Embed Size (px)
Citation preview
Stroke
Judith Coombes
Princess Alexandra Hospital 2018
Objectives
• Overview of Stroke
• Focus on secondary prevention
• Ischemic atherosclerosis case
• AF case
Importance of Stroke
• In Australia 2nd greatest cause of death
after coronary artery disease
• 1/3 die, 1/3 permanent disability
• 4.5% of burden of disease (Aus)
• 1 in 6 will have had a stroke by the age of
85
Stroke in Sri Lanka
• 1 in 6 will develop a stroke
• Dr Ramawaka senior lecturer Kelaniya
• - fastest aging population
– Non communicable diseases eg diabetes
• 7 stroke units only 50 dedicated beds
• 2015 prevalence study showed 1 in 100
have a stroke
Case Study Mrs EC
• Mrs EC 69yr Female
• about to cook when she became (left
sided) weak, called 000 (14.56)
• National Institute of stroke scale (NIHSS-
9)
• Code stroke- lysis is Alteplase 0.9mg/kg
max 90mg 10% bolus then infusion
– Endovascular Clot retrieval –
– admit under stroke unit
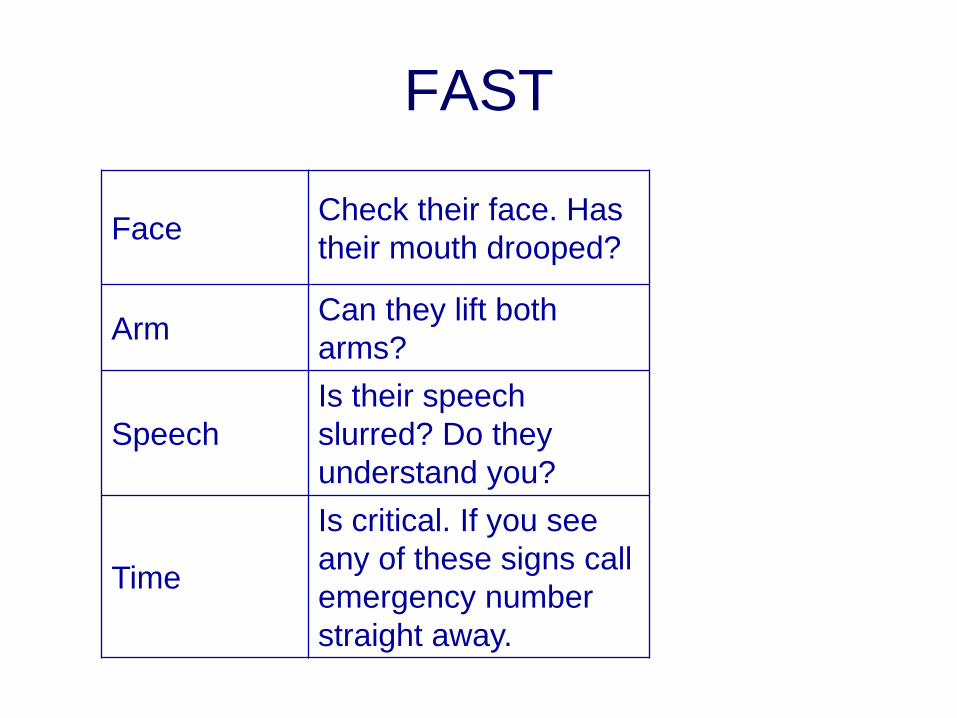
FAST
FaceCheck their face. Has
their mouth drooped?
ArmCan they lift both
arms?
Speech
Is their speech
slurred? Do they
understand you?
Time
Is critical. If you see
any of these signs call
emergency number
straight away.
Stroke Severity
• 0= no symptoms
• 1-4 Minor Stroke
• 5-15 Moderate Stroke
• 16-20 Moderate to severe stroke
• 21-42 Severe stroke
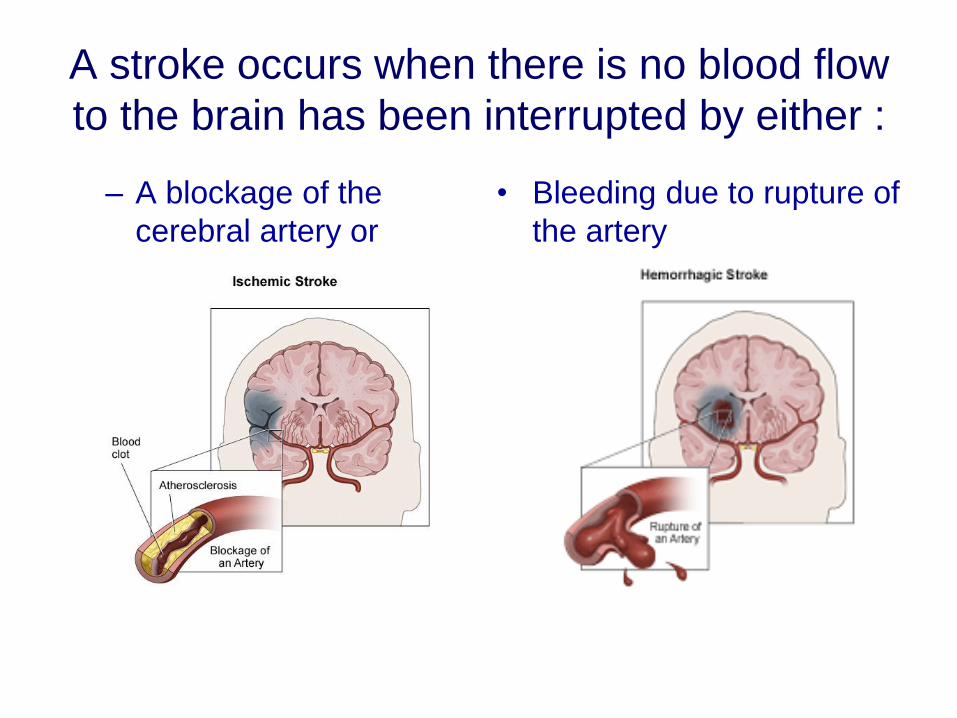
A stroke occurs when there is no blood flow
to the brain has been interrupted by either :
– A blockage of the
cerebral artery or
• Bleeding due to rupture of
the artery
Categorisation
• Ischemic Stroke
– Atherosclerosis
– Embolism
• Haemorrhagic Stroke
Haemorrhagic
• High blood pressure
• Cerebral aneurysms
– Weak or thin spot on blood vessel wall
• Arteriovenous malformations (AVM)
Ischemic
Two main causes
• Atherosclerosis • Embolic
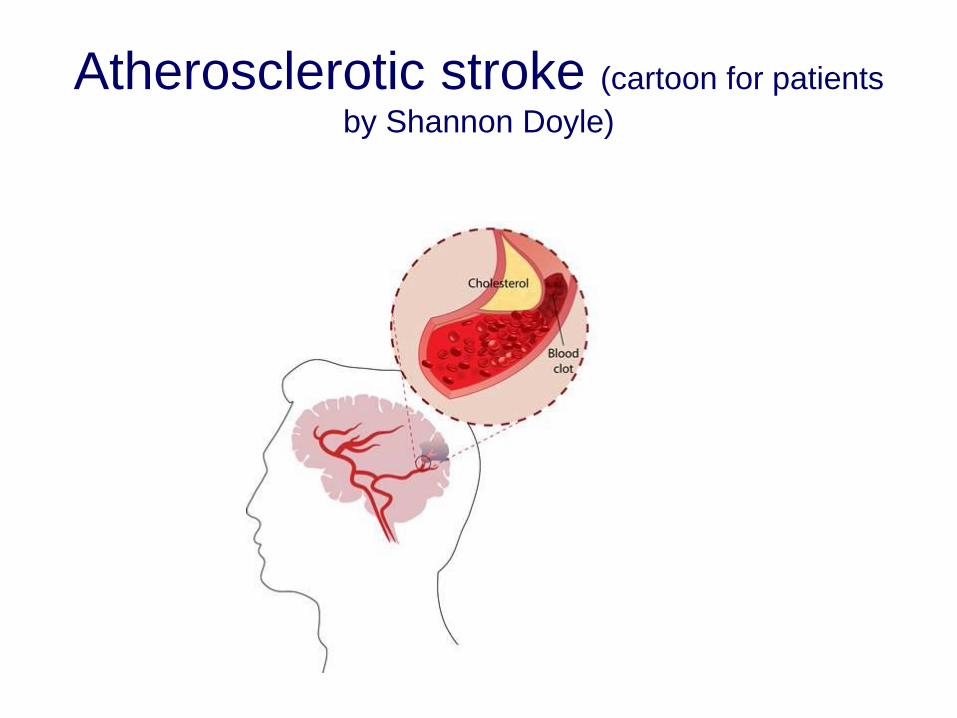
Atherosclerotic stroke (cartoon for patients
by Shannon Doyle)
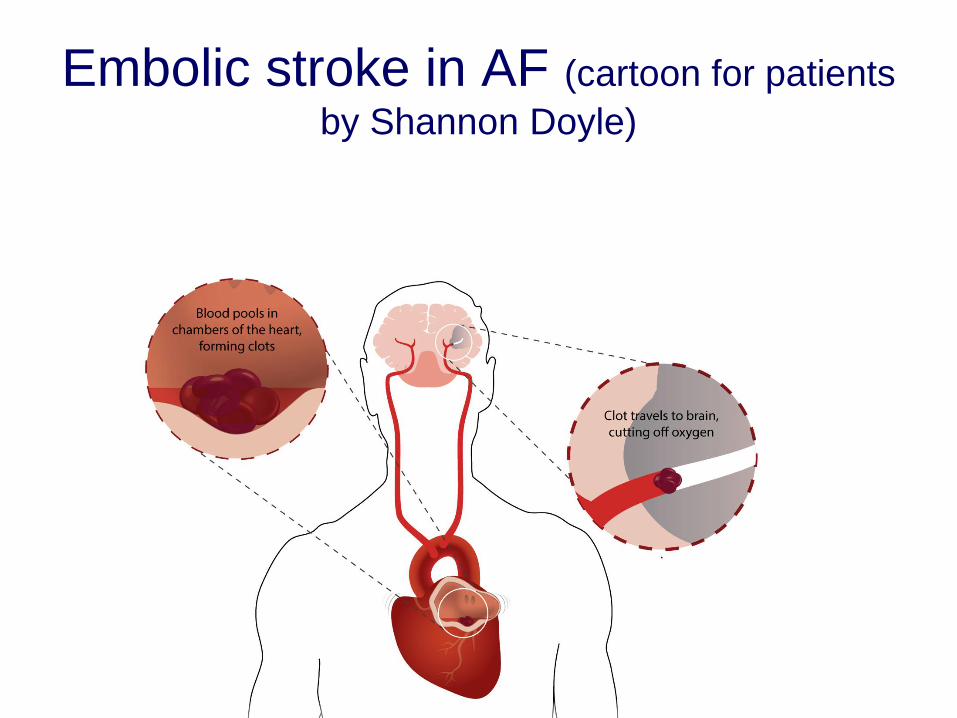
Embolic stroke in AF (cartoon for patients
by Shannon Doyle)
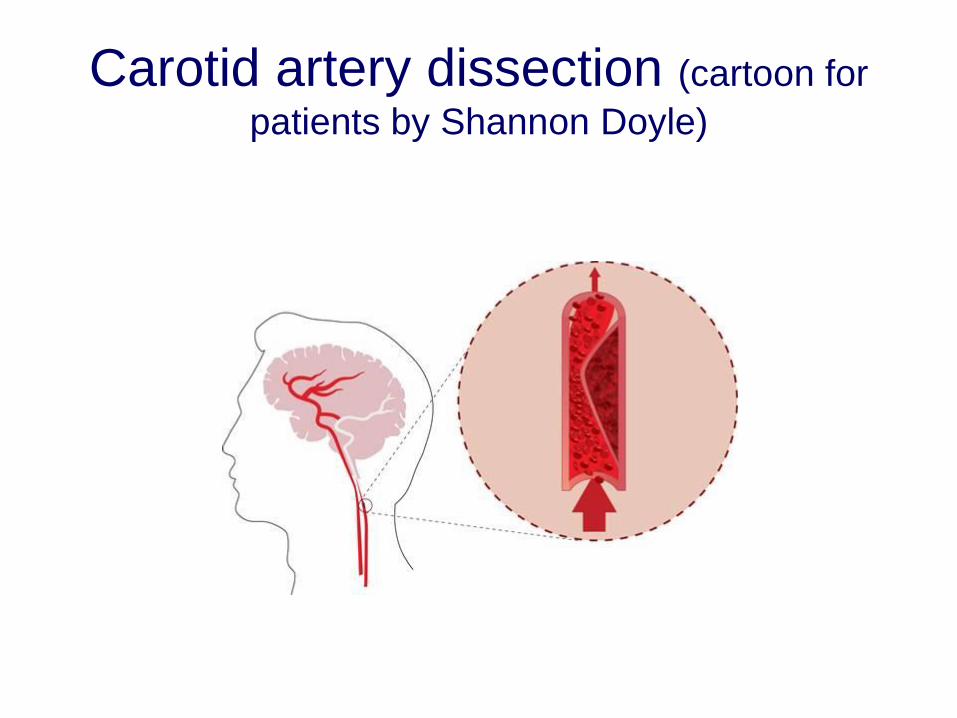
Carotid artery dissection (cartoon for
patients by Shannon Doyle)
Transient Ischemic Attack-TIA
Definition – Symptoms resolve within 24
hours
New Definition- Symptoms resolve and no
Stroke pathology detected on CT scan or
MRI
TIA and Stroke
• TIA- no permanent disability
• 1/3 strokes –no permanent disability
• Recurrence is about 12% in the first year
• So secondary prevention to reduce risk
Acute Medical treatment
• Lysis- TARGET:STROKE cuts door to needle
time improves stroke outcome (JAMA 22/4/14)
• Use tissue plasminogen activator tPA
• Clot retrieval with or without Lysis
• Aspirin 300mg- but take care if poor
swallow
Acute Medical treatment-
Endovascular Clot Retrieval
• Interventional Neuro-radiologists (INRs)
• Mr Clean study showed benefit
Clot Retrieval
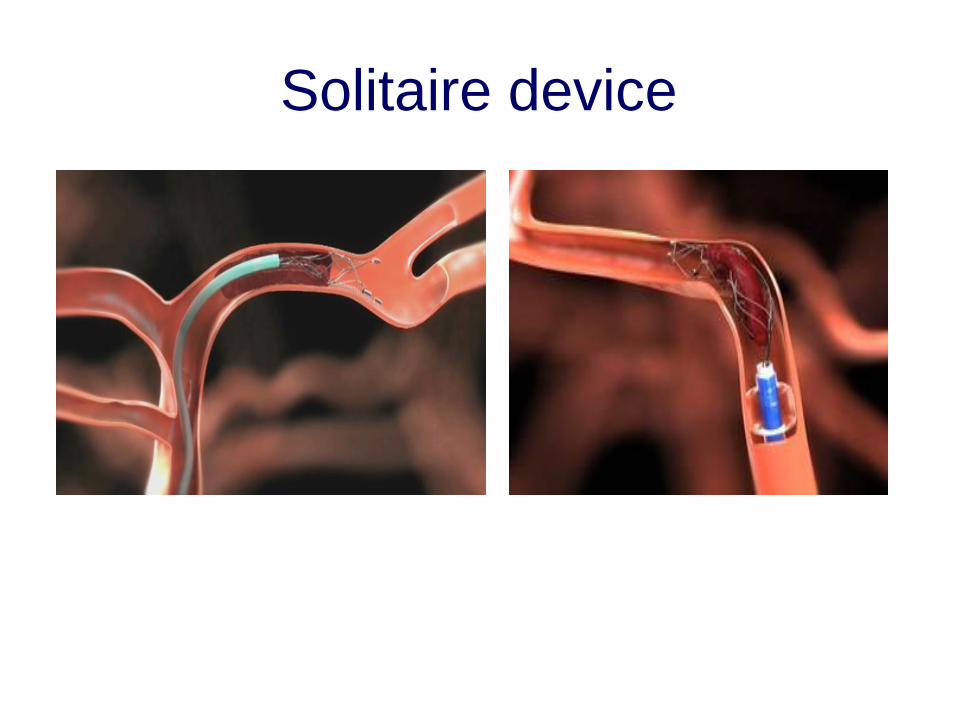
Solitaire device
Post ECR result
• NIHSS 0
• Still some stenosis needs Carotid
endarterectomy in a week
• Dual antiplatelets until then
Recurrence
• cumulative incidence 30-43%,
– highest occurrence in the first 12 months of 12% reducing to about 4 % per year
• After a transient Ischemic attack (TIA) 90 day incidence of stroke is 9.2-17.3%
After TIA first week is critical ABCD2 Age BP Clinical features(speech weakness) Duration less 10 min
Diabetes
>=4/7 high 0-3/7 low
Secondary prevention
RISK REDUCTION
Australian clinical guidelines for stroke management 2017
Non pharmacological
*Control of Diabetes
Smoking cessation
Weight loss
Exercise
Reduce alcohol
Carotid surgery if appropriate
Pharmacological
*Blood Pressure control
*Anti-thrombotics
*Cholesterol lowering
Guidelines
Australian clinical guidelines for stroke
management 2017
• BP-All >140/90 should have treatment
– ACE/ARB, Calcium Chanel Blocker, Thiazide
(not beta-blocker first line)
• High dose statin (Atorvastatin 80mg) if
atherosclerotic contribution and life
expectancy (?greater than 1 year)
Guidelines- antithrombotic
• Aspirin or Clopidogrel or Aspirin with
dipyridamole
Unless
Anticoagulated
• If AF anticoagulate
Mrs EC
• Anti platelet- is individualised
– Stenosis so discharged on Dual oral antiplatelet therapy(Aspirin and Clopidogrel)
– Plan a CEA (carotid endarterectomy) in 1 week then stop Aspirin after 3 weeks
• Antihypertensive
– Blood pressure 140/80 and cause embolic in this case no antihypertensive
• Lipid lowering
– Atorvastatin 80mg
To guide treatment decisions
Assess risk factors for bleeding with
aspirin including:
*increasing age
*any bleeding predisposition
*history of peptic ulcer
*uncontrolled hypertension
*severe renal or hepatic impairment
*concurrent use of NSAIDs or
anticoagulants
aspirin + dipyridamole SR
Reduces stroke risk over Aspirin alone, but
less well tolerated
Previous stroke or TIA relative risk reduction
of non-fatal stroke compared with Aspirin
alone without causing extra bleeding
ESPRIT Trial - 34% (A+D) vs 13% (Aspirin
alone) but many stopped treatment, mainly
because of headache
We do 1 A+D mane and 1 aspirin nocte for a
week the 1 A+D BD and stop aspirin
clopidogrel - a more suitable choice for
some patients
Similar efficacy to Aspirin + Dipyridamole SR in
preventing recurrent stroke
Comparable bleeding risk
Useful if intolerance to Aspirin + Dipyridamole SR OR
co-existing coronary heart disease
CAPRIE - v small benefit for Clopidogrel vs
aspirin(saves 1 more in 200 per year), similar overall
bleed risk.
Avoid aspirin + clopidogrel
• MATCH - Aspirin + Clopidogrel no more
effective than Clopidogrel alone to
prevent vascular events after ischaemic
stroke, TIA. Caused more life-
threatening bleeding.
• Benefit of Aspirin + Clopidogrel exceeds
bleed risk in acute coronary syndrome
or coronary stent
Adherence
• Like all chronic diseases adherence is
reported at 30-70%
• Educate the patient about
– Medications are to reduce risk of further
stroke
– This is lifelong therapy
– Report adverse events or stroke symptoms---
to clinic
Adverse Medication Events
• BP lowering- fainting and falls
• Statins- muscle weakness or pain
• Anti platelets- bleeding and Dipyridamole
causes headache
• Anti diabetes – cause hypoglycaemia
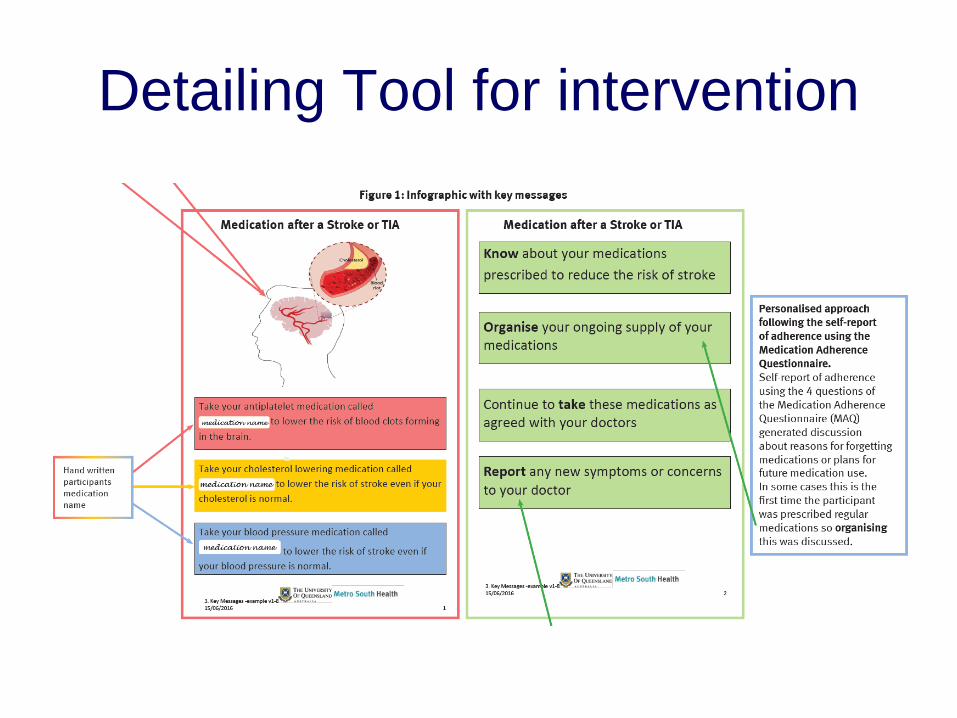
Detailing Tool for intervention
Changes is the last 3 years
• CODE Stroke
• Endovascular Clot Retrieval
• AF and DOACS
– Give a booklet
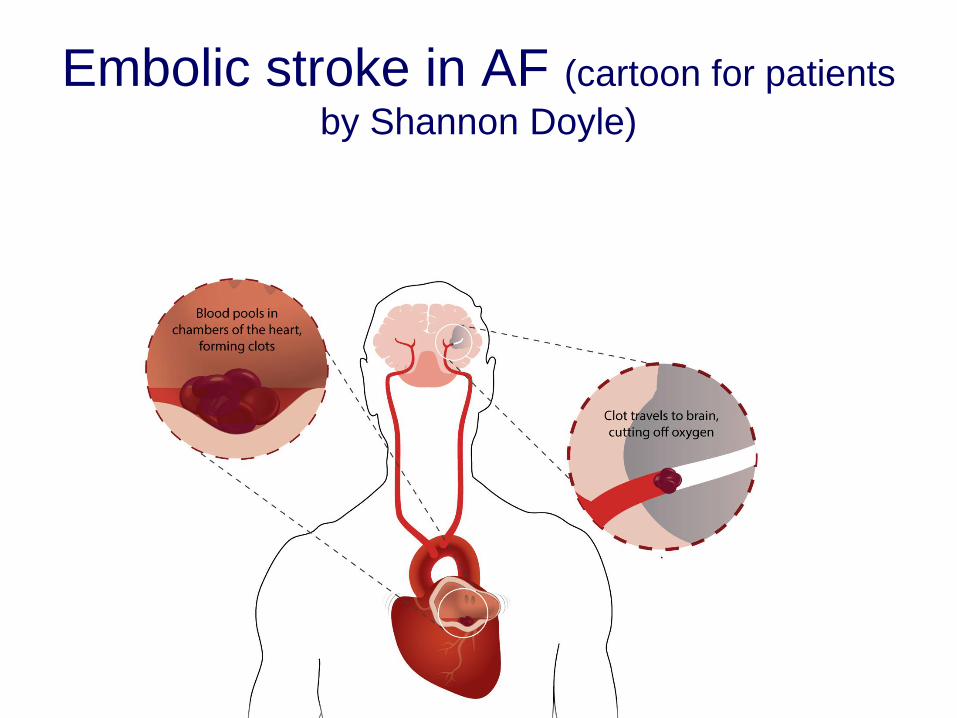
Embolic stroke in AF (cartoon for patients
by Shannon Doyle)
Mr AF 50yr male
• PC –embolic stroke
• PMH
– Hypertension
– High cholesterol
– Atrial fibrillation
Mr AF – Question 1What are Mr AFs risk factors for stroke?
• Hypertension
• Cholesterol risk of atherosclerosis
• Atrial fibrillation
BP
• Keep below 140 mmHg
• No benefits of further intensive lowering
Mr AF Question 2What is the most appropriate antithrombitic
therapy for stroke prevention?
• Prior to his stroke
• After his stroke
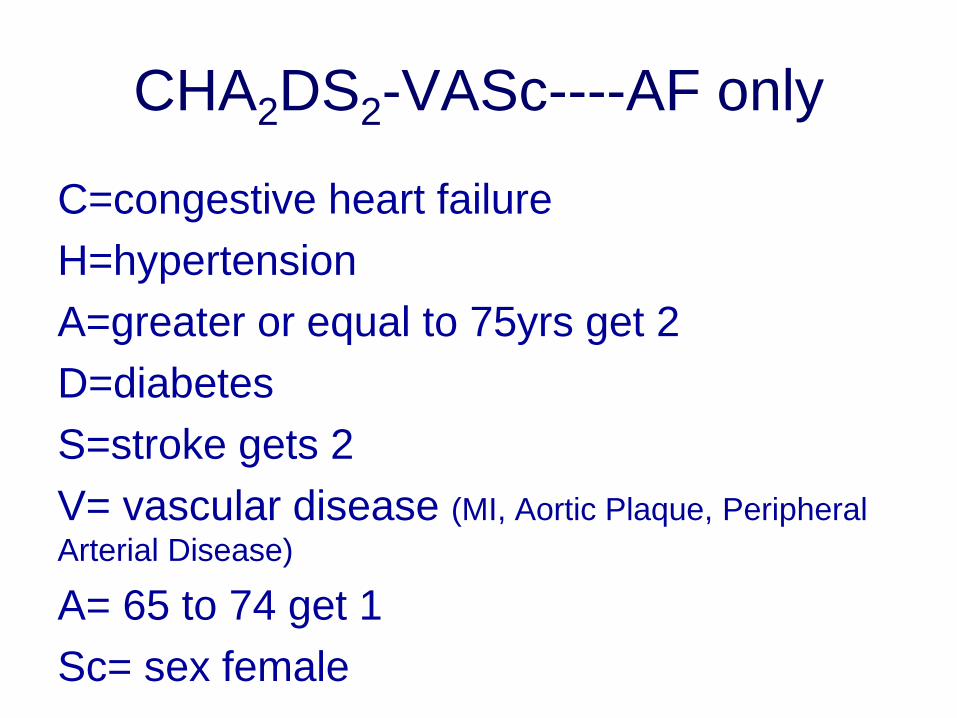
CHA2DS2-VASc----AF only
C=congestive heart failure
H=hypertension
A=greater or equal to 75yrs get 2
D=diabetes
S=stroke gets 2
V= vascular disease (MI, Aortic Plaque, Peripheral
Arterial Disease)
A= 65 to 74 get 1
Sc= sex female
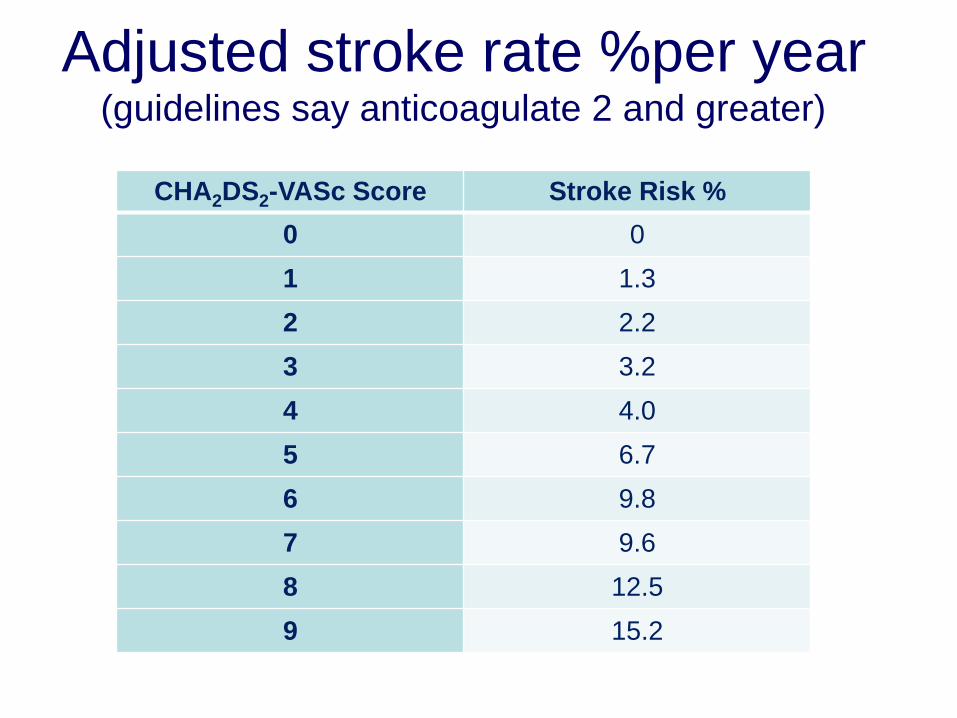
CHA2DS2-VASc Score Stroke Risk %
0 0
1 1.3
2 2.2
3 3.2
4 4.0
5 6.7
6 9.8
7 9.6
8 12.5
9 15.2
Adjusted stroke rate %per year (guidelines say anticoagulate 2 and greater)
National Heart Foundation
Australia
•The sexless CHA2DS2-VA score is recommended to assess stroke
risk, which standardises thresholds across men and women;
anticoagulation is not recommended for a score of 0, and is
recommended for a score of ≥ 2. If anticoagulation is indicated, non-
vitamin K oral anticoagulants are recommended in preference to
warfarin.
https://www.heartfoundation.org.au/for-
professionals/clinical-information
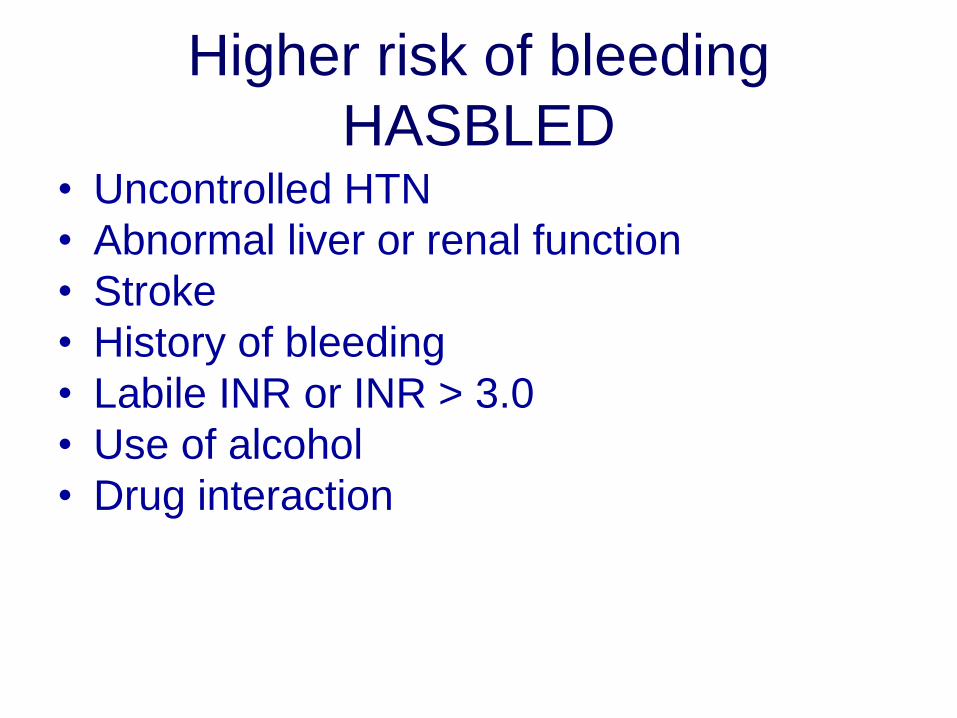
Higher risk of bleeding
HASBLED• Uncontrolled HTN
• Abnormal liver or renal function
• Stroke
• History of bleeding
• Labile INR or INR > 3.0
• Use of alcohol
• Drug interaction
Mr AF – Question 2What is the most appropriate antithrombitic
therapy for stroke prevention?
Warfarin
New/or Direct oral
anticoagulants • Dabigatran (thrombin inhibitor)
• Apixaban (Xa inhibitor)
• Rivaroxaban(Xa inhibitor)
Cholesterol lowering
• All patients with Ischemic stroke or TIA
• And possible atherosclerotic contribution
• Reasonable life expectancy
• Should have high potency statin
• Atorvastatin 80mg
Safety Strategies
• Rash
• Dizziness
• Muscle Weakness
• Bleeding or bruising
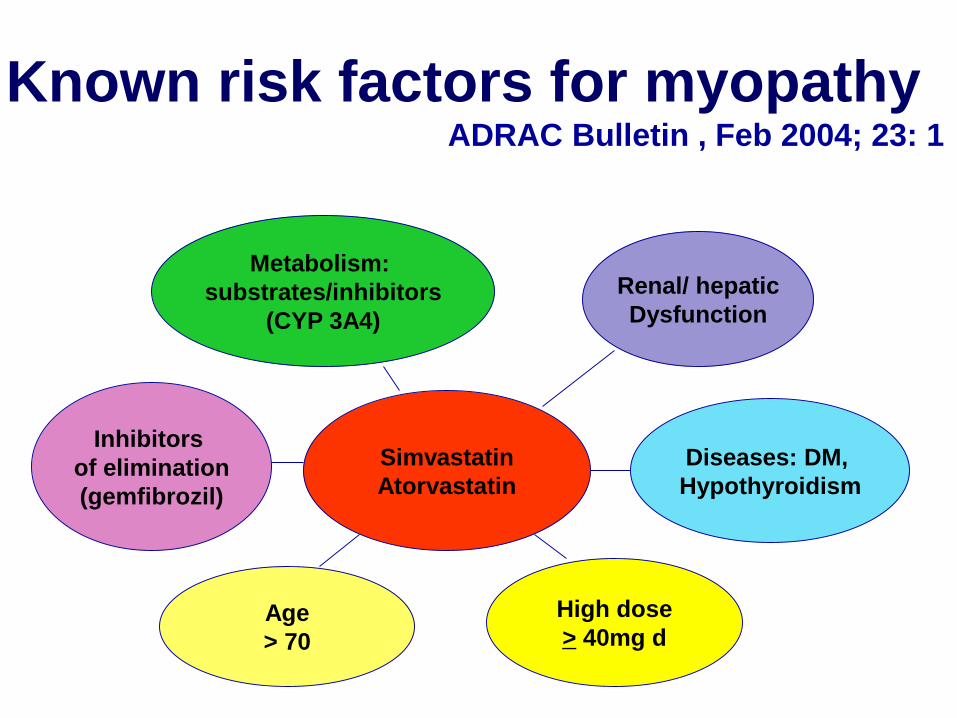
Simvastatin
Atorvastatin
Metabolism:
substrates/inhibitors
(CYP 3A4)
Age
> 70
Diseases: DM,
Hypothyroidism
High dose
> 40mg d
Renal/ hepatic
Dysfunction
Inhibitors
of elimination
(gemfibrozil)
Known risk factors for myopathyADRAC Bulletin , Feb 2004; 23: 1
Useful Reference
• Stroke
– The lancet.com
– Graeme J Hankey
– Published online September 13, 2016
• Australian stroke guidelines 2017
(https://informme.org.au/en/Guidelines/Clinic
al-Guidelines-for-Stroke-Management-2017)
Warfarin Counselling
• Video
• Groups of 3 with warfarin book
– Patient
– Counselling
– Feedback
Then change roles



















