Embed Size (px)
Citation preview

STRESS MEDICINE, VOL. 10: 27-34 (1994)
STRESS EFFECTS ON THE HEALTH OF CHIEF EXECUTIVES OF BUSINESS ORGANIZATIONS
PAUL ROBINSON, BA, BSc(hons) PhD Team Management Services, Auckland, New Zealand
KERR INKSON, MA MPhil, PhD University of Auckland, New Zealand
SUMMARY Ninety-eight chief executive officers of business organizations employing at least 150 staff completed a battery of questionnaires measuring chronic and episodic non-work-related and work-related stressors; trait anxiety, locus of control, and type Ntype B personality; health-related lifestyle practices; and behaviours related to coping with stress. The medical history and blood pressure and blood chemistry measures of each respondent were assessed by a panel of medical experts and an index of physical health risk was computed. Factor analysis was used to refine measures of key dimensions of episodic and chronic work-related stress, and coping behaviours. Physical health risk was regressed as a dependent variable on to the independent variables of stressors, personality traits, and coping and health behaviours. Fifty-seven per cent of the variance in health risk was accounted for, with the four types of stressor, anxiety, lifestyle habits and ‘self-control’ coping mechanisms all contributing to the regression equation. The results particularly indicated the contribution of non-work-related stressors to physical health risk, and the moderating effects of lifestyle habits.
KEY woms-Stress, occupational stressors, personality, coping, physical health, executives.
The effects of occupational stress on physical and mental health have been much studied in recent years. Much of the research has been based on phy- siological studies, which have shown that stress adversely triggers a number of reactions in body cells, hormones, glands, fatty acids, etc. In a number of studies thesechanges in thehuman body have been associated with CHD (coronary heart disease).’ Fre- quent and prolonged exposure to stress can also lead to hypertension, ulcers and kidney disease, as well as to adverse psychological responses such as ner- vous tension, alienation and depressioq2 and to ~ a n c e r . ~ However, studies of the relationship between stress and health have typically only been able to account for about 10 per cent of the variance in illness in terms of
Studies of occupational stress are of three types. First, many studies of specific occupational or orga- nizational groups focus on the relationship between the stressors inherent in the job and perceived stress for the indi~idual.~.~ Secondly, an increasing
Address for correspondence: Prof. K. Inkson, Dept of Manage- ment Studies and Labour Relations, University of Auckland, Private Bag, Auckland, New Zealand. Tel: 010 64 (9) 373 7599, Ext. 7198. Fax: 010 64 (9) 373 7477.
number of studies have recently focused on the influence of ‘moderating’ variables such as persona- lityY7 exercise* and coping behaviour’ in modifying stress effects. Thirdly, studies in occupational epi- demiology have identified stress as a likely interven- ing factor between independent variables of occupation and dependent variables of health and morbidity.” Few studies, however, examine rela- tionships among all of the hypothesized variables (occupational stressors, non-occupational stres- sors, stress levels, moderating variables, and health).
Research on major stressors of professional managers has been reviewed by Glowinowski and Cooper.” They identified a number of potential fac- tors in the executive role leading to chronic stress, including intrinsic job factors, role conflict and ambiguity, relationships, career development fac- tors, and organizational structure and climate. Business executives are frequently stereotyped as suffering health-threatening levels of job-related stress due to their high responsibilities and as prac- tising unhealthy lifestyles (‘workaholism’, little exercise, excessive smoking and alcohol consump- tion, high CHD risk). However, in relation to Kara- sek’sI2 thesis that stress is greatest in roles
0748-8386/94/010027-08$09.00 0 1994 by John Wiley & Sons, Ltd.

28 P. ROBINSON AND K. INKSON
characterized by high demands and low discretion, executives tend to experience high demands but have high discretion. There is evidence that most business executives are generally able to avoid excessive stress and enjoy relatively good health.’’ Nevertheless, within any occupational group there will be major differences of stress level. The objec- tive of the present study was to investigate the rela- tive influences of various stressors, individual difference variables and lifestyle and coping vari- ables on the variance in overall health of a sample of chief executive officers (CEOs) in medium to large (minimum size 150 employees) New Zealand organizations.
MATERIALS AND METHODS
The sample consisted of 98 CEOs of organizations with over 150 employees from the Auckland (New Zealand) metropolitan area who were listed in the New Zealand Business Who’s Who, 26th and 27th editions. Of 125 CEOs recruited, 98 completed the procedure. Detailed demographic information about the sample is provided e1~ewhere.l~ A11 were male. Of the 95 who gave their ages, 78 per cent were aged between 37 and 54. Of the 96 who indi- cated their marital status, 95 per cent were married. Of 95 who indicated their educational attainments, 47 per cent had university degrees.
Each CEO was asked to complete a battery of questionnaires, including details of perceived stres- sors, stress levels, coping strategies, mental and physical health, and tests of dispositional factors likely to moderate stress and health levels. The pro- cedure took on average about 4 hours of each respondent’s time, and not surprisingly data were incomplete for some respondents. Full details of the methodology are provided elsewhere.13
The measurement of stressors acting on respon- dents used a range of instruments. The conceptuali- zation of stress sources involved considering both work-related and non-work-related (eg family) sources of stress. It also involved distinguishing between ‘chronic’ (ongoing) stressors, such as auto- cratic supervision and ongoing family tensions, and ‘episodic’ (single-event) sources, such as a takeover bid for the respondent’s organization or the death of a member of the respondent’s family.
Non-work-related stressors Standardized measures of non-work-related stres- sors were available: for episodic stressors, the 60- item Recent Life Changes questionnaire,“ based on the well-known Life Events Scale;” for chronic stressors, the Chronic Non-Work-Related Stress Evaluation Scale,16 which includes 16 five-point Likert scales enabling respondents to indicate the degree of stressfulness of various family-related and society-related concerns.
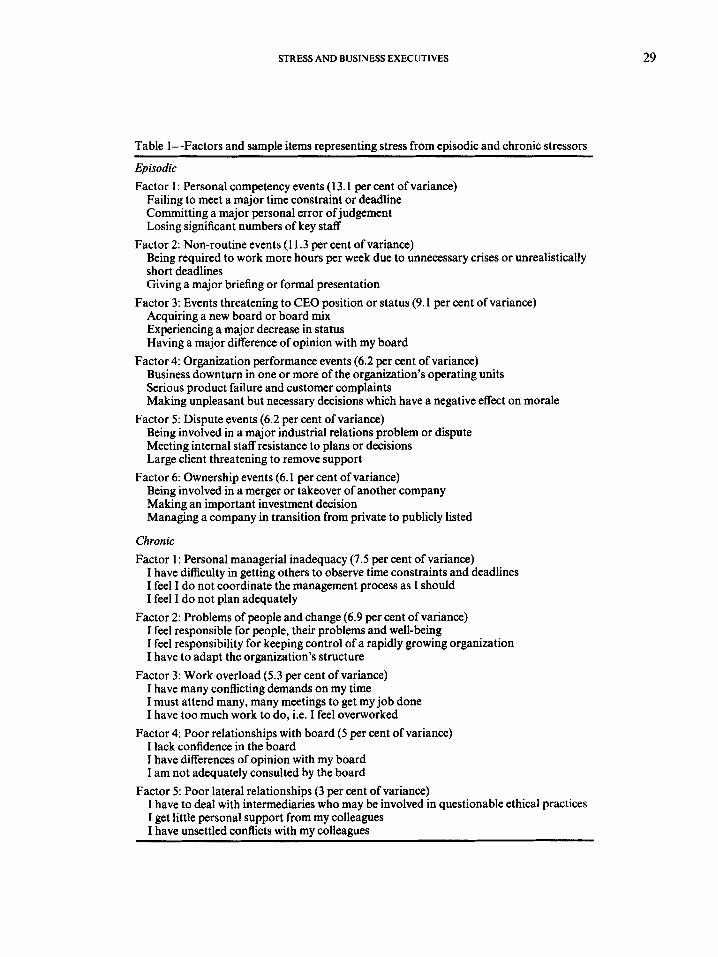
Work-related stressors Because of the uniqueness of the occupational sit- uations of the sample members, purpose-built mea- sures of work-related stressors were developed. First of all, a pilot study involving open-ended interview of 20 CEOs was conducted to generate potential scales for chronic and episodic work- related stressors. This resulted in a 55-item list of episodic stressors and a 60-item list of shronic stres- sors, which were administered to all respondents. In each case ratings of frequency and degree of stress were recorded, to indicate overall stressful- ness. The items on each list were subjected to factor analysis, yielding six interpretable episodic factors and four chronic factors. Measures of these factors were computed for inclusion in subsequent regres- sion analyses. Table 1 lists these factors and includes sample items. Full details of the analysis, factor loadings, etc, are provided elsewhere. l3
Personality factors Standard measures were included of three variables of individual personality which have in other stu- dies commonly been associated with stress. Trait anxiety” was measured by a plication of the Cattell 16PF personality measure’ and utilization of the ‘second-order’ factor anxietyheuroticism. Locus of controllg was measured b an extensively used mea- sure devised by James?’ Type A behaviour pat- tern” was measured by means of a well-validated 14-item measure.”
P
Lifestyle habits Lifestyle habits thought to moderate effects of stress on health were measured by means of the Appraisal of Lifestyle Habits Inventory (ALHI) in which respondents endorse up to seven ‘positive’ lifestyle habits (eg moderate drinking, eating reg- ular meals and no snacks, exercising regularly) they
STRESS AND BUSINESS EXECUTIVES 29
Table 1-Factors and sample items representing stress from episodic and chronic stressors
Episodic Factor 1: Personal competency events (13.1 per cent of variance)
Failing to meet a major time constraint or deadline Committing a major personal error of judgement Losing significant numbers of key staff
Being required to work more hours per week due to unnecessary crises or unrealistically short deadlines Giving a major briefing or formal presentation
Acquiring a new board or board mix Experiencing a major decrease in status Having a major difference of opinion with my board
Business downturn in one or more of the organization’s operating units Serious product failure and customer complaints Making unpleasant but necessary decisions which have a negative effect on morale
Being involved in a major industrial relations problem or dispute Meeting internal staff resistance to plans or decisions Large client threatening to remove support
Being involved in a merger or takeover of another company Making an important investment decision Managing a company in transition from private to publicly listed
Factor 2: Non-routine events (1 1.3 per cent of variance)
Factor 3: Events threatening to CEO position or status (9.1 per cent of variance)
Factor 4: Organization performance events (6.2 per cent of variance)
Factor 5: Dispute events (6.2 per cent of variance)
Factor 6: Ownership events (6.1 per cent of variance)
Chronic Factor 1 : Personal managerial inadequacy (7.5 per cent of variance)
I have difficulty in getting others to observe time constraints and deadlines I feel I do not coordinate the management process as I should I feel I do not plan adequately
Factor 2: Problems of people and change (6.9 per cent of variance) I feel responsible for people, their problems and well-being I feel responsibility for keeping control of a rapidly growing organization I have to adapt the organization’s structure
Factor 3: Work overload (5.3 per cent of variance) I have many conflicting demands on my time I must attend many, many meetings to get my job done I have too much work to do, i.e. I feel overworked
I lack confidence in the board I have differences of opinion with my board I am not adequately consulted by the board
I have to deal with intermediaries who may be involved in questionable ethical practices I get little personal support from my colleagues I have unsettled conflicts with my colleagues
Factor 4: Poor relationships with board (5 per cent of variance)
Factor 5: Poor lateral relationships (3 per cent of variance)
30 P. ROBINSON A N D K. INKSON
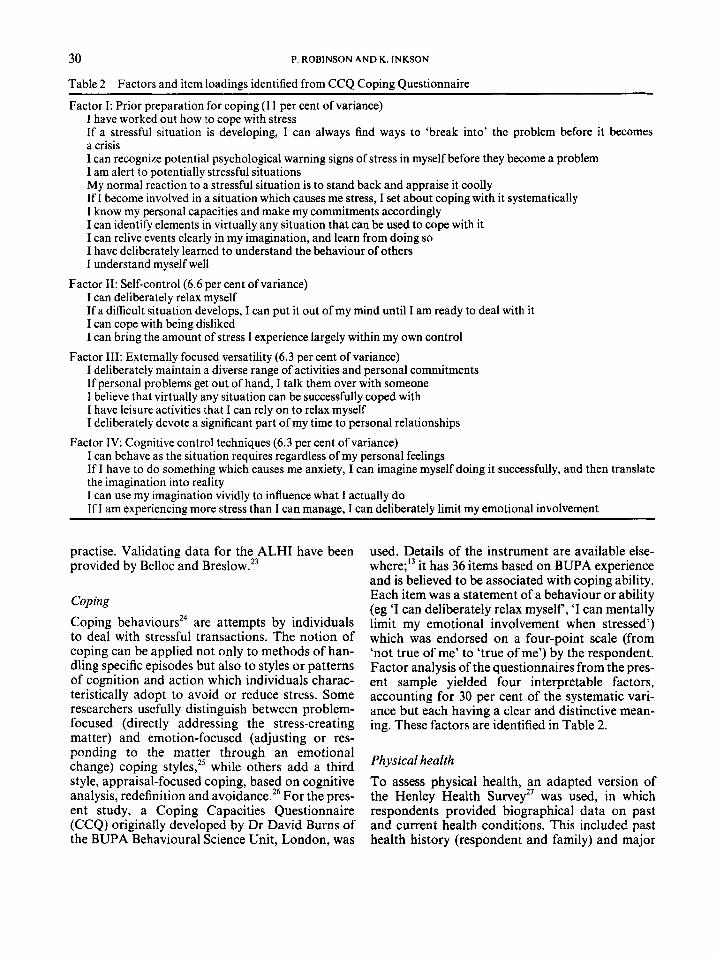
Table 2-Factors and item loadings identified from CCQ Coping Questionnaire
Factor I: Prior preparation for coping (1 1 per cent of variance) 1 have worked out how to cope with stress If a stressful situation is developing, I can always find ways to ‘break into’ the problem before it becomes a crisis I can recognize potential psychological warning signs of stress in myself before they become a problem I am alert to potentially stressful situations My normal reaction to a stressful situation is to stand back and appraise it coolly If I become involved in a situation which causes me stress, I set about coping with it systematically I know my personal capacities and make my commitments accordingly I can identify elements in virtually any situation that can be used to cope with it I can relive events clearly in my imagination, and learn from doing so I have deliberately learned to understand the behaviour of others I understand myself well
I can deliberately relax myself If a difficult situation develops, I can put it out of my mind until I am ready to deal with it I can cope with being disliked I can bring the amount of stress I experience largely within my own control
I deliberately maintain a diverse range of activities and personal commitments If personal problems get out of hand, I talk them over with someone I believe that virtually any situation can be successfully coped with I have leisure activities that I can rely on to relax myself I deliberately devote a significant part of my time to personal relationships
I can behave as the situation requires regardless of my personal feelings If I have to do something which causes me anxiety, I can imagine myself doing it successfully, and then translate the imagination into reality I can use my imagination vividly to influence what I actually do If I am experiencing more stress than I can manage, I can deliberately limit my emotional involvement
Factor 11: Self-control (6.6 per cent of variance)
Factor 111: Externally focused versatility (6.3 per cent of variance)
Factor IV: Cognitive control techniques (6.3 per cent of variance)
practise. Validating data for the ALHI have been provided by Belloc and Breslow.*j
Coping
Coping behavioursZ4 are attempts by individuals to deal with stressful transactions. The notion of coping can be applied not only to methods of han- dling specific episodes but also to styles or patterns of cognition and action which individuals charac- teristically adopt to avoid or reduce stress. Some researchers usefully distinguish between problem- focused (directly addressing the stress-creating matter) and emotion-focused (adjusting or res- ponding to the matter through an emotional change) coping styles,” while others add a third style, appraisal-focused coping, based on cognitive analysis, redefinition and avoidance.26 For the pres- ent study, a Coping Capacities Questionnaire (CCQ) originally developed by Dr David Bums of the BUPA Behavioural Science Unit, London, was
used. Details of the instrument are available else- where;13 it has 36 items based on BUPA experience and is believed to be associated with coping ability. Each item was a statement of a behaviour or ability (eg ‘I can deliberately relax myself, ‘I can mentally limit my emotional involvement when stressed’) which was endorsed on a four-point scale (from ‘not true of me’ to ‘true of me’) by the respondent. Factor analysis of the questionnaires from the pres- ent sample yielded four interpretable factors, accounting for 30 per cent of the systematic vari- ance but each having a clear and distinctive mean- ing. These factors are identified in Table 2.
Physical health To assess physical health, an adapted version of the Henley Health Survey2’ was used, in which respondents provided biographical data on past and current health conditions. This included past health history (respondent and family) and major

STRESS AND BUS11 VESS EXECUTIVES 31
Dependent variable: measure of physical health risk Stepwise regression with forward inclusion
(minimum significance criterion 0.30) was used. To isolate the independent variables which would yield the optimum prediction equation, the cutoff point was determined by statistical criteria suggested by Kerlinger and Pedhazer:28 that the overall F-ratio for the equation was significant, and that the partial regression coefficient (raw beta) for the indepen- dent variable being added was at a statistically sig- nificant level. Due to missing data preventing calculation of all the various measures in specific cases, the number of cases included in the regres- sion analyses was 5 1, a number which imposes limi- tations on the statistical power of the results.
and minor illness in the past 12 months. In addition, height and weight were indicated. With the assist- ance of appropriate1 y qualified paramedical and laboratory personnel, a blood pressure reading and a blood sample were taken from each respondent and the blood sample analysed in terms of the fol- lowing haematological and biochemical indices: MCV, Hb and MCH, ESR, uric acid, blood urea, GGT, blood lipids, cholesterol and LDWHDL cho- lesterol ratios.
In conjunction with Professor Ray West of the Auckland Medical School, an index of physical health risk was devised, to enable each respondent to be given an overall physical health rating based on all the biographical and medical data. A panel of three qualified doctors - a GP, a haematologist and a medical specialist in biochemistry - was con- vened, each member independently assessing each respondent on the scale of physical health risk. The index was represented by a four-point scale as indi- cated in Table 3.
Table 3-Scale of physical health risk and consensus des- criptors according to expert panel
Score Descriptor N O h
0 Negligible medical history contributing little or no future physical health risk 23 29 No consensus - between 0 and 1 3 4 Has some history of problems but these are unlikely to contribute to future health risk 28 35 No consensus - between 1 and 2 6 8
problems which may contribute to future health risk 17 22 No consensus - between 2 and 3 0 0
problems very likely to contribute to
1
2 Significant medical history of
3 Significant medical history of
future physical health risk 2 2
In total, the above procedures provided the fol- lowing variables for consideration in a regression analysis:
Independent variables: four measures of chronic work-related stressors; six measures of episodic work-related stressors; measure of chronic non- work related stressors; measure of episodic non-work-related stressors; three measures of individual personality; measure of lifestyle habits; four measures of coping behaviour
RESULTS
Results for physical health are given in Table 3. The overall health of the sample, represented by a mean score of 1.02, was generally very close to the second descriptor shown (‘has some history of health problems but these are unlikely to contribute to future physical health risk’), indicating that the majority appeared, for a generally middle-aged sample, to be in good health. However, a significant minority (24 per cent) were in the higher-risk cate- gories.
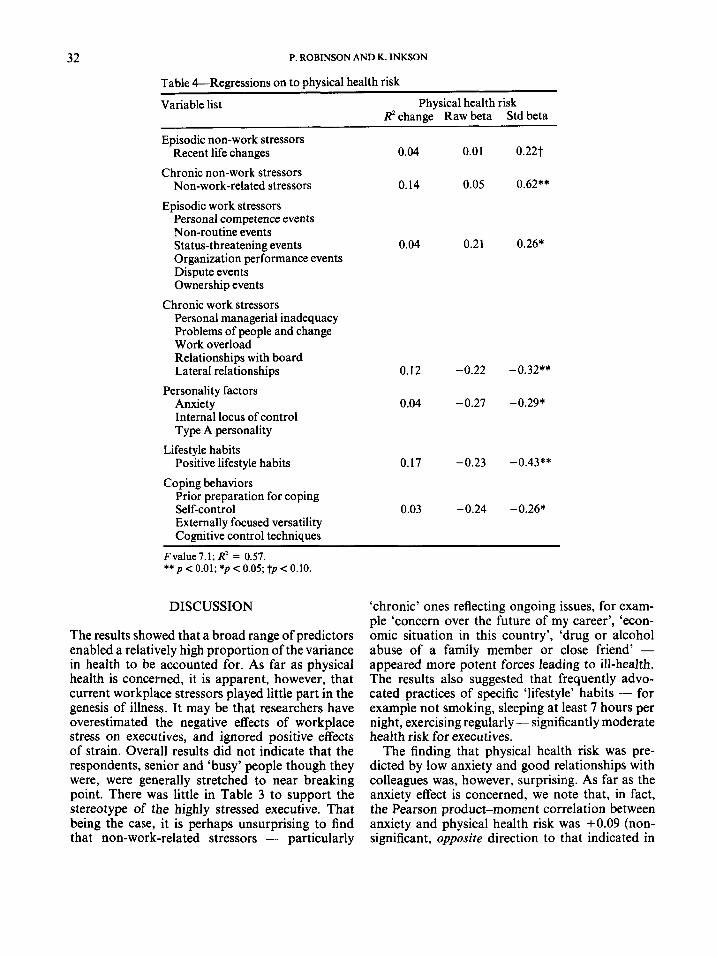
Regression analysis results are shown in Table 4. The optimum combination of measured indepen- dent variables accounted for 57 per cent of the vari- ance in physical health risk. The most striking findings were as follows: (1) each of the seven types of predictor variable (four stressor types, persona- lity, lifestyle habits, coping mechanisms) made a significant independent contribution to the regres- sion; (2) non-work-related stressors (both ‘chronic’ and ‘episodic’) accounted for marginally more (1 8 per cent vs 16 per cent) of the variance than did work-related stressors (however, other results sug- gested that work-related factors had a much more significant effect on mental health, as distinct from physical health, than did non-work-related fac- t o r ~ ; ’ ~ ’ ~ ~ (3) lateral relationships (chronic work- related stressor) and trait anxiety were significantly associated with health risk, in the reverse direction to that predicted by previous research, that is, in this study, those with better lateral relationships and lower levels of anxiety had generally higher health risk; (4) positive lifestyle habits contributed substantiaIIy to the avoidance of health risk.
32 P. ROBINSON AND K. INKSON
Table &Regressions on to physical health risk Variable list Physical health risk
R2 change Raw beta Std beta
Episodic non-work stressors Recent life changes
Chronic non-work stressors Non-work-related stressors
Episodic work stressors Personal competence events Non-routine events Status-threatening events
0.04 0.01 0.22t
0.14 0.05 0.62**
0.04 0.21 0.26* Organization performance events Dispute events Ownership events
Chronic work stressors Personal managerial inadequacy Problems of people and change Work overload Relationships with board Lateral relationships 0.12 -0.22 -0.32**
Personality factors Anxiety Internal locus of control Type A personality
Positive lifestyle habits Lifestyle habits
0.04 -0.27 -0.29*
- 0.17 .0.23 -0.43**
Coping behaviors Prior preparation for coping
Externally focused versatility Cognitive control techniques
Self-control 0.03 -0.24 -0.26*
Fvalue7.1; R2 = 0.57. ** p < 0.01; *p < 0.05; t p < 0.10.
DISCUSSION
The results showed that a broad range of predictors enabled a relatively high proportion of the variance in health to be accounted for. As far as physical health is concerned, it is apparent, however, that current workplace stressors played little part in the genesis of illness. It may be that researchers have overestimated the negative effects of workplace stress on executives, and ignored positive effects of strain. Overall results did not indicate that the respondents, senior and ‘busy’ people though they were, were generally stretched to near breaking point. There was little in Table 3 to support the stereotype of the highly stressed executive. That being the case, it is perhaps unsurprising to find that non-work-related stressors - particularly
‘chronic’ ones reflecting ongoing issues, for exam- ple ‘concern over the future of my career’, ‘econ- omic situation in this country’, ‘drug or alcohol abuse of a family member or close friend’ - appeared more potent forces leading to ill-health. The results also suggested that frequently advo- cated practices of specific ‘lifestyle’ habits - for example not smoking, sleeping at least 7 hours per night, exercising regularly - significantly moderate health risk for executives.
The finding that physical health risk was pre- dicted by low anxiety and good relationships with colleagues was, however, surprising. As far as the anxiety effect is concerned, we note that, in fact, the Pearson product-moment correlation between anxiety and physical health risk was +0.09 (non- significant, opposite direction to that indicated in
STRESS AND BUSINESS EXECUTIVES 33
the regression analysis). It is possible that the find- ing is a statistical artefact caused by the association between anxiety and other predictors which had priority over it in the regression analysis; for exam- ple, there is a correlation of -0.23 between anxiety and lifestyle habits.
Physical health risk appeared to be significantly reduced by the practice of healthy lifestyle habits. The correlation between lifestyle habits and physi- cal health risk was -0.42 @ < 0.001). The study provided confirmation of the benefits of healthy lifestyle practices for executives.
Generally, this study indicated the ability of a wide range of factors representing the social and occupational milieu of chief executives to predict their physical health. Despite factors such as age, social background and family health not being used as predictors, the amount of variance accounted for by social and occupational factors was high.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Ostfeld, A. M. and Eaker, E. D. (Eds) Measuring Psychosocial Variables in Epidemiological Studies of Cardiovascular Disease. NIH publication No. 85- 2270, US Department of Health and Human Ser- vices, 1985. Irwin, J. and Livnat, S. Behavioral influences on the immune system: Stress and conditioning. Prog. Neur- opharmacol. Biol. Psychiat. 1987; 11: 137-143. Cooper, C. L. (Ed.) Psychosocial Stress and Cancer. Wiley, Chichester, 1984. Rabkin, J. G. and Struening, E. L. Life events, stress, and illness. Science 1986; 194: 102&1031. Payne, R., Lane, D. and Leahy, M. Work and non- work as perceived causes of symptoms of psychologi- cal strain. Work Stress 1989; 3(4): 347-351. Brown, J. M. and Campbell, E. A. Sources of occu- pational stress in the police. Work Stress 1990; 4(4):
Cooper, C. L. and Payne, R. (Eds) Personality and Stress: Individual Dixerences in the Stress Process Wiley, Chichester, 1991. Jex, S. M., Spector, P. E., Gudanowski, D. M. and Newman, R. A. Relations between exercise and employee responses to work stressors: A summary of two studies. J. SOC. Behav. Personal. 1991; 6(7): 425-443. Bhagat, R. S., Allie, S. M. and Ford, D. L. Organiza- tional stress, personal life stress, and symptoms of life strains: An enquiry into the moderating role of styles of coping. J. SOC. Behav. Personal. 1991; 6:
Fletcher, B. C. The epidemiology of occupational
305-3 18.
163-184.
stress. In: Causes, Coping, and Consequences of Stress at Work. (Cooper, C. L. and Payne, R. (Eds) Wiley, Chichester, 1988.
11. Glowinowski, S. P. and Cooper, C. L. Organizatio- nal issues in stress research. J. Manager. Psychol.
12. Karasek, R. A. Job decision, job latitude and mental strain: Implications for job design. Admin. Sci. Quart. 1979; 24: 285-308.
13. Robinson P. CHESS: Chief executive stress survival: A study of occupational stress in New Zealand top management. Doctoral Thesis, University of Auck- land, New Zealand, 1991.
14. Spicer, J., McLeod, K. P., O’Brien, K. P. and Scott, P. J. Psychosomatic patterns of coronary risk in a community sample of New Zealand men. J. Chron. Disord. 1981; 34: 271-284.
15. Holmes, T. H. and Rahe, R. H. The social readjust- ment rating scale. J. Psychosom. Res. 1967; 11: 213- 218.
16. Adams, J. S. Understanding and Managing Stress: A Workbook on Changing Lifestyles. University Associates, San Diego, CA, 1980.
17. Payne, R. L. Individual differences in the study of occupational stress. In: Causes, Coping, and Conse- quences of Stress at Work. Cooper, C. L. and Payne, R. (Eds) Wiley, Chichester, 1988.
18. Cattell, R. B., Eber, H. W. and Tatsuko, M. M. Handbook for the 16PF. Institute for Testing and Personality, 1970.
19. Krause, N. and Stryker, S. Stress and well-being: The buffering role of locus of control beliefs. SOC. Sci. Med. 1984; 18: 783-790.
20. James, W. H. Internal versus external control of rein- forcement as a basis variable in learning theory. Unpublished dissertation, Ohio State University, 1957.
21. Friedman, M. and Rosenman, R. ‘Type A’ Behavior and Your Heart. Knopf, New York, 1974.
22. Bortner, R. W. and Rosenman, R. H. The measure- ment of Pattern A behavior. J. Chron. Dis. 1967;
23. Belloc, N. and Breslow, L. (1972) Relationship of physical health status and health practices. Prev. Med. 1972; 1: 409-421.
24. Latack, J. C. Coping with job stress: Measures and future directions for scale development. J. Appl. Psy-
25. Lazarus, R. and Folkman, S. Stress, Appraisal, and Coping. Springer, New York, 1984.
26. Moos, R. and Billings, A. Conceptualising and mea- suring coping resources and processes. In Handbook of Stress: Theoretical and Clinical Aspects. Gold- berger, L. and Breznitz, S. (Eds) Free Press, New York, 1982.
27. Cooper, C. L. and Melhuish, A. Occupational stress and the manager. J. Occup. Med. 1980; 22(9): 582- 592.
1987 l(1): 3-11.
2 0 525-533.
chol. 1986; 71(3): 377-385.

34 P. ROBINSON AND K. INKSON
28. Kerlinger, F. N. and Pedhazer, E. Multiple Regres- sion in Behavior Research. Holt, Rinehart and Win- ston, New York, 1973.
29. Robinson, P. and Inkson, K. A study of stress and health in Chief Executives in New Zealand. NZ J. Bus. 1993; 14 (in press).