylaja PN, Kapral MK, et al.: Differences in strokeoutcome based on sex. Neurology 2010, 74:767–771.
64. Forster A, Gass A, Kern R, et al.: Gender differences in acute ischemicstroke: etiology, stroke patterns and response to thrombolysis. Stroke2009, 40:2428–2432.
Curr Atheroscler Rep (2010) 12:236–243 243