Embed Size (px)
Citation preview

Stephanie Dewar MD, Stephen Hart MD, & Linda Waggoner-Fountain, MD
Children’s Hospital of Pittsburgh of UPMC University of Virginia Department of Pediatrics
March 28, 2015, APPD Annual Meeting
OPTIMIZING THE OUTCOME OF PATIENT HANDOFFS: A PRACTICAL APPROACH TO IMPLEMENTING CURRICULUM
WITH OBSERVATION & FEEDBACK TO TRAINEES

Disclosures
We have nothing to disclose.

Objectives Understand the critical elements of
patient sign-out that should be exchanged by trainees
Review the RRC requirements around transitions in care
Learn techniques to teach trainees how to improve sign-out skills

Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of
standardized curriculum Observation and rating of sign-out Implementation techniques for home Summary

Simulation Exercise Person who has the
information:
May only use words to describe the information to the scribe
MAY NOT show the information to the receiver
MAY NOT look at the interpretation of their words
Person who is receiving the information:
May ask any questions of
the information giver
MAY NOT look at the information
MAY NOT display their work to the giver

Overview of Sign-out

IPCS as Related to Transitions of Care
Communicate effectively with physicians, other health professionals, & health related agencies
The relaying of complete and accurate patient information between individuals or teams in transferring responsibility for patient care in the healthcare setting

Transitions of Care Programs must design clinical assignments to
minimize the number of transitions in patient care.
Sponsoring institutions and programs must ensure and monitor effective, structured hand-over processes to facilitate both continuity of care and patient safety.
Programs must ensure that residents are competent in communicating with team members in the hand-over process.
o 2016 Pediatric Program Requirements, p 15, 16 o 2016 Common Program Requirements, p 11, 17

Pediatric Milestones Provide transfer of care that ensures seamless
transitions Variability in transfer of information (content, accuracy,
efficiency and synthesis) from one patient to the next. Frequent errors of omission and commission in the handoff.
Uses a standard template for the information. Unable to deviate from that template for more complex situations. May have errors of omission and commission in the handoff.
Neither anticipates nor attends to the receiver of the information
Adapts and applies a standard template, relevant to individual contexts, reliably and reproducibly, with minimal errors of omission or commission. Allows ample opportunity for clarification and questions.
Beginning to anticipate potential issues for the transferee. P11 The Pediatrics Milestone Project

Definition of Sign-Out A mechanism of transferring
information, responsibility and/or authority from one set of care-givers to another
Primary objective is the accurate transfer of information about patient’s state and plan of care

Importance of Sign-Out Many residents learn how to sign-out
informally, while on the job.
Sign-out is a lifelong life-long skill • Physicians continue to give and
receive sign-out long after the complete residency

Why Is This A Problem Now? Number of sign-outs between residents ↑ Physician continuity of care during
hospitalizations ↓ Residents have become more dependent
upon exchange of clinical info during sign-outs
De-emphasis of clinical communication in the ‘medical record’
Emphasis of billing and compliance

“EVERY PATIENT IS MY PATIENT!” Sign-out – the handover of patient information & responsibility

Sign-out vs. Sign-Over Culture change
• “This is my patient RIGHT NOW” • “My sign-out is UP TO DATE” • “My team is responsible for our sign-
out.”
Care of the patient as a relay race • Running your leg of the race • Hand off of the baton

Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary

Curriculum What
What not
How

Verbal Sign-out Written Sign-out
Designated time & place Uninterrupted Organized Thorough Concise (2-3 min/pt) Time for questions
Legible Relevant Accurate Up to date Copy available for recipient

Location of Sign-out Designated place With computers Quiet place with minimal interruptions

Sign-out times Morning 6A/7A
Noon 11:30A
Short call 4P
Night Team 7P

Expectations
Verbal Sign-out Team sign-out is optimal Hospital initiatives Consider starting with sickest patients
first OK to go to the bedside

Expectations
Written Sign-out C/ Child and Complexity The ID statement
History/Active issues Include access, new events of the day, better or
worse Plan/To do list Anticipatory Guidance Contingency plans – If…then… statements
? Questions
Delete useless information and update daily

C-Child/Complexity The ID statement (The Big Sentence): Age, relevant PMH, reason for admission, up to
date assessment, pertinent hospital course and workup
Sick or not sick, getting better or not Example: A 6 week old infant admitted with fever, irritability,
poor oral intake and vomiting who has been found to have HSV meningitis is—
A 6 week old with HSV meningitis on IV acyclovir who is now afebrile, drinking well with good urine output

History New events of the day
Access
Example: The patient passed his hearing test today,
was able to wean off supplemental oxygen and has a right antecubital PICC line.

P-Plan Reasonable list of things colleagues
should do while you are away
Labs/Diagnostic tests Discharges with info about what is left to be done (scripts,
home health, etc.) Consults Should we order what the consultant wants?
Example: “Call radiology for MRI report, if it shows osteo,
consult ID for antibiotic recommendations.”

More Plan: Anticipatory Guidance This is your contingency planning. “If X then Y.” ANTICIPATE what will happen to your
patient. Medications, dosages and when to give the
medications, including medications NOT to use. Labs that need to be drawn or cultures that need to be
collected. Example: If patient seizes > 5 minutes, give him Ativan
0.05mg/kg. If he still seizes load him with 5mg/kg of fosphenytoin.
Pain – patient with thrombocytopenia, so don’t use NSAIDS

Cares---? -- Questions
If you are getting sign-out and you don’t know something ASK
If you don’t understand something, ASK
Don’t leave until all questions are asked and answered.

Cerner sign-out tool:


Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary
Now Your Turn Work in trios
One person is the sign-out giver, one is
the sign-out received, one is the observer
Look at your script only

Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary
Sign-Out Mnemonics SBAR – Situation, Background, Assessment, Read-
Back IDEAL – Identify, Determine, Evaluate, Act, Learn DATA – Demographics, Active Issues, To do list,
Anticipatory Guidance (if…then…) SIGNOUT? – Sick or DNR, Identifying Data,
General Hospital Course, New Events of the Day, Overall Health Status, Upcoming Possibilities with Plan, Tasks to Complete with plan, Questions
More Mnemonics SAIF-IR – Summary Statement, Active Issues, If-
then contingency planning, Follow-up Activities – Interactive Questioning, Read-back
SHOUT – Sick or Not Sick, History & Hospital Course, Objective Data (PE, vitals, results), Upcoming Plan, To Do including rationale
I-PASSTHEBATON → I-PASS – Illness Severity, Patient Summary, Action List, Situation Awareness & Contingency Planning, Synthesis by Receiver
Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary

ED to Floor Handover ED-to-Inpatient #1
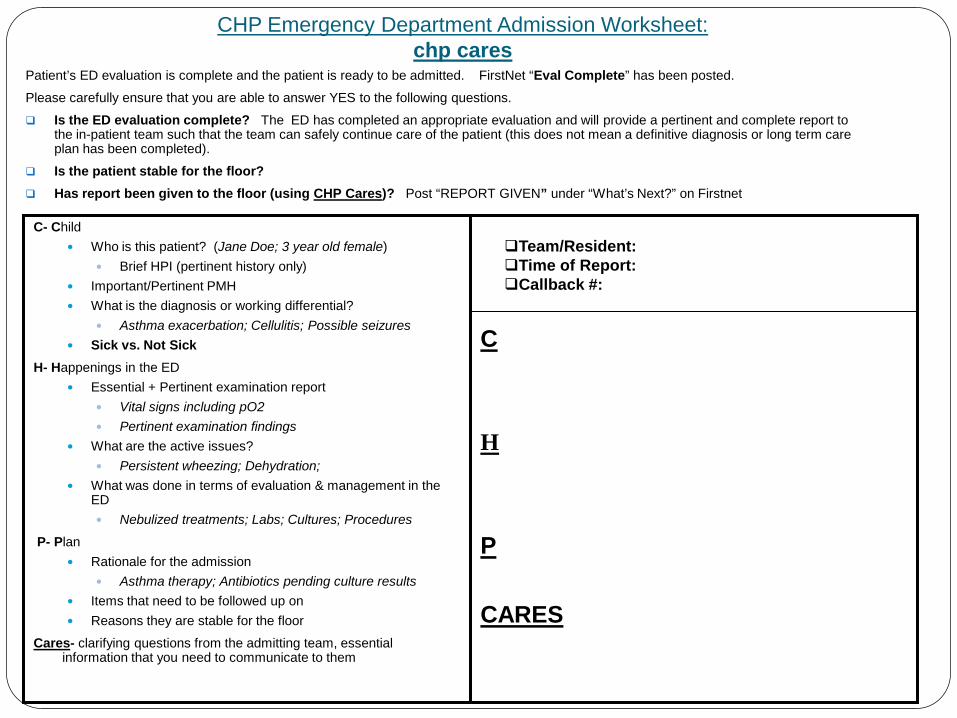
CHP Emergency Department Admission Worksheet: chp cares
Patient’s ED evaluation is complete and the patient is ready to be admitted. FirstNet “Eval Complete” has been posted.
Please carefully ensure that you are able to answer YES to the following questions.
Is the ED evaluation complete? The ED has completed an appropriate evaluation and will provide a pertinent and complete report to the in-patient team such that the team can safely continue care of the patient (this does not mean a definitive diagnosis or long term care plan has been completed).
Is the patient stable for the floor? Has report been given to the floor (using CHP Cares)? Post “REPORT GIVEN” under “What’s Next?” on Firstnet
C- Child
Who is this patient? (Jane Doe; 3 year old female) Brief HPI (pertinent history only)
Important/Pertinent PMH What is the diagnosis or working differential?
Asthma exacerbation; Cellulitis; Possible seizures Sick vs. Not Sick
H- Happenings in the ED Essential + Pertinent examination report
Vital signs including pO2 Pertinent examination findings
What are the active issues? Persistent wheezing; Dehydration;
What was done in terms of evaluation & management in the ED Nebulized treatments; Labs; Cultures; Procedures
P- Plan Rationale for the admission
Asthma therapy; Antibiotics pending culture results Items that need to be followed up on Reasons they are stable for the floor
Cares- clarifying questions from the admitting team, essential information that you need to communicate to them
C H P CARES
Team/Resident: Time of Report: Callback #:


ED to Floor Handover
ED-to-Inpatient #2
ED-to-Inpatient #3


Floor-to-Floor #1
Direct Observation
Floor-to-Floor #2

Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary

Teaching Sign-Out
Sign-out means different things to different people • Levels of experience • Styles of caring for patients • Styles of learning

PL-1 Goals & Objectives for Sign-Out
1. Will be able to identify the five key components for patient sign-out
2. Will recognize effective sign-out by others
3. Will be able to give all five essential components of sign-out without prompting by end of PL-1 year

PL-2 Goals & Objectives for Sign-Out
All skills of PL-1 plus 1. Will understand what read
back/synopsis role is in sign-out 2. Will recognize effective read back
by others 3. Will be able to elicit all 5
components of sign-out from other resident

PL-3 Goals & Objectives for Sign-Out
All skills of PL-2 plus 1. Will demonstrate effective & efficient
sign-out 2. Will demonstrate effective & efficient
read back as receiver in sign-out 3. Will utilize teaching opportunities 4. Will recognize collaborative cross check 5. Will work towards mastery of
collaborative cross check

Attending Goals & Objectives for Sign-Out
All skills of resident plus mastery of collaborative cross check • PL-1 – Information and Accuracy • PL-2 – Synopsis and Query • PL-3 – Efficiency and Collaboration

Process of implementation Emphasis was placed on: Face to face sign-out Standardized location Scheduled sessions Verbal communication Written sign-out tool

Things to Include
1. Name and/or MRN 2. The big sentence 3. Current condition 4. Plan of care 5. Contingency plans (What if’s/questions that
might arise overnight) 6. Read back/summation from receiver 7. Co-orientation & collaborative cross-check
Things Not to Include
Plans for next week that are not important for the next 24 hours
Gossip Too much time on background and pt ID Things easily found elsewhere
• Sign out sheet • Hospital chart or EMR • Medication orders
Who Gives Good Sign-Out and Why?
We surveyed our housestaff and asked them to identify the three (out of 39) residents who give the best sign-out • Three individuals were identified by more than 40%
of their peers “after signing out with them, I feel well prepared for the next
call shift” “they help me anticipate what might go wrong during my call
shift” “they give me a chance to ask questions”

Optimal Sign-out Giver
Arrives on time Brings an updated written sign-out list Invites questions Makes sure that all patient issues are
understood before leaving = Co-orientation is key

Optimal Sign-out Receiver
Arrives on time Is attentive to the sign-out giver Asks clarifying questions Makes sure that he/she understands all patient issues

Social Awareness Strategies
Watch Body Language Don’t Text at Meetings Make Timing Everything Clear Away the Clutter Practice the Art of Listening Go People Watching Catch the Mood of the Room Understand the Rules of the Culture
Game

Steps for Teaching, Observing and Evaluating Sign-out
Senior Resident Leadership Workshops Review expectations for SIGNOUT Share EMR Sign-out template Discuss plans for evaluation and feedback
Intern Orientation Review expectations for SIGNOUT Model adequate vs. inadequate sign-out Practice developing written sign-out
Evaluation of verbal SIGNOUT Verbal SIGNOUT observation tool Direct observation by attendings each week

Agenda Introduction & Overview Essential features of sign-out Delivery of Sign-out Review of available options of standardized
curriculum Observation and rating of sign-out Implementation techniques for home Summary

Summary Trainees need to be taught the critical
elements of patient sign-out
The RRC has clear requirements around transitions in care
There are a variety of techniques to teach trainees how to improve sign-out skills

Contact information Stephanie Dewar MD [email protected]
Stephen A. Hart MD [email protected]
Linda Waggoner-Fountain MD [email protected]





























