Embed Size (px)
Citation preview

Stimulating PCOS Patients
Undergoing IVF
Peter Casson MD
Reproductive Endocrinologyand Infertility
Northeastern Reproductive MedicineColchester, Vermont

Definition of PCOS

PCOS: Causes and
PrevalenceGenetic
Steroid biosynthetic enzymes
Androgen receptor
Insulin receptor
Associated with Family history of NIDDM
Insulin resistance (50%)
Obesity
Prevalence increasing 10-20% of women of
reproductive age
30% of infertile patients

PCOS: Traditional Ovulation
Induction Getting better but not perfect (Legro, NEJM, 2014)
Predictors of failure:
BMI
Hyperinsulinemia
High AMH
Hyperandrogenemia
Letrozole
Clomiphene

Reasons to Move On To IVF
in PCOS Patients
Failed ovulation
Ovulation but no pregnancy ( usually after IUI)
Advancing reproductive age
Other concurrent infertility factors
Concurrent PGS/PGD

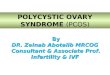
Prevalence OF PCOS in IVF
0
2
4
6
8
10
12
14
16
2005 2006 2007 2008 2009 2010 2011 2012 2013
Ovulatory dysfunction (%)
CDC SART Data

IVF Stimulation in PCOS
Patients: Problems Tough to monitor
Overly vigorous stimulations
Tough retrievals
Variable oocyte quality
? Decreased fertilization rate
OHSS

Strategies to Improve IVF
Stimulations/Outcomes in PCOS
Patients
Metformin
ICSI
IVM
Coasting
Cabergoline
Antagonist cycles
Agonist trigger
Freeze all cycles
Agonist trigger/freeze all cycle

ARS Question 1
I use metformin as an adjunct to IVF in
PCOS patients:
a. in all PCOS patients
b. in lean PCOS patients
c. when there is evidence of
hyperinsulinemia
d. only if the patient has failed a previous
IVF cycle

Metformin: Evidence for a Beneficial
Effect in Ovulation Induction
Small RCTs in POCS patient undergoing hMG ovulation induction
Decreased OHSS, multiple pregnancy, hMG utilization• Yarali Hum Reprod 17(2) 2002
• Tadesmir Arch Gynecol Obstet 269, 2004
Increases mono-ovulatory follicle development• Palomba Hum Reprod 20(10), 2005
Decreased miscarriage rate
Two non-randomized studies demonstrate >50% decrease in first trimester miscarriage in PCO patients
• Jakubowitz JCEM 87(2), 2002
• Glueck, Fertil Steril 75, 2001

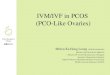
PPCOS I: Metformin is Not as
Effective as Clomiphene
P-value: <0.001
ClomipheneMetforminCombined
Rate of Live Birth
0.0
0.1
0.2
0.3
0.4
0.5
Days from Randomization to Live Birth150 200 250 300 350 400 450 500
Legro, NEJM, 2007

Meta analysis of 9 RCTs
Clinical pregnancy rate higher (OR 1.52, 1.07 to 2.15)
70 % reduction in OHSS (OR 0.29, 0.18 to 0.49)• Tso, Cochrane Database Syst Rev 2014
• Tso Fertil Steril, Sept 2015
Metformin in PCOS/IVF

Metformin in POCS/IVF
WHO Guidelines:
“Metfomin useful to reduce the risk of OHSS”• Balen, Hum Reprod Update August 2016
BFS Guidelines:
“has a positive effect in women with PCOS undergoing IVF”
• Nardo, Hum Fertil 18(1) 2015
SOGC Guideline:
“The addition of metformin should be considered in patients with PCOS undergoing IVF because it may reduce the incidence of OHSS”
• SOGC guideline 315, November 2014

Possible indications for
Metformin use in PCOS/IVF
Indications:
Multiple pregnancy losses
Poor oocyte quality/failed cycle
Lean PCOS
Evidence of insulin resistance
OR
Anyone with clinically diagnosed PCOS

ARS Question 2
I use ICSI in PCOS cycles:
a. in all PCOS/IVF cycles
b. in nulligravid PCOS patients only
c. only when there is concurrent
hyperinsulinemia
d. only when other concurrent indications
for ICSI exist (male factor, failed
fertilization, PGS/PGD)

ICSI in PCO/IVF
Fertilization rate reported lower in patients with PCOS at IVF
Sibling oocyte study (PCO, normal sperm)
1089 oocytes from 60 cycles randomized to ICSI or standard IVF
Higher fertilization rate (72% vs. 45%), lower total fertilization failure (0% vs. 15%)
• Hwang, Hum Reprod 20(5), 2005
No Randomized controlled trials

ICSI Use 2004-2013
SART CDC 201336% to 76% of all IVF cycles from 1996 to 2013

Is ISCI Overused? SART CDC Data
ICSI/Unexplained infertility (n = 317 996)
Lower implantation (23.0% vs 25.2%, RR, 0.93; 95%, 0.91-0.95)
Lower live birth (36.5% vs 39.2%, RR, 0.95; 95% CI, 0.93-0.97)
Boulet JAMA, 313(3), 2015

ICSI in PCOS/IVF:
Recommendation
Use ICSI only if clear indication
Male
Previous failed/suboptimal fertilization
PGS/PGD
? Less than 4 oocytes
OR
Split cycles to see which is better in your lab

ARS Question 3To reduce the risk of hyper stimulation in PCOS
patients being stimulated for IVF, I use:
a. coasting
b. In Vitro maturation
c. low dose hCG trigger (+/-cabergoline)
d. lupron trigger and freeze all

IVM at IVF
Retrieval of immature (GV) oocyte-cumulus complexes from follicles <13 mm with or without a short course of rFSH or hCG priming
In vitro culture with added hCG, FSH for up to 3 days
Used in patients at risk for OHSS and fertility preservation
Faster, less expensive, works best in PCOS patients
No OHSS
Lower pregnancy rates than standard IVF

IVM Exists on a Continuum
ICSI of Immature GV and MI oocytes that matured in vitro on day 1 or 2
Recovery and IVM of immature oocytes in a early–triggered PCO/IVF cycle
Traditional IVM

IVM in PCOS: Conclusions
Requires special expertise
Effective in reducing OHSS but pregnancy rates are lower
Largely superseded by other techniques to avoid OHSS
Variations of IVM may still be useful to maximize embryo yield from immature oocytes obtained at a PCO/IVF retrieval

Coasting
First described by Sher 199
Withholding gonadotropins/hCGtrigger until E2 falls below a threshold level (3,000-5000 pg/ml)
Larger follicles have less FSH requirement, leads to atresia of smaller follicles, less VEGF production
Need to push stimulation until follicles >12-15 mm

Coasting: Results
Oocyte numbers, fertilization, embryo
development and pregnancy rates not
adversely affected
OHSS rate reduced to 2.5%• Delvigne A, Hum Reprod 16:2491, 2001
Coasting has adverse effect if > 3 days• Mansour R Hum Reprod 20, 2005

Stimulation Tricks That Don’t Work
to Reduce the Incidence of OHSS
rFSH vs hMG
hCG vs rLH
10,000 vs 5,000 IU hCG trigger

Cabergoline For OHSS
Dopamine agonists decrease VEGF
production of granulosa cells in Vitro • Ferrero Repro Bio endocr 2015
60-70% reduction in mild and moderate
OHSS• Cochrane 2012 (2 RCTs)
Meta analysis of 7 studies, 858 women:
60% reduction in moderate and severe
OHSS• Leitao Fert Steril 2014
No reduction of pregnancy rate in either analysis

Cabergoline to Prevent OHSS:
0.25 to 0.5 mg daily for 8 days to 3 weeks
Starting at hCG trigger or oocyte retrieval
Often given in conjunction with albumin at retrieval
Done with freeze all or through the first week of
pregnancy

Antagonist Protocols For OHSS
Prevention
Meta analysis of 29 RCTs
Antagonist cycles reduce the risk of OHSS (OR 0.43, 0.33-
0.57)
No difference in pregnancy and live birth• Al-Inany HG Cochrane Database Syst Review 111(5) 2011
Allows for the use of an agonist trigger

Agonist trigger
Pulse of agonist displaces antagonist off GnRH receptors, stimulates endogenous surge of LH/FSH
3-5 mg leuprolide or 0.2 to 0.5mg leuprelin/triptorlin/buserelin 36-40 and again 24 -26 hours before retrieval
Meta analysis of 17 RCTs:
Reduction of OHSS (OR 0.15, 0.05-0.47)
Reduction in live birth rate (OR 0.47, 0.31-0.70)
Higher miscarriage rate (OR 1.74, 1.1-2.75)
No change in pregnancy rate in donor-recipient cyclesYouseff M, Cochrane database syst rev Oct 2014

Agonist Trigger Problems
Lower pregnancy rates in fresh autologous cycles
Freeze all
Intensive luteal supplementation
E, P, supplemental hCG at retrieval or in luteal phase
2% failure rate- no eggs!
Risk factors: prolonged OCP use, hypothalamic anovulation
Check LH, progesterone day after trigger
retrigger if LH <15, reassuring if LH >50
hCG co-trigger (1000-5000 iu hCG)

Freeze all For OHSS Prevention
Demonstrated in 1999 RCT that elective freeze all in at-
risk patients reduced OHSS risk, no difference in
pregnancy rates• Ferraretti, Hum Rep 1999
Problems:
FET rates typically not as high as fresh ETs
Added cost (financial and emotional)
More time commitment
Can still see severe OHSS with no embryo transfer (ie donor
cycles)

Freeze All Vs. Fresh ET in PCOS IVF
Chen et al, NEJM 375(6), 2016
RCT of 1508 PCO patients undergoing IVF (+/- ICSI)
Agonist Stimulation, hCG trigger (4000-8000 IU)
IM Progesterone 80 mg/day for luteal support
Fresh or Frozen ET of 1or 2 day three embryos
Primary outcome live birth
Secondary outcomes:
Clinical pregnancy
Pregnancy loss
OHSS
Intent to treat analysis

Fresh Vs. Freeze All in PCOS/IVF:
Results
Fresh Transfer
(762)
Freeze All
(746)
P Value
Live Birth 42% 49.3% 0.004
Clinical
Pregnancy
56.2% 58.7% 0.32
Loss Rate 25% 14.6% <0.001
Birth Weight,
gr. (singleton)
3349 +/- 553 3511+/-594 0.005
Mod or Severe
OHSS
7.1% 1.3% <0.001
Preeclampsia 1.4% 4.4% 0.009
Chen, NEJM 375(6), 2016

Agonist trigger/Freeze all in PCO
Pros:
Avoid hyperstimulation
Get more eggs
Accrue benefits of FET:
Reduced prematurity, birth defects
Cons:
Can only do if your FET as good as your fresh rate
Additional cost, time, expense
More meds

Optimizing PCOS/IVF Stimulations Metformin reduces OHSS (may improve preg rate)
ICSI not needed (individualize)
Changing gonadotropin, decreasing hCG trigger
has no clear benefit
IVM may help, but requires special expertise
Coasting reduces but does not eliminate OHSS
Cabergoline likely reduces OHSS 60%
antagonist cycles reduce OHSS 50 %
Agonist triggers reduce OHSS 80%
Freeze-all cycles reduce but does not preclude
OHSS
Agonist trigger/freeze all cycles most effective
modality