Embed Size (px)
Citation preview

Regulatory Framework
Coverage
Objectives
Background
Over the past years, we have already…
13
13STRATEGIC REVIEWON HEALTHCARE MANPOWER PLANNING AND PROFESSIONAL DEVELOPMENT
Since 2012First territory-wide, comprehensive review on healthcare manpower planning and professional developmentSteering Committee, Coordinating Committee and six Sub-groups involving over 100 members in the healthcare professions and communityCommissioned studies by –
statutory Boards and Councils(Boards and Councils)
To cope with anticipated demand for healthcare manpowerTo facilitate professional development of healthcare professions
healthcare professions subject to statutory registration
Also looks into other healthcare professions not subject to statutory registration
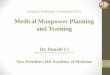
healthcare professionals(figures denote no. of registrants as at end 2016
% denotes % change from total no. of registrants in 2006)
Professional Development
Manpower Projection
Strategic Review Fast Facts
Substantially increased local healthcare training places
For non-locally trained healthcare professionals, relevant Boards and Councils have
The Hospital Authority has
Totalling ~ 1 800 UGC-fundedOver 50% increase in the no. of UGC-funded healthcare training places in the past 10 years (+600)
Increased the frequency of licensing examinationsRefined the exemption arrangement of licensing examinations and internship Set up an online platform for non-locally trained doctors
Totalling ~ 2 400 self-financing
480 nursing, 20 medical laboratory science and 12 radiation therapy training places subsidised under Study Subsidy Scheme for Designated Professions/Sectors ($70 000 per student)
Doctors: 250 → 470 ( ~ 90%)Dentists: 50 → 73 ( ~ 40%)Nurses: 518 → 630 ( ~ 20%)Pharmacists: 30 → 90 ( ~ 200%)OTs: 40 → 100 ( ~ 150%)PTs: 60 → 130 ( ~ 120%)MLTs: 35 → 54 ( ~ 50%)Optometrists: 35 → 40 ( ~ 10%)Radiographers: 35 → 110 ( ~ 210%)
Nurses: 610 → 2 200 Dental Hygienists: 20OTs: 50 (under accreditation)MLTs: 55Radiographers: 15
Rehired retired healthcare professionals
1
2
Medical Registration Ordinance(Cap. 161)
Dentists Registration Ordinance(Cap. 156)
Nurses Registration Ordinance(Cap. 164)
Midwives Registration Ordinance(Cap. 162)
Chinese Medicine Ordinance(Cap. 549)
Pharmacy and Poisons Ordinance(Cap. 138)
Supplementary Medical Professions
Ordinance(Cap. 359)
Chiropractors Registration Ordinance(Cap. 428)
Ordinances
Subsidiary Legislations
Nursing Council of Hong Kong
Medical Council of Hong Kong Dental Council of
Hong Kong
Midwives Council of Hong Kong
Chinese Medicine Council of Hong Kong
Pharmacy and Poisons Board of
Hong Kong
Physiotherapists Board
Occupational Therapists Board
Medical Laboratory Technologists Board
Optometrists Board
Radiographers Board
Chiropractors Council
Supplementary Medical
ProfessionsCouncil
FunctionsMaintain registers of healthcareprofessionalsMaintain professional standardsHandle complaints and take disciplinary actions as necessary against registered healthcare professionals
14 013Doctors+19.4%
424Dental Hygienists
+82.8%
52 389Nurses+43.8% 4 540
Midwives-2.3%
9 909CMPs
+21.4%2 659
Pharmacists +61.2%
1 911OTs
+56.0%2 956PTs
+45.3%3 443MLTs
+33.2%
2 180Optometrists
+13.2%
2 209Radiographers
+37.6%
209Chiropractors
+132.2%
2 441Dentists+23.3%
over99 000

Professional Development and Regulation
Professional Development and Regulation
Recommendations
UK
CanadaAustralia
NewZealand
Healthcare Manpower Planning
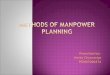
Recommendations Prevailing international trends
Lay participation rate :
Canada NewZealand
Australia UK
recognized list of qualifications(8 out of 11 jurisdictions)multiple pathways in UK and Australia e.g. specialist pathway; area of needs pathway; direct recognition of qualifications
50%33%
investigation
adjudication
More openness and accountability through greater involvement of lay persons in regulatory bodies
1
Mandatory continuing professional education / development has increasingly become the commonly accepted practice
2
Changes have been made to the investigatory and disciplinary functions to reduce conflict of interest. Investigation and adjudication functions are separated from regulatory bodies in some jurisdictions (e.g. UK and Australia)
3
Some jurisdictions are reviewing their measures in attracting healthcare graduates from abroad to help address short-term manpower shortages at home
4
Regulatory bodies usually operate on a self-financing basis through fees and charges paid by professionals
5
9 out of 11 jurisdictions require mandatory CPE/CPD
UK
CanadaAustralia
NewZealand
USUS
Findings at a glance
Manpower Projections
Shortage Sufficient ManpowerIf a shortage is likely to persist for a prolonged period, it is necessary to ensure a steady supply of healthcare professionals to join and serve in the public sector in the short and medium term, while waiting for the long-term measures to take effect
If sufficient manpower is expected for a particular profession, this may not necessarily call for supply adjustment. It may instead better enable us to plan for service enhancement and/or expansion
Considering to increase publicly-funded healthcare training places for disciplines facing manpower shortage
Publicly-fundedHealthcare Training
1
Self-financing Healthcare TrainingMaking better use of the self-financing sector, providing infrastructural and funding support and subsidising students to study specified self-financing healthcare programmes
2
Retaining existing healthcare professionals, attracting retired healthcare professionals to work in the public sector and recruiting non-locally trained doctors under limited registration more proactively
Healthcare Manpower in the Public Sector
3
Non-locally Trained Healthcare ProfessionalsUpholding professional standards, facilitating non-locally trained healthcare professionals to work in HK and strengthening publicity and recruitment efforts
4
Conducting manpower planning and projections once every three years
Healthcare Manpower Planning and Projections
5
Lay Involvement inBoards and CouncilsMaintaining a minimum lay membership of 25% in Boards and Councils
6
Continuing Professional Education / Continuing Professional DevelopmentUpkeeping professional competency by making continuing professional education and/or continuing professional development a mandatory requirement
7
Complaints Investigation and Disciplinary Inquiry MechanismImproving the mechanism for complaint investigation and disciplinary inquiry
8
Cost Recovery of the Operations of the Boards and CouncilsImproving cost recovery of the operations of Boards and Councils
9
Regulation of Healthcare Professions not subject to Statutory RegistrationIntroducing an accreditation scheme for healthcare professionals which are not subject to statutory registration
10
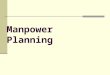
Demand – existing service levels and modelsSupply – current no. of training places
Assumptions:
Focus on the trend and credible interval rather than the absolute gapBase year is 2015, taking into account known shortage in the public and subvented sectors. Manpower demand projected through a sophisticated artificial intelligence computer model developed by HKU, having regard to demographic changes and known and planned services and developments
DoctorsShortage
DentistsShortage
Dental HygienistsShortage
PTsShortage
GeneralNurses
Shortage
OptometristsShortage
OTs Shortage
(Sufficient manpower after taking into account
Tung Wah College’s graduates)
MLTsSlight shortage but
close to equilibrium
RadiographersSlight shortage but
close to equilibrium
Pharmacists Sufficient Manpower
(Short term: slight shortage / close to
equilibrium)
Psychiatric NursesSufficient Manpower
(Short term: slight shortage / close to
equilibrium)
Chiropractors Sufficient Manpower
(Short term: slight shortage / close to
equilibrium)
CMPsSufficient Manpower
(Medium term: slight shortage / close to
equilibrium)