Embed Size (px)
Citation preview
Jalali et al. Cost Eff Resour Alloc (2021) 19:47 https://doi.org/10.1186/s12962-021-00301-8
REVIEW
Strategies for reducing out of pocket payments in the health system: a scoping reviewFaride Sadat Jalali1, Parisa Bikineh1 and Sajad Delavari2*
Abstract
Background: Direct out-of-pocket payments (OOP) are among the most important financing mechanisms in many health systems, especially in developing countries, adversely affecting equality and leading vulnerable groups to pov-erty. Therefore, this scoping review study was conducted to identify the strategies involving OOP reduction in health systems.
Methods: Articles published in English on strategies related to out-of-pocket payments were Searched and retrieved in the Web of Science, Scopus, PubMed, and Embase databases between January 2000 and November 2020, follow-ing PRISMA guidelines. As a result, 3710 papers were retrieved initially, and 40 were selected for full-text assessment.
Results: Out of 40 papers included, 22 (55%) and 18 (45%) of the study were conducted in developing and devel-oped countries, respectively. The strategies were divided into four categories based on health system functions: health system stewardship, creating resources, health financing mechanisms, and delivering health services.As well, developing and developed countries applied different types of strategies to reduce OOP.
Conclusion: The present review identified some strategies that affect the OOP payments According to the health system functions framework. Considering the importance of stewardship, creating resources, the health financing mechanisms, and delivering health services in reducing OOP, this study could help policymakers make better deci-sions for reducing OOP expenditures.
Keywords: OOP, Out of pocket, Health policy, Health system, Financing, Scoping review
© The Author(s) 2021. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/. The Creative Commons Public Domain Dedication waiver (http:// creat iveco mmons. org/ publi cdoma in/ zero/1. 0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
IntroductionNowadays, spending on health is rising, accounting for 10% of global gross domestic product (GDP). Govern-ment expenditures, out-of-pocket payments (OOPs), and sources like voluntary health insurance, employer-pro-vided health programs, and activities by non-governmen-tal organizations are all included in health spending [1].
As defined by the World Health Organization (WHO), OOP expenses are the individuals’ direct payments to healthcare providers at the time of service use [2]. OOPs, include purely private transactions (payments made by individuals to private doctors and pharmacies), offi-cial patient cost-sharing (user fees/copayments) within defined public or private benefit packages, and informal payments (payments beyond the prescriptions entitled as benefits, both in cash and in-kind). Therefore, OOPs may be explicitly some part of a policy or can occur through market transactions, or both [3].
OOP health expenditures may increase whenever households opt to access and receive health services but are not protected against high payments since medical
Open Access
Cost Effectiveness and Resource Allocation
*Correspondence: [email protected] Health Human Resources Research Center, School of Health Management and Information Sciences, Shiraz University of Medical Sciences, Shiraz, IranFull list of author information is available at the end of the article

Page 2 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
costs are high. They do not have access to insurance coverage and other safeguards against OOPs [4]. The following factors significantly affect OOP health care costs: increased patient cost-sharing, development of high-deductible health care plans, and more use of costly biologic or designer drugs. OOP payments are not an efficient way of financing health care and may negatively affect equity and cause vulnerable groups to experience poverty [5]. High OOP medical costs can use up financial savings and damage credits and have a negative impact on the quality of life, medication adherence, and different health outcomes [6].
A new report by the World Bank Group stated that OOP payments accounted for a non-negligible part of total health care expenditures in Central and Eastern European countries. Also, Patients in developing coun-tries spent half a trillion dollars each year (over $80 per person) out of their own pockets to receive health ser-vices [7]. Unfortunately, such expenses significantly harmed the poor [8]. The more the health sector grew, the less reliant it would be on OOP spending. The total OOP spending increased at least twice as much in low- and middle-income countries during 2000–2017 and reached 46% in high-income ones. However, its growth was slower than that of public spending in all income groups [9]. According to Adam Wagstaf (2020), OOP expenditures changed significantly within income groups, ranging from $32 in Sweden to $1200 in Switzer-land in the high-income groups, and from six dollars in Madagascar to $100 in Cambodia, Haiti, and Nepal in the low-income ones [10].
There have been health financing policy reforms and measures in several countries recently to deal with the concerns over high OOP payments. While there is no remedy, available information suggests that having well-designed policies and strategies can help countries reduce OOP and its adverse effects successfully [2, 11]. In general, reforms can apply some key strategies to abol-ish user fees or charges in public health facilities and exempt specific community groups such as the poor and
the vulnerable, and pregnant women and children from official payments. They should also exempt some health services such as maternal and child care from official payments and deliver them free of charge [12].
Due to the lack of resources, implementing effective policies can protect households against the common and high costs of the health system. To date, no known study has reviewed the proposed appreciate strategies for reducing OOP health payments worldwide. So, the pre-sent study aims to investigate strategies of reducing OOP payments in the health system through scoping review studies between 2000 and 2020. This review can help decision-makers learn from the effective experiences of other countries in reducing OOP health payments.
Materials and methodsThis study was carried out based on the Joanna Briggs Institute scoping review method as a framework [13], and a comprehensive systematic scoping review was per-formed to explain the strategies that could effectively reduce OOP health expenditures around the world. A defined question based on the PCC (Population, Con-cept, and Context) elements was raised at the first stage. All the countries in the world (Population), strategies and policies that affected OOP health expenditures (Concept), and all health systems having OOP payments (Context) were included in the question.
The second stage dealt with the target population, which comprised all the studies related to “Out-of-Pocket Expenditures” in various countries. To this end, all related studies conducted since 2000 were retrieved through the research strategy (Table 1).
Thus, the original English keywords appropriate to the research objective were first selected based on the com-ments of the research team and the keywords used in available related studies. Then, PubMed, Scopus, ISI Web of Science, and Embase databases were searched. It was decided to identify all the articles with at least an English abstract indexed in one database.
Table 1 The search strategy of the research
Search strategy
Databases: PubMed, Scopus, ISI Web of Science, Embase (2000–2020)
Limits: Language (resources in English) and date (published after 2000)
Date: up to November 25, 2020
Strategy: #1 AND #2 in title and abstract
#1 “Out-of-Pocket Expenditure” OR “Out-of-Pocket Payment” OR “Out-of-Pocket Cost” OR “Out-of-Pocket Spending” OR “Out-of-pocket health spending” OR “Out of Pocket Expenditures” OR “Out-of-Pocket Expenses” OR “OOP” OR “Out of pocket”
#2 Strategy OR intervention OR policy
Page 3 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
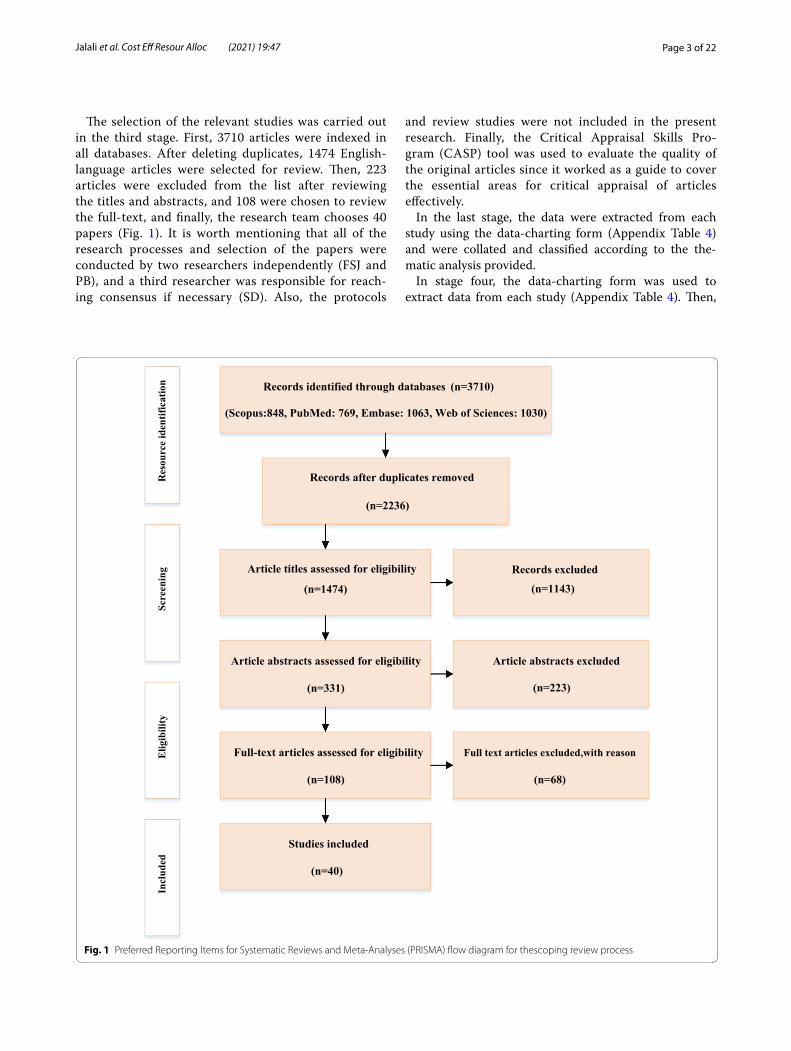
The selection of the relevant studies was carried out in the third stage. First, 3710 articles were indexed in all databases. After deleting duplicates, 1474 English-language articles were selected for review. Then, 223 articles were excluded from the list after reviewing the titles and abstracts, and 108 were chosen to review the full-text, and finally, the research team chooses 40 papers (Fig. 1). It is worth mentioning that all of the research processes and selection of the papers were conducted by two researchers independently (FSJ and PB), and a third researcher was responsible for reach-ing consensus if necessary (SD). Also, the protocols
and review studies were not included in the present research. Finally, the Critical Appraisal Skills Pro-gram (CASP) tool was used to evaluate the quality of the original articles since it worked as a guide to cover the essential areas for critical appraisal of articles effectively.
In the last stage, the data were extracted from each study using the data-charting form (Appendix Table 4) and were collated and classified according to the the-matic analysis provided.
In stage four, the data-charting form was used to extract data from each study (Appendix Table 4). Then,
Records identified through databases (n=3710)
(Scopus:848, PubMed: 769, Embase: 1063, Web of Sciences: 1030)
Records after duplicates removed
(n=2236)
Article titles assessed for eligibility
(n=1474)
Article abstracts assessed for eligibility
(n=331)
Full-text articles assessed for eligibility
(n=108)
Records excluded
(n=1143)
Article abstracts excluded
(n=223)
Full text articles excluded,with reason
(n=68)
Studies included
(n=40)
Res
ourc
e id
entif
icat
ion
Scre
enin
gE
ligib
ility
Incl
uded
Fig. 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for thescoping review process
Page 4 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
the collected data were collated and classified according to the thematic analysis in the last stage.
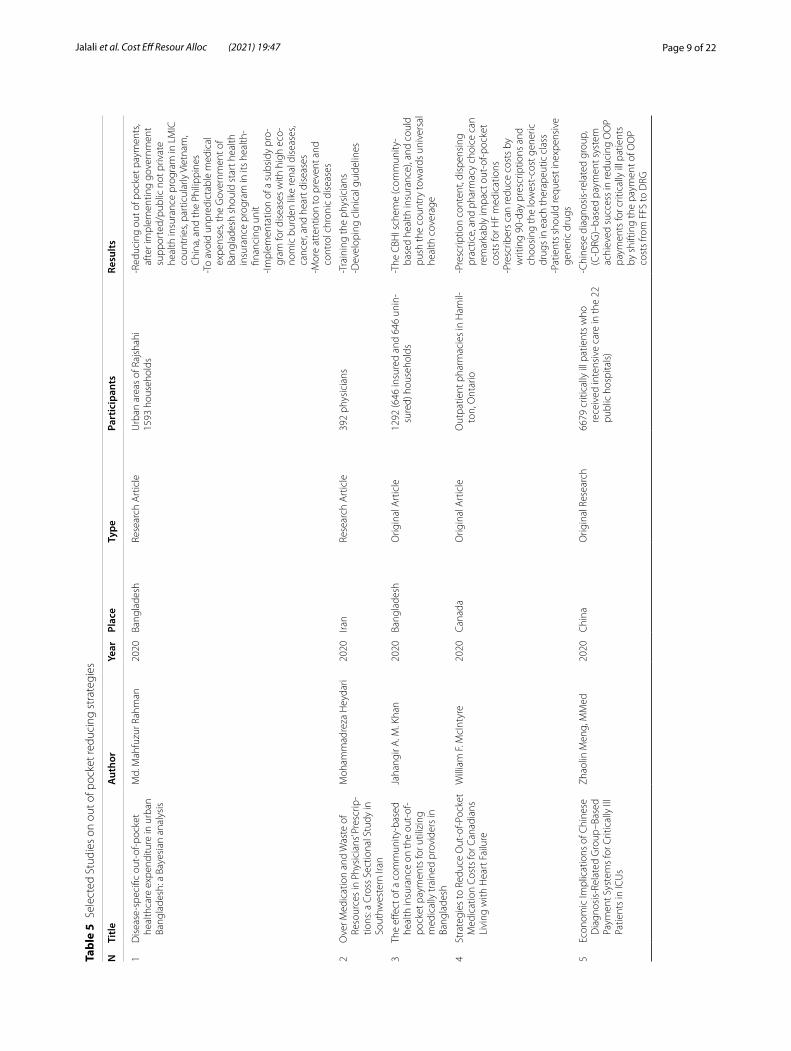
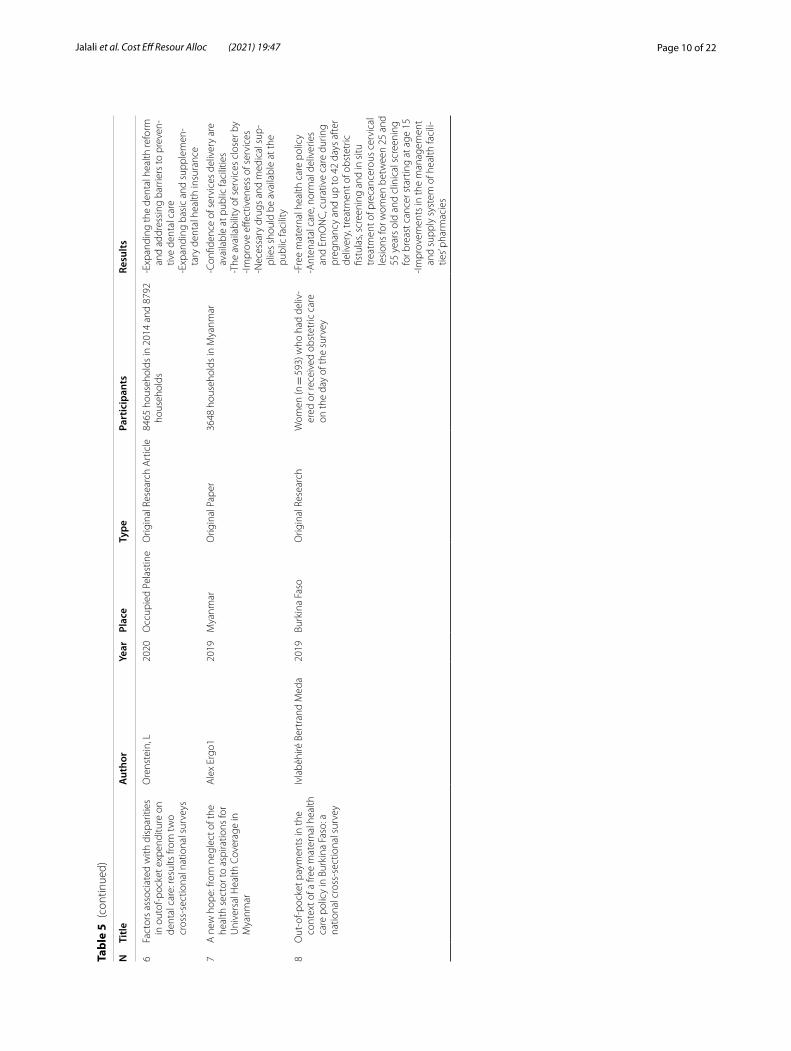
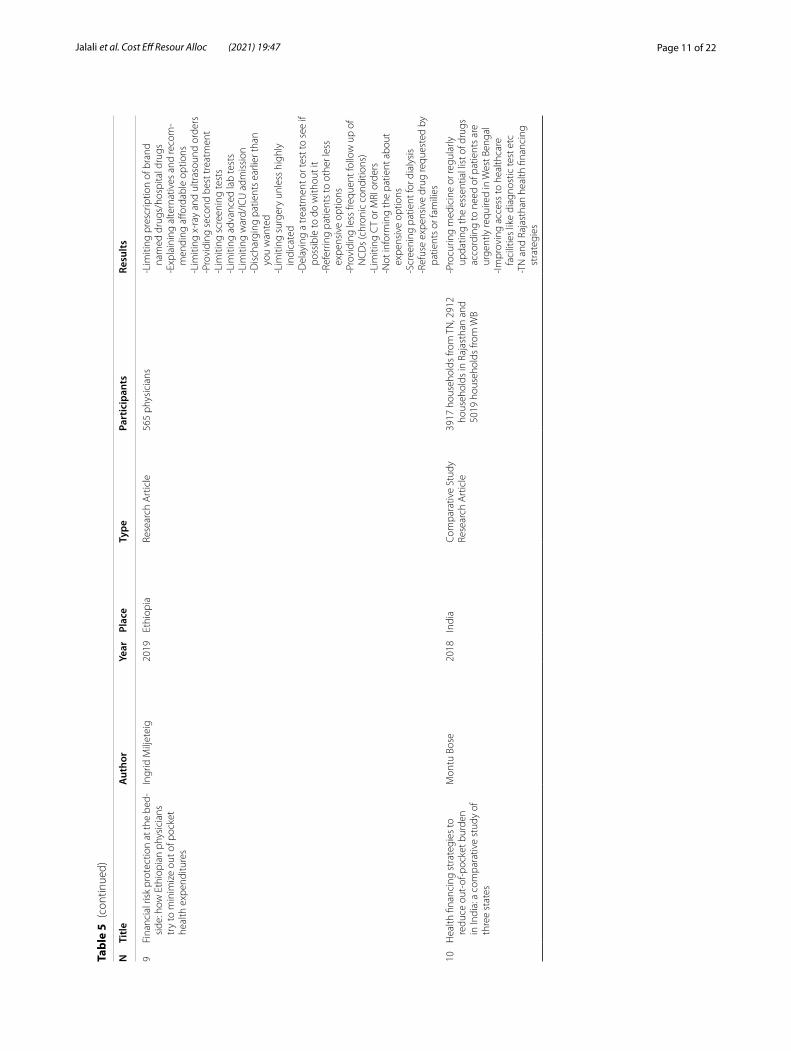
ResultsThe findings resulted from the analysis of 40 studies were summarized in Appendix Table 5. Among these studies, 20 (50%), 13 (32.5%), four (10%), and three (7.5%) stud-ies belonged to Asian, American, European, and African countries, respectively. Furthermore, 22 (55%) and 18 (45%) belonged to developing and developed countries.
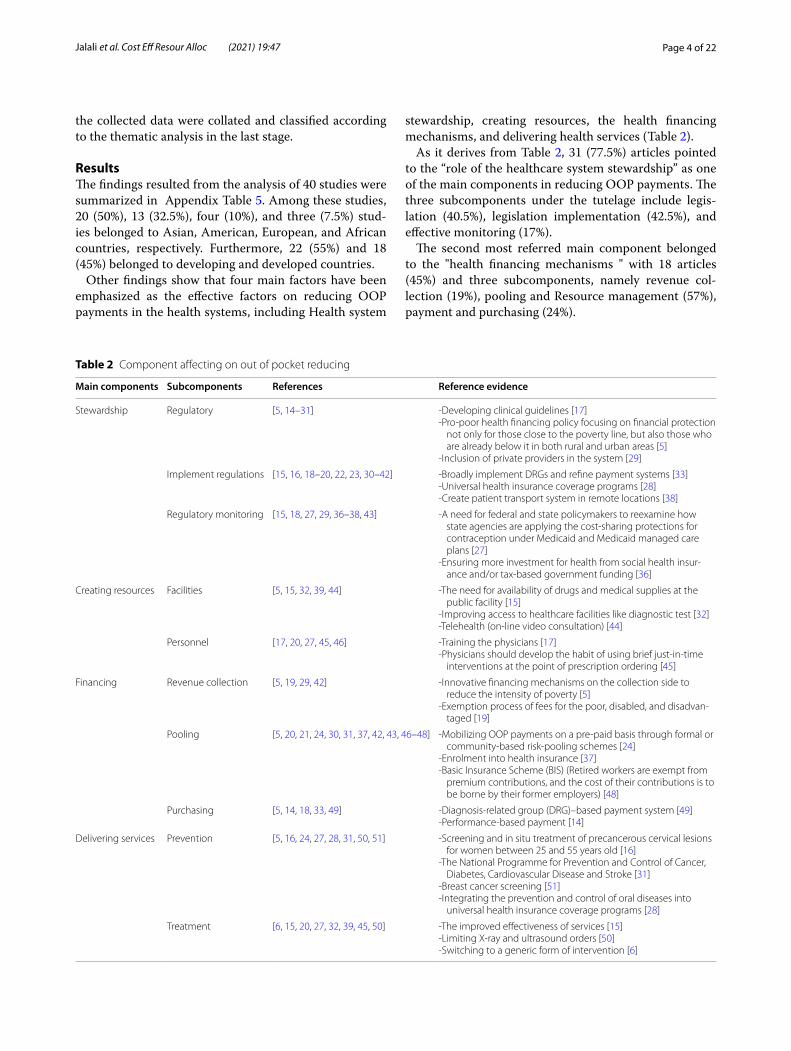
Other findings show that four main factors have been emphasized as the effective factors on reducing OOP payments in the health systems, including Health system
stewardship, creating resources, the health financing mechanisms, and delivering health services (Table 2).
As it derives from Table 2, 31 (77.5%) articles pointed to the “role of the healthcare system stewardship” as one of the main components in reducing OOP payments. The three subcomponents under the tutelage include legis-lation (40.5%), legislation implementation (42.5%), and effective monitoring (17%).
The second most referred main component belonged to the "health financing mechanisms " with 18 articles (45%) and three subcomponents, namely revenue col-lection (19%), pooling and Resource management (57%), payment and purchasing (24%).
Table 2 Component affecting on out of pocket reducing
Main components Subcomponents References Reference evidence
Stewardship Regulatory [5, 14–31] -Developing clinical guidelines [17]-Pro-poor health financing policy focusing on financial protection
not only for those close to the poverty line, but also those who are already below it in both rural and urban areas [5]
-Inclusion of private providers in the system [29]
Implement regulations [15, 16, 18–20, 22, 23, 30–42] -Broadly implement DRGs and refine payment systems [33]-Universal health insurance coverage programs [28]-Create patient transport system in remote locations [38]
Regulatory monitoring [15, 18, 27, 29, 36–38, 43] -A need for federal and state policymakers to reexamine how state agencies are applying the cost-sharing protections for contraception under Medicaid and Medicaid managed care plans [27]
-Ensuring more investment for health from social health insur-ance and/or tax-based government funding [36]
Creating resources Facilities [5, 15, 32, 39, 44] -The need for availability of drugs and medical supplies at the public facility [15]
-Improving access to healthcare facilities like diagnostic test [32]-Telehealth (on-line video consultation) [44]
Personnel [17, 20, 27, 45, 46] -Training the physicians [17]-Physicians should develop the habit of using brief just-in-time
interventions at the point of prescription ordering [45]
Financing Revenue collection [5, 19, 29, 42] -Innovative financing mechanisms on the collection side to reduce the intensity of poverty [5]
-Exemption process of fees for the poor, disabled, and disadvan-taged [19]
Pooling [5, 20, 21, 24, 30, 31, 37, 42, 43, 46–48] -Mobilizing OOP payments on a pre-paid basis through formal or community-based risk-pooling schemes [24]
-Enrolment into health insurance [37]-Basic Insurance Scheme (BIS) (Retired workers are exempt from
premium contributions, and the cost of their contributions is to be borne by their former employers) [48]
Purchasing [5, 14, 18, 33, 49] -Diagnosis-related group (DRG)–based payment system [49]-Performance-based payment [14]
Delivering services Prevention [5, 16, 24, 27, 28, 31, 50, 51] -Screening and in situ treatment of precancerous cervical lesions for women between 25 and 55 years old [16]
-The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke [31]
-Breast cancer screening [51]-Integrating the prevention and control of oral diseases into
universal health insurance coverage programs [28]
Treatment [6, 15, 20, 27, 32, 39, 45, 50] -The improved effectiveness of services [15]-Limiting X-ray and ultrasound orders [50]-Switching to a generic form of intervention [6]

Page 5 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
The number of article on “delivering health services” were 15 (37.5%). It has two sub-components of preven-tive services (50%), and treatment (50%) have been con-sidered as one of the main components affecting the reduction of OOP payments in health systems.
“Creating Resource” with ten articles (25%) and two sub-components, namely the physical resources (50%), human capital investment, and training (50%), also have the least referred in the articles.
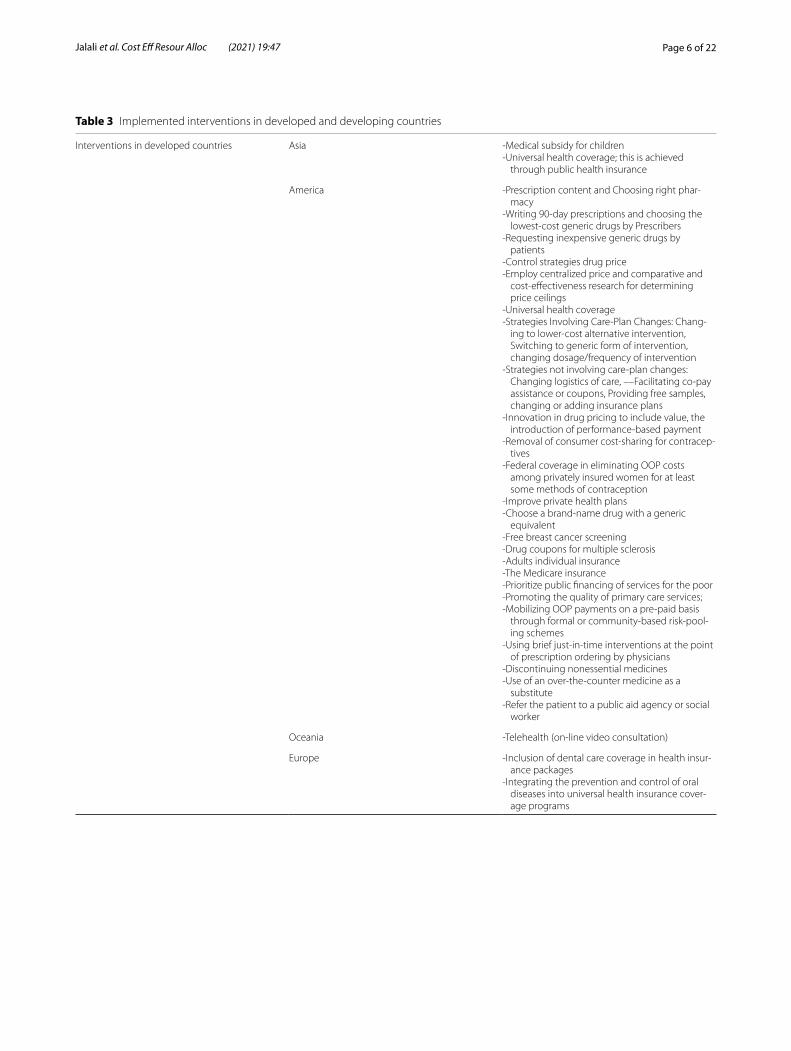
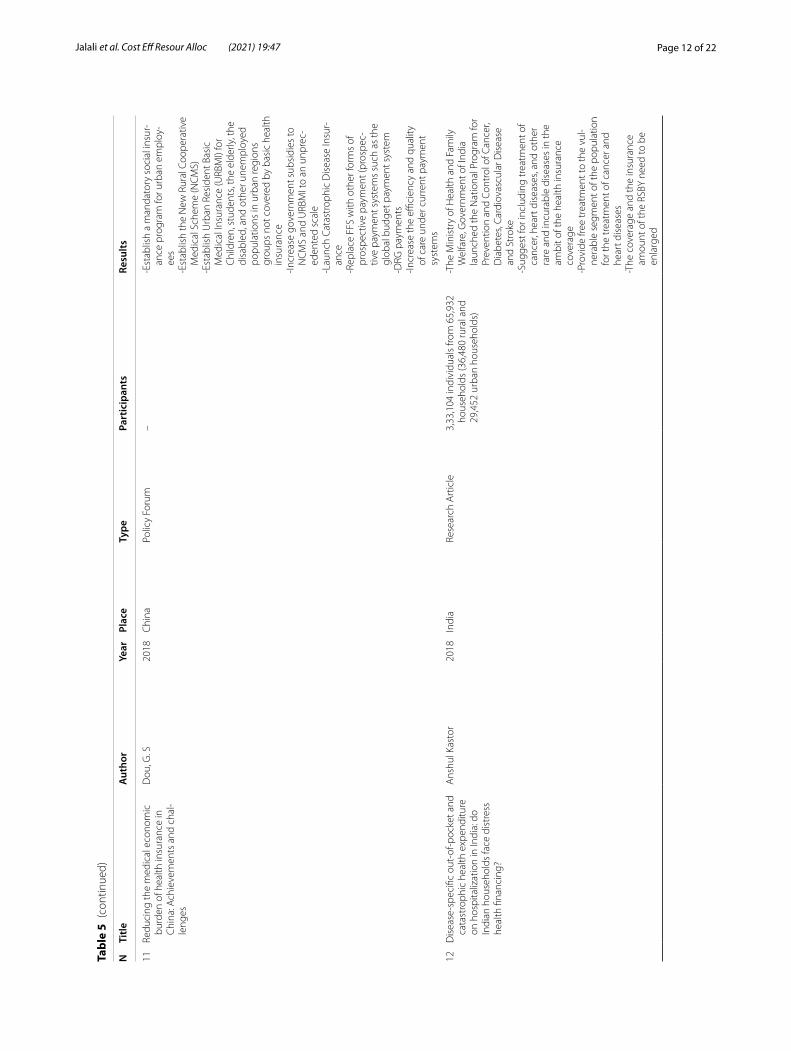
As Table 3 shows, developed and developing countries have implemented various strategies to reduce OOP. Developed Asian countries have applied medical sub-sidy, universal health coverage, Choosing the right phar-macy, requesting inexpensive generic drugs by patients, the inclusion of dental care coverage in health insurance packages, control strategies drug price, performance-based payment, eliminating OOP costs for methods of contraception, choose a brand-name drug with a generic equivalent, free screening, drug coupons, promoting the quality of primary care services, ordering by physicians and telehealth as effective strategies in reducing OOP payments. Government support of public health insur-ance program, subsidy program for diseases with high economic burden, prevent and control chronic diseases, training the physicians, developing clinical guidelines, universal health coverage, diagnosis-related group (DRG) based payment system, expanding the dental health reform, providing care closer to home, Insurance for chil-dren, students, the elderly, the disabled, and other unem-ployed populations in urban regions groups not covered by basic health insurance catastrophic disease insurance, increase the efficiency and quality of care, free treat-ment to the vulnerable segment of the population, clear the system from informal payment, -innovative financ-ing mechanisms on the collection, pooling and purchas-ing side, free gynecologic screening and discharging patients earlier are some strategies that Asian developing countries such as Iran, India, China, Bangladesh and the Philippines and African countries such as Ethiopia and Ghana have implemented to reduce their OOP payments.
DiscussionOverall, the results showed that four main components—health system stewardship, financing mechanisms, ser-vice delivery, and creating resources—have been effective in reducing OOP payments in health systems of different countries. This category is similar to the functions intro-duced by the WHO report in 2000 [52].
Legislation, legislation implementation, and effective monitoring are considered as proposed subcomponents of the stewardship. The results of many studies have shown that health care governance around the world can reduce household health expenditures by legislation. For
example, Rahman et al. (2020), in their research in Bang-ladesh, stated that health care governance, strengthen-ing the rules and regulations related to care subsidies by public health centers, counseling and planning clin-ics for parents, and Community-based health centers for low-income consumers and patients with high eco-nomic burden can play an important role in reducing OOP healthcare costs [31]. Sarnak et al. (2017) cited federal government negotiations and legislation on the announcement of centralized prices. They approved drug ceiling rates in the United States as one factor in reducing OOP payments [22].
Ensuring implementation and monitoring the correct-ness of the laws by health system governance can also help reduce OOP payments. Several studies have iden-tified the implementation of laws and programs related to global health care coverage as a way to protect house-holds from these expenditures [22, 23, 28, 35, 36].
Control on the efficiency and quality of care and pay-ment systems [18], Careful monitoring to clear the informal payments [29, 37] and ensuring the supply and availability of essential medicines [38] is also helpful in this regard.
According to the present study results, by investing in human capital investment and training and physical facil-ities, OOP payments can also be reduced. Providing the infrastructure for online video consultation in Australia [44], improving access to health facilities in India [32], physicians’ training on various fields in Iran [17] and the United States [45], had been reported as effective strate-gies in reducing OOP.
On the other hand, the lack of financial protection has been recognized as a health system disease. OOP pay-ments are one of the major financing mechanisms in many developing countries and put the poor’s greatest pressure. Adequate financing and its functions, includ-ing revenue collection, risk pooling and purchasing, are introduced as the most important mechanisms in reduc-ing the share of direct OOP payment [53]. For example, Aryeetey et al. (2016), in their study in Ghana, stated that enrolment into health insurance would reduce OOP pay-ments by 80% [37].
Several studies have also expanded the intensity and health insurance coverage for dental services [21]، rare and incurable diseases treatment [31], and mentioned the support for vulnerable groups as effective factors in this regard [42]. A study in India found that using new meth-ods of health financing to collect, pooling and purchasing would reduce the severity of poverty and OOP payments [5], including pay for performances [14] and diagnosis-related groups (DRGs) payments [18, 33, 49].
Also in this research, the provision of prevention and treatment services have been included as two
Page 6 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Table 3 Implemented interventions in developed and developing countries
Interventions in developed countries Asia -Medical subsidy for children-Universal health coverage; this is achieved
through public health insurance
America -Prescription content and Choosing right phar-macy
-Writing 90-day prescriptions and choosing the lowest-cost generic drugs by Prescribers
-Requesting inexpensive generic drugs by patients
-Control strategies drug price-Employ centralized price and comparative and
cost-effectiveness research for determining price ceilings
-Universal health coverage-Strategies Involving Care-Plan Changes: Chang-
ing to lower-cost alternative intervention, Switching to generic form of intervention, changing dosage/frequency of intervention
-Strategies not involving care-plan changes: Changing logistics of care, ––Facilitating co-pay assistance or coupons, Providing free samples, changing or adding insurance plans
-Innovation in drug pricing to include value, the introduction of performance-based payment
-Removal of consumer cost-sharing for contracep-tives
-Federal coverage in eliminating OOP costs among privately insured women for at least some methods of contraception
-Improve private health plans-Choose a brand-name drug with a generic
equivalent-Free breast cancer screening-Drug coupons for multiple sclerosis-Adults individual insurance-The Medicare insurance-Prioritize public financing of services for the poor-Promoting the quality of primary care services;-Mobilizing OOP payments on a pre-paid basis
through formal or community-based risk-pool-ing schemes
-Using brief just-in-time interventions at the point of prescription ordering by physicians
-Discontinuing nonessential medicines-Use of an over-the-counter medicine as a
substitute-Refer the patient to a public aid agency or social
worker
Oceania -Telehealth (on-line video consultation)
Europe -Inclusion of dental care coverage in health insur-ance packages
-Integrating the prevention and control of oral diseases into universal health insurance cover-age programs

Page 7 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
sub-components of providing health services. Some stud-ies have shown that taking precautionary measures can prevent many OOP payments in the future. Meda et al. (2019) stated that the implementation of screening pro-grams for gynecological diseases in reproductive age would prevent cancer in later years and thus will lead to individual financial protection [16].
The results of a study by Kastor et al. Showed that launching national prevent and control cancer, diabetes, cardiovascular disease, and stroke programs in India sig-nificantly reduces OOP payment [31].
It is worth mentioning that the studies obtained from the present study showed that in addition to preventive services, the providers’ behaviors and actions are also effective in reducing OOP payments. physicians can
Table 3 (continued)
Interventions in developing countries Asia -Government support of public health insurance program
-Subsidy program for diseases with a high eco-nomic burden
-Prevent and control chronic diseases-Training the physicians-Developing clinical guidelines-Universal health coverage-Diagnosis-related group (DRG)–based payment
system-Expanding the dental health reform-Providing care closer to home-Improve the effectiveness of services-Regularly updating the essential list of drugs
according to need of patients-Mandatory social insurance program for urban
employees-Insurance for children, students, the elderly, the
disabled, and other unemployed populations in urban regions groups not covered by basic health insurance
-Catastrophic Disease Insurance-Increase the efficiency and quality of care-National Program for Prevention and Control of
Cancer, Diabetes, Cardiovascular Disease, and Stroke
-Free treatment to the vulnerable segment of the population for the treatment of cancer and heart diseases
-Create patient transport system in remote loca-tions
-Fees exemption for the poor, disabled, and disadvantaged
-Public and private insurance-More investment for health from social health
insurance and tax-based government funding-Inclusion of private providers in the system-Decrease and even eliminate the copayments for
those at low-income levels-Clear the system from informal payments-Innovative financing mechanisms on the collec-
tion, pooling, and purchasing side
Africa -Free maternal health care policy-Screening and in situ treatment of precancerous
cervical lesions for women between 25 and 55 years old and clinical screening for breast cancer at age 15
-Limiting prescription of brand-name drugs, x-ray and ultrasound orders, screening tests, advanced lab tests, ward/ICU admission, surgery
-Discharging patients earlier-Refuse expensive drug requested by patients or
families-Reducing informal fees

Page 8 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
replace generic drugs with brand drugs in their prescrip-tions [20, 39, 45] Limiting diagnostic-therapeutic tests and surgeries and preventing unnecessary admissions in special intensive care wards and alternative interven-tions, discharge patients quickly [50] And improve the quality and effectiveness of services [15, 18], play an effective role in reducing OOP payments.
Also, as this study shows, employing cost-effective-ness research for determining price ceilings, dental care coverage in health insurance packages, control strate-gies drug price, and on-line video consultation are some strategies implemented in developed countries. But developing countries have implemented strategies, such as government support of public health insurance programs, subsidy programs for diseases with high economic burdens, training the physicians, eliminate informal payments, and discharging patients earlier. Strategies such as free screening programs, universal health coverage, pay for performance, promoting the quality of care services and replacing the brand drug with generic have been common in both developed and developing countries. The reason for these differences can be sought in factors such as the medical capacity of countries, per capita government funding, differ-ent patterns of disease, the governing system, and the health financing system. A study in Iran cited economic factors, policy factors, social support organizations, insurance, cost of health services, tariffs, health services organizations, providers and consumers’ behaviors, and epidemiological conditions as factors influencing OOP health payments [54].
It should be noted that this study by a research team has reviewed articles related to effective solutions to reduce OOP payments in the health systems of different countries. The search strategy consisted of four electronic databases, and two independent researchers evaluated each article.
This study faces several limitations including limitations related to databases and search strategies by researchers. As well the suggested strategies were not surveyed regard-ing to effectiveness or cost. Therefore, more studies are needed to check the cost and effectiveness of suggested strategies for reducing OOP.
ConclusionOne of the most important characteristics of successful countries in providing maximum health for their commu-nities is the rationality of the financing method and maxi-mizing the share of the public sector in the share of OOP payments in health services so that people feel comfortable when the disease occurs. In case of disability and poverty, do not give up health services.
The present review identified the importance of each health system’s functions that affect the reduction of OOP payments. Given that OOP payments are the worst form of financing in any health system, the strategies proposed and successfully implemented worldwide must be con-sidered by policymakers when making future decisions to target health systems. Approach their goals, which include promoting health, increasing accountability, and equitable financial participation.
Appendix 1See Tables 4 and 5.
Table 4 A draft chart of data extraction
General information
Title of the manuscript
Article No Language
Year of the publication First author
Place (Country) Corresponding
Type of article Journal name
Article characteristics
Aims of the study
Study approach study design
Methodology
Sampling method study environment
Data collection study population
Data analysis sample size
Results
Main results
Conclusion
Recommendations
Limitations
Page 9 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
Sele
cted
Stu
dies
on
out o
f poc
ket r
educ
ing
stra
tegi
es
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
1D
isea
se-s
peci
fic o
ut-o
f-poc
ket
heal
thca
re e
xpen
ditu
re in
urb
an
Bang
lade
sh: a
Bay
esia
n an
alys
is
Md.
Mah
fuzu
r Rah
man
2020
Bang
lade
shRe
sear
ch A
rtic
leU
rban
are
as o
f Raj
shah
i15
93 h
ouse
hold
s-R
educ
ing
out o
f poc
ket p
aym
ents
, af
ter i
mpl
emen
ting
gove
rnm
ent
supp
orte
d/pu
blic
not
priv
ate
heal
th in
sura
nce
prog
ram
in L
MIC
co
untr
ies,
part
icul
arly
Vie
tnam
, C
hina
, and
the
Phili
ppin
es-T
o av
oid
unpr
edic
tabl
e m
edic
al
expe
nses
, the
Gov
ernm
ent o
f Ba
ngla
desh
sho
uld
star
t hea
lth
insu
ranc
e pr
ogra
m in
its
heal
th-
finan
cing
uni
t-Im
plem
enta
tion
of a
sub
sidy
pro
-gr
am fo
r dis
ease
s w
ith h
igh
eco-
nom
ic b
urde
n lik
e re
nal d
isea
ses,
canc
er, a
nd h
eart
dis
ease
s-M
ore
atte
ntio
n to
pre
vent
and
co
ntro
l chr
onic
dis
ease
s
2O
ver M
edic
atio
n an
d W
aste
of
Reso
urce
s in
Phy
sici
ans’
Pres
crip
-tio
ns: a
Cro
ss S
ectio
nal S
tudy
in
Sout
hwes
tern
Iran
Moh
amm
adre
za H
eyda
ri20
20Ira
nRe
sear
ch A
rtic
le39
2 ph
ysic
ians
-Tra
inin
g th
e ph
ysic
ians
-Dev
elop
ing
clin
ical
gui
delin
es
3Th
e eff
ect o
f a c
omm
unity
-bas
ed
heal
th in
sura
nce
on th
e ou
t-of
-po
cket
pay
men
ts fo
r util
izin
g m
edic
ally
trai
ned
prov
ider
s in
Ba
ngla
desh
Jaha
ngir
A. M
. Kha
n20
20Ba
ngla
desh
Orig
inal
Art
icle
1292
(646
insu
red
and
646
unin
-su
red)
hou
seho
lds
-The
CBH
I sch
eme
(com
mun
ity-
base
d he
alth
insu
ranc
e), a
nd c
ould
pu
sh th
e co
untr
y to
war
ds u
nive
rsal
he
alth
cov
erag
e
4St
rate
gies
to R
educ
e O
ut-o
f-Poc
ket
Med
icat
ion
Cost
s fo
r Can
adia
ns
Livi
ng w
ith H
eart
Fai
lure
Will
iam
F. M
cInt
yre
2020
Cana
daO
rigin
al A
rtic
leO
utpa
tient
pha
rmac
ies
in H
amil-
ton,
Ont
ario
-Pre
scrip
tion
cont
ent,
disp
ensi
ng
prac
tice,
and
pha
rmac
y ch
oice
can
re
mar
kabl
y im
pact
out
-of-p
ocke
t co
sts
for H
F m
edic
atio
ns-P
resc
riber
s ca
n re
duce
cos
ts b
y w
ritin
g 90
-day
pre
scrip
tions
and
ch
oosi
ng th
e lo
wes
t-co
st g
ener
ic
drug
s in
eac
h th
erap
eutic
cla
ss-P
atie
nts
shou
ld re
ques
t ine
xpen
sive
ge
neric
dru
gs
5Ec
onom
ic Im
plic
atio
ns o
f Chi
nese
D
iagn
osis
-Rel
ated
Gro
up–B
ased
Pa
ymen
t Sys
tem
s fo
r Crit
ical
ly Il
l Pa
tient
s in
ICU
s
Zhao
lin M
eng,
MM
ed20
20C
hina
Orig
inal
Res
earc
h66
79 c
ritic
ally
ill p
atie
nts
who
re
ceiv
ed in
tens
ive
care
in th
e 22
pu
blic
hos
pita
ls)
-Chi
nese
dia
gnos
is-r
elat
ed g
roup
, (C
-DRG
)–ba
sed
paym
ent s
yste
m
achi
eved
suc
cess
in re
duci
ng O
OP
paym
ents
for c
ritic
ally
ill p
atie
nts
by s
hift
ing
the
paym
ent o
f OO
P co
sts
from
FFS
to D
RG
Page 10 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
6Fa
ctor
s as
soci
ated
with
dis
parit
ies
in o
utof
-poc
ket e
xpen
ditu
re o
n de
ntal
car
e: re
sults
from
two
cros
s-se
ctio
nal n
atio
nal s
urve
ys
Ore
nste
in, L
2020
Occ
upie
d Pe
last
ine
Orig
inal
Res
earc
h A
rtic
le84
65 h
ouse
hold
s in
201
4 an
d 87
92
hous
ehol
ds-E
xpan
ding
the
dent
al h
ealth
refo
rm
and
addr
essi
ng b
arrie
rs to
pre
ven-
tive
dent
al c
are
-Exp
andi
ng b
asic
and
sup
plem
en-
tary
den
tal h
ealth
insu
ranc
e
7A
new
hop
e: fr
om n
egle
ct o
f the
he
alth
sec
tor t
o as
pira
tions
for
Uni
vers
al H
ealth
Cov
erag
e in
M
yanm
ar
Ale
x Er
go1
2019
Mya
nmar
Orig
inal
Pap
er36
48 h
ouse
hold
s in
Mya
nmar
-Con
fiden
ce o
f ser
vice
s de
liver
y ar
e av
aila
ble
at p
ublic
faci
litie
s-T
he a
vaila
bilit
y of
ser
vice
s cl
oser
by
-Impr
ove
effec
tiven
ess
of s
ervi
ces
-Nec
essa
ry d
rugs
and
med
ical
sup
-pl
ies
shou
ld b
e av
aila
ble
at th
e pu
blic
faci
lity
8O
ut-o
f-poc
ket p
aym
ents
in th
e co
ntex
t of a
free
mat
erna
l hea
lth
care
pol
icy
in B
urki
na F
aso:
a
natio
nal c
ross
-sec
tiona
l sur
vey
Ivla
bèhi
ré B
ertr
and
Med
a20
19Bu
rkin
a Fa
soO
rigin
al R
esea
rch
Wom
en (n
= 5
93) w
ho h
ad d
eliv
-er
ed o
r rec
eive
d ob
stet
ric c
are
on th
e da
y of
the
surv
ey
-Fre
e m
ater
nal h
ealth
car
e po
licy
-Ant
enat
al c
are,
nor
mal
del
iver
ies
and
EmO
NC
, cur
ativ
e ca
re d
urin
g pr
egna
ncy
and
up to
42
days
aft
er
deliv
ery,
trea
tmen
t of o
bste
tric
fis
tula
s, sc
reen
ing
and
in s
itu
trea
tmen
t of p
reca
ncer
ous
cerv
ical
le
sion
s fo
r wom
en b
etw
een
25 a
nd
55 y
ears
old
and
clin
ical
scr
eeni
ng
for b
reas
t can
cer s
tart
ing
at a
ge 1
5-Im
prov
emen
ts in
the
man
agem
ent
and
supp
ly s
yste
m o
f hea
lth fa
cili-
ties’
phar
mac
ies
Page 11 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
9Fi
nanc
ial r
isk
prot
ectio
n at
the
bed-
side
: how
Eth
iopi
an p
hysi
cian
s tr
y to
min
imiz
e ou
t of p
ocke
t he
alth
exp
endi
ture
s
Ingr
id M
iljet
eig
2019
Ethi
opia
Rese
arch
Art
icle
565
phys
icia
ns-L
imiti
ng p
resc
riptio
n of
bra
nd
nam
ed d
rugs
/hos
pita
l dru
gs-E
xpla
inin
g al
tern
ativ
es a
nd re
com
-m
endi
ng a
fford
able
opt
ions
-Lim
iting
x-r
ay a
nd u
ltras
ound
ord
ers
-Pro
vidi
ng s
econ
d be
st tr
eatm
ent
-Lim
iting
scr
eeni
ng te
sts
-Lim
iting
adv
ance
d la
b te
sts
-Lim
iting
war
d/IC
U a
dmis
sion
-Dis
char
ging
pat
ient
s ea
rlier
than
yo
u w
ante
d-L
imiti
ng s
urge
ry u
nles
s hi
ghly
in
dica
ted
-Del
ayin
g a
trea
tmen
t or t
est t
o se
e if
poss
ible
to d
o w
ithou
t it
-Ref
errin
g pa
tient
s to
oth
er le
ss
expe
nsiv
e op
tions
-Pro
vidi
ng le
ss fr
eque
nt fo
llow
up
of
NC
Ds
(chr
onic
con
ditio
ns)
-Lim
iting
CT
or M
RI o
rder
s-N
ot in
form
ing
the
patie
nt a
bout
ex
pens
ive
optio
ns-S
cree
ning
pat
ient
for d
ialy
sis
-Ref
use
expe
nsiv
e dr
ug re
ques
ted
by
patie
nts
or fa
mili
es
10H
ealth
fina
ncin
g st
rate
gies
to
redu
ce o
ut-o
f-poc
ket b
urde
n in
Indi
a: a
com
para
tive
stud
y of
th
ree
stat
es
Mon
tu B
ose
2018
Indi
aCo
mpa
rativ
e St
udy
Rese
arch
Art
icle
3917
hou
seho
lds
from
TN
, 291
2 ho
useh
olds
in R
ajas
than
and
50
19 h
ouse
hold
s fro
m W
B
-Pro
curin
g m
edic
ine
or re
gula
rly
upda
ting
the
esse
ntia
l lis
t of d
rugs
ac
cord
ing
to n
eed
of p
atie
nts
are
urge
ntly
requ
ired
in W
est B
enga
l-Im
prov
ing
acce
ss to
hea
lthca
re
faci
litie
s lik
e di
agno
stic
test
etc
-TN
and
Raj
asth
an h
ealth
fina
ncin
g st
rate
gies
Page 12 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
11Re
duci
ng th
e m
edic
al e
cono
mic
bu
rden
of h
ealth
insu
ranc
e in
C
hina
: Ach
ieve
men
ts a
nd c
hal-
leng
es
Dou
, G. S
2018
Chi
naPo
licy
Foru
m–
-Est
ablis
h a
man
dato
ry s
ocia
l ins
ur-
ance
pro
gram
for u
rban
em
ploy
-ee
s-E
stab
lish
the
New
Rur
al C
oope
rativ
e M
edic
al S
chem
e (N
CM
S)-E
stab
lish
Urb
an R
esid
ent B
asic
M
edic
al In
sura
nce
(URB
MI)
for
Chi
ldre
n, s
tude
nts,
the
elde
rly, t
he
disa
bled
, and
oth
er u
nem
ploy
ed
popu
latio
ns in
urb
an re
gion
s gr
oups
not
cov
ered
by
basi
c he
alth
in
sura
nce
-Incr
ease
gov
ernm
ent s
ubsi
dies
to
NC
MS
and
URB
MI t
o an
unp
rec-
eden
ted
scal
e-L
aunc
h Ca
tast
roph
ic D
isea
se In
sur-
ance
-Rep
lace
FFS
with
oth
er fo
rms
of
pros
pect
ive
paym
ent (
pros
pec-
tive
paym
ent s
yste
ms
such
as
the
glob
al b
udge
t pay
men
t sys
tem
-DRG
pay
men
ts-In
crea
se th
e effi
cien
cy a
nd q
ualit
y of
car
e un
der c
urre
nt p
aym
ent
syst
ems
12D
isea
se-s
peci
fic o
ut-o
f-poc
ket a
nd
cata
stro
phic
hea
lth e
xpen
ditu
re
on h
ospi
taliz
atio
n in
Indi
a: d
o In
dian
hou
seho
lds
face
dis
tres
s he
alth
fina
ncin
g?
Ans
hul K
asto
r20
18In
dia
Rese
arch
Art
icle
3,33
,104
indi
vidu
als
from
65,
932
hous
ehol
ds (3
6,48
0 ru
ral a
nd
29,4
52 u
rban
hou
seho
lds)
-The
Min
istr
y of
Hea
lth a
nd F
amily
W
elfa
re, G
over
nmen
t of I
ndia
la
unch
ed th
e N
atio
nal P
rogr
am fo
r Pr
even
tion
and
Cont
rol o
f Can
cer,
Dia
bete
s, Ca
rdio
vasc
ular
Dis
ease
an
d St
roke
-Sug
gest
for i
nclu
ding
trea
tmen
t of
canc
er, h
eart
dis
ease
s, an
d ot
her
rare
and
incu
rabl
e di
seas
es in
the
ambi
t of t
he h
ealth
insu
ranc
e co
vera
ge-P
rovi
de fr
ee tr
eatm
ent t
o th
e vu
l-ne
rabl
e se
gmen
t of t
he p
opul
atio
n fo
r the
trea
tmen
t of c
ance
r and
he
art d
isea
ses
-The
cov
erag
e an
d th
e in
sura
nce
amou
nt o
f the
RSB
Y ne
ed to
be
enla
rged
Page 13 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
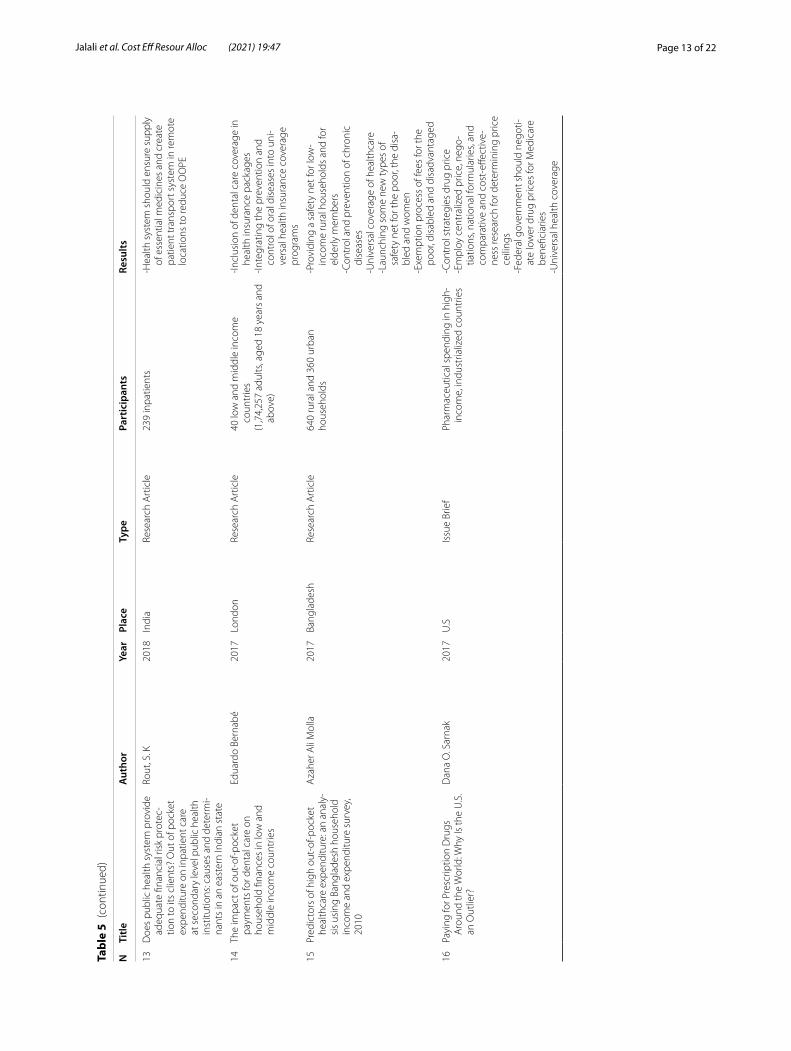
13D
oes
publ
ic h
ealth
sys
tem
pro
vide
ad
equa
te fi
nanc
ial r
isk
prot
ec-
tion
to it
s cl
ient
s? O
ut o
f poc
ket
expe
nditu
re o
n in
patie
nt c
are
at s
econ
dary
leve
l pub
lic h
ealth
in
stitu
tions
: cau
ses
and
dete
rmi-
nant
s in
an
east
ern
Indi
an s
tate
Rout
, S. K
2018
Indi
aRe
sear
ch A
rtic
le23
9 in
patie
nts
-Hea
lth s
yste
m s
houl
d en
sure
sup
ply
of e
ssen
tial m
edic
ines
and
cre
ate
patie
nt tr
ansp
ort s
yste
m in
rem
ote
loca
tions
to re
duce
OO
PE
14Th
e im
pact
of o
ut-o
f-poc
ket
paym
ents
for d
enta
l car
e on
ho
useh
old
finan
ces
in lo
w a
nd
mid
dle
inco
me
coun
trie
s
Edua
rdo
Bern
abé
2017
Lond
onRe
sear
ch A
rtic
le40
low
and
mid
dle
inco
me
coun
trie
s(1
,74,
257
adul
ts, a
ged
18 y
ears
and
ab
ove)
-Incl
usio
n of
den
tal c
are
cove
rage
in
heal
th in
sura
nce
pack
ages
-Inte
grat
ing
the
prev
entio
n an
d co
ntro
l of o
ral d
isea
ses
into
uni
-ve
rsal
hea
lth in
sura
nce
cove
rage
pr
ogra
ms
15Pr
edic
tors
of h
igh
out-
of-p
ocke
t he
alth
care
exp
endi
ture
: an
anal
y-si
s us
ing
Bang
lade
sh h
ouse
hold
in
com
e an
d ex
pend
iture
sur
vey,
20
10
Aza
her A
li M
olla
2017
Bang
lade
shRe
sear
ch A
rtic
le64
0 ru
ral a
nd 3
60 u
rban
hous
ehol
ds-P
rovi
ding
a s
afet
y ne
t for
low
-in
com
e ru
ral h
ouse
hold
s an
d fo
r el
derly
mem
bers
-Con
trol
and
pre
vent
ion
of c
hron
ic
dise
ases
-Uni
vers
al c
over
age
of h
ealth
care
-Lau
nchi
ng s
ome
new
type
s of
sa
fety
net
for t
he p
oor,
the
disa
-bl
ed a
nd w
omen
-Exe
mpt
ion
proc
ess
of fe
es fo
r the
po
or, d
isab
led
and
disa
dvan
tage
d
16Pa
ying
for P
resc
riptio
n D
rugs
A
roun
d th
e W
orld
: Why
Is th
e U
.S.
an O
utlie
r?
Dan
a O
. Sar
nak
2017
U.S
Issu
e Br
ief
Phar
mac
eutic
al s
pend
ing
in h
igh-
inco
me,
indu
stria
lized
cou
ntrie
s-C
ontr
ol s
trat
egie
s dr
ug p
rice
-Em
ploy
cen
tral
ized
pric
e, n
ego-
tiatio
ns, n
atio
nal f
orm
ular
ies,
and
com
para
tive
and
cost
-effe
ctiv
e-ne
ss re
sear
ch fo
r det
erm
inin
g pr
ice
ceili
ngs
-Fed
eral
gov
ernm
ent s
houl
d ne
goti-
ate
low
er d
rug
pric
es fo
r Med
icar
e be
nefic
iarie
s-U
nive
rsal
hea
lth c
over
age
Page 14 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
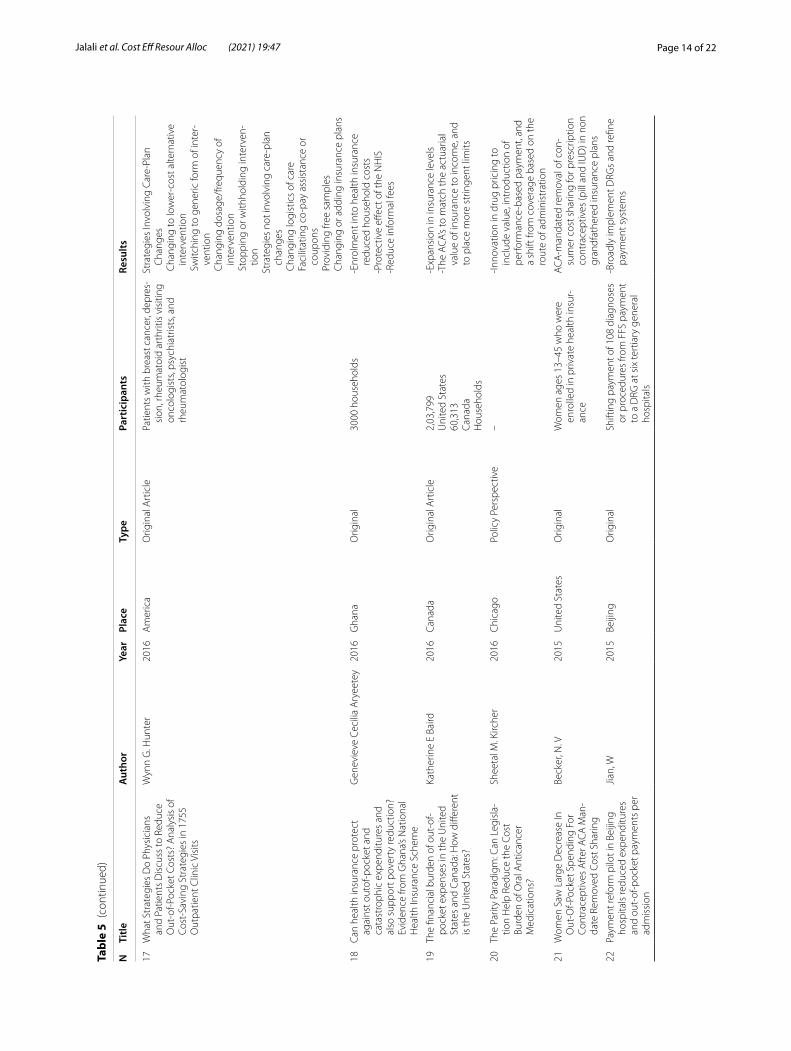
17W
hat S
trat
egie
s D
o Ph
ysic
ians
an
d Pa
tient
s D
iscu
ss to
Red
uce
Out
-of-P
ocke
t Cos
ts?
Ana
lysi
s of
Co
st-S
avin
g St
rate
gies
in 1
755
Out
patie
nt C
linic
Vis
its
Wyn
n G
. Hun
ter
2016
Am
eric
aO
rigin
al A
rtic
lePa
tient
s w
ith b
reas
t can
cer,
depr
es-
sion
, rhe
umat
oid
arth
ritis
vis
iting
on
colo
gist
s, ps
ychi
atris
ts, a
nd
rheu
mat
olog
ist
Stra
tegi
es In
volv
ing
Care
-Pla
n C
hang
es C
hang
ing
to lo
wer
-cos
t alte
rnat
ive
inte
rven
tion
Sw
itchi
ng to
gen
eric
form
of i
nter
-ve
ntio
n C
hang
ing
dosa
ge/f
requ
ency
of
inte
rven
tion
Sto
ppin
g or
with
hold
ing
inte
rven
-tio
nSt
rate
gies
not
invo
lvin
g ca
re-p
lan
chan
ges
Cha
ngin
g lo
gist
ics
of c
are
Fac
ilita
ting
co-p
ay a
ssis
tanc
e or
co
upon
s P
rovi
ding
free
sam
ples
Cha
ngin
g or
add
ing
insu
ranc
e pl
ans
18Ca
n he
alth
insu
ranc
e pr
otec
t ag
ains
t out
of-p
ocke
t and
ca
tast
roph
ic e
xpen
ditu
res
and
also
sup
port
pov
erty
redu
ctio
n?
Evid
ence
from
Gha
na’s
Nat
iona
l H
ealth
Insu
ranc
e Sc
hem
e
Gen
evie
ve C
ecili
a A
ryee
tey
2016
Gha
naO
rigin
al30
00 h
ouse
hold
s-E
nrol
men
t int
o he
alth
insu
ranc
e re
duce
d ho
useh
old
cost
s-P
rote
ctiv
e eff
ect o
f the
NH
IS-R
educ
e in
form
al fe
es
19Th
e fin
anci
al b
urde
n of
out
-of-
pock
et e
xpen
ses
in th
e U
nite
d St
ates
and
Can
ada:
How
diff
eren
t is
the
Uni
ted
Stat
es?
Kath
erin
e E
Baird
2016
Cana
daO
rigin
al A
rtic
le2,
03,7
99U
nite
d St
ates
60,3
13Ca
nada
Hou
seho
lds
-Exp
ansi
on in
insu
ranc
e le
vels
-The
AC
A’s
to m
atch
the
actu
aria
l va
lue
of in
sura
nce
to in
com
e, a
nd
to p
lace
mor
e st
ringe
nt li
mits
20Th
e Pa
rity
Para
digm
: Can
Leg
isla
-tio
n H
elp
Redu
ce th
e Co
st
Burd
en o
f Ora
l Ant
ican
cer
Med
icat
ions
?
Shee
tal M
. Kirc
her
2016
Chi
cago
Polic
y Pe
rspe
ctiv
e–
-Inno
vatio
n in
dru
g pr
icin
g to
in
clud
e va
lue,
intr
oduc
tion
of
perf
orm
ance
-bas
ed p
aym
ent,
and
a sh
ift fr
om c
over
age
base
d on
the
rout
e of
adm
inis
trat
ion
21W
omen
Saw
Lar
ge D
ecre
ase
In
Out
-Of-P
ocke
t Spe
ndin
g Fo
r Co
ntra
cept
ives
Aft
er A
CA
Man
-da
te R
emov
ed C
ost S
harin
g
Beck
er, N
. V20
15U
nite
d St
ates
Orig
inal
Wom
en a
ges
13–4
5 w
ho w
ere
enro
lled
in p
rivat
e he
alth
insu
r-an
ce
AC
A-m
anda
ted
rem
oval
of c
on-
sum
er c
ost s
harin
g fo
r pre
scrip
tion
cont
race
ptiv
es (p
ill a
nd IU
D) i
n no
n gr
andf
athe
red
insu
ranc
e pl
ans
22Pa
ymen
t ref
orm
pilo
t in
Beiji
ng
hosp
itals
redu
ced
expe
nditu
res
and
out-
of-p
ocke
t pay
men
ts p
er
adm
issi
on
Jian,
W20
15Be
ijing
Orig
inal
Shift
ing
paym
ent o
f 108
dia
gnos
es
or p
roce
dure
s fro
m F
FS p
aym
ent
to a
DRG
at s
ix te
rtia
ry g
ener
al
hosp
itals
-Bro
adly
impl
emen
t DRG
s an
d re
fine
paym
ent s
yste
ms
Page 15 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
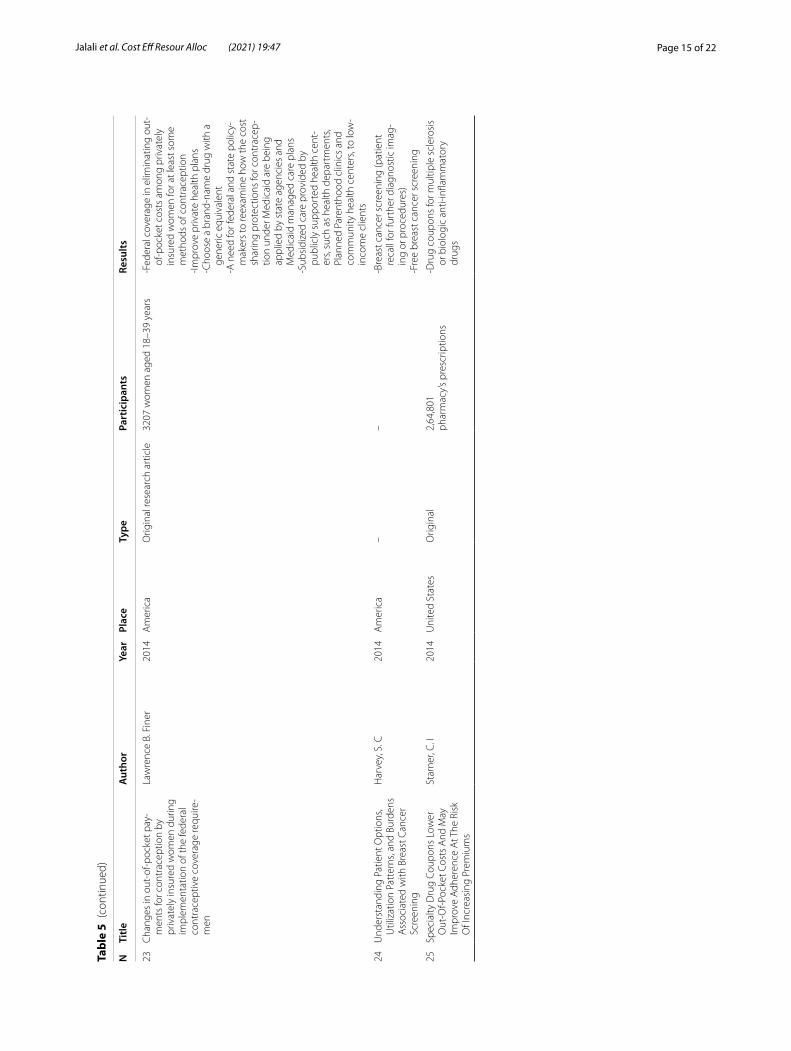
23C
hang
es in
out
-of-p
ocke
t pay
-m
ents
for c
ontr
acep
tion
by
priv
atel
y in
sure
d w
omen
dur
ing
impl
emen
tatio
n of
the
fede
ral
cont
race
ptiv
e co
vera
ge re
quire
-m
en
Law
renc
e B.
Fin
er20
14A
mer
ica
Orig
inal
rese
arch
art
icle
3207
wom
en a
ged
18–3
9 ye
ars
-Fed
eral
cov
erag
e in
elim
inat
ing
out-
of-p
ocke
t cos
ts a
mon
g pr
ivat
ely
insu
red
wom
en fo
r at l
east
som
e m
etho
ds o
f con
trac
eptio
n-Im
prov
e pr
ivat
e he
alth
pla
ns-C
hoos
e a
bran
d-na
me
drug
with
a
gene
ric e
quiv
alen
t-A
nee
d fo
r fed
eral
and
sta
te p
olic
y-m
aker
s to
reex
amin
e ho
w th
e co
st
shar
ing
prot
ectio
ns fo
r con
trac
ep-
tion
unde
r Med
icai
d ar
e be
ing
appl
ied
by s
tate
age
ncie
s an
d M
edic
aid
man
aged
car
e pl
ans
-Sub
sidi
zed
care
pro
vide
d by
pu
blic
ly s
uppo
rted
hea
lth c
ent-
ers,
such
as
heal
th d
epar
tmen
ts,
Plan
ned
Pare
ntho
od c
linic
s an
d co
mm
unity
hea
lth c
ente
rs, t
o lo
w-
inco
me
clie
nts
24U
nder
stan
ding
Pat
ient
Opt
ions
, U
tiliz
atio
n Pa
tter
ns, a
nd B
urde
ns
Ass
ocia
ted
with
Bre
ast C
ance
r Sc
reen
ing
Har
vey,
S. C
2014
Am
eric
a–
–-B
reas
t can
cer s
cree
ning
(pat
ient
re
call
for f
urth
er d
iagn
ostic
imag
-in
g or
pro
cedu
res)
-Fre
e br
east
can
cer s
cree
ning
25Sp
ecia
lty D
rug
Coup
ons
Low
er
Out
-Of-P
ocke
t Cos
ts A
nd M
ay
Impr
ove
Adh
eren
ce A
t The
Ris
k O
f Inc
reas
ing
Prem
ium
s
Star
ner,
C. I
2014
Uni
ted
Stat
esO
rigin
al2,
64,8
01ph
arm
acy’
s pr
escr
iptio
ns-D
rug
coup
ons
for m
ultip
le s
cler
osis
or
bio
logi
c an
ti-in
flam
mat
ory
drug
s
Page 16 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
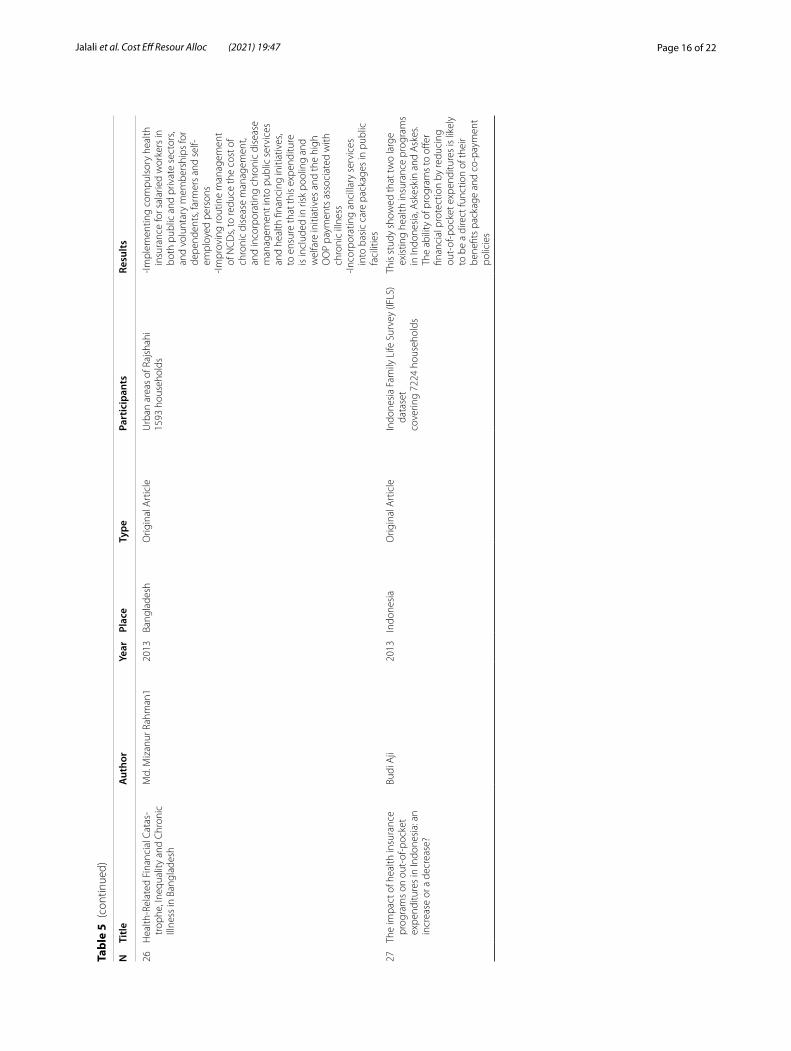
26H
ealth
-Rel
ated
Fin
anci
al C
atas
-tr
ophe
, Ine
qual
ity a
nd C
hron
ic
Illne
ss in
Ban
glad
esh
Md.
Miz
anur
Rah
man
120
13Ba
ngla
desh
Orig
inal
Art
icle
Urb
an a
reas
of R
ajsh
ahi
1593
hou
seho
lds
-Impl
emen
ting
com
puls
ory
heal
th
insu
ranc
e fo
r sal
arie
d w
orke
rs in
bo
th p
ublic
and
priv
ate
sect
ors,
and
volu
ntar
y m
embe
rshi
ps fo
r de
pend
ents
, far
mer
s an
d se
lf-em
ploy
ed p
erso
ns-Im
prov
ing
rout
ine
man
agem
ent
of N
CD
s, to
redu
ce th
e co
st o
f ch
roni
c di
seas
e m
anag
emen
t, an
d in
corp
orat
ing
chro
nic
dise
ase
man
agem
ent i
nto
publ
ic s
ervi
ces
and
heal
th fi
nanc
ing
initi
ativ
es,
to e
nsur
e th
at th
is e
xpen
ditu
re
is in
clud
ed in
risk
poo
ling
and
wel
fare
initi
ativ
es a
nd th
e hi
gh
OO
P pa
ymen
ts a
ssoc
iate
d w
ith
chro
nic
illne
ss-In
corp
orat
ing
anci
llary
ser
vice
s in
to b
asic
car
e pa
ckag
es in
pub
lic
faci
litie
s
27Th
e im
pact
of h
ealth
insu
ranc
e pr
ogra
ms
on o
ut-o
f-poc
ket
expe
nditu
res
in In
done
sia:
an
incr
ease
or a
dec
reas
e?
Budi
Aji
2013
Indo
nesi
aO
rigin
al A
rtic
leIn
done
sia
Fam
ily L
ife S
urve
y (IF
LS)
data
set
cove
ring
7224
hou
seho
lds
This
stu
dy s
how
ed th
at tw
o la
rge
exis
ting
heal
th in
sura
nce
prog
ram
s in
Indo
nesi
a, A
skes
kin
and
Ask
es.
The
abili
ty o
f pro
gram
s to
offe
r fin
anci
al p
rote
ctio
n by
redu
cing
ou
t-of
-poc
ket e
xpen
ditu
res
is li
kely
to
be
a di
rect
func
tion
of th
eir
bene
fits
pack
age
and
co-p
aym
ent
polic
ies
Page 17 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
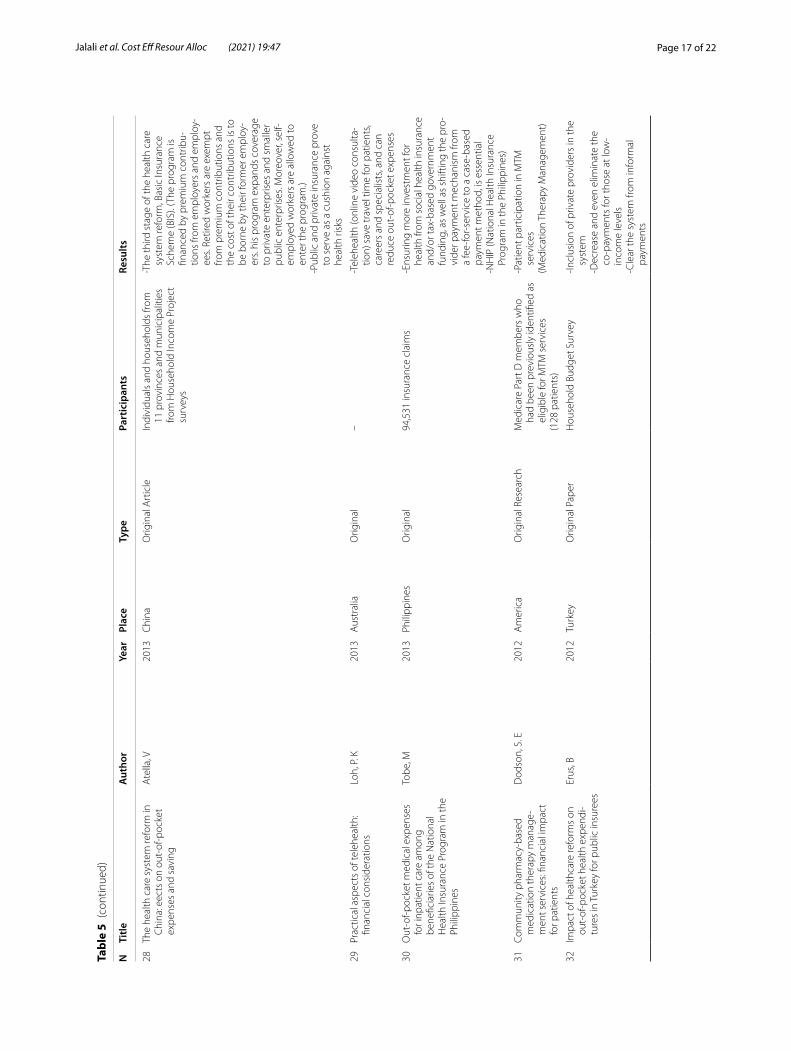
28Th
e he
alth
car
e sy
stem
refo
rm in
C
hina
: eec
ts o
n ou
t-of
-poc
ket
expe
nses
and
sav
ing
Ate
lla, V
2013
Chi
naO
rigin
al A
rtic
leIn
divi
dual
s an
d ho
useh
olds
from
11
pro
vinc
es a
nd m
unic
ipal
ities
fro
m H
ouse
hold
Inco
me
Proj
ect
surv
eys
-The
third
sta
ge o
f the
hea
lth c
are
syst
em re
form
, Bas
ic In
sura
nce
Sche
me
(BIS
). (T
he p
rogr
am is
fin
ance
d by
pre
miu
m c
ontr
ibu-
tions
from
em
ploy
ers
and
empl
oy-
ees.
Retir
ed w
orke
rs a
re e
xem
pt
from
pre
miu
m c
ontr
ibut
ions
and
th
e co
st o
f the
ir co
ntrib
utio
ns is
to
be b
orne
by
thei
r for
mer
em
ploy
-er
s. hi
s pr
ogra
m e
xpan
ds c
over
age
to p
rivat
e en
terp
rises
and
sm
alle
r pu
blic
ent
erpr
ises
. Mor
eove
r, se
lf-em
ploy
ed w
orke
rs a
re a
llow
ed to
en
ter t
he p
rogr
am.)
-Pub
lic a
nd p
rivat
e in
sura
nce
prov
e to
ser
ve a
s a
cush
ion
agai
nst
heal
th ri
sks
29Pr
actic
al a
spec
ts o
f tel
ehea
lth:
finan
cial
con
side
ratio
nsLo
h, P
. K20
13A
ustr
alia
Orig
inal
–-T
eleh
ealth
(onl
ine
vide
o co
nsul
ta-
tion)
sav
e tr
avel
tim
e fo
r pat
ient
s, ca
reer
s an
d sp
ecia
lists
, and
can
re
duce
out
-of-p
ocke
t exp
ense
s
30O
ut-o
f-poc
ket m
edic
al e
xpen
ses
for i
npat
ient
car
e am
ong
bene
ficia
ries
of th
e N
atio
nal
Hea
lth In
sura
nce
Prog
ram
in th
e Ph
ilipp
ines
Tobe
, M20
13Ph
ilipp
ines
Orig
inal
94,5
31 in
sura
nce
clai
ms
-Ens
urin
g m
ore
inve
stm
ent f
or
heal
th fr
om s
ocia
l hea
lth in
sura
nce
and/
or ta
x-ba
sed
gove
rnm
ent
fund
ing,
as
wel
l as
shift
ing
the
pro-
vide
r pay
men
t mec
hani
sm fr
om
a fe
e-fo
r-se
rvic
e to
a c
ase-
base
d pa
ymen
t met
hod,
is e
ssen
tial
-NH
IP (N
atio
nal H
ealth
Insu
ranc
e Pr
ogra
m in
the
Phili
ppin
es)
31Co
mm
unity
pha
rmac
y-ba
sed
med
icat
ion
ther
apy
man
age-
men
t ser
vice
s: fin
anci
al im
pact
fo
r pat
ient
s
Dod
son,
S. E
2012
Am
eric
aO
rigin
al R
esea
rch
Med
icar
e Pa
rt D
mem
bers
who
ha
d be
en p
revi
ousl
y id
entifi
ed a
s el
igib
le fo
r MTM
ser
vice
s(1
28 p
atie
nts)
-Pat
ient
par
ticip
atio
n in
MTM
se
rvic
es(M
edic
atio
n Th
erap
y M
anag
emen
t)
32Im
pact
of h
ealth
care
refo
rms
on
out-
of-p
ocke
t hea
lth e
xpen
di-
ture
s in
Tur
key
for p
ublic
insu
rees
Erus
, B20
12Tu
rkey
Orig
inal
Pap
erH
ouse
hold
Bud
get S
urve
y-In
clus
ion
of p
rivat
e pr
ovid
ers
in th
e sy
stem
-Dec
reas
e an
d ev
en e
limin
ate
the
co-p
aym
ents
for t
hose
at l
ow-
inco
me
leve
ls-C
lear
the
syst
em fr
om in
form
al
paym
ents
Page 18 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
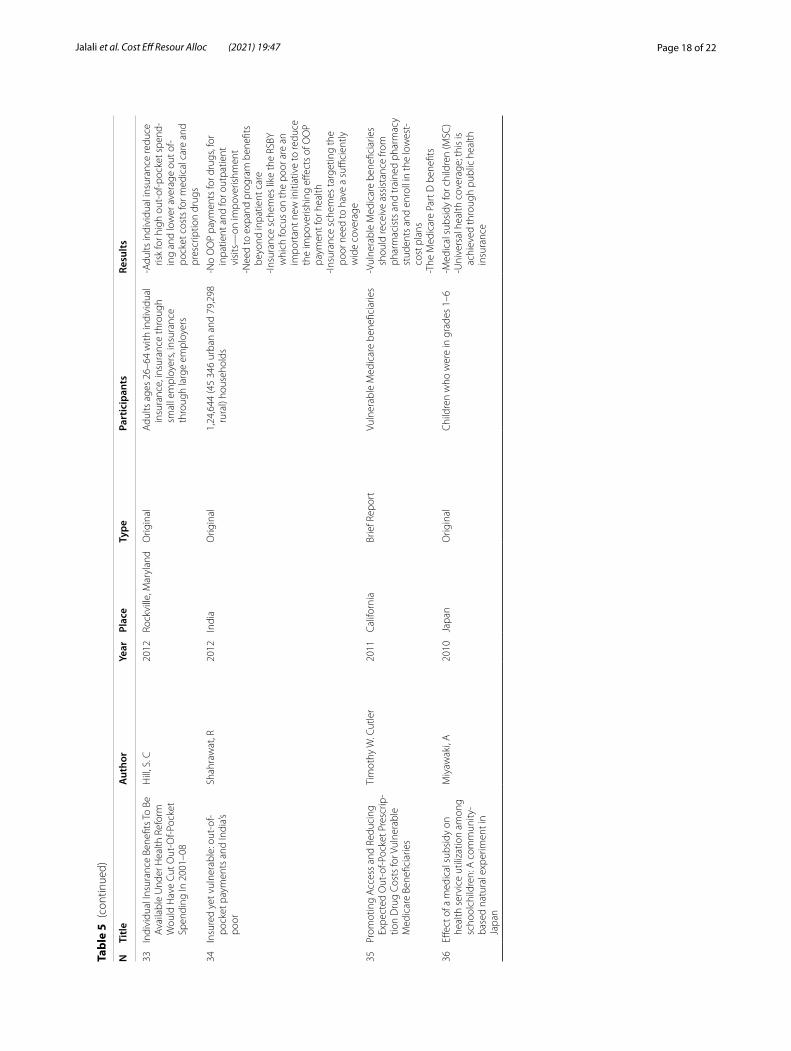
33In
divi
dual
Insu
ranc
e Be
nefit
s To
Be
Ava
ilabl
e U
nder
Hea
lth R
efor
m
Wou
ld H
ave
Cut O
ut-O
f-Poc
ket
Spen
ding
In 2
001–
08
Hill
, S. C
2012
Rock
ville
, Mar
ylan
dO
rigin
alA
dults
age
s 26
–64
with
indi
vidu
al
insu
ranc
e, in
sura
nce
thro
ugh
smal
l em
ploy
ers,
insu
ranc
e th
roug
h la
rge
empl
oyer
s
-Adu
lts in
divi
dual
insu
ranc
e re
duce
ris
k fo
r hig
h ou
t-of
-poc
ket s
pend
-in
g an
d lo
wer
ave
rage
out
of-
pock
et c
osts
for m
edic
al c
are
and
pres
crip
tion
drug
s
34In
sure
d ye
t vul
nera
ble:
out
-of-
pock
et p
aym
ents
and
Indi
a’s
poor
Shah
raw
at, R
2012
Indi
aO
rigin
al1,
24,6
44 (4
5 34
6 ur
ban
and
79,2
98
rura
l) ho
useh
olds
-No
OO
P pa
ymen
ts fo
r dru
gs, f
or
inpa
tient
and
for o
utpa
tient
vi
sits
—on
impo
veris
hmen
t-N
eed
to e
xpan
d pr
ogra
m b
enefi
ts
beyo
nd in
patie
nt c
are
-Insu
ranc
e sc
hem
es li
ke th
e RS
BY
whi
ch fo
cus
on th
e po
or a
re a
n im
port
ant n
ew in
itiat
ive
to re
duce
th
e im
pove
rishi
ng e
ffect
s of
OO
P pa
ymen
t for
hea
lth-In
sura
nce
sche
mes
targ
etin
g th
e po
or n
eed
to h
ave
a su
ffici
ently
w
ide
cove
rage
35Pr
omot
ing
Acc
ess
and
Redu
cing
Ex
pect
ed O
ut-o
f-Poc
ket P
resc
rip-
tion
Dru
g Co
sts
for V
ulne
rabl
e M
edic
are
Bene
ficia
ries
Tim
othy
W. C
utle
r20
11Ca
lifor
nia
Brie
f Rep
ort
Vuln
erab
le M
edic
are
bene
ficia
ries
-Vul
nera
ble
Med
icar
e be
nefic
iarie
s sh
ould
rece
ive
assi
stan
ce fr
om
phar
mac
ists
and
trai
ned
phar
mac
y st
uden
ts a
nd e
nrol
l in
the
low
est-
cost
pla
ns-T
he M
edic
are
Part
D b
enefi
ts
36Eff
ect o
f a m
edic
al s
ubsi
dy o
n he
alth
ser
vice
util
izat
ion
amon
g sc
hool
child
ren:
A c
omm
unity
-ba
sed
natu
ral e
xper
imen
t in
Japa
n
Miy
awak
i, A
2010
Japa
nO
rigin
alC
hild
ren
who
wer
e in
gra
des
1–6
-Med
ical
sub
sidy
for c
hild
ren
(MSC
)-U
nive
rsal
hea
lth c
over
age;
this
is
achi
eved
thro
ugh
publ
ic h
ealth
in
sura
nce
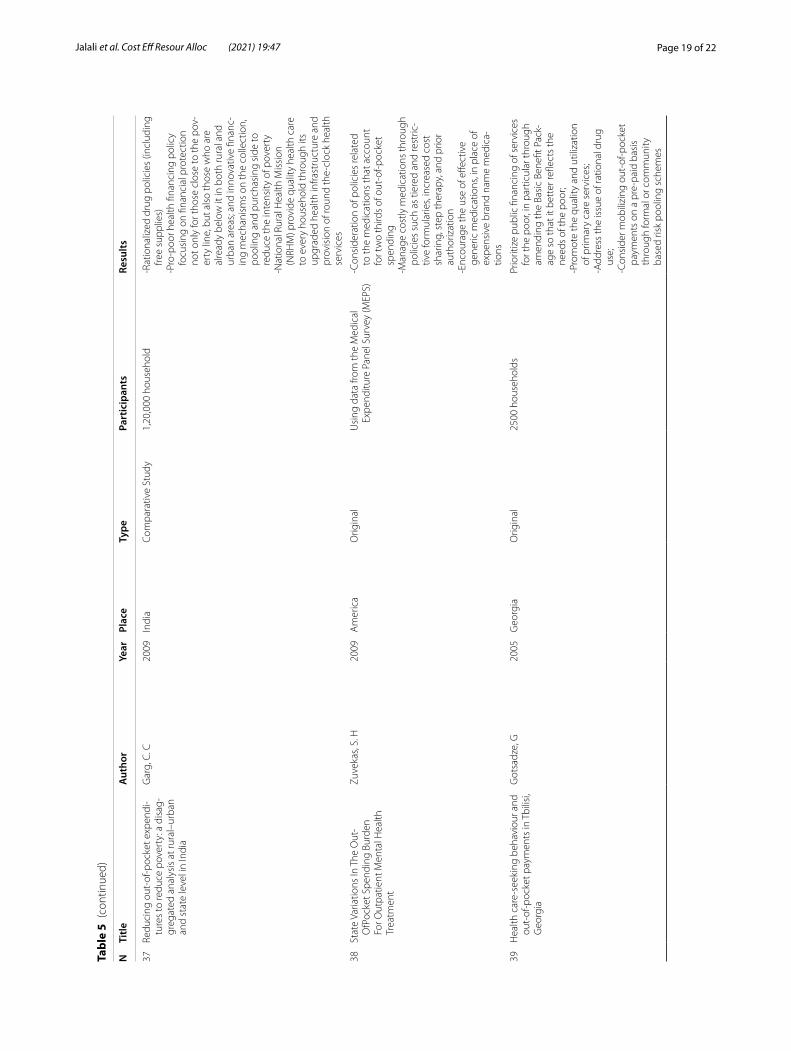
Page 19 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
37Re
duci
ng o
ut-o
f-poc
ket e
xpen
di-
ture
s to
redu
ce p
over
ty: a
dis
ag-
greg
ated
ana
lysi
s at
rura
l–ur
ban
and
stat
e le
vel i
n In
dia
Gar
g, C
. C20
09In
dia
Com
para
tive
Stud
y1,
20,0
00 h
ouse
hold
-Rat
iona
lized
dru
g po
licie
s (in
clud
ing
free
supp
lies)
-Pro
-poo
r hea
lth fi
nanc
ing
polic
y fo
cusi
ng o
n fin
anci
al p
rote
ctio
n no
t onl
y fo
r tho
se c
lose
to th
e po
v-er
ty li
ne, b
ut a
lso
thos
e w
ho a
re
alre
ady
belo
w it
in b
oth
rura
l and
ur
ban
area
s; an
d in
nova
tive
finan
c-in
g m
echa
nism
s on
the
colle
ctio
n,
pool
ing
and
purc
hasi
ng s
ide
to
redu
ce th
e in
tens
ity o
f pov
erty
-Nat
iona
l Rur
al H
ealth
Mis
sion
(N
RHM
) pro
vide
qua
lity
heal
th c
are
to e
very
hou
seho
ld th
roug
h its
up
grad
ed h
ealth
infra
stru
ctur
e an
d pr
ovis
ion
of ro
und
the-
cloc
k he
alth
se
rvic
es
38St
ate
Varia
tions
In T
he O
ut-
OfP
ocke
t Spe
ndin
g Bu
rden
Fo
r Out
patie
nt M
enta
l Hea
lth
Trea
tmen
t
Zuve
kas,
S. H
2009
Am
eric
aO
rigin
alU
sing
dat
a fro
m th
e M
edic
al
Expe
nditu
re P
anel
Sur
vey
(MEP
S)-C
onsi
dera
tion
of p
olic
ies
rela
ted
to th
e m
edic
atio
ns th
at a
ccou
nt
for t
wo
third
s of
out
-of-p
ocke
t sp
endi
ng-M
anag
e co
stly
med
icat
ions
thro
ugh
polic
ies
such
as
tiere
d an
d re
stric
-tiv
e fo
rmul
arie
s, in
crea
sed
cost
sh
arin
g, s
tep
ther
apy,
and
prio
r au
thor
izat
ion
-Enc
oura
ge th
e us
e of
effe
ctiv
e ge
neric
med
icat
ions
, in
plac
e of
ex
pens
ive
bran
d na
me
med
ica-
tions
39H
ealth
car
e-se
ekin
g be
havi
our a
nd
out-
of-p
ocke
t pay
men
ts in
Tbi
lisi,
Geo
rgia
Got
sadz
e, G
2005
Geo
rgia
Orig
inal
2500
hou
seho
lds
Prio
ritiz
e pu
blic
fina
ncin
g of
ser
vice
s fo
r the
poo
r, in
par
ticul
ar th
roug
h am
endi
ng th
e Ba
sic
Bene
fit P
ack-
age
so th
at it
bet
ter r
eflec
ts th
e ne
eds
of th
e po
or;
-Pro
mot
e th
e qu
ality
and
util
izat
ion
of p
rimar
y ca
re s
ervi
ces;
-Add
ress
the
issu
e of
ratio
nal d
rug
use;
-Con
side
r mob
ilizi
ng o
ut-o
f-poc
ket
paym
ents
on
a pr
e-pa
id b
asis
th
roug
h fo
rmal
or c
omm
unity
ba
sed
risk
pool
ing
sche
mes
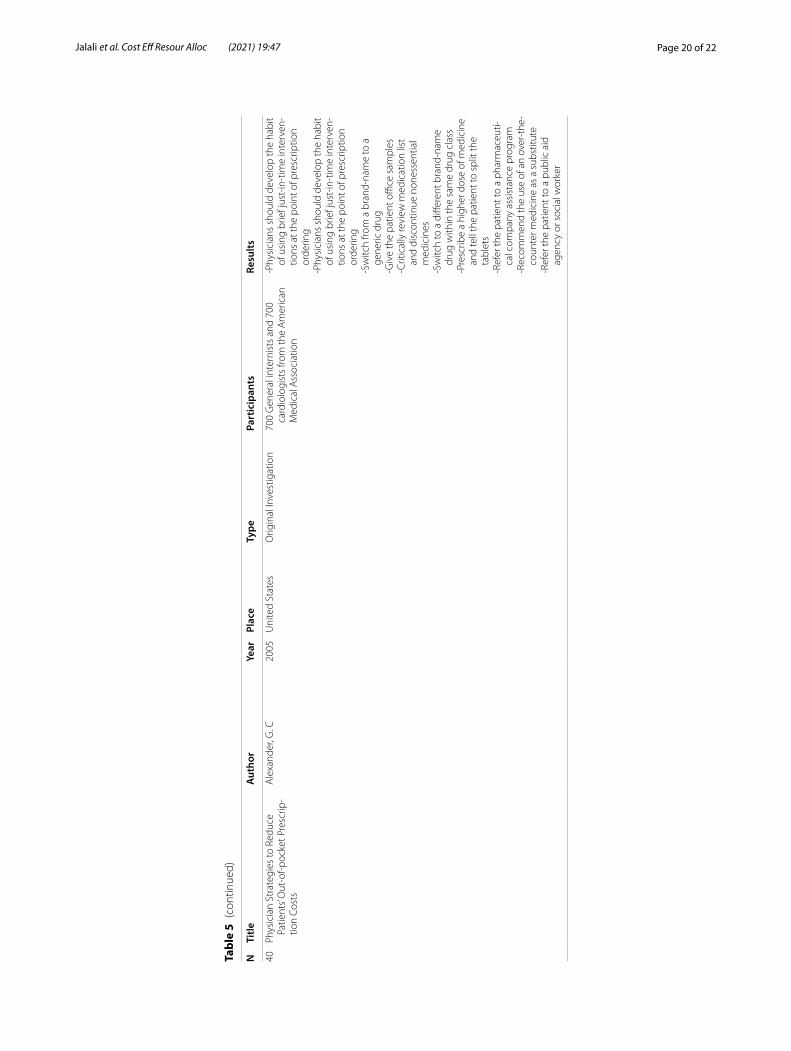
Page 20 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
Tabl
e 5
(con
tinue
d)
NTi
tleA
utho
rYe
arPl
ace
Type
Part
icip
ants
Resu
lts
40Ph
ysic
ian
Stra
tegi
es to
Red
uce
Patie
nts’
Out
-of-p
ocke
t Pre
scrip
-tio
n Co
sts
Ale
xand
er, G
. C20
05U
nite
d St
ates
Orig
inal
Inve
stig
atio
n70
0 G
ener
al in
tern
ists
and
700
ca
rdio
logi
sts
from
the
Am
eric
an
Med
ical
Ass
ocia
tion
-Phy
sici
ans
shou
ld d
evel
op th
e ha
bit
of u
sing
brie
f jus
t-in
-tim
e in
terv
en-
tions
at t
he p
oint
of p
resc
riptio
n or
derin
g-P
hysi
cian
s sh
ould
dev
elop
the
habi
t of
usi
ng b
rief j
ust-
in-t
ime
inte
rven
-tio
ns a
t the
poi
nt o
f pre
scrip
tion
orde
ring
-Sw
itch
from
a b
rand
-nam
e to
a
gene
ric d
rug
-Giv
e th
e pa
tient
offi
ce s
ampl
es-C
ritic
ally
revi
ew m
edic
atio
n lis
t an
d di
scon
tinue
non
esse
ntia
l m
edic
ines
-Sw
itch
to a
diff
eren
t bra
nd-n
ame
drug
with
in th
e sa
me
drug
cla
ss-P
resc
ribe
a hi
gher
dos
e of
med
icin
e an
d te
ll th
e pa
tient
to s
plit
the
tabl
ets
-Ref
er th
e pa
tient
to a
pha
rmac
euti-
cal c
ompa
ny a
ssis
tanc
e pr
ogra
m-R
ecom
men
d th
e us
e of
an
over
-the
-co
unte
r med
icin
e as
a s
ubst
itute
-Ref
er th
e pa
tient
to a
pub
lic a
id
agen
cy o
r soc
ial w
orke
r
Page 21 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
AcknowledgementsAuthors would like to thank Shiraz University of Medical Sciences (SUMS) for financial support of the research.
Authors’ contributionsFSJ and PB did the search and screaning and data extraction. SD raised the research idea and supervises all phase of the research. All authors have equal contribution in drafting and reviewing the manuscript. All authors have read and approved the final manuscript.
FundingThe study has been funded by Shiraz University of Medical Sciences (SUMS) under the code of 23113.
Availability of data and materialsData of this research is available and could be sent upon contact with the corresponding author.
Declarations
Ethics approval and consent to participateThe study protocol has been approved by ethics committee of Shiraz Univer-sity of Medical Sciences under the code of IR.SUMS.REC.1400.030.
Consent for publicationNot applicable.
Competing interestsThe authors declare they have no competing interest regarding to this research.
Author details1 Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran. 2 Health Human Resources Research Center, School of Health Manage-ment and Information Sciences, Shiraz University of Medical Sciences, Shiraz, Iran.
Received: 6 June 2021 Accepted: 28 July 2021
References 1. World Health Organization. Countries are spending more on health, but
people are still paying too much out of their own pockets. 2019. 2. Kalantari H, Davari M, Akbari M, Hejazi SM, Kalantari M, Zakerin S, et al.
The estimation of direct medical costs of treating patients with chronic hepatitis B and C in iran. Int J Prev Med. 2012;3(3):191.
3. Tarricone R. Cost-of-illness analysis: what room in health economics? Health Policy. 2006;77(1):51–63.
4. Sriram S, Khan MM. Effect of health insurance program for the poor on out-of-pocket inpatient care cost in India: evidence from a nationally rep-resentative cross-sectional survey. BMC Health Serv Res. 2020;20(1):1–21.
5. Garg CC, Karan AK. Reducing out-of-pocket expenditures to reduce poverty: a disaggregated analysis at rural-urban and state level in India. Health Policy Plan. 2009;24(2):116–28.
6. Hunter WG, Zhang CZ, Hesson A, Davis JK, Kirby C, Williamson LD, et al. What strategies do physicians and patients discuss to reduce out-of-pocket costs? Analysis of cost-saving strategies in 1755 outpatient clinic visits. Med Decis Making. 2016;36(7):900–10.
7. Baji P, Pavlova M, Gulácsi L, Groot W. Changes in equity in out-of-pocket payments during the period of health care reforms: evidence from Hun-gary. Int J Equity Health. 2012;11(1):36.
8. World Bank: People Spend Half a Trillion Dollars Out-Of-Pocket on Health in Developing Countries Annually. 2019.
9. World Health Organization.Global spending on health: a world in transi-tion. 2019.
10. Wagstaff A, Eozenou P, Smitz M. Out-of-pocket expenditures on health: a global stocktake. World Bank Res Obs. 2020;35(2):123–57.
11. Tabari-Khomeiran R, Delavari S, Rezaei S, Rad EH, Shahmoradi M. The effect of Iranian health system reform plan on payments and costs of coronary artery bypass surgery in private hospitals of Iran. Int J Hum Rights Healthc. 2019;12(3):208–14.
12. World Health Organization. Developing a national health financing strategy. 2017.
13. Schofield D, Cunich M, Shrestha R, Passey M, Veerman L, Tanton R, et al. The indirect costs of ischemic heart disease through lost productive life years for Australia from 2015 to 2030: results from a microsimulation model. BMC Public Health. 2019;19(1):1–13.
14. Kircher SM, Meeker CR, Nimeiri H, Geynisman DM, Zafar SY, Shankaran V, et al. The parity paradigm: can legislation help reduce the cost burden of oral anticancer medications? Value Health. 2016;19(1):88–98.
15. Ergo A, Htoo TS, Badiani-Magnusson R, Royono R. A new hope: from neglect of the health sector to aspirations for Universal Health Coverage in Myanmar. Health Policy Plan. 2019;34(Supplement_1):i38–46.
16. Meda IB, Baguiya A, Ridde V, Ouédraogo HG, Dumont A, Kouanda S. Out-of-pocket payments in the context of a free maternal health care policy in Burkina Faso: a national cross-sectional survey. Heal Econ Rev. 2019;9(1):11.
17. Heydari M, Mehraeen M, Joulaei H. Over Medication and Waste of Resources in Physicians’ Prescriptions: A Cross Sectional Study in South-western Iran. Shiraz E Med J. 2020. https:// doi. org/ 10. 5812/ semj. 97662.
18. Dou G, Wang Q, Ying X. Reducing the medical economic burden of health insurance in China: achievements and challenges. Biosci Trends. 2018;12(3):215–9.
19. Molla AA, Chi C, Mondaca ALN. Predictors of high out-of-pocket health-care expenditure: an analysis using Bangladesh household income and expenditure survey, 2010. BMC Health Serv Res. 2017;17(1):94.
20. Zuvekas SH, Meyerhoefer CD. State variations in the out-of-pocket spending burden for outpatient mental health treatment. Health Aff. 2009;28(3):713–22.
21. Orenstein L, Chetrit A, Oberman B, Benderly M, Kalter-Leibovici O. Factors associated with disparities in out-of-pocket expenditure on dental care: results from two cross-sectional national surveys. Isr J Health Policy Res. 2020;9(1):1–17.
22. Sarnak DO, Squires D, Kuzmak G, Bishop S. Paying for prescription drugs around the world: why is the US an outlier? Issue Br. 2017;2017:1–14.
23. Miyawaki A, Kobayashi Y. Effect of a medical subsidy on health service uti-lization among schoolchildren: a community-based natural experiment in Japan. Health Policy. 2019;123(4):353–9.
24. Gotsadze G, Bennett S, Ranson K, Gzirishvili D. Health care-seeking behav-iour and out-of-pocket payments in Tbilisi, Georgia. Health Policy Plan. 2005;20(4):232–42.
25. Starner CI, Alexander GC, Bowen K, Qiu Y, Wickersham PJ, Gleason PJ. Spe-cialty drug coupons lower out-of-pocket costs and may improve adher-ence at the risk of increasing premiums. Health Aff. 2014;33(10):1761–9.
26. Becker NV, Polsky D. Women saw large decrease in out-of-pocket spend-ing for contraceptives after ACA mandate removed cost sharing. Health Aff. 2015;34(7):1204–11.
27. Finer LB, Sonfield A, Jones RK. Changes in out-of-pocket payments for contraception by privately insured women during implementation of the federal contraceptive coverage requirement. Contraception. 2014;89(2):97–102.
28. Bernabé E, Masood M, Vujicic M. The impact of out-of-pocket payments for dental care on household finances in low and middle income coun-tries. BMC Public Health. 2017;17(1):109.
29. Erus B, Aktakke N. Impact of healthcare reforms on out-of-pocket health expenditures in Turkey for public insurees. Eur J Health Econ. 2012;13(3):337–46.
30. Rahman MM, Gilmour S, Saito E, Sultana P, Shibuya K. Health-related financial catastrophe, inequality and chronic illness in Bangladesh. PLoS One. 2013;8(2):e56873.
31. Kastor A, Mohanty SK. Disease-specific out-of-pocket and catastrophic health expenditure on hospitalization in India: Do Indian households face distress health financing? PLoS One. 2018;13(5):e0196106.
32. Bose M, Dutta A. Health financing strategies to reduce out-of-pocket burden in India: a comparative study of three states. BMC Health Serv Res. 2018;18(1):830.
Page 22 of 22Jalali et al. Cost Eff Resour Alloc (2021) 19:47
• fast, convenient online submission
•
thorough peer review by experienced researchers in your field
• rapid publication on acceptance
• support for research data, including large and complex data types
•
gold Open Access which fosters wider collaboration and increased citations
maximum visibility for your research: over 100M website views per year •
At BMC, research is always in progress.
Learn more biomedcentral.com/submissions
Ready to submit your researchReady to submit your research ? Choose BMC and benefit from: ? Choose BMC and benefit from:
33. Jian W, Lu M, Chan KY, Poon AN, Han W, Hu M, et al. Payment reform pilot in Beijing hospitals reduced expenditures and out-of-pocket payments per admission. Health Aff. 2015;34(10):1745–52.
34. Rahman MM, Zhang C, Swe KT, Rahman MS, Islam MR, Kamrujjaman M, et al. Disease-specific out-of-pocket healthcare expenditure in urban Bangladesh: a Bayesian analysis. PLoS One. 2020;15(1):e0227565.
35. Khan JA, Ahmed S, Sultana M, Sarker AR, Chakrovorty S, Rahman MH, et al. The effect of a community-based health insurance on the out-of-pocket payments for utilizing medically trained providers in Bangladesh. Int Health. 2020;12(4):287–98.
36. Tobe M, Stickley A, del Rosario Jr RB, Shibuya K. Out-of-pocket medi-cal expenses for inpatient care among beneficiaries of the National Health Insurance Program in the Philippines. Health Policy Plan. 2013;28(5):536–48.
37. Aryeetey GC, Westeneng J, Spaan E, Jehu-Appiah C, Agyepong IA, Baltussen R. Can health insurance protect against out-of-pocket and catastrophic expenditures and also support poverty reduction? Evidence from Ghana’s National Health Insurance Scheme. Int J Equity Health. 2016;15(1):116.
38. Rout SK, Choudhury S. Does public health system provide adequate financial risk protection to its clients? Out of pocket expenditure on inpatient care at secondary level public health institutions: causes and determinants in an eastern Indian state. Int J Health Plann Manage. 2018;33(2):e500–11.
39. McIntyre WF, Belesiotis P, McClure GR, Demers C, Chahill G, Hayes A, et al. Strategies to reduce out-of-pocket medication costs for Canadians living with heart failure. Cardiovasc Drugs Ther. 2020. https:// doi. org/ 10. 1007/ s10557- 020- 07046-1.
40. Hill SC. Individual insurance benefits to be available under health reform would have cut out-of-pocket spending in 2001–08. Health Aff. 2012;31(6):1349–56.
41. Aji B, De Allegri M, Souares A, Sauerborn R. The impact of health insur-ance programs on out-of-pocket expenditures in Indonesia: an increase or a decrease? Int J Environ Res Public Health. 2013;10(7):2995–3013.
42. Shahrawat R, Rao KD. Insured yet vulnerable: out-of-pocket payments and India’s poor. Health Policy Plan. 2012;27(3):213–21.
43. Baird KE. The financial burden of out-of-pocket expenses in the United States and Canada: how different is the United States? SAGE Open Med. 2016;4:2050312115623792.
44. Loh P, Sabesan S, Allen D, Caldwell P, Mozer R, Komesaroff PA, et al. Practical aspects of telehealth: financial considerations. Intern Med J. 2013;43(7):829–34.
45. Alexander GC, Casalino LP, Meltzer DO. Physician strategies to reduce patients’ out-of-pocket prescription costs. Arch Intern Med. 2005;165(6):633–6.
46. Cutler TW, Stebbins MR, Smith AR, Patel RA, Lipton HL. Promoting access and reducing expected out-of-pocket prescription drug costs for vulner-able medicare beneficiaries: a pharmacist-directed model. Med Care. 2011;1:343–7.
47. Dodson SE, Ruisinger JF, Howard PA, Hare SE, Barnes BJ. Community pharmacy-based medication therapy management services: financial impact for patients. Pharm Pract. 2012;10(3):119.
48. Atella V, Brugiavini A, Pace N. The health care system reform in China: effects on out-of-pocket expenses and saving. China Econ Rev. 2015;34:182–95.
49. Meng Z, Ma Y, Song S, Li Y, Wang D, Si Y, et al. Economic implications of chinese diagnosis-related group-based payment systems for critically Ill patients in ICUs. Crit Care Med. 2020;48(7):e565–73.
50. Miljeteig I, Defaye FB, Wakim P, Desalegn DN, Berhane Y, Norheim OF, et al. Financial risk protection at the bedside: How Ethiopian physi-cians try to minimize out-of-pocket health expenditures. PLoS One. 2019;14(2):e0212129.
51. Harvey SC, Vegesna A, Mass S, Clarke J, Skoufalos A. Understanding patient options, utilization patterns, and burdens associated with breast cancer screening. J Womens Health. 2014;23(S1):S-3-S-9.
52. World Health Organization. The world health report 2000: health systems: improving performance. Geneva: World Health Organization, 2000.
53. Asefzadeh S, Alijanzadeh M, Peyravian F. Out of pocket expenditures for outpatient clinics in teaching hospitals. Payesh. 2014;13(3):267–76.
54. Kavosi Z, Lankarani KB, Dehnavieh R, Ghorbanian A. Influential factors of out of pocket payments for health care in Iran: A foresight approach using the cross impact analysis. J Pak Med Assoc. 2020;70(11):1918–26.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in pub-lished maps and institutional affiliations.




![health...Coverage (UHC) [1]. The path to UHC involves securing resources, reducing the reliance on direct out of pocket payments for health services, and improv-ing efficiency and](https://img.pdfslide.us/doc/110x75/5f4f58052afa395c63034d5c/health-coverage-uhc-1-the-path-to-uhc-involves-securing-resources-reducing.jpg)