Embed Size (px)
DESCRIPTION
Â
Citation preview
1
Waking Up To Sleep ApneaThe Perils of an Underdiagnosed Disorder
STEVE ADAMS

2
Table of ContentsTable of Contents... 2Dedication... 5Foreward... 6Introduction... 81. Why is Good Sleep so Important... 122. Treatments: Reverse Vacuum Cleaners, Bad Braces & Open Jaw Surgery?... 153. Lessons For Sleep Apnea from Diabetes... 24
3
Certian activities contribute to bad sleep such as (clockwise) Electronics less than an hour before bed, TV less than an hour before bed, bright lights, and carobhydrates such as cereal.

4
5
This book is dedicated to anyone and everyone who loves sleep but doesn’t always get enough of it.
6
FOREWORDWhen we began deciding what we would look into for our research papers, I re-ally wasn’t sure what topic I wanted to choose. I contemplated several ideas but eventually decided that only one would be possible to complete within the project guidelines. That was sleep deprivation. This was still a very wide topic, and so as we continued working on our project I eventually refined my topic down to specifically sleep apnea. I realized that this would be a great subject to explore because I have this condition, and so do several family members and friends of mine.Through the course of my research I discovered what a prevalent problem I was looking into, and not only prevalent, but very under recognized. As I interviewed people and looked through sources and websites, I discovered a disturbing fact, there are no sure fire treatments for sleep apnea. I looked up statistics for successes and failures of the various treatments. This brought me to my argument: If more people know about sleep apnea, more can be done to develop more and better treatments.The interesting thing about sleep deprivation in general is that people don’t take it very seriously. While it may just make you tired, it can cause more serious, some-times life threatening issues. In this paper I will explore what sleep apnea is, how it is treated, and what can be done to help it be better treated. I interviewed people with sleep apnea, doctors, and students on various aspects of the topic. Some of them have very interesting things to say and stories to tell. And who knows, you may discover that you yourself are a victim of this condition.
7
8
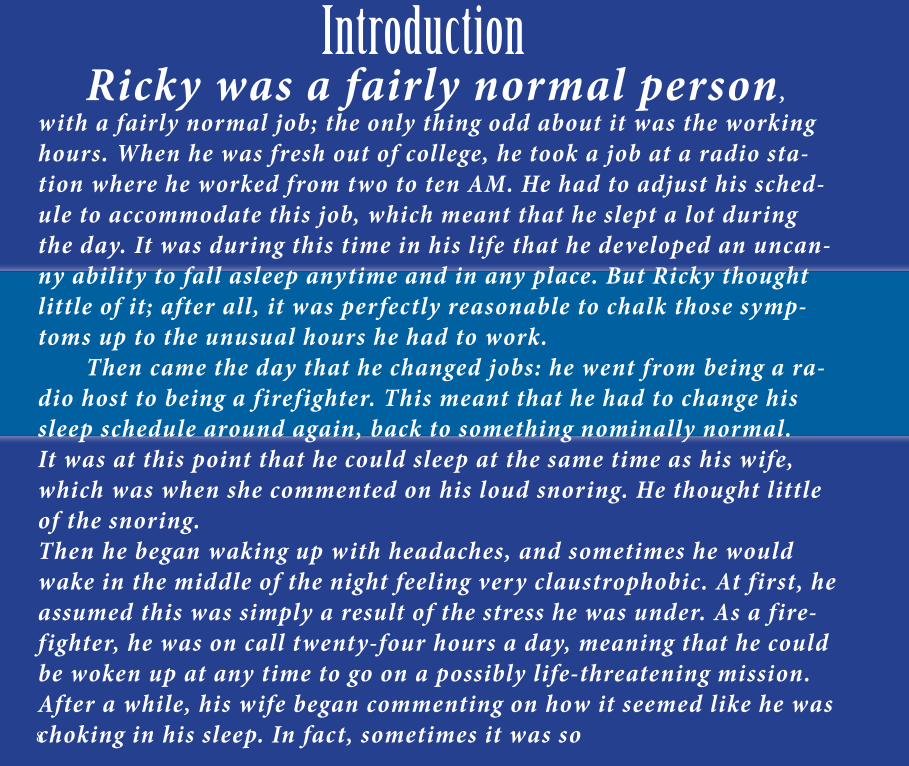
Ricky was a fairly normal person, with a fairly normal job; the only thing odd about it was the working hours. When he was fresh out of college, he took a job at a radio sta-tion where he worked from two to ten AM. He had to adjust his sched-ule to accommodate this job, which meant that he slept a lot during the day. It was during this time in his life that he developed an uncan-ny ability to fall asleep anytime and in any place. But Ricky thought little of it; after all, it was perfectly reasonable to chalk those symp-toms up to the unusual hours he had to work. Then came the day that he changed jobs: he went from being a ra-dio host to being a firefighter. This meant that he had to change his sleep schedule around again, back to something nominally normal. It was at this point that he could sleep at the same time as his wife, which was when she commented on his loud snoring. He thought little of the snoring. Then he began waking up with headaches, and sometimes he would wake in the middle of the night feeling very claustrophobic. At first, he assumed this was simply a result of the stress he was under. As a fire-fighter, he was on call twenty-four hours a day, meaning that he could be woken up at any time to go on a possibly life-threatening mission. After a while, his wife began commenting on how it seemed like he was choking in his sleep. In fact, sometimes it was so
Introduction
9The dreaded clock that each of us must face each morning.
10Caffeine can be used to keep people awake as a compensator for bad sleep, but it is no solution.
11
loud that she would have to sleep somewhere else. This got him thinking: each morning he needed two massive cups of coffee to make it through the day. This could indicate he was getting poor sleep, but the fact that he was hav ing all these strange sy mptoms while he was sleeping made him curious. He wondered if all of this was connected. After do-ing a bit of research, he went to a doctor, who had him go to a sleep clinic, where he was diag nosed w ith moderate sleep apnea. You may be wondering, what is sleep apnea? In simple terms, it is a sleep disor-der in which the air way becomes par tially or fully obstructed during sleep. This causes one to have diff iculty getting the oxygen needed for the body. The brain, in turn, has to wake up the body so that it can open the air way and breathe again. So what exactly does one do about sleep apnea? There are different approaches to it , but they all star t by getting it diag nosed, which means that you go to a doctor, who then sends you to a sleep center. One of these sleep centers is called the Palo Alto Medical Foundation Sleep Center. Here, you w ill be taken to a room that is like a motel room, where there is a bed, a TV, and a bathroom w ith a shower. However, you are not here simply to sleep the night. When you decide you are ready to go to bed, an atten-dant (or two) w ill come to your room, sit you dow n, and beg in gluing sensors all over your body. The sensors record data like hear tbeat, breathing, and brain wave activ-ity. After they have f inished w iring you up, you w ill lie dow n and do your best to fall asleep. In the morning, usually quite early, maybe around six o’clock or so, they w ill come in, wake you up, and take off all your sensors, after which you can use their show-er to wash all the glue off your skin and out of your hair. After this, you can go home. They w ill send the doctor their results, and you w ill know whether or not you have sleep apnea. You can go from there in terms of treatments. So what is the moral of the stor y? Sleep apnea can be hard to catch, but it is affecting people in negative ways, and it needs more public attention so that more can be done about it.
12
Doctors and the public in general have a fairly good idea of what bad sleep is. Re-sults can include restlessness, problems breathing while sleeping, and waking up at night. World-renowned sleep surgeon Dr. Kasey Li talks about some of the symptoms of sleep apnea:In kids, a lot of [symptoms] are bedwetting, moving around a lot in bed, restless sleep, sleep walking, sleep talking, nightmares, night terrors, and hyperactivity. A lot of kids have hyperactivity and concentration issues, attention deficits and that sort of thing. As they get older and become teenagers and puberty sets in, then they start to convert to an adult pattern of tiredness and fatigue... unrefreshing sleep... It could also be waking up with headaches.Dr. Vadim Kagramanov of Palo Alto Medical Foundation also notes that in relation to sleep loss, “cognitive thinking problems are fairly common.” He goes on to explain, “our bodies and brains tend to react to sleep fragmentation as well as they would to lack of sleep altogether.” Sleep fragmentation is the term that describes the waking up at night that happens due to sleep apnea. Bad sleep does not simply affect behav-ior and concentration issues, however. Kagramanov points out that:Another way sleep apnea affects one’s health is by exposing the body to the negative effects of low oxygen levels at night. This is why sleep apnea is one of the significant risk factors for the development of high blood pressure, diabetes, strokes, heart at-tacks, depression, irregular heart rate, and other medical issues later in life.
1. Why Is Good Sleep So Impor-tant?
13
The contrast between the symptoms of child and adult sleep apnea is acted out here with the child being hyper and the adult sleeping.
14
Basically, bad sleep, and sleep apnea is particular, can cause some very serious conditions. Jeff Adams was diagnosed with sleep apnea ten years ago. His story explains first-hand some of the perils of sleep loss:“Ever since I can remember, I was just simply always tired, and certainly on weekends and in the summer I would sleep in until eleven or noon and still never feel rested, and I can remember friends saying ‘Boy, you sure sleep a lot.’ I just never really knew why. Since I didn’t know I had it in school, I just dealt with it, I was young and I could deal with it, but as I got older, it would just simply manifest itself in feeling exhausted and tired all the time which leads to problems with concentration and focus and the ability to stay focused and take in complex information and have it stick in your head, I would have to re-read things over and over and over for it to make sense, and later on as the apnea got worse and worse I would start falling asleep, kind of like a narcoleptic, just be so tired that I would have little micro-sleeps, and we all have some of those, but I had a lot more than I should have. That’s how it manifested itself and played out, just being tired, and then it started to affect my ability to function and concentrate and work and every-thing else.”Jeff is not alone in this, in fact, an estimated eighteen million Americans, or 6.62 percent of the population, have been diagnosed with it. So, if one in fifteen people have a lower quality of life because of this condition, one would be wise to look at one’s own life, and try to identify any of the symptoms. The only problem with this, as Dr. Li explains, is that, “there are vast differences in terms of people’s symptoms.” As you read earlier, some people may get headaches, while oth-ers suffer from cognitive thinking problems, and there is a range of symptoms that you could be experiencing. The confusing part about this is that many of these symptoms can be attributed to other causes, like stress in Ricky’s case. This is why sleep clinics like the PAMF one remain the only way of reliably testing for sleep apnea. To answer the question, “why is good sleep impor-tant?” succinctly: without good sleep, you will suffer from impaired social and mental functions, and you may also greatly increase your risk of life-threatening medical complications.
15
2. Treatments: Reverse Vacuum Cleaners, Bad Braces, and Open Jaw Surgery?
A CPAP Machine
16
There are several contenders when it comes to treating sleep apnea. In terms of treatment, there is one main method that doctors tend to prescribe first to their patients. This treatment is called a Continuous Positive Airway Pres-sure device, or CPAP. A CPAP machine works by blowing air down your air-way and opening it up so that you can breathe while you sleep, essentially fixing the problem. Mr. Adams describes it as “a small vacuum cleaner run-ning in reverse, forcing air down your throat.” Dr. Kagramanov calls it “the medical gold standard for treatment of sleep apnea.” The only issue with this treatment is the way that it’s done. The patient wears a mask that is gener-ally fairly non-conducive to sleep. Dr. Li points out that:The biggest side effect is psychological. People don’t want to ‘have to be hooked up to a machine for the rest of their life.’ That’s the one thing that people tell me all the time. They don’t want to feel like they are dependent on a machine every time they go to sleep. And the thought of having to use that for the rest of their life, I think that’s the biggest hurdle. Many patients will stop using a CPAP device because they simply don’t want to use it. For example, after being diagnosed with sleep apnea, Jeff tried us-ing CPAP for a year and half, and he simply could not tolerate it. One study showed that compliance with CPAP over a long-term period also was directly linked to the severity of apnea (McArdle et al.) If a patient has more severe sleep apnea, s/he is more inclined to use the machine. The reason for its suc-cess, however, is that it is fairly easy to use and has only minor downsides.While CPAP may be the gold standard, as you can see, it is not perfect, and it does not work for everybody. So what happens next? What other treatments are there for this condition?
17
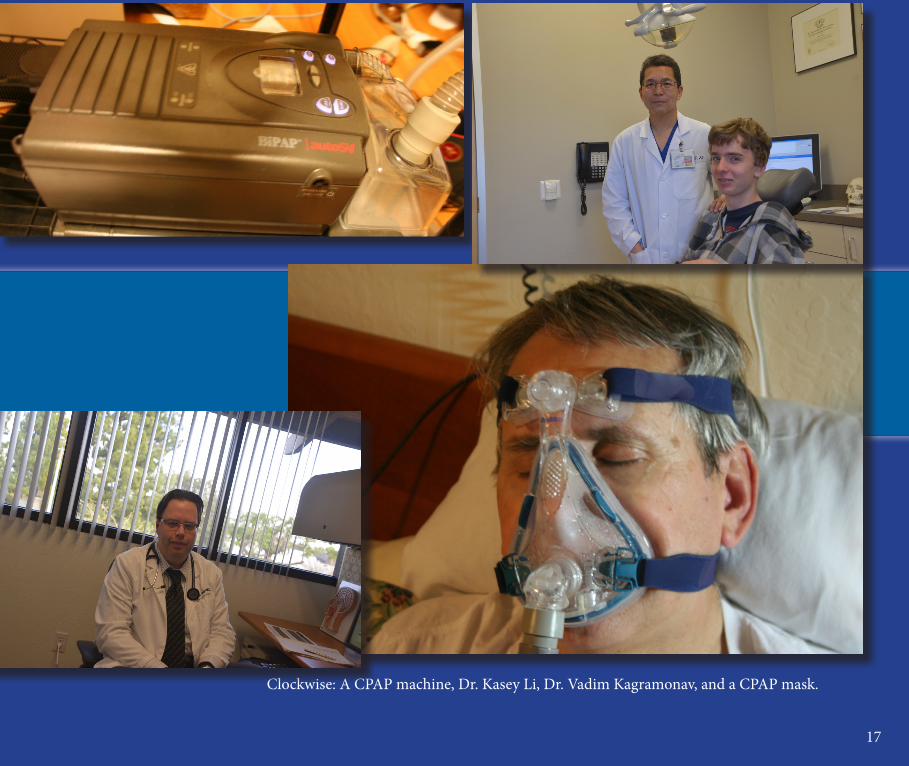
Clockwise: A CPAP machine, Dr. Kasey Li, Dr. Vadim Kagramonav, and a CPAP mask.
18
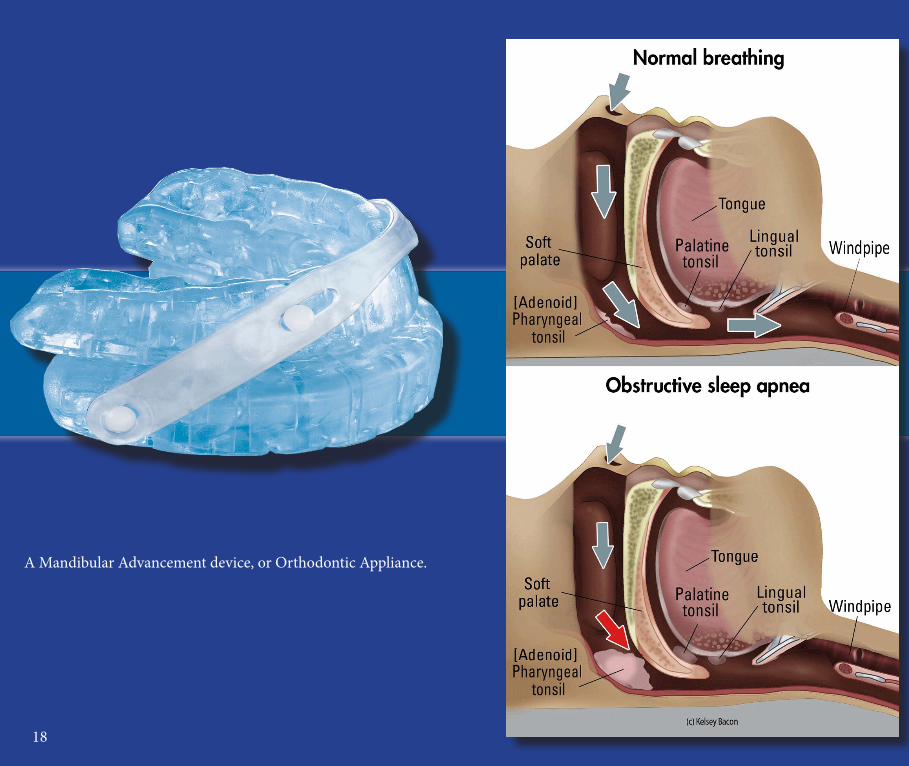
A Mandibular Advancement device, or Orthodontic Appliance.
19
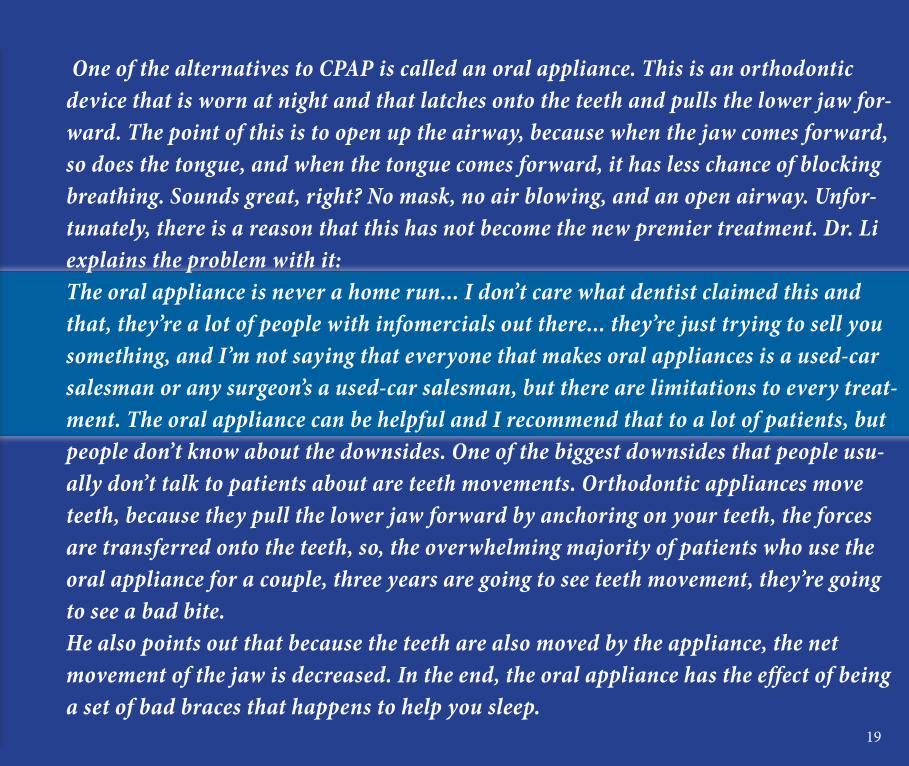
One of the alternatives to CPAP is called an oral appliance. This is an orthodontic device that is worn at night and that latches onto the teeth and pulls the lower jaw for-ward. The point of this is to open up the airway, because when the jaw comes forward, so does the tongue, and when the tongue comes forward, it has less chance of blocking breathing. Sounds great, right? No mask, no air blowing, and an open airway. Unfor-tunately, there is a reason that this has not become the new premier treatment. Dr. Li explains the problem with it: The oral appliance is never a home run... I don’t care what dentist claimed this and that, they’re a lot of people with infomercials out there... they’re just trying to sell you something, and I’m not saying that everyone that makes oral appliances is a used-car salesman or any surgeon’s a used-car salesman, but there are limitations to every treat-ment. The oral appliance can be helpful and I recommend that to a lot of patients, but people don’t know about the downsides. One of the biggest downsides that people usu-ally don’t talk to patients about are teeth movements. Orthodontic appliances move teeth, because they pull the lower jaw forward by anchoring on your teeth, the forces are transferred onto the teeth, so, the overwhelming majority of patients who use the oral appliance for a couple, three years are going to see teeth movement, they’re going to see a bad bite.He also points out that because the teeth are also moved by the appliance, the net movement of the jaw is decreased. In the end, the oral appliance has the effect of being a set of bad braces that happens to help you sleep.
20
There is a third treatment, which is the most dramatic of the three: maxillomandibular advancement, or MMA. Basi-cally, MMA is a surgery where the upper and lower jaw are cut and moved forward through the use of metal plates and pins. The idea behind it is similar to that of the oral appliance: if your jaw is moved forward, you have more room to breathe in your air-way, and you can sleep better. Mr. Adams notes about the outcome of this surgery: “It’s quite dramatic to see the airway before, and then the new airway after the surgery. It goes from the size of a toothpick to the size of a garden hose.” Dr. Li specializes in MMA, and says that in teenagers and young adults, the success rate is great. Ninety to ninety-five percent of people in that age group feel and sleep dramatically better after surgery. In other age groups, the percentage can drop to about eighty percent, but this is still a good percentage. In fact, one study of MMA in 21 patients showed that 20 of them had significant improvement, with increased oxy-gen saturation and improved quality of sleep (Hochban). Another study by Dr. Jeffrey R. Prisnell showed that fifty out of fifty pa-tients showed significant improvement. “Snoring was eliminated in 44 of 50; depression, moodiness, and/or irritability was reduced in 36 of 39; and morning headaches were alleviated in 28 of 29 pa-tients” (Prisnell.) The study lists a range of other symptoms that were also alleviated in the majority of patients.
21
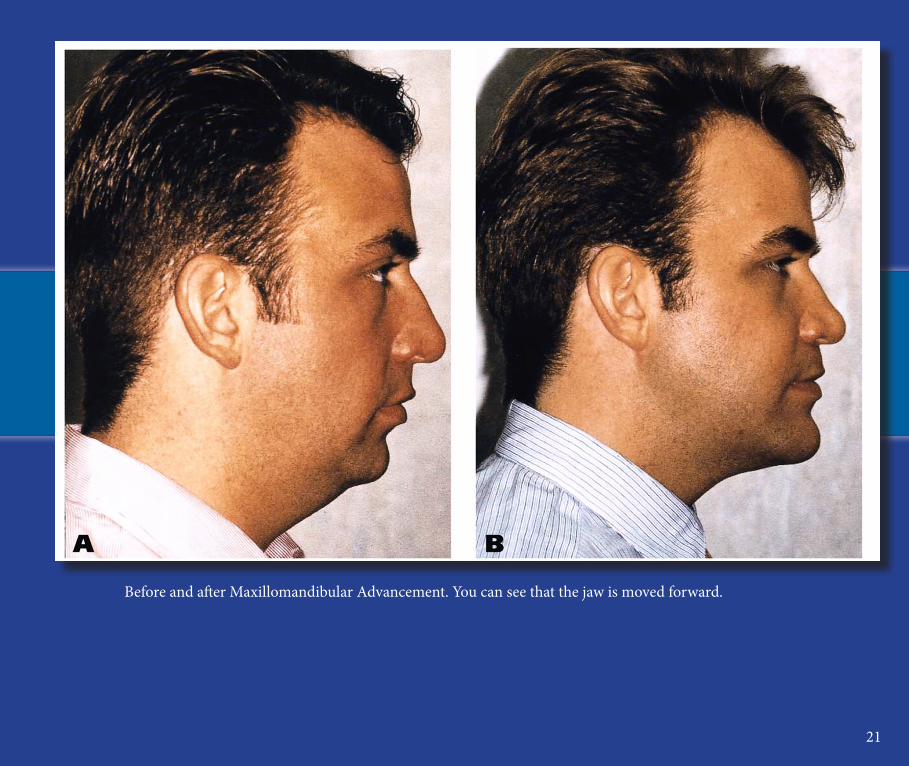
Before and after Maxillomandibular Advancement. You can see that the jaw is moved forward.
22
Jeff Adams
23
So if MMA is so great, why not just use MMA on everyone with sleep apnea?One word: downsides. First of all, operating on people that are older than their early to mid sixties is never a good idea, according to Dr. Li. Secondly, MMA is a major procedure, and full recovery takes multiple months. Your jaw is wired shut for the first four weeks or so, so talking is difficult. You are also restricted to a liquid diet at the start. Also, the fact that you don’t feel very well in general. This causes people to miss significant amounts of work, school, and other activities. Thirdly, MMA can change the way you look. Granted, it’s usually not very dra-matic, but the jaw is moved forward, and some people are very uncomfortable with the concept. Fourthly, as with any surgery, there is the possibility of compli-cations. Dr. Li explains:I had a patient with chronic pain following surgery, that’s rare, one in several hundred, it’s not because of, so much, the surgery, but because the person’s nerves are wired differently, meaning that if you do some research on phantom limb pain in the Civil War because of amputation. Not everyone develops phantom limb pain, but some people develop phantom limb pain because their brain is wired a little differently. As I said earlier though, MMA is not always successful. Jeff explains his ex-perience with the procedure: “I was supposed to feel wonderful the very next day and that didn’t happen for me, unfortunately. So after several weeks of [working with the doctor]... some of the symptoms were improved. But the ultimate goal of feeling rested was still elusive.” In short, MMA can be very helpful, especially for younger people, but it has downsides that cannot be denied. Overall, there are multiple treatments that can help and even fix sleep ap-nea, but none of them are guaranteed successes, and they put strain on the lives of the users.
24
3. Lessons for Sleep Apnea from Diabetes Everyone knows what diabetes is, right? About the same amount of people are diagnosed with diabetes as are di-agnosed with sleep apnea. Yet when I interviewed fellow stu-dents, only about 2/3 of them had an idea of what sleep apnea was, and every single one I talked to knew what diabetes was. So why it is that sleep apnea is more obscure? The answer seems to be that sleep apnea’s symptoms can be downright confusing, whereas those of diabetes are not as much so. The question becomes, what would happen if the public knew as much about sleep apnea as it did about diabetes? More than one billion dollars per year is allocated to diabetes research by the U.S. government, while only a quarter of that is allo-cated to all combined sleep research (National Institutes of Health). Obviously, diabetes is quite a different problem, and arguably a more urgent one, that needs more funding. How-ever, if people knew more about sleep apnea, and could recog-nize when they had it, this could lead to an increase in fund-ing and research and eventually to better treatments.
25
“ You are at a greater risk of having sleep apnea if you are overweight, male, smoke a lot, drink a lot, have nasal congestion and a good number of other things.”
26
Some of Doctor Li’s awards.
27
Because of the very nature of sleep apnea, many people could be living with it without even knowing. In fact, according to government statistics, about 20% of the adult population suffers from sleep apnea (pubmed.gov), even though, as we said, only about 6.6% are diagnosed. Let’s do some math. Twenty percent of the adult population suffers from sleep apnea. The population of the U.S. is approximately 314,000,000, accord-ing the 2012 estimate. Seventy-six percent of the population is adults, or about 239,000,000 people (U.S. Census Bureau). That translates to about 47,800,000 American adults that have sleep apnea. That’s one in five adults. If this significant portion of the population were to become aware that they have this condition, research for more effective cures would skyrocket. One of the things people can be made aware of besides the ac-tual consequences of sleep apnea, are the risk factors. You are at a great-er risk of having sleep apnea if you are overweight, male, smoke a lot, drink a lot, have nasal congestion and a good number of other factors.
28
Both Doctors Li and Kagramanov agree that awareness in general has gotten better in the past decade or so; however, they also agree that it is still significantly under-diagnosed and not well known enough. How can something be properly addressed if it is not known as much as it should be? Solving sleep apnea in a more effective way will come down to getting people to understand how prevalent the problem is, so that they can do more about it.
29
Works CitedAdams, Jeff. Personal interview. 7 March. 2013.
“Age and Sex Composition in the United States.” U.S. Census Bureau., 1 April. 2010. Web. 25. March. 2013.
Courson, Andrew. Maxillomandibular Advancement: Before and After. n.d. Texas.
“Estimates of Funding for Various Research, Condition, and Disease Categories (RCDC).” National Institutes of
Health. U.S. Department of Health & Human Services, 13 February. 2012. Web. 25 March. 2013.
Hochban, W. “Surgical Treatment of Obstructive Sleep Apnea by Maxillomandibular Advancement.” Sleep
(1994): 624-629. Web. 25 March. 2013.
Kagramanov, Vadim. Personal interview. 14 March. 2013.
Li, Kasey. Personal interview. 14 March. 2013.
McArdle, Nigel; Devereux, Graham; Heidarnejad, Hassan; Engleman, Heather, M; Mackay, Thomas,W; and
Douglas, Neil, J. “Long-term Use of CPAP Therapy for Sleep Apnea/Hypopnea Syndrome” (1998). Web. 25
March. 2013.
“Prevalence of Undiagnosed Obstructive Sleep Apnea Among Adult Surgical Patients in an Academic Medical
Center.” U.S. National Library of Medicine. 10 August. 2009. Web. 25 March. 2013.
Prisnell, Jeffrey, R. “Maxillomandibular Advancement Surgery in a Site-Specific Treatment Approach for Ob-
structive Sleep Apnea in 50 Consecutive Patients” Chest Journal (1999). Web. 25 March. 2013.
SnoozeHead [Ricky]. “My Story... And I’m sticking to it.” Apnea Support Forum. American Sleep Apnea Associa-
tion, 4 March. 2013. Web. 25 March. 2013.
Unknown. Mandibular Advancement Device. 2012. United Kingdom.
Unknown. Sleep Apnea Diagram. n.d.

30
The End





























