Embed Size (px)
Citation preview

Stroke Education Series - 2010Stroke Education Series - 2010
Phaniraj Iyengar MDPhaniraj Iyengar MDDirectorDirector
Phaniraj Iyengar MDPhaniraj Iyengar MDDirectorDirector
Hypercoaguable states & StrokeHypercoaguable states & Stroke

DisclosureDisclosure
• I am on the speaker panel for Bristol Myers and Sanofi Aventis
• I am on the speaker panel for Bristol Myers and Sanofi Aventis

Discussion PointsDiscussion Points1. Introduction2. Hemostasis3. Thrombosis4. Neurologist workup philosophy5. Inherited hypercoaguable states6. Acquired hypercoaguable states 7. Case presentations (Two)8. Final summary
1. Introduction2. Hemostasis3. Thrombosis4. Neurologist workup philosophy5. Inherited hypercoaguable states6. Acquired hypercoaguable states 7. Case presentations (Two)8. Final summary

Hypercoaguable states & StrokeHypercoaguable states & Stroke• Coagulation disorders that predispose to
strokes remain POORLY DEFINED. • They may have been implicated in venous
strokes (Cerebral venous thrombosis) rather than arterial strokes.
• Known hematological abnormalities are estimated to account for about 4% of all strokes. This proportion may be higher for younger people.
• Coagulation disorders that predispose to strokes remain POORLY DEFINED.
• They may have been implicated in venous strokes (Cerebral venous thrombosis) rather than arterial strokes.
• Known hematological abnormalities are estimated to account for about 4% of all strokes. This proportion may be higher for younger people.

Hypercoaguability and StrokeHypercoaguability and Stroke
HemostasisHemostasis

IntroductionIntroduction
• The ability of blood to coagulate is ESSENTIAL to the survival of the species.
• In humans, when coagulation is TOO EFFICIENT, thrombosis becomes one of THE MOST COMMON CAUSES of morbidity and mortality in developed countries – specifically CAD & STROKE.
• The ability of blood to coagulate is ESSENTIAL to the survival of the species.
• In humans, when coagulation is TOO EFFICIENT, thrombosis becomes one of THE MOST COMMON CAUSES of morbidity and mortality in developed countries – specifically CAD & STROKE.

Hemostatic ProcessThe Three main Steps
Hemostatic ProcessThe Three main Steps
1. Primary hemostasis Local vasoconstriction
& platelet plug formation.
2. Coagulation cascade.
3. Fibrinolysis
1. Primary hemostasis Local vasoconstriction
& platelet plug formation.
2. Coagulation cascade.
3. Fibrinolysis

HemostasisHemostasis
A very complex process!!!A very complex process!!!

Rube Goldberg MachinePencil Sharpener
Rube Goldberg MachinePencil Sharpener
Open window (A) and fly kite (B). String (C) lifts small door (D) allowing moths (E) to escape and eat red flannel shirt (F). As weight of shirt becomes less, shoe (G) steps on switch (H) which heats electric iron (I) and burns hole in pants (J). Smoke (K) enters hole in tree (L), smoking out opossum (M) which jumps into basket (N), pulling rope (O) and lifting cage (P), allowing woodpecker (Q) to chew wood from pencil (R), exposing lead. Emergency knife (S) is always handy in case opossum or the woodpecker gets sick and can't work.

Platelet Activation & AggregationFirst Step
Platelet Activation & AggregationFirst Step
Exposed endothelial surfaceExposed endothelial surface
Platelets exposed to collagenPlatelets exposed to collagen
Platelets are activatedPlatelets are activated
Release contents of cytoplasmic granulesRelease contents of cytoplasmic granules
Adenosine Diphosphate (ADP)Adenosine Diphosphate (ADP) Thromboxane (TxA2)Thromboxane (TxA2)Accelerates Platelet activationPlatelet aggregation
Accelerates Platelet activationPlatelet aggregation
VasoconstrictionIncreases ADP releasefrom Platelets
VasoconstrictionIncreases ADP releasefrom Platelets

Hemostatic ProcessCoagulation Cascade
Hemostatic ProcessCoagulation Cascade
To stabilize and reinforce the weak platelet plug
Fibrinogen → fibrin Three main steps:
1. Formation of prothrombin activator
2. Conversion of prothrombin into thrombin
3. Conversion of fibrinogen to fibrin
To stabilize and reinforce the weak platelet plug
Fibrinogen → fibrin Three main steps:
1. Formation of prothrombin activator
2. Conversion of prothrombin into thrombin
3. Conversion of fibrinogen to fibrin

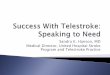
Coagulation Cascade
Coagulation Cascade
TF =tissue factorPK = prekallikreinHK=high molecular kininogena = activated
Roberts HR, et al. Current Concepts for Hemostasis. Anesthesiology 2004;100:3. 722-30.

“Contact Activation” Tissue Factor + VIITissue Factor + VII
XIIIXIIIaa
XIIIXIII
Thrombin
XL-XL-Fibrin
PolymerFibrinogen Fibrin
Monomer
IX
XIXI
XIXIaa
IXa
XaVVaa
XIIXIIaaProthrombin
TF-VIITF-VIIaa
(Prothrombinase)
PLPL
PL, Ca2+
(Tenase)
VIIIVIIIaa
PL, Ca2+
XX
Intrinsic Pathway
PrekallikreinHMW
Kininogen
Extrinsic Pathway
Common Pathway
“TF Pathway”
Anticoagulation proteins: Protein C, Protein S, Antithrombin III, TFPI
Ca2+
Coagulation PathwaysCoagulation Pathways

Coagulation is a MULTIFACTORIAL PATHWAY of "accelerators".Coagulation is TIGHTLY REGULATED and only a SMALL quantity of each coagulation enzyme is converted to its active form. Regulation is important - there is enough clotting potential in 1 mL of blood to CLOT ALL THE FIBRINOGEN IN THE BODY in 10 to 15 seconds!
CoagulationSome facts to consider…
CoagulationSome facts to consider…

Hypercoaguability and StrokeHypercoaguability and Stroke
ThrombosisThrombosis

ThrombosisAn Eye OpenerThrombosisAn Eye Opener
Thrombosis Is
Clotting In
the Wrong Place
Thrombosis Is
Clotting In
the Wrong Place

IntroductionIntroduction• Thrombosis can be divided anatomically into
VENOUS and ARTERIAL thrombosis.• Pathophysiology of these two types of clotting is
quite different.• Clotting in the low flow venous system is generally
associated with DEPOSITION OF FIBRIN, whereas in the arterial system, thrombosis is associated with PLATELET REACTIVITY AND VASCULAR WALL DAMAGE.
• Thrombosis can be divided anatomically into VENOUS and ARTERIAL thrombosis.
• Pathophysiology of these two types of clotting is quite different.
• Clotting in the low flow venous system is generally associated with DEPOSITION OF FIBRIN, whereas in the arterial system, thrombosis is associated with PLATELET REACTIVITY AND VASCULAR WALL DAMAGE.

Arterial ThrombosisPathophysiology
Arterial ThrombosisPathophysiology
Arterial thrombosis is the result of an Atheromatous plaque rupture that causes platelet activation and aggregation resulting in an obstructive lesion that subsequently leads to tissue damage.
Arterial thrombosis is the result of an Atheromatous plaque rupture that causes platelet activation and aggregation resulting in an obstructive lesion that subsequently leads to tissue damage.

HypercoaguabilityHypercoaguability
Factors that ACCELERATE the hemostatic mechanism or INHIBIT mechanisms that counteract hemostasis CONTRIBUTE to an INCREASED state of THROMBOGENICITY or HYPERCOAGUABILITY, and thereby play an etiological role in strokes.
Factors that ACCELERATE the hemostatic mechanism or INHIBIT mechanisms that counteract hemostasis CONTRIBUTE to an INCREASED state of THROMBOGENICITY or HYPERCOAGUABILITY, and thereby play an etiological role in strokes.

Hypercoaguable Workup in StrokeIs Challenging because of
Hypercoaguable Workup in StrokeIs Challenging because of
The relative LOW PREVALENCE of these disorders in stroke patients
Their UNCERTAIN SIGNIFICANCE Their POTENTIAL INTERACTION with traditional
stroke risk factors The HIGH COST of testing The LACK OF diagnostic gold standards The DIFFICULTY WITH INTERPRETATION of
some tests in the setting of acute thrombosis.*
The relative LOW PREVALENCE of these disorders in stroke patients
Their UNCERTAIN SIGNIFICANCE Their POTENTIAL INTERACTION with traditional
stroke risk factors The HIGH COST of testing The LACK OF diagnostic gold standards The DIFFICULTY WITH INTERPRETATION of
some tests in the setting of acute thrombosis.*
Brigden ML. The hypercoagulable state: who, how, and when to test and treat. Postgrad Med.1997; 101: 249–267.
Bushnell CD, Goldstein LB. Diagnostic testing for coagulopathies in patients with ischemic stroke. Stroke. 2000; 31: 3067–3078.
Bushnell CD, Siddiqi Z, Morgenlander JC, Goldstein LB. Use of specialized coagulation testing in the evaluation of patients with acute ischemic stroke. Neurology. 2001; 56: 624–627.
Brigden ML. The hypercoagulable state: who, how, and when to test and treat. Postgrad Med.1997; 101: 249–267.
Bushnell CD, Goldstein LB. Diagnostic testing for coagulopathies in patients with ischemic stroke. Stroke. 2000; 31: 3067–3078.
Bushnell CD, Siddiqi Z, Morgenlander JC, Goldstein LB. Use of specialized coagulation testing in the evaluation of patients with acute ischemic stroke. Neurology. 2001; 56: 624–627.

Before ordering please………Before ordering please……… Attempt to connect the dots by asking
the right questions especially in the context of History Presentation Imaging
Attempt to connect the dots by asking the right questions especially in the context of History Presentation Imaging
Because these tests are expensive!!!Because these tests are expensive!!!

Cost of Hypercoaguabilty workupCost of Hypercoaguabilty workup
Test Approximate Cost*
Natural anticoagulants
(antithrombin, protein C, protein S):
$450-750
Genetic tests
(factor V Leiden, prothrombin G20210A):
$600
Antiphospholipid antibodies: $1000-1500
Other (factor VIII, homocysteine): $200
TOTAL PANEL COST $2250-3050
* Duke Coagulation Laboratory

Hypercoaguability and StrokeHypercoaguability and Stroke
Neurologists Hypercoaguability Workup
philosophy
Neurologists Hypercoaguability Workup
philosophy

Workup of a suspected Hypercoaguable state causing Stroke
Workup of a suspected Hypercoaguable state causing Stroke Fifty-nine (75%) surveys were completed. Specialized coagulation tests were reported
to INFREQUENTLY influence stroke patient management (<25% of the time or NEVER for 95% of respondents).
Factors reported to INCREASE test-ordering included young patient age (76%), history of thrombosis (46%), history of miscarriages (36%), and HAVING FEW traditional stroke risk factors (35%).
Fifty-nine (75%) surveys were completed. Specialized coagulation tests were reported
to INFREQUENTLY influence stroke patient management (<25% of the time or NEVER for 95% of respondents).
Factors reported to INCREASE test-ordering included young patient age (76%), history of thrombosis (46%), history of miscarriages (36%), and HAVING FEW traditional stroke risk factors (35%).

MOST (88%) indicated they would order specialized coagulation tests for a hypothetical young patient with NO known stroke risk factors.
In contrast, ONLY A FEW (14%) would obtain the tests for a patient having traditional stroke risk factors, and
NONE would order the tests for a stroke patient with Atrial fibrillation.
MOST (88%) indicated they would order specialized coagulation tests for a hypothetical young patient with NO known stroke risk factors.
In contrast, ONLY A FEW (14%) would obtain the tests for a patient having traditional stroke risk factors, and
NONE would order the tests for a stroke patient with Atrial fibrillation.
Workup of a suspected Hypercoaguable state causing Stroke
Workup of a suspected Hypercoaguable state causing Stroke

Laboratory EvaluationLaboratory EvaluationRISK FACTOR LABORATORY ASSAY
Antithrombin Deficiency AT activity
Protein C Deficiency Protein C Deficiency PC activity (clotting or chromogenic)
Protein S Deficiency Protein S Free Antigen (ELISA, LIA)
APC Resistance / Factor V Leiden Mutation
APC Resistance (aPTT); FV Leiden genetic test if abnormal
Prothrombin Mutation G20210A Genetic Test
Hypherhomocysteinemia EIA, HPLC
Lupus Anticoagulant DRVVT Clotting Assay
Anticardiolipin Antibody, IgG / IgM
aCL IgG / IgM Antigen ELISA

Hypercoaguability and StrokeHypercoaguability and Stroke
Evaluation for Causes of a Hypercoaguable State is
Complicated
Evaluation for Causes of a Hypercoaguable State is
Complicated
What the Mind Does Not Know, The Eye Does Not See
What the Mind Does Not Know, The Eye Does Not See

Factors leading to ThrombosisFactors leading to ThrombosisInherited Risk Factors
APC resistance-Factor V Leiden
Anti-Thrombin deficiency Protein C deficiency Protein S deficiency Prothrombin Mutation Fibrinogen Mutations Platelet protein
polymorphisms Sickle cell disease
Inherited Risk Factors APC resistance-Factor V
Leiden Anti-Thrombin deficiency Protein C deficiency Protein S deficiency Prothrombin Mutation Fibrinogen Mutations Platelet protein
polymorphisms Sickle cell disease
Acquired Risk Factors Age Malignancy Immobilization Trauma, Post-op Pregnancy Estrogen use Antiphospholipid Antibodies Long distance flights Hematologic Diseases
TTP
Acquired Risk Factors Age Malignancy Immobilization Trauma, Post-op Pregnancy Estrogen use Antiphospholipid Antibodies Long distance flights Hematologic Diseases
TTP
Inherited or Acquired Risk FactorsHyperhomocystenemiaElevated levels of Factor VIII, IX,XI

Hypercoaguability and StrokeHypercoaguability and Stroke
Inherited Hypercoaguable
States
Inherited Hypercoaguable
States

Inherited Hypercoaguable StatesInherited Hypercoaguable States
MUTATIONS
RARE Antithrombin III
deficiency. Protein C deficiency. Protein S deficiency
MUTATIONS
RARE Antithrombin III
deficiency. Protein C deficiency. Protein S deficiency
POLYMORPHISMS
COMMON Factor V Leiden. Prothrombin gene
polymorphism. Thermolabile MTHFR
variant.
POLYMORPHISMS
COMMON Factor V Leiden. Prothrombin gene
polymorphism. Thermolabile MTHFR
variant.

Inherited Hypercoaguable StatesInherited Hypercoaguable StatesDefect Incidence % of
Hypercoaguable States
Factor V Leiden 2 – 8 % 40-60%
Prothtombin Gene Mutation 1-2 % ?10%
Protein C deficiency 1: 200 5-10%
Protein S deficiency 1: 5,000 5-10%
Antithrombin III deficiency 1: 2- 5000 1-3%
Dysfibrinogenemia rare 1%

Inherited Hypercoaguable StatesPolymorphisms of coagulation proteins
Inherited Hypercoaguable StatesPolymorphisms of coagulation proteins
• The MOST common cause of venous thrombosis is Activated Protein C resistance (APC Resistance) which is MOST OFTEN associated with a single mutation causing substitution of arginine by glutamine at residue 506 of Factor V gene (Factor V Leiden).
• The MOST common cause of venous thrombosis is Activated Protein C resistance (APC Resistance) which is MOST OFTEN associated with a single mutation causing substitution of arginine by glutamine at residue 506 of Factor V gene (Factor V Leiden).

Inherited Hypercoaguable States
Factor V Leiden
Inherited Hypercoaguable States
Factor V Leiden
Most common inherited cause of thrombosis in Caucasians
3-8% Caucasians carry the mutation and 0.1% are homozygotes
Homozygotes have 80 fold increased risk of thrombosis
Most common inherited cause of thrombosis in Caucasians
3-8% Caucasians carry the mutation and 0.1% are homozygotes
Homozygotes have 80 fold increased risk of thrombosis

Inherited Hypercoaguable States Factor V Leiden
Inherited Hypercoaguable States Factor V Leiden
Occurs in 5-7% of the population Occurs in 20% of patients with DVT. Occurs in 60% of patients with recurrent
DVT’s. Incidence of Factor V Leiden with stroke is
UNKNOWN.
Occurs in 5-7% of the population Occurs in 20% of patients with DVT. Occurs in 60% of patients with recurrent
DVT’s. Incidence of Factor V Leiden with stroke is
UNKNOWN.

Inherited Hypercoaguable States Factor V Leiden
Inherited Hypercoaguable States Factor V Leiden
Factor V Leiden is suspected to be associated with paradoxical emboli or with venous sinus thrombosis.
At this time, the data available DO NOT suggest any role between factor V Leiden and arterial thrombosis (stroke, heart attack).
Factor V Leiden is suspected to be associated with paradoxical emboli or with venous sinus thrombosis.
At this time, the data available DO NOT suggest any role between factor V Leiden and arterial thrombosis (stroke, heart attack).

Treatment Warfarin x 6 months or until thrombosis
free for 2 months LMWH x 2 wks after Warfarin then retested Long term anticoagulation if persist or
recurrent thrombotic event
Treatment Warfarin x 6 months or until thrombosis
free for 2 months LMWH x 2 wks after Warfarin then retested Long term anticoagulation if persist or
recurrent thrombotic event
Inherited Hypercoaguable States Factor V Leiden
Inherited Hypercoaguable States Factor V Leiden

Inherited Hypercoaguable States
Antithrombin deficiency
Inherited Hypercoaguable States
Antithrombin deficiency
1965 - First inherited trait associated with thrombophilia.
Although called anti-thrombin, it actually serves to inhibit virtually ALL of the coagulation enzymes to at least some extent.
1965 - First inherited trait associated with thrombophilia.
Although called anti-thrombin, it actually serves to inhibit virtually ALL of the coagulation enzymes to at least some extent.

• Although isolated reports exist of arterial disease in patients with heterozygous antithrombin deficiency, there is NO clear evidence of increased arterial disease in antithrombin deficiency.
• Although isolated reports exist of arterial disease in patients with heterozygous antithrombin deficiency, there is NO clear evidence of increased arterial disease in antithrombin deficiency.
Inherited Hypercoaguable States Antithrombin deficiency
Inherited Hypercoaguable States Antithrombin deficiency

Inherited Hypercoaguable States
Prothrombin Gene Mutation
Inherited Hypercoaguable States
Prothrombin Gene Mutation
Genetic defect at nucleotide position 20210A in prothrombin gene results in high prothrombin levels which causes
increased thrombin generation
2-3% in Caucasians, 4-5% in Mediterranean Less severe clinical manifestation
Genetic defect at nucleotide position 20210A in prothrombin gene results in high prothrombin levels which causes
increased thrombin generation
2-3% in Caucasians, 4-5% in Mediterranean Less severe clinical manifestation

Inherited Hypercoaguable States Prothrombin Gene Mutation
Inherited Hypercoaguable States Prothrombin Gene Mutation
At this time, there is CONTRADICTING evidence regarding the role of the Prothrombin Gene mutation and arterial thrombosis (stroke, heart attack).
At this time, there is CONTRADICTING evidence regarding the role of the Prothrombin Gene mutation and arterial thrombosis (stroke, heart attack).

Inherited Hypercoaguable States Prothrombin Gene Mutation and Stroke
Inherited Hypercoaguable States Prothrombin Gene Mutation and Stroke
Based on these data, for persons with the prothrombin gene mutation, the MOST IMPORTANT preventive steps for the purposes of arterial disease are controlling other risk factors including: Smoking, Hypertension, Hyperlipidemia, Obesity and a sedentary lifestyle (limited activity).
Based on these data, for persons with the prothrombin gene mutation, the MOST IMPORTANT preventive steps for the purposes of arterial disease are controlling other risk factors including: Smoking, Hypertension, Hyperlipidemia, Obesity and a sedentary lifestyle (limited activity).

Inherited Hypercoaguable States Protein C
Inherited Hypercoaguable States Protein C
Vitamin K dependent plasma glycoprotein Functions by inactivating factors Va and
VIIIa Protein C activity is enhanced by Protein S Autosomal dominant inheritance
Vitamin K dependent plasma glycoprotein Functions by inactivating factors Va and
VIIIa Protein C activity is enhanced by Protein S Autosomal dominant inheritance

Prevalence in normal population ~0.2-0.4% Present in ~3-4% of patients with venous
thromboembolism. Homozygosity is associated with neonatal
purpura fulminans. 50% of patients with protein C deficiency
WILL have a thrombosis by age 36 years.
Prevalence in normal population ~0.2-0.4% Present in ~3-4% of patients with venous
thromboembolism. Homozygosity is associated with neonatal
purpura fulminans. 50% of patients with protein C deficiency
WILL have a thrombosis by age 36 years.
Inherited Hypercoaguable States Protein C deficiency
Inherited Hypercoaguable States Protein C deficiency

• At this time, the data available DO NOT suggest any role between protein C deficiency and arterial thrombosis (stroke, heart attack).
• At this time, the data available DO NOT suggest any role between protein C deficiency and arterial thrombosis (stroke, heart attack).
Inherited Hypercoaguable States Protein C deficiency
Inherited Hypercoaguable States Protein C deficiency

Inherited Hypercoaguable States Protein S
Inherited Hypercoaguable States Protein S
Vitamin K dependent anticoagulant Cofactor to protein C and enhances its
activity against factors Va and VIIIa.
Vitamin K dependent anticoagulant Cofactor to protein C and enhances its
activity against factors Va and VIIIa.

Prevalence in the normal population ~0.003% Present in ~2-3% of patients with venous
thromboembolism. Homozygosity is associated with neonatal
purpura fulminans. 50% of patients with protein S deficiency
WILL have a thrombosis by age 36 years.
Prevalence in the normal population ~0.003% Present in ~2-3% of patients with venous
thromboembolism. Homozygosity is associated with neonatal
purpura fulminans. 50% of patients with protein S deficiency
WILL have a thrombosis by age 36 years.
Inherited Hypercoaguable States
Protein S Deficiency
Inherited Hypercoaguable States
Protein S Deficiency

A prospective study did find free Protein S deficiency in 23% of young patients with Stroke of Uncertain Cause, but this finding could be associated with higher levels of C4b (an acute phase reactant that decreases free Protein S Levels).
A prospective study did find free Protein S deficiency in 23% of young patients with Stroke of Uncertain Cause, but this finding could be associated with higher levels of C4b (an acute phase reactant that decreases free Protein S Levels).
Inherited Hypercoaguable States
Protein S Deficiency and Stroke
Inherited Hypercoaguable States
Protein S Deficiency and Stroke

At this time, the data available DO NOT suggest any role between protein S deficiency and arterial thrombosis (stroke, heart attack).
At this time, the data available DO NOT suggest any role between protein S deficiency and arterial thrombosis (stroke, heart attack).
Inherited Hypercoaguable States Protein S Deficiency and Stroke
Inherited Hypercoaguable States Protein S Deficiency and Stroke

Elevated Fibrinogen levels are a common and consistent finding in patients with Stroke
Serum fibrinogen levels are variable and can increase in response to infectious or inflammatory conditions as part of the acute phase response.
Polymorphisms within the Fibrinogen gene have been associated with Stroke.
Elevated Fibrinogen levels are a common and consistent finding in patients with Stroke
Serum fibrinogen levels are variable and can increase in response to infectious or inflammatory conditions as part of the acute phase response.
Polymorphisms within the Fibrinogen gene have been associated with Stroke.
Inherited Hypercoaguable States
Fibrinogen
Inherited Hypercoaguable States
Fibrinogen

Results from the Austrian Stroke Study showed an association between a polymorphism in the beta chain of fibrinogen at position 148 and Carotid atherosclerosis.
Results from a Japanese study showed an association between a polymorphism at position 455 with cerebrovascular disease.
Results from the Austrian Stroke Study showed an association between a polymorphism in the beta chain of fibrinogen at position 148 and Carotid atherosclerosis.
Results from a Japanese study showed an association between a polymorphism at position 455 with cerebrovascular disease.
Inherited Hypercoaguable States
Fibrinogen Polymorphisms and Stroke
Inherited Hypercoaguable States
Fibrinogen Polymorphisms and Stroke

Over time, more polymorphisms are likely to be discovered in the Fibrinogen gene that are related to stroke.
Over time, more polymorphisms are likely to be discovered in the Fibrinogen gene that are related to stroke.
Inherited Hypercoaguable States
Fibrinogen Polymorphisms and Stroke
Inherited Hypercoaguable States
Fibrinogen Polymorphisms and Stroke

A common point mutation in glycoprotein IIIa, termed PLA2, leads to a substitution of proline for leucine at position 33.
PLA2 has been suggested as a risk factor for CAD1.
Although potentially associated with CAD, several studies have suggested that this polymorphism is UNLIKELY to be associated with Stroke2.
A common point mutation in glycoprotein IIIa, termed PLA2, leads to a substitution of proline for leucine at position 33.
PLA2 has been suggested as a risk factor for CAD1.
Although potentially associated with CAD, several studies have suggested that this polymorphism is UNLIKELY to be associated with Stroke2.
Inherited Hypercoaguable States Polymorphisms of Platelet Proteins & CAD Inherited Hypercoaguable States
Polymorphisms of Platelet Proteins & CAD
1Wciss EJ et al. N Engl J Med 1996;334:1090-10942Carlsson LE at al. Stroke 1997;28:1392-1395
1Wciss EJ et al. N Engl J Med 1996;334:1090-10942Carlsson LE at al. Stroke 1997;28:1392-1395

The Glycoprotein Ib/IX/V complex is a platelet protein responsible for platelet adhesion using vWF as the ligand.
A polymorphism in the region of the glycoprotein Lb gene responsible for keeping the ligand binding region distal to the platelet surface leads to a variable number (1,2,3,4) of tandem repeats.
There appears to be an association of repeat number genotype with Cerebrovascular disease1.
The Glycoprotein Ib/IX/V complex is a platelet protein responsible for platelet adhesion using vWF as the ligand.
A polymorphism in the region of the glycoprotein Lb gene responsible for keeping the ligand binding region distal to the platelet surface leads to a variable number (1,2,3,4) of tandem repeats.
There appears to be an association of repeat number genotype with Cerebrovascular disease1.
Inherited Hypercoaguable States Platelet Protein Polymorphisms & Stroke Inherited Hypercoaguable States Platelet Protein Polymorphisms & Stroke
Gonzalez-ConejeroR et al. Blood 1998;92:2771-2776Gonzalez-ConejeroR et al. Blood 1998;92:2771-2776

Inherited Hypercoaguable States
Hyperhomocysteinemia
Inherited Hypercoaguable States
Hyperhomocysteinemia Hyperhomocystenemia is associated with a
Vasculopathy. Unlike most other hypercoaguable states, it
causes more arterial strokes than venous strokes.
Elevated levels of Homocysteine and related disulfitide compounds are clear risk factors for Stroke
Hyperhomocystenemia is associated with a Vasculopathy.
Unlike most other hypercoaguable states, it causes more arterial strokes than venous strokes.
Elevated levels of Homocysteine and related disulfitide compounds are clear risk factors for Stroke

Homocysteine
Mutations,heterozygotic
1-2%Nutrition30-40%
Mutations,homozygotic
<<1%
Polymorphisms30-40%
Renalinsufficiency
Endothelialdysfunction
Venousthrombosis
CVD
PVD
CAD
Oxidativestress
Inherited Hypercoaguable States Hyperhomocysteinemia
Inherited Hypercoaguable States Hyperhomocysteinemia

Caused by two primary enzyme defects
1. Cystathionine Beta-Synthase (CBS)
2. Methylene-Tetra-Hydro-Folate Reductase (MTHFR),
Caused by two primary enzyme defects
1. Cystathionine Beta-Synthase (CBS)
2. Methylene-Tetra-Hydro-Folate Reductase (MTHFR),
Inherited Hypercoaguable States
Homocysteinemia
Inherited Hypercoaguable States
Homocysteinemia

1. Ocular manifestations – ectopia lentis
1. Ocular manifestations – ectopia lentis
Inherited HomocysteinemiaClinical Manifestations
Inherited HomocysteinemiaClinical Manifestations

2. Marfanoid appearance combined with CNS manifestations, like mental retardation
Inherited HomocysteinemiaClinical Manifestations
Inherited HomocysteinemiaClinical Manifestations

3. Musculo-skeletal manifestations - osteoporosis
3. Musculo-skeletal manifestations - osteoporosis
Inherited HomocysteinemiaClinical Manifestations
Inherited HomocysteinemiaClinical Manifestations

4. Vascular manifestations – vascular occlusions, thromboembolism
Inherited HomocysteinemiaClinical Manifestations
Inherited HomocysteinemiaClinical Manifestations

Most common genetic cause of severe homocysteinemia.
Classic homocystinuria is homozygous deficiency of CBS.
Inherited as autosomal recessive trait. Occurs in 1 in 100,000 live births.
Most common genetic cause of severe homocysteinemia.
Classic homocystinuria is homozygous deficiency of CBS.
Inherited as autosomal recessive trait. Occurs in 1 in 100,000 live births.
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms

Fasting tHcy levels up to 40 fold seen A vascular event occurs before the age of 30
in over 50% of untreated homozygotes.
Fasting tHcy levels up to 40 fold seen A vascular event occurs before the age of 30
in over 50% of untreated homozygotes.
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms - Homozygotes
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms - Homozygotes

Risk of vascular events is unclear as it is often associated with normal tHcy levels and may present with a mild clinical picture.
Over 60 mutations of CBS gene have been described with the most common being I278T and G307S.
Risk of vascular events is unclear as it is often associated with normal tHcy levels and may present with a mild clinical picture.
Over 60 mutations of CBS gene have been described with the most common being I278T and G307S.
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms - Heterozygotes
Inherited Hypercoaguable States Homocysteinemia from CBS
Polymorphisms - Heterozygotes

Homozygous deficiency is extremely rare and results in early death.
10-30% of white population is homozygous for this mutation.
This defect in the presence of suboptimal folate intake will result in moderately elevated tHcy plasma levels.
Homozygous deficiency is extremely rare and results in early death.
10-30% of white population is homozygous for this mutation.
This defect in the presence of suboptimal folate intake will result in moderately elevated tHcy plasma levels.
Inherited Hypercoaguable States Homocysteinemia from MTHFR
Polymorphisms
Inherited Hypercoaguable States Homocysteinemia from MTHFR
Polymorphisms

MTHFR C677T, Homozygous TT or A1298C are NOT risk factors for cerebral arterial or venous thrombosis.
MTHFR C677T, Homozygous TT or A1298C are NOT risk factors for cerebral arterial or venous thrombosis.
Inherited Hypercoaguable States
MTHR Polymorphisms & Stroke Inherited Hypercoaguable States
MTHR Polymorphisms & Stroke

The incidence of stroke increases with increasing Homocysteine levels.
Experimental studies suggest Homocysteine promotes ATHEROGENESIS and THROMBOEMBOLISM.
All young patients with unexplained stroke, especially those with atherosclerosis, SHOULD have Homcysteine levels checked.
The incidence of stroke increases with increasing Homocysteine levels.
Experimental studies suggest Homocysteine promotes ATHEROGENESIS and THROMBOEMBOLISM.
All young patients with unexplained stroke, especially those with atherosclerosis, SHOULD have Homcysteine levels checked.
Inherited Hypercoaguable States Homocysteinemia and Stroke
Inherited Hypercoaguable States Homocysteinemia and Stroke

Treated directly with vitamin supplementation.
Primary vitamin used is folate. Taking folate and vitamin B12 can lead to an
additional decrease in Homocysteine levels above that seen with folate alone.
Treated directly with vitamin supplementation.
Primary vitamin used is folate. Taking folate and vitamin B12 can lead to an
additional decrease in Homocysteine levels above that seen with folate alone.
Inherited Hypercoaguable States Homocysteinemia Treatment
Inherited Hypercoaguable States Homocysteinemia Treatment

Anticoagulation following vascular thrombosis Generally used for 3-6 months. Further continuation is generally not indicated in
hyperhomocysteinemia after a single thromboembolic episode given the risk of bleeding associated with anticoagulation.
Patients with multiple thromboembolic episodes may need to be on long-term anticoagulation.
Anticoagulation following vascular thrombosis Generally used for 3-6 months. Further continuation is generally not indicated in
hyperhomocysteinemia after a single thromboembolic episode given the risk of bleeding associated with anticoagulation.
Patients with multiple thromboembolic episodes may need to be on long-term anticoagulation.
Inherited Hypercoaguable States Homocysteinemia Treatment
Inherited Hypercoaguable States Homocysteinemia Treatment

Autosomal recessive genetic disease: β-globin gene (chromosome 11q) mutation
GAGGTG at 6th codon Glutamic Acid Valine at the 6th amino acid
along the β-globin chain
α2β2 = normal hemoglobin
α2βS = heterozygote = Sickle trait
α2S2 = homozygous recessive = Sickle cell disease
Autosomal recessive genetic disease: β-globin gene (chromosome 11q) mutation
GAGGTG at 6th codon Glutamic Acid Valine at the 6th amino acid
along the β-globin chain
α2β2 = normal hemoglobin
α2βS = heterozygote = Sickle trait
α2S2 = homozygous recessive = Sickle cell disease
INHERITED RISK FACTOR
Sickle Cell Disease INHERITED RISK FACTOR
Sickle Cell Disease

Sickle cell disease causes a vasculopathy that, along with stasis in small arteries, is a principal mechanism by which it causes strokes.
The mechanism is a progressive, segmental narrowing of the distal internal carotid artery and portions of the circle of willis and proximal branches of the major intracranial arteries.
Sickle cell disease causes a vasculopathy that, along with stasis in small arteries, is a principal mechanism by which it causes strokes.
The mechanism is a progressive, segmental narrowing of the distal internal carotid artery and portions of the circle of willis and proximal branches of the major intracranial arteries.
INHERITED RISK FACTOR
Sickle Cell Disease INHERITED RISK FACTOR
Sickle Cell Disease

The incidence of brain infarction peaks around age 10 years.
The incidence of stroke in patients with Hb SS is 10% and those with Hb SC is 2-5%.
The incidence of brain infarction peaks around age 10 years.
The incidence of stroke in patients with Hb SS is 10% and those with Hb SC is 2-5%.
INHERITED RISK FACTOR
Sickle Cell Disease INHERITED RISK FACTOR
Sickle Cell Disease

Hypercoaguability and StrokeHypercoaguability and Stroke
Acquired Hypercoaguable
States
Acquired Hypercoaguable
States

Hypercoaguability and StrokeHypercoaguability and Stroke
Antiphospholipid SyndromeAntiphospholipid Syndrome

Antiphospholipid SyndromeAntiphospholipid Syndrome
Most common acquired thrombophilia Described by Dr. Graham Hughes (1983)
now at the Lupus Center, London, UK.
A syndrome characterized by the association of: thrombosis, obstetric complications and/or
thrombocytopenia antibodies against phospholipids or against proteins
bound to phospholipids.
Most common acquired thrombophilia Described by Dr. Graham Hughes (1983)
now at the Lupus Center, London, UK.
A syndrome characterized by the association of: thrombosis, obstetric complications and/or
thrombocytopenia antibodies against phospholipids or against proteins
bound to phospholipids.

Antiphospholipid Syndrome Etiology
Antiphospholipid Syndrome Etiology
• Combination of genetic background and environmental factors: infection, trauma, drugs
- infections – molecular mimicry with B2GPI
• Combination of genetic background and environmental factors: infection, trauma, drugs
- infections – molecular mimicry with B2GPI

APS PathophysiologyAPS Pathophysiology
platelets
Coagulation cascade
Endothelial cells
Activate platelet
aggregation
Inhibit Protein C, Protein S,
thrombomodulin, antithrombin III
fibrinolysis
TF, adhesion molecules and
proinflammatory cytokines
Placental tissue
Trophoblastic cell growth,
apoptosis
IL-3
Complement system
aCLaCL

• Venous thrombosis: Most common: deep or superficial veins of the legs Less common: IVC, iliofemoral, axillary, renal, portal, hepatic, or retinal veins
• Arterial thrombosis: Most common: Cerebral infarct, cardiogenic emboli. Less common: Coronary, retinal, and visceral artery
• Cutaneous: Livedo reticularis (up to 80%), splinter hemorrhages, leg ulcer, skin insarcts, blue toe syndrome
• Venous thrombosis: Most common: deep or superficial veins of the legs Less common: IVC, iliofemoral, axillary, renal, portal, hepatic, or retinal veins
• Arterial thrombosis: Most common: Cerebral infarct, cardiogenic emboli. Less common: Coronary, retinal, and visceral artery
• Cutaneous: Livedo reticularis (up to 80%), splinter hemorrhages, leg ulcer, skin insarcts, blue toe syndrome
• Neuro: Multi-infarct dementia, chorea, transverse myelopathy, Pseudotumor cerebri, cerebral venous thrombosis APLA are found in as many as 50% of patients who get migraines
• Cardiac: CAD, valve vegetations or thickening 30%, intracardiac thrombus
• Hematologic: Thrmobocytopenia (40% of patients), hemolytic anemia
• Obstetric: Fetal loss (15-75%), IUGR
• Neuro: Multi-infarct dementia, chorea, transverse myelopathy, Pseudotumor cerebri, cerebral venous thrombosis APLA are found in as many as 50% of patients who get migraines
• Cardiac: CAD, valve vegetations or thickening 30%, intracardiac thrombus
• Hematologic: Thrmobocytopenia (40% of patients), hemolytic anemia
• Obstetric: Fetal loss (15-75%), IUGR
Antiphospholipid SyndromeClinical manifestations
Antiphospholipid SyndromeClinical manifestations

Antiphospholipid AntibodiesThree primary classes of AntibodiesAntiphospholipid Antibodies
Three primary classes of Antibodies
1. Lupus Anticoagulant (LA) antibodies are directed against plasma proteins bound to anionic phospholipids
2. Anti-Cardiolipin (aCL) antibodies are directed against phospholipids bound to proteins Can be IgA, M, or G (subclasses 1-4) IgG (esp G2) associated with a greater risk of APS
3. Anti Beta 2 Glycoprotein (2GPI) antibodies are
directed against a plasma protein that binds phospholipid with high affinity
1. Lupus Anticoagulant (LA) antibodies are directed against plasma proteins bound to anionic phospholipids
2. Anti-Cardiolipin (aCL) antibodies are directed against phospholipids bound to proteins Can be IgA, M, or G (subclasses 1-4) IgG (esp G2) associated with a greater risk of APS
3. Anti Beta 2 Glycoprotein (2GPI) antibodies are
directed against a plasma protein that binds phospholipid with high affinity

Many patients have laboratory evidence of APS antibodies WITHOUT clinical disease.
APS antibodies found in 10% of healthy donors, 30-50% of SLE patients
APS may develop in 50 to 70 % of patients with both SLE and APS antibodies after 20 years of follow-up.
Nonetheless, up to 30 percent of patients with SLE and anticardiolipin antibodies lacked any clinical evidence of APS over an average follow-up of seven years.
Many patients have laboratory evidence of APS antibodies WITHOUT clinical disease.
APS antibodies found in 10% of healthy donors, 30-50% of SLE patients
APS may develop in 50 to 70 % of patients with both SLE and APS antibodies after 20 years of follow-up.
Nonetheless, up to 30 percent of patients with SLE and anticardiolipin antibodies lacked any clinical evidence of APS over an average follow-up of seven years.
Antiphospholipid SyndromeEpidemiology
Antiphospholipid SyndromeEpidemiology

Population aCL LA
Normal individuals: 2-5% 0-1%
Normal pregnancy: 1-10% -
Elderly (>70 years of age): >50% -
Patients with SLE: 17-86% 7-65%
Family members of patients with APS: 8-31% -
Antiphospholipid SyndromeFrequency of APS antibodies in different
populations
Antiphospholipid SyndromeFrequency of APS antibodies in different
populations

Antiphospholipid Syndrome Risk of thrombosis in patients with APS
antibodies
Antiphospholipid Syndrome Risk of thrombosis in patients with APS
antibodies
Incidence of thrombosis: ~2-2.5%†. Coincident risk factors for thrombosis: up to 50%‡.
Incidence of thrombosis: ~2-2.5%†. Coincident risk factors for thrombosis: up to 50%‡.
Odds Ratios for VTE
SLE with lupus anticoagulant 6.32 (3.80-8.27)*
Non-SLE with lupus anticoagulant
11.1 (3.81-32.3)**
Lupus (1997) 6: 467. ** Lupus (1998) 7: 15.† Am J Med (1996) 100: 530. ‡ J Rheumatol (2004) 31: 1560.

Despite the frequent concordance between lupus anticoagulant antibodies and either anticardiolipin or anti– B 2 Glycoprotein I antibodies, these antibodies are NOT identical.
In general, lupus anticoagulant antibodies are MORE SPECIFIC for the antiphospholipid syndrome, whereas anticardiolipin antibodies are MORE SENSITIVE.
Despite the frequent concordance between lupus anticoagulant antibodies and either anticardiolipin or anti– B 2 Glycoprotein I antibodies, these antibodies are NOT identical.
In general, lupus anticoagulant antibodies are MORE SPECIFIC for the antiphospholipid syndrome, whereas anticardiolipin antibodies are MORE SENSITIVE.
Antiphospholipid AntibodiesDetection & Clinical Relevance
Antiphospholipid AntibodiesDetection & Clinical Relevance

The SPECIFICITY of anti-cardiolipin antibodies for APS INCREASES WITH TITER and is HIGHER for IgG than for the IgM isotope.
MULTIPLE TESTS for antiphospholipid antibodies SHOULD BE USED, since patients may be negative according to one test yet positive according to another.
The SPECIFICITY of anti-cardiolipin antibodies for APS INCREASES WITH TITER and is HIGHER for IgG than for the IgM isotope.
MULTIPLE TESTS for antiphospholipid antibodies SHOULD BE USED, since patients may be negative according to one test yet positive according to another.
Antiphospholipid AntibodiesDetection & Clinical Relevance
Antiphospholipid AntibodiesDetection & Clinical Relevance

Primary APS If the patient HAS NO known underlying
autoimmune disorder.
Secondary APS If the patient HAS an underlying
autoimmune disorder, such as SLE.
Primary APS If the patient HAS NO known underlying
autoimmune disorder.
Secondary APS If the patient HAS an underlying
autoimmune disorder, such as SLE.
Antiphospholipid SyndromeClassification
Antiphospholipid SyndromeClassification

Studies have NOT SHOWN any clear differences between patients with Primary APS versus Secondary APS.
A risk of recurrent thrombi, both arterial and venous, is associated with both types of APS.
Most studies suggest that patients who have a recurrent episode will have it in a similar blood vessel type.
Studies have NOT SHOWN any clear differences between patients with Primary APS versus Secondary APS.
A risk of recurrent thrombi, both arterial and venous, is associated with both types of APS.
Most studies suggest that patients who have a recurrent episode will have it in a similar blood vessel type.
Antiphospholipid SyndromeClassification
Antiphospholipid SyndromeClassification

Antiphospholipid SyndromeDiagnosis - Clinical Criteria
Antiphospholipid SyndromeDiagnosis - Clinical Criteria
Vascular thrombosis: One episode of arterial, venous, or small vessel, in any
tissue or organ, confirmed by objective validated criteria
Pregnancy morbidity: Unexplained fetal death at or beyond 10 weeks gestation Premature birth before 34 weeks gestation because of
eclampsia, severe pre-eclampsia, or placental insufficiency
Three or more consecutive spontaneous abortions before 10 weeks gestation
Vascular thrombosis: One episode of arterial, venous, or small vessel, in any
tissue or organ, confirmed by objective validated criteria
Pregnancy morbidity: Unexplained fetal death at or beyond 10 weeks gestation Premature birth before 34 weeks gestation because of
eclampsia, severe pre-eclampsia, or placental insufficiency
Three or more consecutive spontaneous abortions before 10 weeks gestation
International Consensus Statement on Classification Criteria for APS (2006).Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306
International Consensus Statement on Classification Criteria for APS (2006).Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306

• Lupus anticoagulant (LA), present on at least 2 occasions, at least 12 weeks apart
• Anticardiolipin antibodies (aCL), IgG or IgM >30 units for both, present on at least 2 occasions, at least 12 weeks apart
• Anti-beta-2-glycoprotein I antibodies (anti-B2GPI), IgG or IgM >20 units for both, present on at least 2 occasions, at least 12 wks apart
• Lupus anticoagulant (LA), present on at least 2 occasions, at least 12 weeks apart
• Anticardiolipin antibodies (aCL), IgG or IgM >30 units for both, present on at least 2 occasions, at least 12 weeks apart
• Anti-beta-2-glycoprotein I antibodies (anti-B2GPI), IgG or IgM >20 units for both, present on at least 2 occasions, at least 12 wks apart
Antiphospholipid SyndromeDiagnosis - Laboratory Criteria
Antiphospholipid SyndromeDiagnosis - Laboratory Criteria
International Consensus Statement on Classification Criteria for APS (2006).Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306
International Consensus Statement on Classification Criteria for APS (2006).Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306

A diagnosis of Antiphospholipid Syndrome should NOT be made if a period of greater than five years separates the clinical event and positive laboratory test.
Although antiphospholipid antibodies ALSO OCCUR in association with other conditions (including infections, cancer, and the use of drugs or hemodialysis), they are usually IgM antibodies that are present at low levels and ARE NOT associated with thrombotic events.
A diagnosis of Antiphospholipid Syndrome should NOT be made if a period of greater than five years separates the clinical event and positive laboratory test.
Although antiphospholipid antibodies ALSO OCCUR in association with other conditions (including infections, cancer, and the use of drugs or hemodialysis), they are usually IgM antibodies that are present at low levels and ARE NOT associated with thrombotic events.
Antiphospholipid SyndromeDiagnosis
Antiphospholipid SyndromeDiagnosis

Hypercoaguability and StrokeHypercoaguability and Stroke
Antiphospholipid Syndrome and Stroke
Antiphospholipid Syndrome and Stroke

• Published figures range from 7% of all strokes1 to 41% of all strokes2 (study relied on one single aPL assessment)
• In the younger population (under 45), it may be as high as one in 5 of all strokes associated with aPL.
• Published figures range from 7% of all strokes1 to 41% of all strokes2 (study relied on one single aPL assessment)
• In the younger population (under 45), it may be as high as one in 5 of all strokes associated with aPL.
Antiphospholipid Syndrome & StrokeIncidence
Antiphospholipid Syndrome & StrokeIncidence
1Montalban J et al. Stroke 1991;22:750-7532Levine SR et al. JAMA 2004;291:576-584
1Montalban J et al. Stroke 1991;22:750-7532Levine SR et al. JAMA 2004;291:576-584

Antiphospholipid Syndrome & StrokeAPASS Study 2004
Antiphospholipid Syndrome & StrokeAPASS Study 2004
Only RCT Study (prospective cohort study). Conducted within the WARSS study. 720 of the 1770 patients in WARSS tested positive
for aPL (41%) Compared warfarin (target INR 1.4 to 2.8) vs. ASA. Analyzed antiphospholipid status after stroke. Composite outcome measure including death,
ischemic stroke, or other thromboembolic events.
Only RCT Study (prospective cohort study). Conducted within the WARSS study. 720 of the 1770 patients in WARSS tested positive
for aPL (41%) Compared warfarin (target INR 1.4 to 2.8) vs. ASA. Analyzed antiphospholipid status after stroke. Composite outcome measure including death,
ischemic stroke, or other thromboembolic events.

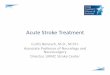
APASS StudyOutcomes
APASS StudyOutcomes
Warfarin Aspirin0
10
20
30
aPL +aPL -
Treatment Group
Pro
porti
on w
ithE
vent
at 2
Yea
rs
APASS Investigators, JAMA, 2004; 291: 576.

Patients from the general population who have sustained an initial non-cardioembolic stroke and are POSITIVE for LA and aCL (ELISA – low, medium or high titers included) within 30 days of the Stroke (patients tested once) DO NOT have a different prognosis than those who test NEGATIVE.
This result was consistent the Aspirin and Warfarin arms of the trial.
Patients from the general population who have sustained an initial non-cardioembolic stroke and are POSITIVE for LA and aCL (ELISA – low, medium or high titers included) within 30 days of the Stroke (patients tested once) DO NOT have a different prognosis than those who test NEGATIVE.
This result was consistent the Aspirin and Warfarin arms of the trial.
Antiphospholipid Syndrome & StrokeAPASS Study 2004 - Caveats
Antiphospholipid Syndrome & StrokeAPASS Study 2004 - Caveats

Hypercoaguability and StrokeHypercoaguability and Stroke
TreatmentTreatment

• Prevention of noncardioembolic cerebral ischemic events.– For most patients, we recommend antiplatelet
agents over oral anticoagulation (Grade 1A).– For patients with ‘well-documented’
prothrombotic disorders, we suggest oral anticoagulation over antiplatelet agents (Grade 2C).
• Prevention of noncardioembolic cerebral ischemic events.– For most patients, we recommend antiplatelet
agents over oral anticoagulation (Grade 1A).– For patients with ‘well-documented’
prothrombotic disorders, we suggest oral anticoagulation over antiplatelet agents (Grade 2C).
Albers, et al., Chest, 2004; 126 (Supplement): 483S.
Antiphospholipid SyndromeACCP Guidelines
Antiphospholipid SyndromeACCP Guidelines

• Retrospective studies suggest target INR > 3.0.– Rosove & Brewer (1992).– Khamashta, et al. (1995).
• Prospective randomized trials suggest target INR of 2 to 3.– Crowther, et al. (2003).– Finazzi, et al. (2005).
• Retrospective studies suggest target INR > 3.0.– Rosove & Brewer (1992).– Khamashta, et al. (1995).
• Prospective randomized trials suggest target INR of 2 to 3.– Crowther, et al. (2003).– Finazzi, et al. (2005).
Antiphospholipid SyndromeEvidence for Treatment Recommendations
Antiphospholipid SyndromeEvidence for Treatment Recommendations

We conclude that the presence of a persistent aPL has NOT been demonstrated as such an important risk factor for recurrent thrombosis that it warrants more intensive (and more risk-bearing) treatment1.
Patients with positive aPL tests would really be helped with data from studies that enable evidence based recommendations for treatment1.
We conclude that the presence of a persistent aPL has NOT been demonstrated as such an important risk factor for recurrent thrombosis that it warrants more intensive (and more risk-bearing) treatment1.
Patients with positive aPL tests would really be helped with data from studies that enable evidence based recommendations for treatment1.
Antiphospholipid Syndrome Treatment of aPL positive patients
Antiphospholipid Syndrome Treatment of aPL positive patients
1RHWM Derkson et al. Lupus 2010 19. 470-4741RHWM Derkson et al. Lupus 2010 19. 470-474

Hypercoaguability and StrokeHypercoaguability and Stroke
Thrombotic Thrombocytopenic Purpura
(TTP)
Thrombotic Thrombocytopenic Purpura
(TTP)

TTPHistoryTTP
History
• In 1924, Dr.Eli Moschcowitz described a 16- year old girl with abrupt onset of petechiae, pallor, followed by paralysis, coma, and death.
• Autopsy showed ‘hyaline’ thrombi occluding terminal arterioles and capillaries.
• In 1924, Dr.Eli Moschcowitz described a 16- year old girl with abrupt onset of petechiae, pallor, followed by paralysis, coma, and death.
• Autopsy showed ‘hyaline’ thrombi occluding terminal arterioles and capillaries.

TTPPresentation
TTPPresentation
Clinical findings1. Fever2. Neurologic changes3. Renal impairment
Laboratory findings4. Microangiopathic hemolytic anemia (Hb <
10g/dl)5. Thrombocytopenia (Platelets < 20,000/µl)
Clinical findings1. Fever2. Neurologic changes3. Renal impairment
Laboratory findings4. Microangiopathic hemolytic anemia (Hb <
10g/dl)5. Thrombocytopenia (Platelets < 20,000/µl)
Classic PentadAll 5 criteria present
Classic PentadAll 5 criteria present

TTPClinical Presentation
TTPClinical Presentation
• Approx. 1000 new cases occur each year
• Common in middle age; median age = 40
• Female : male (2:1)
• Acute onset and fulminant course
• Mortality rate >90% in pre-pheresis era.
• Relapse rates, 10-40% ranging from months to years have been reported.
• Approx. 1000 new cases occur each year
• Common in middle age; median age = 40
• Female : male (2:1)
• Acute onset and fulminant course
• Mortality rate >90% in pre-pheresis era.
• Relapse rates, 10-40% ranging from months to years have been reported.

TTPPathogenesis
TTPPathogenesis
Deficiency of VWF- cleaving protease Termed ADAMTS13 Corresponding gene : chromosome 9q34.
Deficiency of VWF- cleaving protease Termed ADAMTS13 Corresponding gene : chromosome 9q34.

TTPPathogenesis – ADAMTS13
TTPPathogenesis – ADAMTS13
CUBS MP CysDD Spacer11 22 33 44 55 66 77 88 CUB
Metalloprotease
Disintegrin
Thrombospondin 1
A Disintegrin-like And Metalloprotease with ThromboSpondin-1 repeats (ADAMTS13)
Discovered in 1996 by Tsai and by Furlan
Requires Ca2+ and Zn2+ ions
Cleaves VWF between Tyr1605 - Met1606
Activated by shear stress, mild denaturants
Discovered in 1996 by Tsai and by Furlan
Requires Ca2+ and Zn2+ ions
Cleaves VWF between Tyr1605 - Met1606
Activated by shear stress, mild denaturants

Proteolysis by ADAMTS13Cleaves VWF Tyr1605-Met1606 INCREASE causes VWD (type 2A)DECREASE causes TTP
TTPPathogenesis – ADAMTS13
TTPPathogenesis – ADAMTS13

TTPPrimary TTP
TTPPrimary TTP
1. Familial recurrent TTP: Constitutional deficiency of VWF
1. Familial recurrent TTP: Constitutional deficiency of VWF

TTPSecondary TTP
TTPSecondary TTP
• Drug-induced– Acute immune mediated:
• Ticlopidine - frequency is 1/2000-1/5000 in pts receiving ticlid post-coronary stent1.
• Plavix – frequency is <1/20,000. Usually occurs in first 2 weeks, responds to stopping medication2.
– Dose-related: mitomycin, tacrolimus, pencillin, cyclosporine, cisplatin, bleomycin, OCP
– Quinine: HUS like illness.
• Drug-induced– Acute immune mediated:
• Ticlopidine - frequency is 1/2000-1/5000 in pts receiving ticlid post-coronary stent1.
• Plavix – frequency is <1/20,000. Usually occurs in first 2 weeks, responds to stopping medication2.
– Dose-related: mitomycin, tacrolimus, pencillin, cyclosporine, cisplatin, bleomycin, OCP
– Quinine: HUS like illness.
1Bennett et al Ann Inter Med 19982Bennett et al N Engl J Med 2000
1Bennett et al Ann Inter Med 19982Bennett et al N Engl J Med 2000

TTPSecondary TTP
TTPSecondary TTP
• Pregnancy and post-partum.• Allogenic bone marrow transplant.• Autoimmune disorders (SLE,scleroderma)• HIV infection.
• Pregnancy and post-partum.• Allogenic bone marrow transplant.• Autoimmune disorders (SLE,scleroderma)• HIV infection.

TTPDiagnosis – There is no Gold Standard
TTPDiagnosis – There is no Gold Standard
Primary diagnostic criteria Thrombocytopenia ( often below <20,000) Microangiopathic hemolytic anemia
Negative Coomb’s test. Fragmented red cells (schistocytes) on peripheral smear LDH elevation is the hallmark of RBC destruction and tissue
injury related to ischemia.
Presence of above criteria is sufficient to establish presumptive diagnosis & begin PE
Primary diagnostic criteria Thrombocytopenia ( often below <20,000) Microangiopathic hemolytic anemia
Negative Coomb’s test. Fragmented red cells (schistocytes) on peripheral smear LDH elevation is the hallmark of RBC destruction and tissue
injury related to ischemia.
Presence of above criteria is sufficient to establish presumptive diagnosis & begin PE

TTPDiagnosis
TTPDiagnosis
• At present there are no confirmatory tests available.
• Other features in pentad support the diagnosis.
• Tests for ADAMTS13 deficiency or inhibitors are not readily available and lack standardization.
• At present there are no confirmatory tests available.
• Other features in pentad support the diagnosis.
• Tests for ADAMTS13 deficiency or inhibitors are not readily available and lack standardization.

TTPDifferential Diagnosis
TTPDifferential Diagnosis
• Disseminated intravascular coagulation.
• Sepsis: cytomegalovirus, rocky mountain spotted fever, meningococcemia.
• Preeclampsia/eclampsia, HELLP.
• Disseminated malignancy.
• Hemolytic-uremic syndrome
• Evans syndrome
• Malignant hypertension.
• Disseminated intravascular coagulation.
• Sepsis: cytomegalovirus, rocky mountain spotted fever, meningococcemia.
• Preeclampsia/eclampsia, HELLP.
• Disseminated malignancy.
• Hemolytic-uremic syndrome
• Evans syndrome
• Malignant hypertension.

TTPTreatment
TTPTreatment
Plasma exchange: Untreated TTP has 80-90% mortality. Removes ULvWF multimers, autoantibody
and replaces metalloproteinase. Randomized controlled trial (Rock et al, 1991) FFP as the replacement fluid is most widely
used and cost effective.
Plasma exchange: Untreated TTP has 80-90% mortality. Removes ULvWF multimers, autoantibody
and replaces metalloproteinase. Randomized controlled trial (Rock et al, 1991) FFP as the replacement fluid is most widely
used and cost effective.

TTPResponse To Treatment
TTPResponse To Treatment
Mental Status changes improve dramatically. Thrombocytopenia require several days. Parameters of hemolysis improve promptly, yet
anemia may continue to worsen. Recovery from renal failure is unpredictable and
often slow. Prolonged courses of Plasma Exchange, with
frequent exacerbations is characteristic of idiopathic TTP
Mental Status changes improve dramatically. Thrombocytopenia require several days. Parameters of hemolysis improve promptly, yet
anemia may continue to worsen. Recovery from renal failure is unpredictable and
often slow. Prolonged courses of Plasma Exchange, with
frequent exacerbations is characteristic of idiopathic TTP

TTPDuration of treatment.
TTPDuration of treatment.
No studies precisely determine optimal schedule AABB extracorporeal therapy committee: daily PE
until plt ct > 150k for 2-3 days. American Society for Apheresis: daily PE until Plt
> 100k, complete normalization of LDH. Tapering schedule to 3 times per week after
sustained response is highly recommended.
No studies precisely determine optimal schedule AABB extracorporeal therapy committee: daily PE
until plt ct > 150k for 2-3 days. American Society for Apheresis: daily PE until Plt
> 100k, complete normalization of LDH. Tapering schedule to 3 times per week after
sustained response is highly recommended.

TTPTreatment
TTPTreatment
AVOID prophylactic platelet transfusion UNLESS life-threatening bleeding is present1,2 because Platelet transfusion provides additional
substrate for thrombus formation. MI and strokes have reportedly occurred after
transfusion.
AVOID prophylactic platelet transfusion UNLESS life-threatening bleeding is present1,2 because Platelet transfusion provides additional
substrate for thrombus formation. MI and strokes have reportedly occurred after
transfusion.
1Gordon et al , 1987; 2Harkness et al 1981
1Gordon et al , 1987; 2Harkness et al 1981

Plasma exchange DOES NOT address the underlying autoimmune disorder
Refractory disease MAY benefit from immunosuppression
ADAMTS13 and inhibitor assays MAY become useful to guide therapy
Plasma exchange DOES NOT address the underlying autoimmune disorder
Refractory disease MAY benefit from immunosuppression
ADAMTS13 and inhibitor assays MAY become useful to guide therapy
TTPTreatment
TTPTreatment

TTPOther Treatment Options
TTPOther Treatment Options
Antiplatelet Therapy Steroids Splenectomy (Crowther et al, 1996) Chemotherapy: Cytoxan, Vincristine,
Rituxan, CHOP. High- dose IV IgG Protein A immunoadsorption columns.
Antiplatelet Therapy Steroids Splenectomy (Crowther et al, 1996) Chemotherapy: Cytoxan, Vincristine,
Rituxan, CHOP. High- dose IV IgG Protein A immunoadsorption columns.

TTPFollow-up and outcome
TTPFollow-up and outcome
Follow up Duration of initial treatment is undefined Monitor CBC and LDH
Outcome Relapse rates 29-82% Chronic renal insufficiency (~25%) Long term neurological effects (incidence ?)
Follow up Duration of initial treatment is undefined Monitor CBC and LDH
Outcome Relapse rates 29-82% Chronic renal insufficiency (~25%) Long term neurological effects (incidence ?)

Hypercoaguability and StrokeHypercoaguability and Stroke
Case Presentations
Case #1
Case Presentations
Case #1

Case #1Case #1 Mrs FC 44y R handed White female, non-smoker with h/o
Migraines on Maxalt who presented with new right handed numbness and weakness after a week following an uncomplicated tubal ligation done as an outpatient.
Past medical history significant for DVT during pregnancy (2nd and 4th) and had been on anticoagulation with Coumadin for 6 months after the last pregnancy.
Extensively worked up for a hypercoaguable state on multiple occasions including 6 months prior – all unremarkable / inconclusive.
Her evaluation during this hospitalization revealed a cortical infarct in the left hemisphere.
Mrs FC 44y R handed White female, non-smoker with h/o
Migraines on Maxalt who presented with new right handed numbness and weakness after a week following an uncomplicated tubal ligation done as an outpatient.
Past medical history significant for DVT during pregnancy (2nd and 4th) and had been on anticoagulation with Coumadin for 6 months after the last pregnancy.
Extensively worked up for a hypercoaguable state on multiple occasions including 6 months prior – all unremarkable / inconclusive.
Her evaluation during this hospitalization revealed a cortical infarct in the left hemisphere.

Case #1Case #1
Repeat hypercoaguable work up – Protein C / S, Homocysteine, aCL, LA, Factor V Leiden, Prothrombin gene mutation, ANA, RA all negative.
TEE – Normal, No PFO. Hematology consultation Started on Zocor, ASA and
discharged with 21 day event monitor set up.
Repeat hypercoaguable work up – Protein C / S, Homocysteine, aCL, LA, Factor V Leiden, Prothrombin gene mutation, ANA, RA all negative.
TEE – Normal, No PFO. Hematology consultation Started on Zocor, ASA and
discharged with 21 day event monitor set up.
Will this be her last admission for a Stroke?GOK
Will this be her last admission for a Stroke?GOK

Hypercoaguability and StrokeHypercoaguability and Stroke
Case Presentations
Case #2
Case Presentations
Case #2

Case #2Case #2Mrs WW 55 yr old AA, h/o HTN. Non smoker. Dad had CVA at 50. In February 2003, she presented with her first stroke at age
48. After an inconclusive Stroke in the Young, started on Plavix along with BP meds.
In July 2005, she presented with her second stroke and was started on Aggrenox. Had a repeat inconclusive Stroke in the Young work up.
In February 2006 presented with TIA like symptoms along with thrombocytopenia. Aggrenox suspected as cause of Thrombocytopenia. Seen by Hematology. Started on Coumadin.
In May 2007, presented with non-specific complaints, Platelets down to 13,000. Peripheral smear showed some hemolysis. Seen by hematologist and diagnosed with TTP. Started on Plasmapheresis and Steroids. Coumadin stopped.
Mrs WW 55 yr old AA, h/o HTN. Non smoker. Dad had CVA at 50. In February 2003, she presented with her first stroke at age
48. After an inconclusive Stroke in the Young, started on Plavix along with BP meds.
In July 2005, she presented with her second stroke and was started on Aggrenox. Had a repeat inconclusive Stroke in the Young work up.
In February 2006 presented with TIA like symptoms along with thrombocytopenia. Aggrenox suspected as cause of Thrombocytopenia. Seen by Hematology. Started on Coumadin.
In May 2007, presented with non-specific complaints, Platelets down to 13,000. Peripheral smear showed some hemolysis. Seen by hematologist and diagnosed with TTP. Started on Plasmapheresis and Steroids. Coumadin stopped.

Case #2Case #2
Mrs WW In July 2007 she presented with sepsis / septic shock,
treated and discharged. In October 2008, she presented with her third stroke. I saw
her then. Repeated stroke n the young work up again along with a cardiac MRI – negative. Continued on ASA 81mgs.
In December 2008, presented with worsening thrombocytopenia and admitted and started on plasmapheresis and steroids.
In April 2009, she presented with her fourth stroke. Started on Plasmapheresis and steroids and continued on ASA 81mgs. Then refused chemotherapy and splenectomy.
Mrs WW In July 2007 she presented with sepsis / septic shock,
treated and discharged. In October 2008, she presented with her third stroke. I saw
her then. Repeated stroke n the young work up again along with a cardiac MRI – negative. Continued on ASA 81mgs.
In December 2008, presented with worsening thrombocytopenia and admitted and started on plasmapheresis and steroids.
In April 2009, she presented with her fourth stroke. Started on Plasmapheresis and steroids and continued on ASA 81mgs. Then refused chemotherapy and splenectomy.

Case #2Case #2Mrs WW In April 2010 she presented with her fifth stroke. Again
started on Plasmapheresis and steroids and continued on ASA 81mgs. Again refused chemotherapy and splenectomy.
In May 2010 she presented with her sixth stroke. Again started on Plasmapheresis and steroids and continued on ASA 81mgs. Her ADAMTS 13 inhibitor levels were 6.8 (normal < 0.4) suggestive of a possible recurrence. This time she agreed to be started on the Rituximab and an elective splenectomy.
She was discharged on May 17, 2010.
Mrs WW In April 2010 she presented with her fifth stroke. Again
started on Plasmapheresis and steroids and continued on ASA 81mgs. Again refused chemotherapy and splenectomy.
In May 2010 she presented with her sixth stroke. Again started on Plasmapheresis and steroids and continued on ASA 81mgs. Her ADAMTS 13 inhibitor levels were 6.8 (normal < 0.4) suggestive of a possible recurrence. This time she agreed to be started on the Rituximab and an elective splenectomy.
She was discharged on May 17, 2010.
Will this be her last admission for a Stroke?GOK
Will this be her last admission for a Stroke?GOK

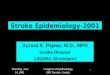
Case # 2 – MRI DWI ImagingCase # 2 – MRI DWI Imaging
Oct 2008Oct 2008 Feb 2009Feb 2009
Apr 2010Apr 2010 May 2010May 2010
Feb 2003Feb 2003 Jul 2005Jul 2005

Hypercoaguability and StrokeHypercoaguability and Stroke
Final SummaryFinal Summary

Connect the dots….Connect the dots….1. ASK the right questions in History.2. LOOK for embolic strokes or venous strokes on
MRI Imaging. 3. CONFIRM presence or absence of PFO.4. ORDER patient specific Hypercoaguable workup. 5. OBTAIN hematologist consultation BEFORE
initiating anticoagulation.6. NEVER forget to address the usual stroke
causes.7. PRAY for and with your patient.
1. ASK the right questions in History.2. LOOK for embolic strokes or venous strokes on
MRI Imaging. 3. CONFIRM presence or absence of PFO.4. ORDER patient specific Hypercoaguable workup. 5. OBTAIN hematologist consultation BEFORE
initiating anticoagulation.6. NEVER forget to address the usual stroke
causes.7. PRAY for and with your patient.

Remember….Site of Thrombosis Vs. Coagulation Defect
Remember….Site of Thrombosis Vs. Coagulation Defect
Abnormality Arterial VenousFactor V Leiden - +
Prothrombin G20210A - +
Antithrombin deficiency - +
Protein C deficiency - +
Protein S deficiency - +
Hyperhomocysteinemia + +
LA/ aCL / aPL + +
Abnormality Arterial VenousFactor V Leiden - +
Prothrombin G20210A - +
Antithrombin deficiency - +
Protein C deficiency - +
Protein S deficiency - +
Hyperhomocysteinemia + +
LA/ aCL / aPL + +

Hypercoaguability and StrokeHypercoaguability and Stroke
The End
Thank You
Questions / Comments
The End
Thank You
Questions / Comments