Embed Size (px)
Citation preview

STRIDOR IN CHILDREN
By: Maj Vishal Gaurav
Moderator: Dr A Sethi

Definition
Harsh, high-pitched, noisy respiration/musical sound produced by turbulent airflow through partially obstructed upper airway
• Stridor is a symptom/sign, not a diagnosis/ disease
• Always indicative of airway obstruction

• Stertor Low-pitched snoring type

Further Terminology
• Supraglottic obstruction: – Inspiratory stridor (high-pitched)
• Extrathoracic trachea obstruction – includes glottis & subglottis: – Biphasic stridor (intermediate pitch)
• Intrathoracic trachea obstruction: – Expiratory stridor (wheeze)

Physics
• Poiseuille’s Law: Resistance inversely proportional to radius to 4th power
• Bernoulli’s Law: Pressure decreases as velocity increases, causing tendency to collapse

Anatomy
• LARYNX IN CHILDREN– HIGHER– LUMEN SMALLER– MORE ACUTE– EPIGLOTTIS: tubular & less rigid– OTHER LARYNGEAL CARTILAGES: less
rigid
Predictably stridor is more in children

Etiology
• Congenital
– Laryngomalacia
– Subglottic Stenosis
– Laryngeal Web
– Subglottic Haemangioma
– Congenital Vocal Cord Palsy

Etiology
• Inflammatory
– Acute Supraglottitis
– Acute Laryngo-Tracheo-Bronchitis
– Laryngeal Edema
– Amyloidosis
– Scleroma
– Neck Space Infections / Abscess

Etiology
• Neoplastic
– Benign
• Salivary Tumors of Airway
• Haemangioma
• Adenoma
• Fibroma

Etiology
• Neoplastic
– Malignant
• Squamous Cell Carcinoma
• Thyroid Malignancies
• Lymphoma

Etiology
• Traumatic
– Laryngo-Tracheal Trauma
– Iatrogenic
• Thyroid Surgery
• Cardiothoracic Surgery
• Prolonged Intubation
– Thermal Injury
– Smoke Inhalation

Etiology
• Miscellaneous
– Foreign Bodies
– Laryngospasm
– Angioedema
– Tracheomalacia
– Laryngocele

Causes of Laryngeal Inspiratory Stridor
• Congenital– Web– Subglottic stenosis– Cyst– Laryngomalacia– VC Paralysis– Micrognathia– Cleft Larynx– Lymphangioma– Hemangioma
• Acquired– Pyrexial
• Ac Epiglottitis• Ac Laryngitis• Ac L-T-Bronchitis• Diphtheria
– Apyrexial• FB• Injury• Scald• Papilloma

Associated Symptoms
• Dyspnoea– Stridor & Dyspnoea are both manifestations of
airway obstruction; severity of one reflects severity of the other
• Cough– Harsh, barking
• Hoarseness– of speech/ cry
• Deglutition– Stridor increases during feeding– Stidorous infants are poor feeders

History taking
• Continuous (more serious) / Intermittent
• Severity– loudness, cyanosis, apnoea
• Age at onset– Congenital disease , manifest some time after
birth (activity, first URTI)
• Relationship to feeding/crying/exercise– May only be noticeable then

Physical examination
• Signs of increased airway resistance– Flaring of nostrils– suprasternal/intercostal/substernal recession
• Tachypnoea• Cyanosis• Rising Pulse rate• Periods of apnoea• Bronchopneumonia• Emphysema• Bronchiectasis

Radiology
• Plain lat Soft-tissue X-rays– Epiglottis– Subglottis

• X-ray Chest– atelectasis, consolidation, emphysema
• CT scan, MRI
• Barium swallow

Endoscopy
All children with stridor should be
endoscoped
Laryngoscopy• Bronchoscopy• Microlaryngoscopy• Flexible endoscopy – problematic in infants
Documentation

Evaluation of a Case of Stridor

HISTORY
• Onset
• Duration
• Any Cough / Fever / Spasmodic Cough?
• Abnormal cry / Hoarseness
• Any feeding difficulty / Dysphagia?
• Aggravating / Relieving factors
• Related to feeding/ posture?
• Weight loss

Examination
• General Examination
– TPR, Nutrition, Colour
– While Sleeping
– Effect of effort on stridor
– Note quality of cry – Dysphonia?
– Study while feeding
– Change positions and see
• Chest Examination

ENT Examination
• Throat
• Indirect Laryngoscopy
• Video Laryngoscopy
• Flexible Fiberoptic Laryngoscopy
• Neck Examination

Investigations
• If time permits
• Blood Counts, ABG, Electrolytes
• X-Ray Chest (PA), X-Ray Soft Tissue Neck (Lat)
• Fluoroscopy
• Rarely, Ba Swallow, CT Scan
• Direct Laryngoscopy with / without anaesthesia
• Bronchoscopy, if reqd.
• Oesophagoscopy under GA

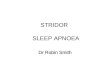
Laryngomalacia• Most common congenital cause
• Soft supraglottic Lx, decreased inlet
• Long epiglottis, curled
• Short aryepiglottic folds
• Lx suprastructure sucked in during inspiration
• Stridor increased on crying, decreased in prone position
• Disappears by 3rd – 4th year
• Inspiratory stridor without hoarseness suggestive
• Dx following DLS
• Rx - Reassurance

Laryngeal Web
• Generally seen b/w the VC’s anteriorly
• Stridor, aphonia from birth
• If big – early surgery/ Laser
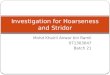
CONGENITAL VOCAL CORD PALSY

Congenital Subglottic Stenosis• If mild – resp infections cause dyspnoea /
stridor
• Dx if subglottic diameter is < 4 mm in a full term neonate

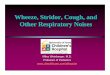
Subglottic Haemangioma
• Increase in size at 3-6 months age
• HPV infection
• Associated cutaneous haemangioma
• Dx FOB or DLS
• Rx Endoscopic surgical removal/ Laser + Adjuvant medical therapy (prolonged steroid adm)

Laryngocoele
• Dilatation of saccule of larynx – extending between the thyroid cartilage and ventricle
• Internal/ External

Principles of Management
• ASSESSMENT OF RESPIRATORY IN SUFFICIENCY
• ASSESSMENT OF THE LIKELY CAUSE
• ESTABLISHING AN AIRWAY
• TREATING THE CAUSE

Management
• Stridor with pyrexia
– Assess quickly
– Humidity, Warmth
– Antibiotics
– Steroids – Inhaled / Parenteral
– Racemic Epinephrine
– If no improvement in few hours hospitalisation

Management
• In hospital
– Assessed by Paed, ENT, Anaes
– Investigations
– Direct Laryngoscopy Intubation (if reqd)
– Alternative Airway
• Tracheostomy
• Cricothyroidotomy
– Treatment of specific cause

Conclusion
• Airway Emergency
• Rapid Assessment
• Treatment of Cause
• Prevent Hypoxia
• Alternative Airway
• Constant Monitoring