Embed Size (px)
Citation preview
1
AAPM 2007 Annual Meeting, Minnea polis , MinnesotaTherapy Continuing Education CourseWednes day, July 25, 2007; 7:30-8:25 am, Bal lro om B
Stereotacti c Bod y Radiat ion Therapy:Part 1. Clin ical and Bio log ical Finding s
Brian D. Kavanagh, MD, MPHDepartment of Radiation Oncology
University of ColoradoComprehensive Cancer Center
Stereotactic Body Radia tion Therapy :Part 1. Clinical and Biologica l Findings
Educational Objectives
1. To present the operational definition of SBRT
2. To present the clinical rationale for theapplication of SBRT in the most commonly usedindications
3. To review reported clinical outcomes datafor SBRT, with discussion of the practicalradiobiological ramifications
I hope this is where we are with SBRT…[insert gratuitous puppy photos here]
Stereotactic Body Radia tion Therapy :Part 1. Clinical and Biologica l Findings
Educational Objectives
1. To present the operational definition of SBRT
2. To present the clinical rationale for theapplication of SBRT in the most commonly usedindications
3. To review reported clinical outcomes datafor SBRT, with discussion of the practicalradiobiological ramifications
2
SBRT is a treatment that couples a high degree of anatomictargeting accuracy and reproducibility with very high doses ofextremely precise, externally generated, ionizing radiation,thereby maximizing the cell-killing effect on the target(s) whileminimizing radiation-related injury in adjacent normal tissues.
ASTRO SBRT PolicyDefinition, continued
• “stereotactic” implies target localization relative to 3-Dcoordinates– eg a body frame with external reference markers, implanted
fiducial markers that can be visualized with kV x-rays, and CTimaging-based systems
• All SBRT is performed with IGRT of some kind– To minimize breathing-related or other intra-treatment tumor
motion, some form of motion control or “gating” may be used
• SBRT may be fractionated (up to 5 fractions)– Each fraction requires an identical degree of precision,
localization and image guidance– A course of treatment >5 fractions is not considered SBRT
King Tut
ASTRO SBRT PolicyDefinition, continued:the fuzzy parts…
• The border/overlap withcranial SRS
– Base of skull region– Nasopharynx– Paranasal sinuses– Note: SRS can be up to 5
fractions, also
• Is there a minimum dosefor SBRT?
Stereotactic Body Radia tion Therapy :Part 1. Clinical and Biologica l Findings
Educational Objectives
1. To present the operational definition of SBRT
2. To present the clinical rationale for theapplication of SBRT in the most commonly usedindications
3. To review reported clinical outcomes datafor SBRT, with discussion of the practicalradiobiological ramifications
3
Spectrum of potential indications for SBRT
• Intensified treatment to a primary cancer– Stage I lung cancer
• Best studied to date– Primary HCC– Pancreas cancer– Prostate cancer
• Favorable due to low alpha/beta ratio• Treatment of selected spinal/paraspinal lesions• Palliation for challenging sites of recurrence
– Retroperitoneal– Previously irradiated volumes
• Adjuvant systemic cytoreductive therapy– “Radical” treatment for isolated liver, lung, and other mets
Spectrum of potential indications for SBRT
• Intensified treatment to a primary cancer– Stage I lung cancer
• Best studied to date– Primary HCC– Pancreas cancer– Prostate cancer
• Favorable due to low alpha/beta ratio• Treatment of selected spinal/paraspinal lesions• Palliation for challenging sites of recurrence
– Retroperitoneal– Previously irradiated volumes
• Adjuvant systemic cytoreductive therapy– “Radical” treatment for isolated liver, lung, and other mets
Why SBRT for medically inoperableearly stage NSCLC?
• Conventional RT results generallyunderwhelming– 50+% local failure– 30% or less 3-5 yr disease-specific survival
• SBRT might allow higher doses– Careful delivery technique– Biologically more potent…
So why do we think SBRT is biologicallymore potent?…and a quick caveat, before we overestimate…
Fowler JF, Tome WA, Welsh JS. In Stereotactic Body RadiationTherapy, Lippincott Williams & Wilkins, 2005.
dndBED 1
Where
n = number of fractions
d = dose per fraction
/ = tissue characteristicNote:
MODELS LOOK GOOD ON PARISIAN
RUNWAYS, BUT THIS BATTLE IS
RADIATION versus CANCER AND NOT
RALPH LAUREN versus CALVIN KLEIN!

4
Prospective Trials of SBRT for Stage I NSCLC
2 yr local control 88%37.5 Gy/3-5 fractions
68
Technical University, Munich
1 yr local control 94%30 Gy/1 fraction33
University of Marburg
1 yr local control 98%60 Gy/3 fractions70
Radiation Therapy Oncology Group (RTOG) 0236
1 yr local control 95%50 Gy/10 fractions43
Air Force General Hospital, Beijing
2 yr local control 95%48 Gy/4 fractions45
Kyoto University2 yr local control 85%45 Gy/3 fractions4
0Aarhus University
1 yr local control 98%60-66 Gy/3 fractions
70
Indiana University
Phase I study; maximum tolerated dose (MTD) not reached for T1 lesions; MTD 66 Gy for T2 lesions
24-66 Gy/3 fractions
47
Indiana University
ResultsSBRT dose and fractionation
NInstitution
Example case:T1N0 medically inoperable lung cancer
• 52-year-old male, h/oemphysema, on 3-5 L/minsupplemental O2
– 70 pack-yr smoker
• CT in 2003 revealed LUL lesion(?)
– Repeat CT 3 mos later showedenlargement of the left upper lobenodule, up to 1.5 x 2 cm
• Biopsy: adenocarcinoma
• FEV1 0.9 L (28% of predicted)
Treatment: 60 Gy/3 fractions Characteristic radiographic findings
baseline
4 mos, CR8 mos,soft tissuewindow
12 mos,lungwindow 18 mos, NED
5
Summary of forthcoming RTOGtrials of SBRT for lung cancer
• RTOG 0618 (R Timmerman):– SBRT for Medically Operable NSCLC– Still a potential inhomogeneity correction snag
• RTOG 0624/NCCTG (B Kavanagh, PI) ?????:– SBRT (60 Gy/3) v another fractionation
schedule?
• RTOG 0633 ( A Bejzak, PI):– SBRT for Pulmonary lesions near the proximal
bronchial tree
• RTOG 06xx (V Stieber, PI):– SBRT for Pulmonary Metastases
Spectrum of potential indications for SBRT
• Intensified treatment to a primary cancer– Stage I lung cancer
• Best studied to date– Primary HCC– Pancreas cancer– Prostate cancer
• Favorable due to low alpha/beta ratio• Treatment of selected spinal/paraspinal lesions• Palliation for challenging sites of recurrence
– Retroperitoneal– Previously irradiated volumes
• Adjuvant systemic cytoreductive therapy– “Radical” treatment for isolated liver, lung, and other mets
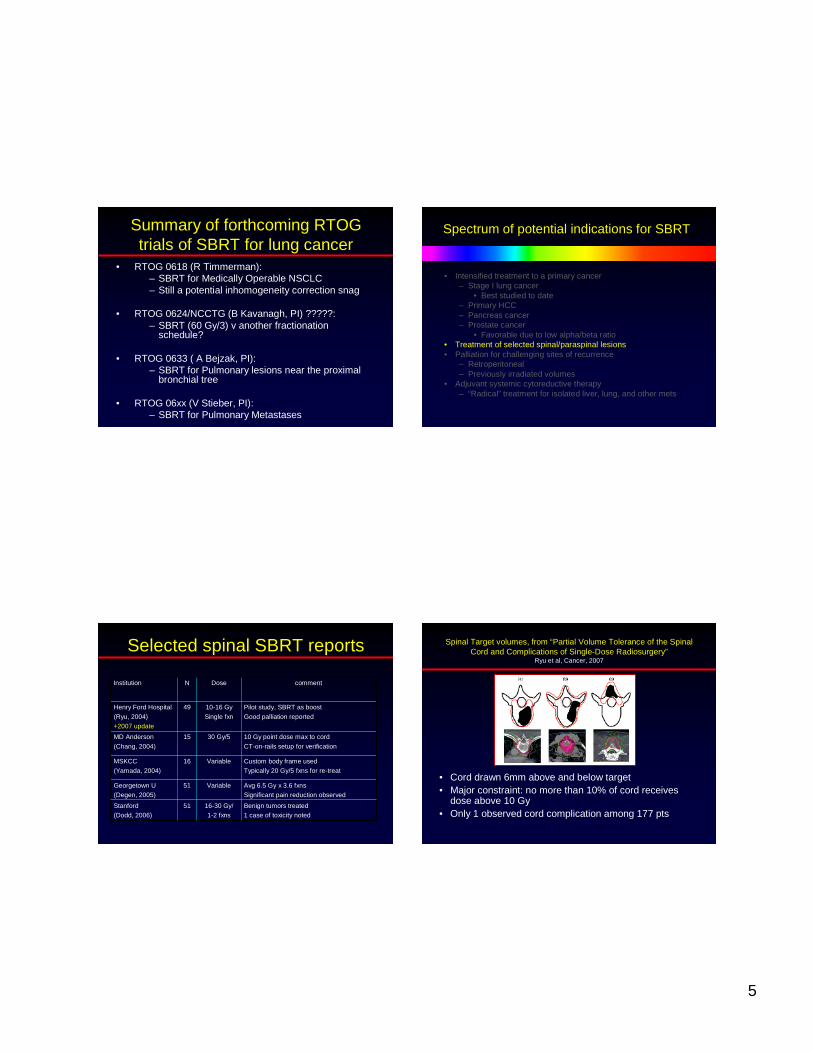
Selected spinal SBRT reports
Avg 6.5 Gy x 3.6 fxnsSignificant pain reduction observed
Variable51Georgetown U(Degen, 2005)
Benign tumors treated1 case of toxicity noted
16-30 Gy/1-2 fxns
51Stanford(Dodd, 2006)
Custom body frame usedTypically 20 Gy/5 fxns for re-treat
Variable16MSKCC(Yamada, 2004)
10 Gy point dose max to cord
CT-on-rails setup for verification
30 Gy/515MD Anderson
(Chang, 2004)
Pilot study, SBRT as boost
Good palliation reported
10-16 Gy
Single fxn
49Henry Ford Hospital
(Ryu, 2004)+2007 update
commentDoseNInstitution
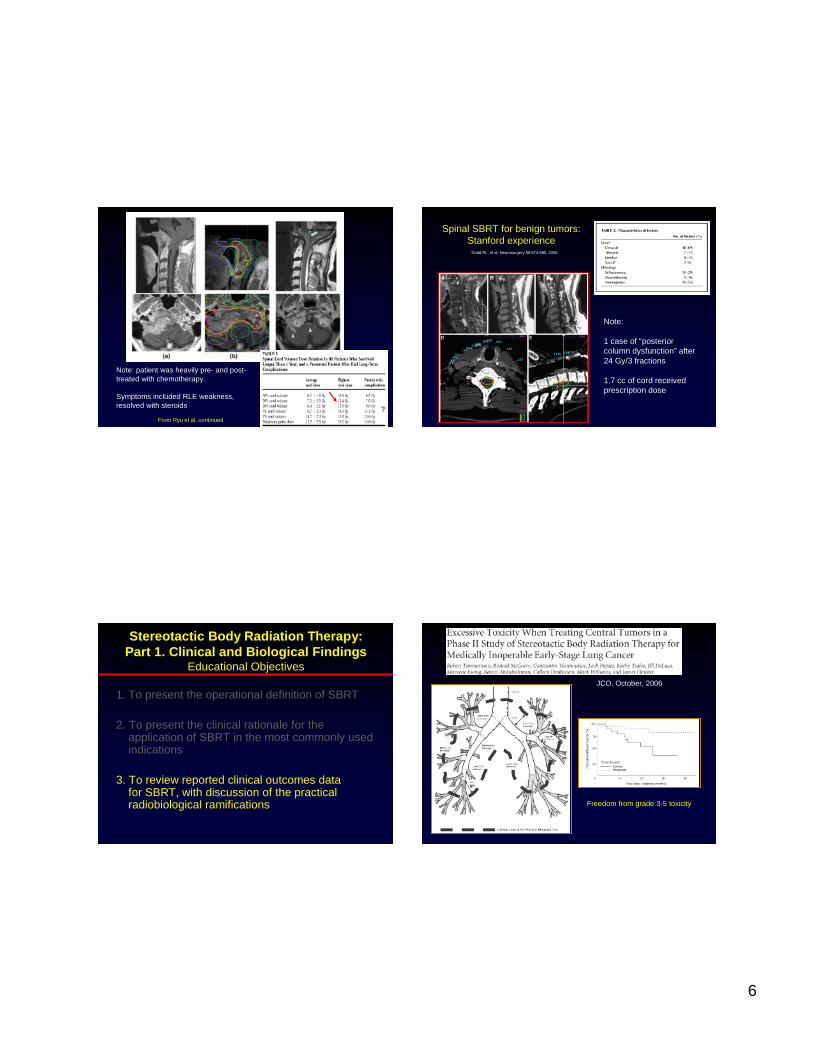
Spinal Target volumes, from “Partial Volume Tolerance of the SpinalCord and Complications of Single-Dose Radiosurgery”
Ryu et al, Cancer, 2007
• Cord drawn 6mm above and below target• Major constraint: no more than 10% of cord receives
dose above 10 Gy• Only 1 observed cord complication among 177 pts
6
From Ryu et al, continued
Note: patient was heavily pre- and post-treated with chemotherapy.
Symptoms included RLE weakness,resolved with steroids ?
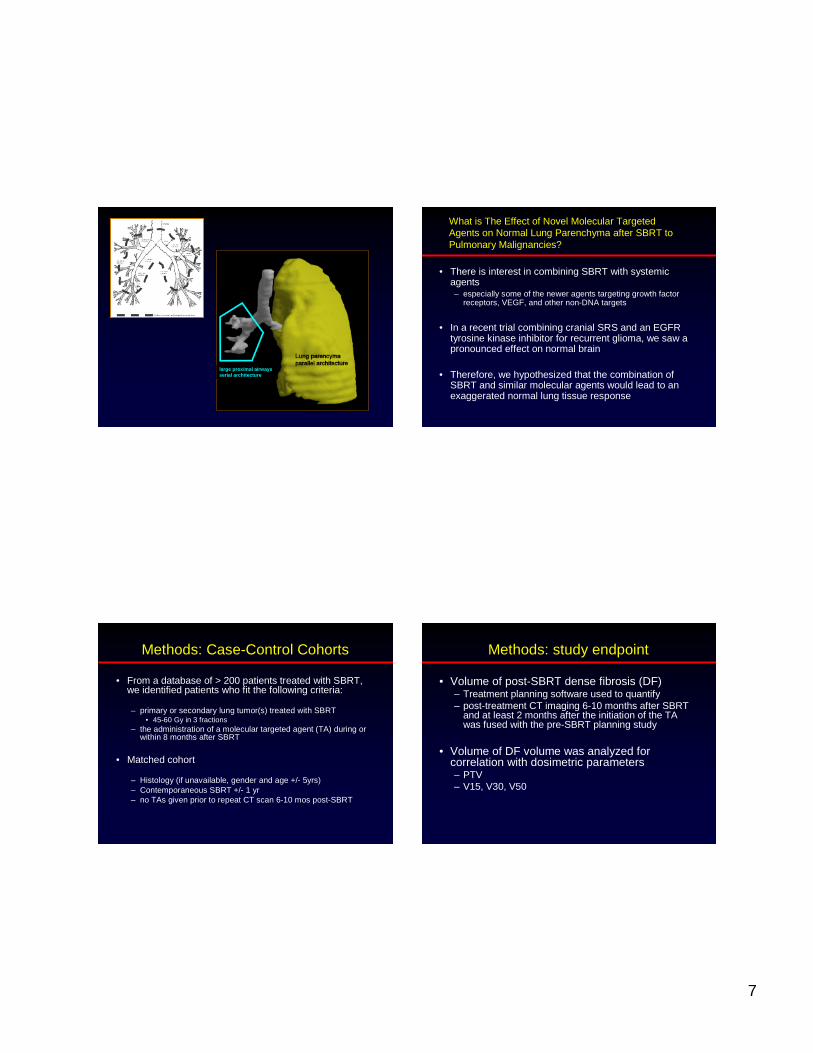
Dodd RL, et al. Neurosurgery 58:674-685, 2006
Spinal SBRT for benign tumors:Stanford experience
Note:
1 case of “posteriorcolumn dysfunction” after24 Gy/3 fractions
1.7 cc of cord receivedprescription dose
Stereotac tic Body Radiation Therapy:Part 1. Clinical and Biolo gical Finding s
Educational Objectives
1. To present the operational definition of SBRT
2. To present the clinical rationale for theapplication of SBRT in the most commonly usedindications
3. To review reported clinical outcomes datafor SBRT, with discussion of the practicalradiobiological ramifications
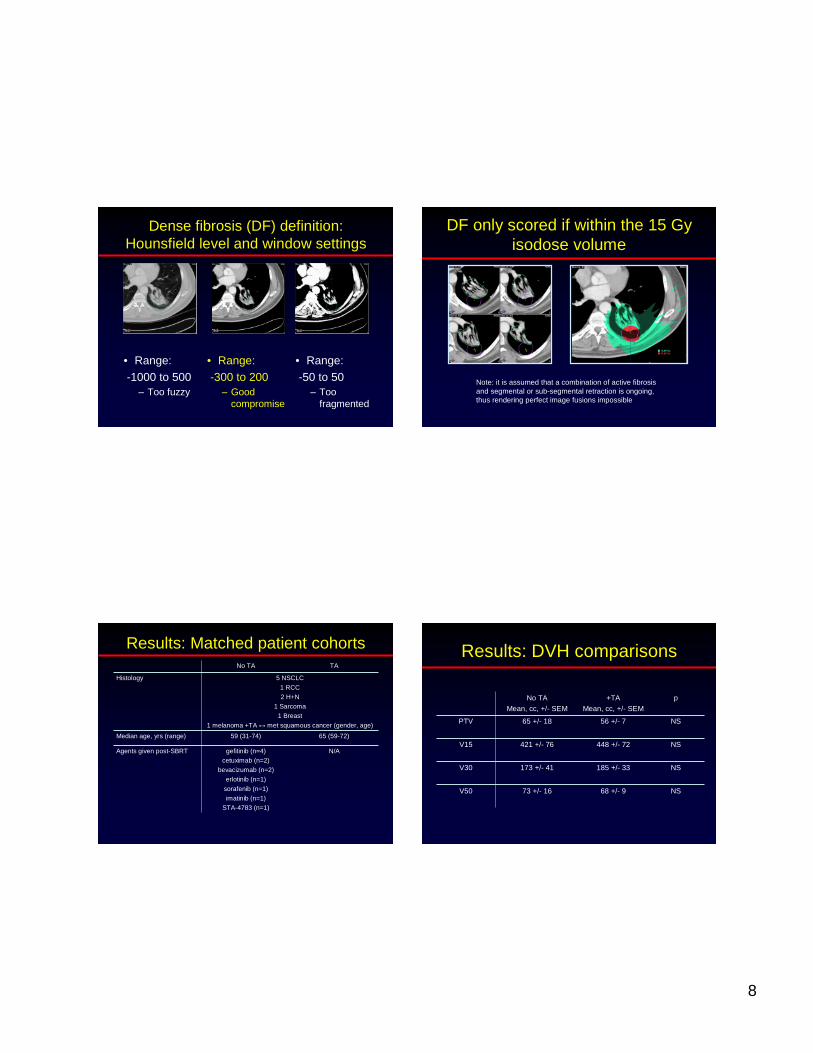
JCO, October, 2006
Freedom from grade 3-5 toxicity
7
large proximal airwaysserial archit ecture
What is The Effect of Novel Molecular TargetedAgents on Normal Lung Parenchyma after SBRT toPulmonary Malignancies?
• There is interest in combining SBRT with systemicagents– especially some of the newer agents targeting growth factor
receptors, VEGF, and other non-DNA targets
• In a recent trial combining cranial SRS and an EGFRtyrosine kinase inhibitor for recurrent glioma, we saw apronounced effect on normal brain
• Therefore, we hypothesized that the combination ofSBRT and similar molecular agents would lead to anexaggerated normal lung tissue response
• From a database of > 200 patients treated with SBRT,we identified patients who fit the following criteria:
– primary or secondary lung tumor(s) treated with SBRT• 45-60 Gy in 3 fractions
– the administration of a molecular targeted agent (TA) during orwithin 8 months after SBRT
• Matched cohort
– Histology (if unavailable, gender and age +/- 5yrs)– Contemporaneous SBRT +/- 1 yr– no TAs given prior to repeat CT scan 6-10 mos post-SBRT
Methods: Case-Control Cohorts
• Volume of post-SBRT dense fibrosis (DF)– Treatment planning software used to quantify– post-treatment CT imaging 6-10 months after SBRT
and at least 2 months after the initiation of the TAwas fused with the pre-SBRT planning study
• Volume of DF volume was analyzed forcorrelation with dosimetric parameters– PTV– V15, V30, V50
Methods: study endpoint
8
Dense fibrosis (DF) definition:Hounsfield level and window settings
• Range:-1000 to 500
– Too fuzzy
• Range:-50 to 50
– Toofragmented
• Range:-300 to 200
– Goodcompromise
DF only scored if within the 15 Gyisodose volume
Note: it is assumed that a combination of active fibrosisand segmental or sub-segmental retraction is ongoing,thus rendering perfect image fusions impossible
Results: Matched patient cohorts
N/Agefitinib (n=4)cetuximab (n=2)
bevacizumab (n=2)erlotinib (n=1)
sorafenib (n=1)imatinib (n=1)
STA-4783 (n=1)
Agents given post-SBRT
65 (59-72)59 (31-74)Median age, yrs (range)
5 NSCLC
1 RCC2 H+N
1 Sarcoma1 Breast
1 melanoma +TA ↔ met squamous cancer (gender, age)
Histology
TANo TA
Results: DVH comparisons
NS56 +/- 765 +/- 18PTV
68 +/- 9
185 +/- 33
448 +/- 72
+TA
Mean, cc, +/- SEM
NS421 +/- 76V15
NS173 +/- 41V30
NS73 +/- 16V50
pNo TA
Mean, cc, +/- SEM
9
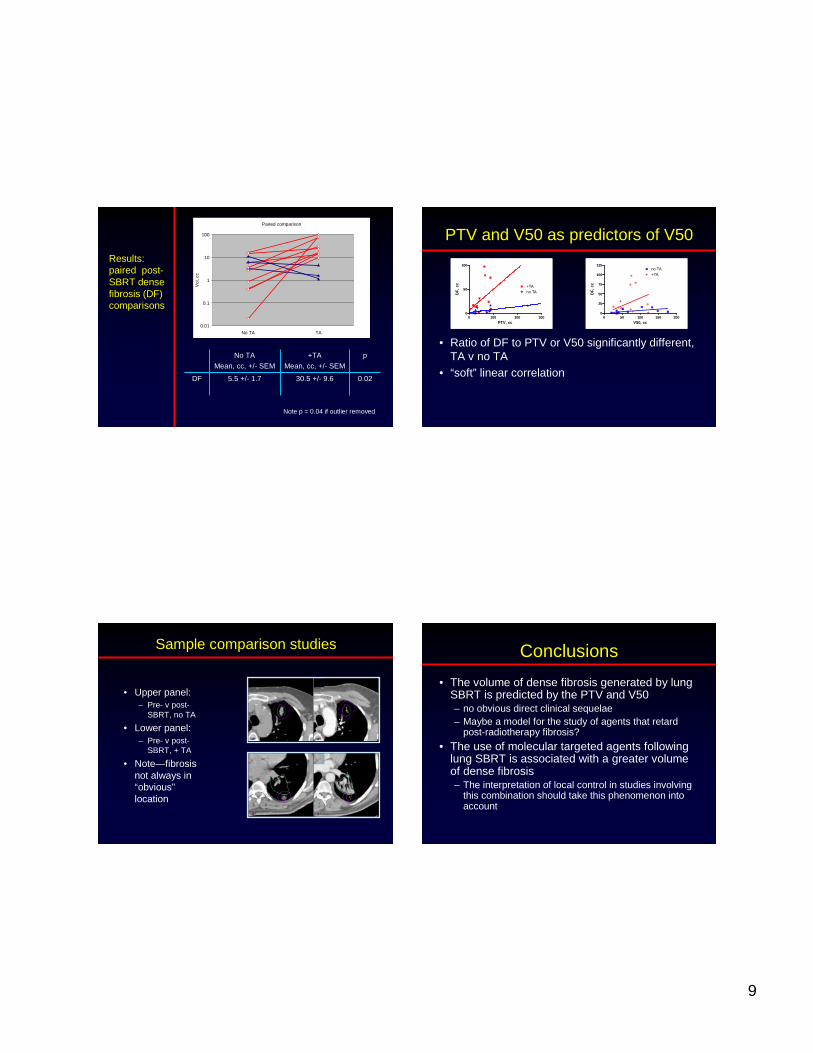
Results:paired post-SBRT densefibrosis (DF)comparisons
Paired comparison
0.01
0.1
1
10
100
No TA TA
Vol
,cc
0.0230.5 +/- 9.65.5 +/- 1.7DF
+TA
Mean, cc, +/- SEM
pNo TA
Mean, cc, +/- SEM
Note p = 0.04 if outlier removed
PTV and V50 as predictors of V50
0 100 200 3000
50
100
+TAno TA
PTV, cc
DF
,cc
0 50 100 150 2000
25
50
75
100
125no TA+TA
V50, cc
DF
,cc
• Ratio of DF to PTV or V50 significantly different,TA v no TA
• “soft” linear correlation
Sample comparison studies
• Upper panel:– Pre- v post-
SBRT, no TA
• Lower panel:– Pre- v post-
SBRT, + TA
• Note—fibrosisnot always in“obvious”location
Conclusions
• The volume of dense fibrosis generated by lungSBRT is predicted by the PTV and V50– no obvious direct clinical sequelae– Maybe a model for the study of agents that retard
post-radiotherapy fibrosis?
• The use of molecular targeted agents followinglung SBRT is associated with a greater volumeof dense fibrosis– The interpretation of local control in studies involving
this combination should take this phenomenon intoaccount
10
• NTCP-based– Eg, PMH experience, Dawson et al
Strategies for setting normal liverdose constraints
• Critical volume model– At least 700 cc normal
liver received < 15 Gycumulative
0
500
1000
1500
2000
2500
0 10 20 30 40 50
dose
abso
lute
volu
me
ofun
ivol
ved
liver
,cc
This differencemust be > 700
Liver Reactions on CT after SBRT:Herfarth classification
• Type 1 reaction:– Hypodensity in portal-
venous– isodensity in the late
contrast• Type 2 reaction:
– Hypodensity in portal-venous
– hyperdensity in the latecontrast
• Type 3 reaction:– Isodensity / hyperdensity in
portal-venous
Type 1, 6 weeks after SBRT
Sample case:metastatic nasophayngeal cancer
• 71F T1N2cM0 nasopharynx ca– cisplatin and 70 Gy
• 8 mos later, neck recurrence– salvage dissection and
brachytherapy
• 9 mos later, bx-proven liver met– weekly gemcitabine and cisplatin
– Transient minor response
• 6 mos later, Phase I SBRT study
11
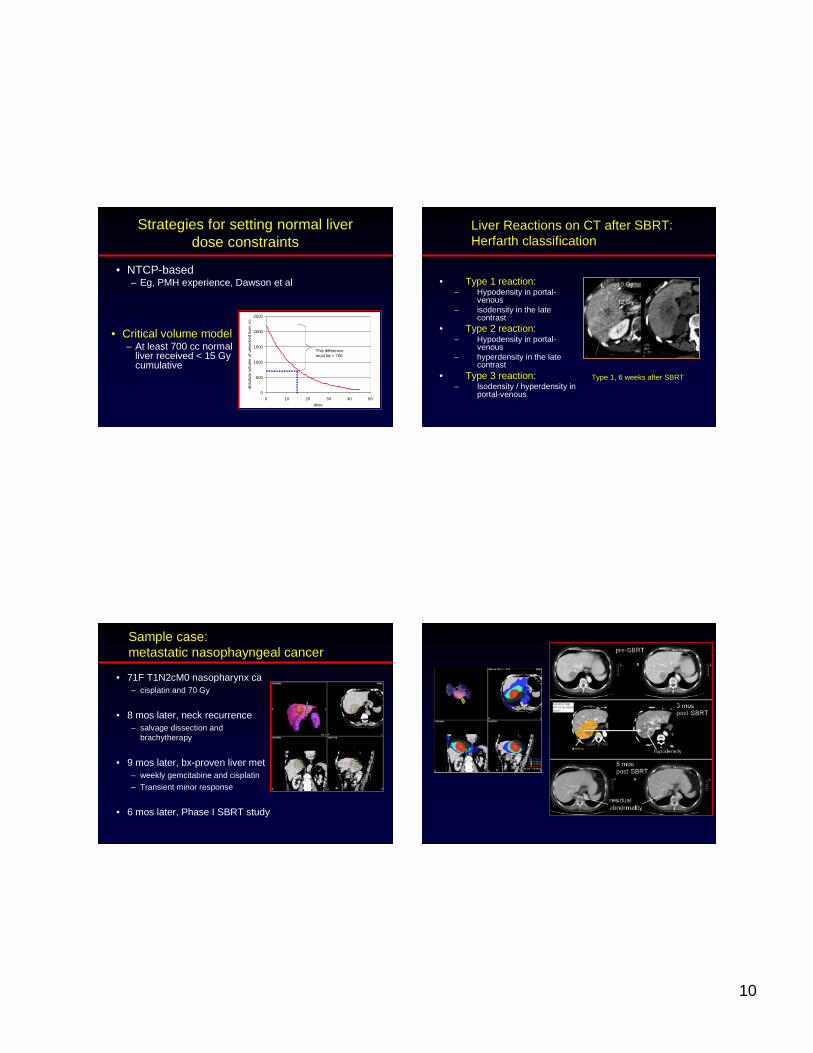
Histologic analysis of early liverSBRT effects
• Case study:– Pre-op chemoRT for rectal cancer– SBRT for solitary liver met– At time of APR, resection of treated liver and new, previously
unknown other liver met
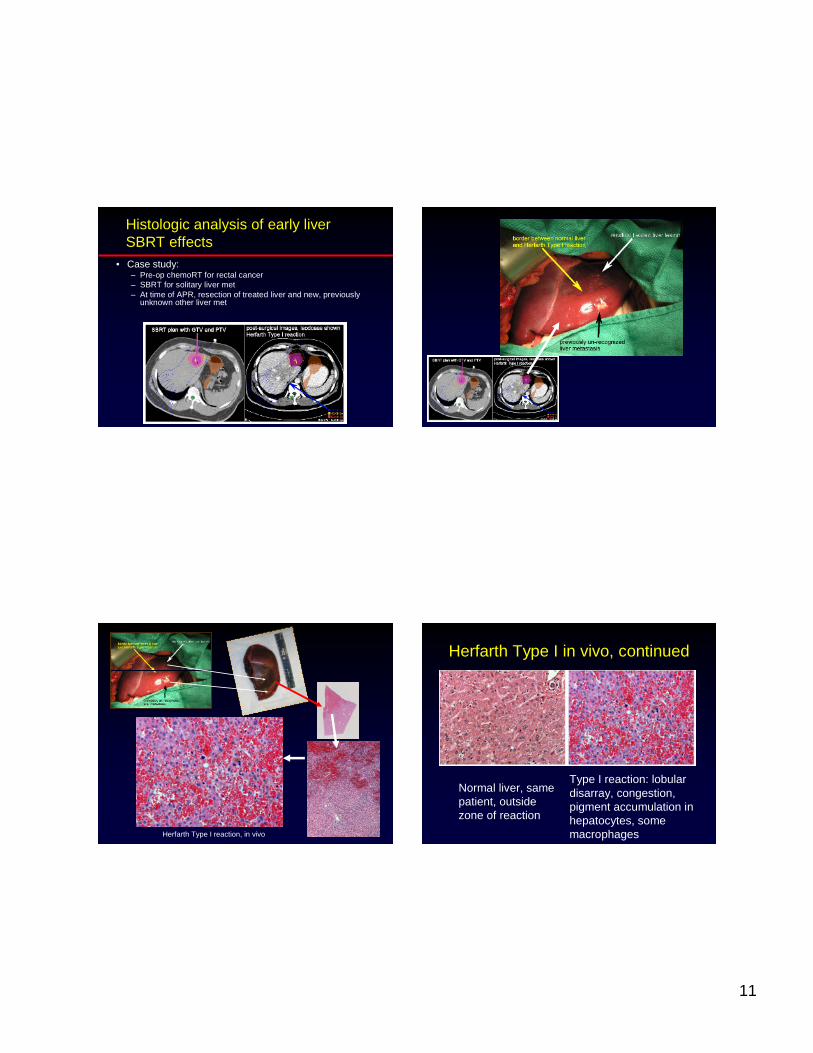
Herfarth Type I reaction, in vivo
Herfarth Type I in vivo, continued
Normal liver, samepatient, outsidezone of reaction
Type I reaction: lobulardisarray, congestion,pigment accumulation inhepatocytes, somemacrophages
12
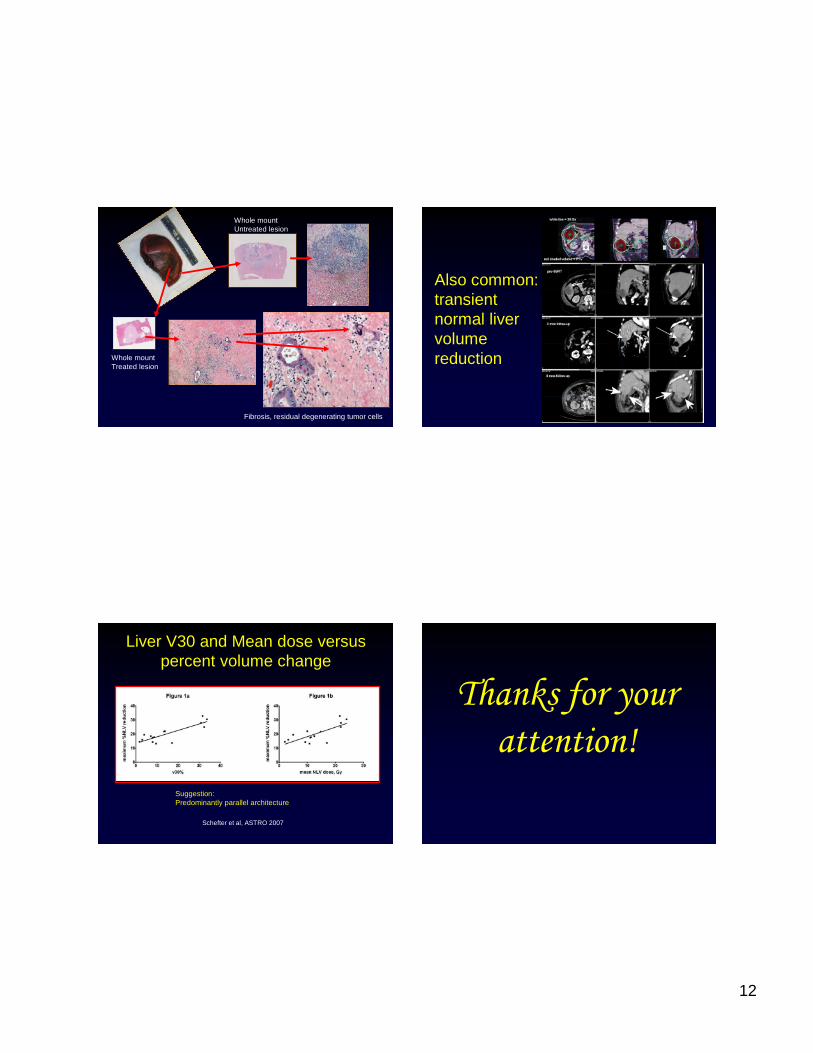
Whole mountUntreated lesion
Whole mountTreated lesion
Fibrosis, residual degenerating tumor cells
Also common:transientnormal livervolumereduction
Liver V30 and Mean dose versuspercent volume change
Schefter et al, ASTRO 2007
Suggestion:Predominantly parallel architecture
Thanks for your attention!





























