Embed Size (px)
Citation preview

Graefe's Arch C]in Exp Ophthalmol (1988)226:230-234 Graefe's Archive for Clinical and Experimental
Ophthalmology © Springer-Verlag 1988
Strabismus in craniofacial dysostosis* Jean D.A. Carruthers Clinical Associate Professor, Department of Ophthalmology, Associate Member, Department of Medical Genetics, University of British Columbia, Canada
Abstract. Ten infants and children who presented with cran- iofacial dysostosis are discussed; four had Apert's syn- drome, four had Crouzon's syndrome, one had Pfeiffer's syndrome, and one had hypertelorism. The follow-up of the patients ranged from 3 months to 7 years, with an aver- age of 19 months. Patients had bifrontal and biparietal craniectomies to correct frontal and temporal orbital retru- sion, while two had left unilateral procedures only. One patient (T.S.) had had three similar procedures before he was 3 years old and patient B.B. had two before he was 11 months old due to the complete failure of bony orbital growth. Before the cranial surgery, one patient had a preex- isting esotropia with bilateral congenital sixth nerve paresis, one had a V-pattern exotropia, and one had a right inter- mittent hypotropia due to right superior rectus weakness. In no case was there a change in the ocular alignment after infantile craniectomy. There were assorted ophthalmologic anomalies, such as congenital bilateral sixth nerve paresis, absent superior rectus function, bilateral ptosis in addition to absent superior rectus function, and two patients pre- sented with frank and repeated exorbitism.
Introduction
Craniofacial dysostosis is a collective term applying to ei- ther local or generalized anomalies in the development of the bones of the skull and orbit in which there is a prema- ture synostosis of suture lines. Premature closure of a crani- al suture results in inhibition of growth of the bone in a direction 90 degrees to the axis of the suture. The onset is presumably early in intrauterine life and in fact at concep- tion in those individuals in whom there is a positive family history. Normally the cranial sutures do not close perma- nently until adulthood [11].
Ocular features include horizontal and vertical strabis- mus, absent, bifid or anomalously inserted extraocular mus- cles, exorbitism, proptosis, corneal exposure, papilledema, and optic atrophy. Apert in 1906 [1] is credited with the first description of acrocephalosyndactyly as a separate dis- ease entity. Descriptions of variants of this were made by
* Dedicated to Dr. G.K. von Noorden on the occasion of his 60th birthday
Offprint requests to: J.D.A. Carruthers, Suite 210, 2730 Commer- cial Drive, Vancouver, B.C. V5N 5P4, Canada
Crouzon in 1912 [3], while Greig in 1924 described hyperte- lorism [7].
The first cranial surgical procedure addressing the prob- lem of severe craniofacial anomalies was designed in 1967 by P. Tessier in Paris [15], who used monoblock osteosto- mies to move the orbits sagitally and anteriorly with simul- taneous correction of the maxillary retrusion. This surgery used to be performed in older children and was like a mira- cle, making their appearance far more normal. In the past several years, an infantile craniectomy has been done in 3- to 4-month-old infants with the desired effect of encour- aging cranial and orbital growth early, to avoid the psycho- logical adaptation to the negative reaction of peers and others to the extreme craniofacial deformities. The surgery described here is jointly performed by a pediatric plastic surgeon and a neurosurgeon of the British Columbia Chip dren's Hospital Craniofacial Team. The technique has been described elsewhere [9].
Method
The patients reported here were sequentially referred by our team's pediatric plastic surgeon and neurosurgeon. All patients represented sporadic occurrence in their families.
All the children were assessed for visual acuity with the HTOV letter-matching test if old enough and by fixa- tion reflex to "central, steady, and maintained," if not. Stereopsis was tested with the Titmus or Lang test. Align- ment was measured in all positions of gaze at 1/3 m and 6 m using accommodation controlling targets. In the very young, fusion was assumed if there was no shift on alternate cover testing. In those patients with a short attention span, strabismus was evaluated using the Krimsky method.
Versions, ductions, and convergence were examined. The anterior segments of each globe were studied using the Kowa SL5 biomicroscope. All children had cycloplegic refraction and fundoscopy.
The case histories are summarized in Table 1.
Case history
Patient 6 (T.S.) was first seen at age 21/2 after three previous orbital advancements due to persistent complaints that "the left eye pops out." He had not received any treatment for his strabismus or exorbitism. In his general health he suf- fered from global developmental delay and growth retarda- tion. He had moderate bilateral hearing loss and was unable to walk because of a congenital hip deformity. There was

Table 1. Summary of 10 patients studied
Patient Diagnosis Ocular exam
231
1. Apert's syndrome A.A. 17/11/83 female
2. Crouzon's disease B.L. 23/7/80 female
3. Hypertelorism K.M. with left coronal synostosis 14/3/86 female
4. Premature left coronal synostosis C.R. with Crouzon's disease, 18/3/87 absent right superior female rectus function
5. Apert's syndrome K.A. 3/12/83 female
6. Pfeiffer's syndrome T.S. 3/11/83 male
7. Bilateral congenital ptosis, P.G. poor hearing, 6/5/81 delayed development male
8. Apert's syndrome R.K. 20/2/86 male
9. Apert's syndrome C.Y. 4/6/87 female
10. Crouzon's disease B.B. 30/11/86 male
10/25 right, 10/10 left, 200 s arc, V-pattern exotropia with bilateral inferior oblique overactions and superior oblique underaction, antimongoloid palpebral fissures
20/20 vision right and left, orthophoria in gaze positions, wide intercanthal distance
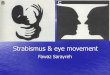
Constant left esotropia 20 prism diopters with bilateral sixth nerve paresis, left inferior oblique overaction and fine rotary congenital nystagmus; bilateral moderate hyperopia + 3.00/+ 0.75 x 90 right, + 4.00 diopters left. 11/2/87 recession of medial rectus of each eye 3 mm with bilateral inferior oblique myectomy, at surgery found to have a bifid right medial rectus (see Fig. 1)
Treatment, part-time patching of the left eye
V-pattern exotropia with inferior oblique overactions, fusing with chin-up compensatory head position 29/10/86 bilateral inferior oblique myectomy 7/1/87 bilateral lateral rectus recession with superoposition of the tendons by 1/2 tendon width
V-pattern exotropia with bilateral absent superior rectus function and left exorbitism with left corneal exposure despite left lateral tarsorrhaphy, 3 previous coronal synostosis repairs and craniectomies for orbital advancement, bilateral hearing loss, and congenital hip anomalies, in addition to congenital hydrocephalus with ventriculoperitoneal shunt
Monofixation right esotropia, bilateral ptosis with 3 mm levator action, and absent superior rectus function treated with bilateral lid slings
V-pattern exotropia with bilateral inferior oblique overaction and fusion in primary and downgaze, no exorbitism
Equal fixation, V-pattern exotropia with positive Bielschowsky head-tilt test left, moderate hyperopia, bilateral frontolateral and inferior wall advancement by craniectomy at age 4 months
V-pattern exotropia with bilateral superior and inferior rectus underactions with frank exorbitism on the left side with inferior corneal exposure and "intertrigo" between the palpebral and orbital portions of the lower left lid, in addition to the bilateral proptosis partially restrained with the bilateral tarsorrhaphy and intermittent pendular nystagmus; both fundi were completely normal; past medical history included two craniectomies and coronal orbital advancements, tracheostomy, two ventriculoperitoneal shunt revisions, and a persistent tracheostomy and gastrostomy
no family history o f any similar condit ion. On examinat ion he had an extremely short a t tent ion span, but was able to fixate and follow equally with each eye. He had marked oxycephaly and hydrocephalus with shallow orbits bilater- ally despite his three previous advancements. He had anti- mongoloid pa lpebra l apertures and had a V-pat tern exotro- pia which was variable but measured approximate ly 60 pr ismdiopters in upgaze, 30 in pr imary, and 10 in down- gaze. He had bilateral absent superior rectus function and Bell's phenomenon. Due to sleeping with both eyes wide open and despite the topical Dura tears ointment appl ied by his family, he developed a marked exposure kerati t is
on the left necessitating medical therapy with topical antibi- otics as well as a left lateral tarsorrhaphy. Despite the tar- sorrhaphy, the exorbit ism continues to be a persistent prob- lem. It was obvious at this t ime that a fourth orbi tal ad- vancement was indicated but the child was extremely ill und succumbed to pneumonia at age 3 pr ior to any defini- tive further therapy.
Incidence of strabismus
Nine of the 10 patients had strabismus in at least one field of gaze. Six patients had exotropia, 2 had esotropia, and

232
I had intermittent vertical strabismus. Of the two patients with esotropia, patient 7 had a monofixation esotropia and patient 3 had an esotropia due to congenital bilateral sixth nerve pareses. All but one of the patients with exotropia had a large V-pattern, with the exception of patient 1 who had monofixation exotropia. The incidence of exotropia was 66%, the esotropia 22%, and vertical strabismus 11%.
Incidence of V-pattern
Six of the 9 strabismus patients (66%) had a V-pattern. This is seen in 5 patients with exotropia and 1 with esotro- pia. All patients had marked bilateral inferior oblique over- actions, with the exception of patient 3 who with hyperte- lorism had only a moderate left inferior oblique overaction.
Absence of extraocular muscle function
Superior rectus dysfunction was seen in 4 of the 9 strabismic patients (44%) and lateral rectus dysfunction was seen in I of the 9 strabismic patients (11%). One patient, no. 10, had in addition apparent reduced inferior rectus ductions bilaterally.
Incidence of fusion
Sensory fusion was found in 3 out of 4 Apert's syndrome patients and 2 out of 4 Crouzon's patients. No patients appeared to be bifoveal. Testing with the Titmus test found two patients with Crouzon's disease with respectively 100 and 200 s arc of stereopsis and in 3 patients with Apert's disease, 200 s arc in two patients and 550 s arc in a third, but the latter measurement was on the Lang test as the child refused to wear the glasses for the Wirt. There appears to be motor fusion in patient 4 on cover testing, although the patient is too young to cooperate on sensory tests. This is also true of patients 3, 6, 9, and 10. It is therefore possible that the incidence is slightly higher were one able to obtain the information.
Incidence of surgical intervention
Strabismus surgical repair would have been indicated in 2 patients, no. 6 and no. 10, had they been well enough from a general point of view to undergo strabismus surgery. Two further patients had strabismus surgical repair. Pa- tient 3 with hypertelorism and bilateral congenital sixth nerve pareses had bilateral medial rectus recessions and in- ferior oblique myectomies. At surgery the main belly of the left medial rectus was found to insert 4.5 mm from the limbus and a second head inserted approximately 2.5 mm from the limbus (Fig. 1). Patient 5 with Apert's syn- drome had bilateral inferior oblique myectomies and subse- quent bilateral lateral rectus recessions with superoplace- merit of the insertions by one half tendon width. This pa- tient fused to 100 s in primary position and stopped needing to hold a chin-up compensatory head position for fusion. She subsequently had bilateral Tessier orbital translocations with no change in her alignment.
Discussion
The high incidence of exodeviations (66%) compared with 22% for esodeviation has not always been found in other
Fig. 1. Bifid right medial rectus in patient 3 with hypertelorism
series in the literature. Morax [12], in his examination of children with craniofacial dysostosis, found 9 patients with Crouzon's disease and 2 with Apert's syndrome; 8 of the Crouzon's patients (89%) had exotropia and the 2 with Apert's syndrome had esotropia. In contrast the Walker and Wybar series of 35 cases [16] found an equal incidence of eso- and exotropia, as did Nelson and coworkers in their Crouzon's syndrome patients [13]. There is therefore some variability in the literature as to the incidence of eso- and exotropia. In hypertelorism, Morax found a trend towards exodeviation but our one patient with hypertelorism was in fact esotropic due to bilateral congenital sixth nerve par- eses which antedated her cranial surgery.
Incidence of V-pattern
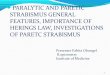
V-pattern was seen in 6 of 9 (66%) strabismic patients and in all cases was associated with an exodeviation with the exception of patient 3 with the esotropia and bilateral sixth nerve pareses. All affected patients except this one had ap- parent marked bilateral inferior oblique overaction. There seemed to be some variability in whether or not patients would have an associated positive Bielschowsky head-tilt test. The V-pattern is an extremely common association of strabismus in craniofacial dysostosis. Limon de Brown [8] found 100% of the V-phenomenon in 10 cases of oxyce- phaly and Crouzon's disease. It was less common in Walker and Wybar's series [16] at 70%, and in Nelson's series [13] the V-pattern was seen in 11 patients with Apert's syndrome of whom 6 had exotropia and 4 esotropia. Thus, the V- pattern can be associated with either eso or exo horizontal derivations. Limon de Brown has hypothesized that the high incidence of the V-pattern is due to the shallowness of the orbit in an anteroposterior direction causing an over- dependence of the globe on the inferior muscles associated with Lockwood's ligament. This results in an overaction of these inferior muscles, with secondary underaction of the superior oblique and superior rectus. Another theory that might possibly explain the V-pattern is that of anoma- lous biomechanical vectors for action of the superior ob- lique muscle, again due to anteroposterior orbital shallow- ness. The normal superior oblique tendon reflects at an

HYPOTHESIS PRIMARY S.O. UNDERACTiON
MECHANICAL ?. ANGULATION S.O. NOT 54
540 ~~
Fig. 2. Anteroposterior shallowness of orbit interferes with normal acute reflection of superior oblique tendon, thus reducing efficiency of superior oblique action, allowing overaction of ipsilateral inferi- or oblique, and causing a V-pattern
angle of 54 degees with the orbital axis [14]. Because of this shallowness, if the globe was situated relatively anterior in the orbit to the trochlea, there would perhaps be as great an angle as 90 degrees between the reflected part of the superior oblique tendon and its medial orbital wall compo- nent. This would mean there would be a great mechanical disadvantage to the superior oblique allowing a secondary overaction of the opposing inferior oblique and thus caus- ing the V-pattern (see Fig. 2).
Absence of superior rectus
Four of 9 (44.4%) strabismic patients had superior rectus dysfunction, 1 of 9 (11.1%) lateral rectus dysfunction and 1 of 9 (11.1%) inferior rectus dysfunction. Absence of supe- rior rectus was first described in craniofacial dysostosis by Weinstock and Hardesty [17]; subsequent authors have re- ported this manifestation in as many as one-third of the patients [4], while in another series it is slightly less frequent at 24% [13]. It is interesting to speculate about patient 7 who has Crouzon's disease and bilateral superior rectus dysfunction and complete bilateral ptosis. In this patient it is not difficult to conceive of a complete absence of meso- dermal development superiorly in both orbits. However, the incidence of ptosis in craniofacial dysostosis is low and it is difficult to understand, given that there is a common embryologic anlage for the levator and superior rectus mus- cle during the 22 to 30 mm stage of embryogenesis. Dia- mond and coworkers [6] have hypothesized a secondary atrophy or abiotrophy of the superior rectus muscles after levator muscle differentiation has occurred.
Incidence of fusion
Five of 9 strabismic patients and 6 of 10 patients studied had fusion when tested using the Titmus test and the Lang stereo test. The sensory adaptations in a large group of patients with craniofacial dysostosis were studied by Nel- son, Ingoglia, and Breinin in 1981 [13]. Fusion was obtained with bifoveal fusion in 7 out of 21 patients with Crouzon's syndrome, I out of 4 patients with Apert's syndrome, and in 2 out of 7 patients with Pfeiffer's syndrome. These au- thors found that " the ability of the cortex to function nor-
233
mally in response to normal disparity input, or to show the expected adaptations to altered visual input in these patients, is surprising when one considers how unlikely it is for the sensor motor system to escape unscathed." Their feeling was that these children should be treated like any other young patients with an infantile strabismus syndrome, including surgery prior to orbital surgery, in order to give them the best possible opportunity to develop fusion. This opinion has been echoed by Diamond and Whitaker [5].
Etiology of strabismus in craniofacial dysostosis
It would seem logical to postulate a multifactorial etiology for strabismus in craniofacial dysostosis, with mechanical factors perhaps being more important than innervational pattern. The mechanical factors would include the outward orientation of the orbital axes and the lack of inferior and lateral orbital support for the globe; structural anomalies of the extraocular muscles, both macro and microscopic, may also be important. Macroscopic anomalies would in- clude absent muscles such as absent superior rectus. Captuo and Lingua [2] have reported a bifid medial rectus insertion with anomalous insertions of the horizontal recti to within 2 to 3 mm of the limbus. In addition, anomalous dispropor- tion of orbit and globe and extraocular muscle length may cause anomalous vectors of action, as with the common V-pattern strabismus. Microscopic anomalies were found by Margolis et al. [10] on electron microscopic examination of an inferior oblique muscle in a patient with Apert 's syn- drome. Diamond et al. [6] support this with a report of 42% of a series of 36 patients having extraocular muscle anomalies including absent superior and inferior recti and superior oblique tendon.
Does orbital relocation alter coexisting strabismus or create new strabismus?
There has been controvery in the literature as to whether realignment of the visual axes results from major craniofa- cial reconstruction or not. Diamond and coworkers [6] stud- ied 140 children undergoing major craniofacial reconstruc- tion pre- and postoperatively. Only 10 had surgically in- duced alteration in their horizontal alignment in the prima- ry position, with 6 of the 10 being less than 10 prism diopters. Two out of 140 children had a new strabismus in the primary position created by the craniofacial surgery and both of these were due to cranial nerve palsies. In the European literature there has been a similar opinion, with the exception that in hypertelorism in Walker and Wybar's series [16] one case of esotropia was found preoper- atively in hypertelorism and 9 were found afterwards. These appear to be related largely to sixth nerve pareses, presum- ably also due to subperiosteal dissection of the orbital wall. Although the sixth nerve paresis may resolve spontaneously postoperatively in some patients, the esodeviation remained and became a concomitant deviation requiring a subsequent strabismus repair. In the French literature, Morax [12] also has described an eso trend in the postoperative period after Tessier monoblock osteotomy for hypertelorism repair. In- terestingly, 10 out of the 12 patients with hypertelorism de- veloped a vertical deviation postoperatively with a V-syn- drome with bilateral superor oblique weakness and excyclo- torsion presumably related to the surgical treatment of the trochlea. This experience was similar to that of the Philadel-

234
phia group, described by Diamond and coworkers [5], who noted a great variability in the superior oblique pareses. These could vary from frank compensatory head tilt to- wards the opposite shoulder to hypertropia of the involved eye, but more commonly presented as an overelevation in adduction with a V-pattern. Possibly a more stringent ap- proach to the reattachment o f the trochlea at the time of orbital and cranial surgical repair might preclude the high incidence o f this problem.
Exorbitism
Twenty years ago Tessier [14] coined the term exorbitism to mean the spontaneous and involuntary extrusion of the globe from the orbit. This was a major problem in patient 6 and there was concern that any further reduction in relative orbital growth would result in complete corneal exposure. Only patients 6 and patient 10, who both had had multiple orbital advancements without permanent effect, required tarsorrhaphies. The presence o f persistent exorbitism and persistent nonresponse to multiple orbital advancements seems to be associated with those patients with a much poorer general prognosis.
Conclusions
Ten consecutive patients with craniosynostosis were evalu- ated for sensorimotor disturbances and related ocular find- ings. Four patients each of Apert 's syndrome and Crou- zon's syndrome, one with Pfeiffer's syndrome, and one with hypertelorism were examined. Ninety percent o f the pa- tients had strabismus and 66% of the strabismic patients had a V-pattern. Superior rectus dysfunction was seen in 44% of the strabismic patients, lateral rectus dysfunction in 11%, and inferior rectus dysfunction in 11%. Three o f four Apert 's patients and two of four Crouzon 's patients showed peripheral fusion (50% of patients studied to date).
Although strabismus may be a small part of the total syndrome, management as for any other infantile strabis- mus patient will give the most favorable outcome with re- gard to sensory fusion. With the exception of orbital trans- location repair for hypertelorism, infantile craniectomy and Tessier orbital relocations do not commonly appear to
create new strabismus. Thus, treatment of strabismus can be based on common principles o f infantile strabismus man- agement rather than planning around the timing of orbital relocations.
References
1. Apert ME (1906) De L'acrocephalosyndactyly. Bull Soc Mem Hop Paris 23:1310
2. Captuo AR, Lingua RW (1980) Aberrant muscle insertions in Crouzon's disease. J Pediatr Ophthalmol Strabismus 17 : 239-241
3. Crouzon MO (1912) Dysostosis craniofaciale hereditaire. Presse Med 73 : 737
4. Cultore J, Bragis P, Miller M, Folk S (1979) Absence of the superior rectus muscle in Apert's syndrome. J Pediatr Ophthal- mol Strabismus 16:349
5. Diamond G, Whitaker L (1984) Ocular motility in craniofacial reconstruction. Plast Reconstr Surg 73:31-35
6. Diamond LR, Katowitz JA, Whitaker LA, Quinn GE, Schaffer DB (1980) Variations in extraocular muscle number and struc- ture in craniofacial dysostosis. Am J Ophthalmol 90:416418
7. Greig DM (1924) Hypertelorism: A hitherto undifferentiated craniofacial deformity. Edinburgh Med J 31:560-593
8. Limon de Brown E 0974) Strabismus in Crouzon's disease. Trans Int Strabismol Assoc 2nd meeting, Marseilles, pp 192- 198
9. Marchek D, Renier D (1982) Craniofacial surgery for cranial synostosis. Little Brown, Boston
10. Margolis S, Pachter BR, Breinin GM (1977) Structural alter- ations of extraocular muscle associated with Apert's syndrome. Br J Ophthalmol 61:683
11. Miller M, Folk E (1975) Strabismus associated with craniofa- cial anomalies. Am Orthopt J 25:27
12. Morax S (1984) Change in eye position after craniofacial sur- gery. J Maxillofac Surg 12:47-55
13. Nelson LB, Ingoglia, Breinin GM (1981) Sensorimotor distur- bances in craniodysostosis. J Pediatr Ophthalmol Strabismus 18 : 32-41
14. Noorden GK yon (1977) Arias of strabismus, 3rd edn. Mosby, St Louis
15. Tessier P (1967) Entretiens sur la chirurgie orbito-cranienne. Ann Chir Plast Esthet 12:273
16. Walker J, Wybar K (1966) Ocular motility problems in cranio- facial dysostosis. In: Moore S, Stockbridge L (eds) Orthoptics, past, present, future. Stratton, Intercontinental Medical, New York, pp 299-310
17. Weinstock FJ, Hardesty HH (1965) Absence of superior recti in craniofacial dysostosis. Arch Ophthalmol 74:152