Embed Size (px)
Citation preview
Step TherapyThe ClearScript Step Therapy program promotes the cost-effective use of medications when more than one drug isavailable to treat a medical condition.
What is Step Therapy?If you are taking a medication in the Step Therapy program, you are required to try one or more first step drugs before asecond step drug is considered for coverage. Talk with your physician about which first step medication might be a goodchoice for you. A review may be required before a second step drug is covered.
If you have questions about the Step Therapy Program, contact ClearScript Member Services at the number on the backof your ID Card.
Important Note: The drugs included on this list may not be covered by all benefit plans. Your benefit plan determinescoverage for all medications. Additional coverage restrictions may apply for the medications included on this list. This list issubject to change throughout the year.
Condition / Drug Class First Step Drugs Second Step Drugs
Asthma/COPD - Long-Acting Combo Inhalers
History of TWO of the following generics or preferredbrands: ADVAIR DISKUS/HFA, BREO ELLIPTA,fluticasone-salmeterol OR SYMBICORT.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
AIRDUO DIGIHALERAIRDUO RESPICLICK
Patient is 5 years of age with a trial and failure orintolerance to ONE fluticasone-salmeterol containingproduct OR patient is 6 years of age or older with a trialand failure or intolerance to any TWO of the followinggenerics or preferred brands: ADVAIR DISKUS/HFA,BREO ELLIPTA, fluticasone-salmeterol ORSYMBICORT.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
DULERA
Asthma/COPD - Long-Acting Inhalers
History of the following preferred brand: SPIRIVA INCRUSE ELLIPTASEEBRI NEOHALERTUDORZA PRESSAIR
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 1
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
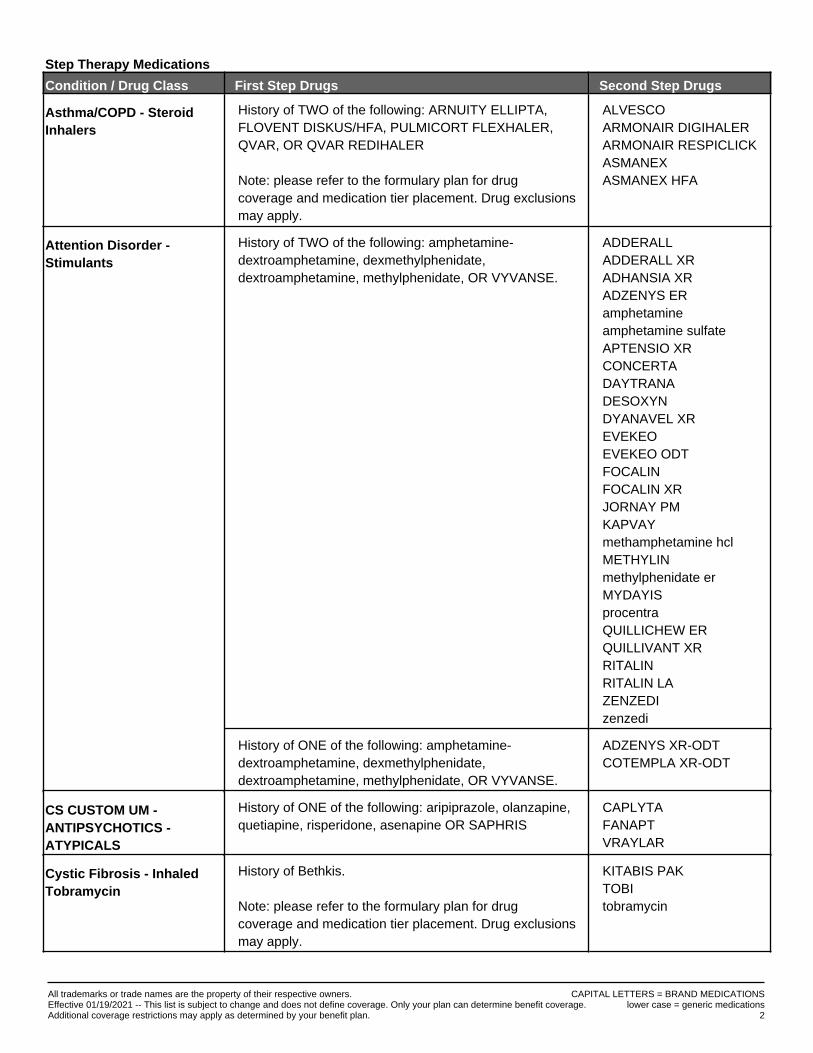
Asthma/COPD - SteroidInhalers
History of TWO of the following: ARNUITY ELLIPTA,FLOVENT DISKUS/HFA, PULMICORT FLEXHALER,QVAR, OR QVAR REDIHALER
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
ALVESCOARMONAIR DIGIHALERARMONAIR RESPICLICKASMANEXASMANEX HFA
Attention Disorder -Stimulants
History of TWO of the following: amphetamine-dextroamphetamine, dexmethylphenidate,dextroamphetamine, methylphenidate, OR VYVANSE.
ADDERALLADDERALL XRADHANSIA XRADZENYS ERamphetamineamphetamine sulfateAPTENSIO XRCONCERTADAYTRANADESOXYNDYANAVEL XREVEKEOEVEKEO ODTFOCALINFOCALIN XRJORNAY PMKAPVAYmethamphetamine hclMETHYLINmethylphenidate erMYDAYISprocentraQUILLICHEW ERQUILLIVANT XRRITALINRITALIN LAZENZEDIzenzedi
History of ONE of the following: amphetamine-dextroamphetamine, dexmethylphenidate,dextroamphetamine, methylphenidate, OR VYVANSE.
ADZENYS XR-ODTCOTEMPLA XR-ODT
CS CUSTOM UM -ANTIPSYCHOTICS -ATYPICALS
History of ONE of the following: aripiprazole, olanzapine,quetiapine, risperidone, asenapine OR SAPHRIS
CAPLYTAFANAPTVRAYLAR
Cystic Fibrosis - InhaledTobramycin
History of Bethkis.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
KITABIS PAKTOBItobramycin
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 2
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
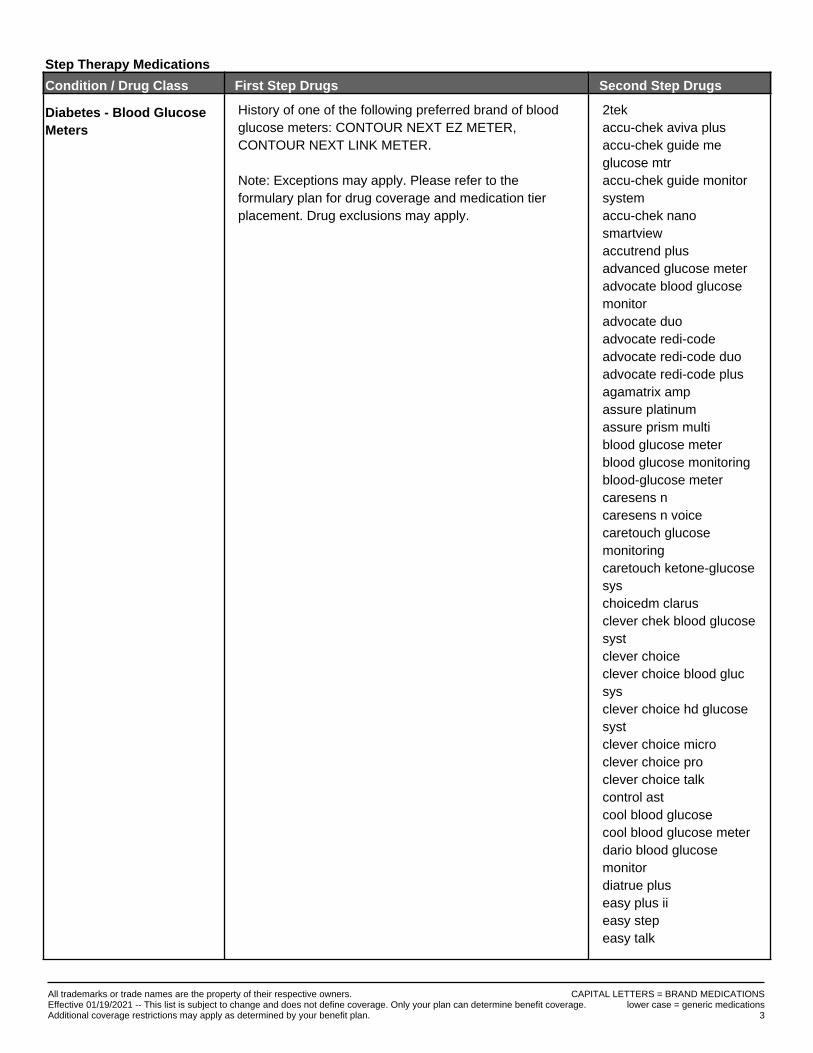
Diabetes - Blood GlucoseMeters
History of one of the following preferred brand of bloodglucose meters: CONTOUR NEXT EZ METER,CONTOUR NEXT LINK METER.
Note: Exceptions may apply. Please refer to theformulary plan for drug coverage and medication tierplacement. Drug exclusions may apply.
2tekaccu-chek aviva plusaccu-chek guide meglucose mtraccu-chek guide monitorsystemaccu-chek nanosmartviewaccutrend plusadvanced glucose meteradvocate blood glucosemonitoradvocate duoadvocate redi-codeadvocate redi-code duoadvocate redi-code plusagamatrix ampassure platinumassure prism multiblood glucose meterblood glucose monitoringblood-glucose metercaresens ncaresens n voicecaretouch glucosemonitoringcaretouch ketone-glucosesyschoicedm clarusclever chek blood glucosesystclever choiceclever choice blood glucsysclever choice hd glucosesystclever choice microclever choice proclever choice talkcontrol astcool blood glucosecool blood glucose meterdario blood glucosemonitordiatrue pluseasy plus iieasy stepeasy talk
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 3
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
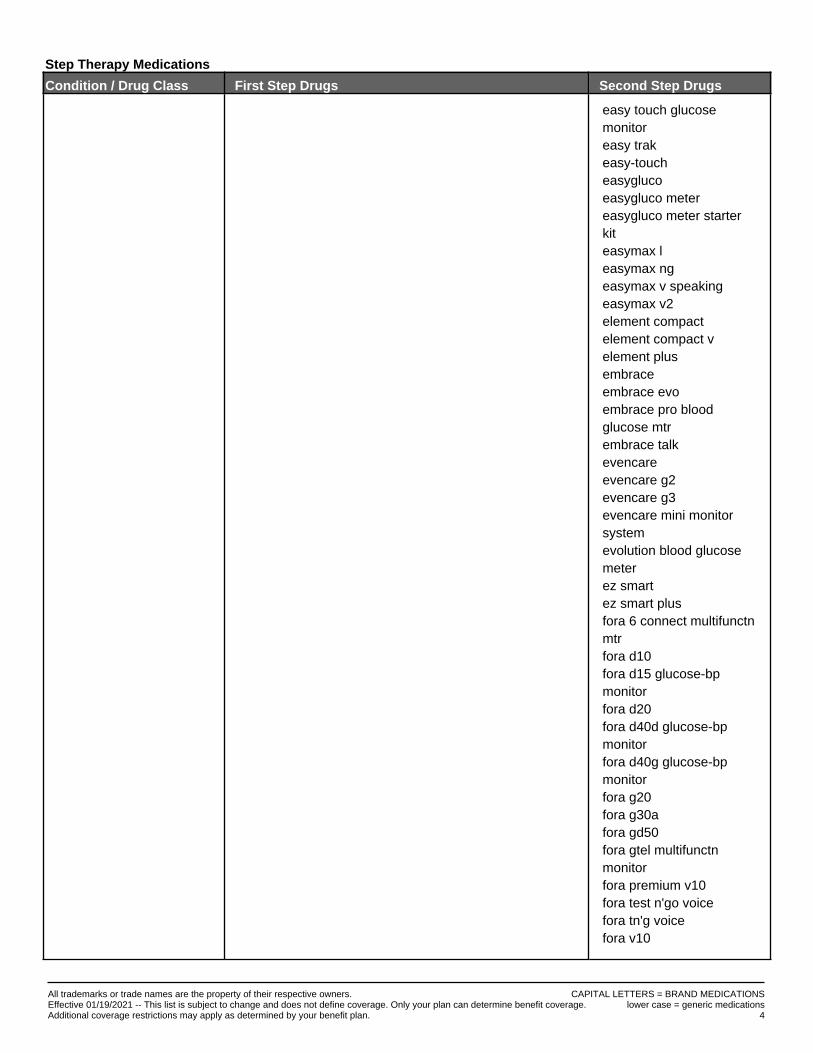
easy touch glucosemonitoreasy trakeasy-toucheasyglucoeasygluco metereasygluco meter starterkiteasymax leasymax ngeasymax v speakingeasymax v2element compactelement compact velement plusembraceembrace evoembrace pro bloodglucose mtrembrace talkevencareevencare g2evencare g3evencare mini monitorsystemevolution blood glucosemeterez smartez smart plusfora 6 connect multifunctnmtrfora d10fora d15 glucose-bpmonitorfora d20fora d40d glucose-bpmonitorfora d40g glucose-bpmonitorfora g20fora g30afora gd50fora gtel multifunctnmonitorfora premium v10fora test n'go voicefora tn'g voicefora v10
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 4
Step Therapy Medications
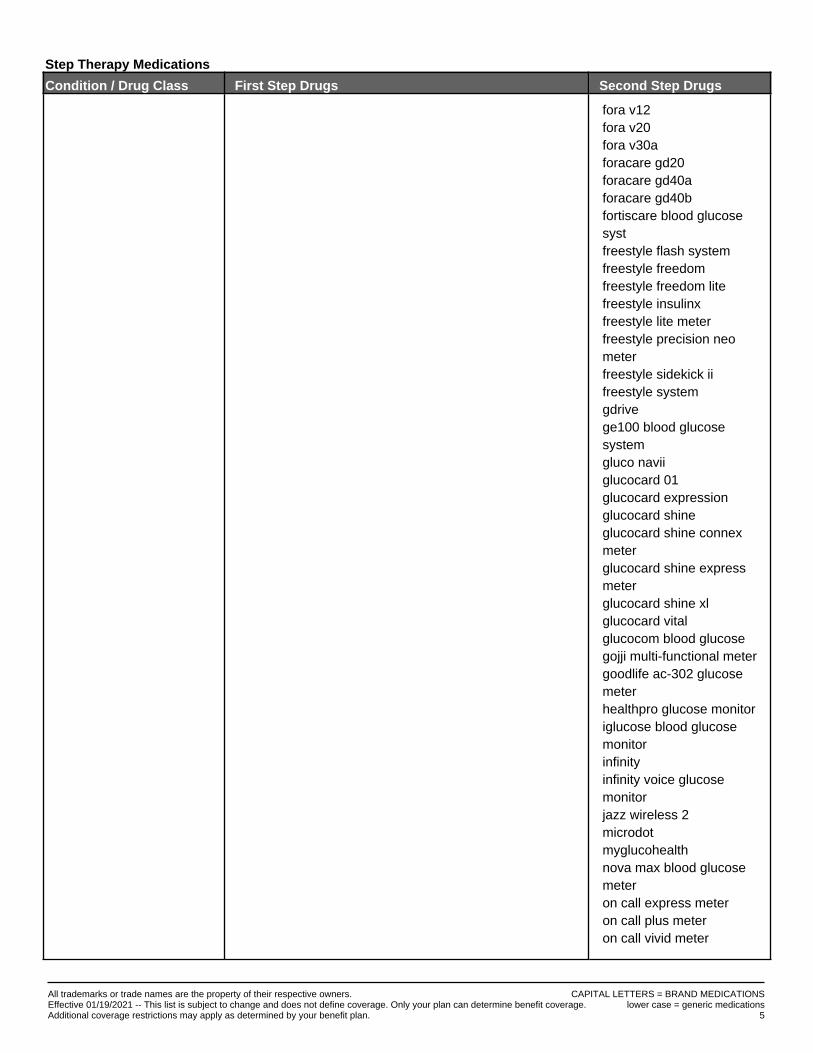
Condition / Drug Class First Step Drugs Second Step Drugs
fora v12fora v20fora v30aforacare gd20foracare gd40aforacare gd40bfortiscare blood glucosesystfreestyle flash systemfreestyle freedomfreestyle freedom litefreestyle insulinxfreestyle lite meterfreestyle precision neometerfreestyle sidekick iifreestyle systemgdrivege100 blood glucosesystemgluco naviiglucocard 01glucocard expressionglucocard shineglucocard shine connexmeterglucocard shine expressmeterglucocard shine xlglucocard vitalglucocom blood glucosegojji multi-functional metergoodlife ac-302 glucosemeterhealthpro glucose monitoriglucose blood glucosemonitorinfinityinfinity voice glucosemonitorjazz wireless 2microdotmyglucohealthnova max blood glucosemeteron call express meteron call plus meteron call vivid meter
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 5
Step Therapy Medications
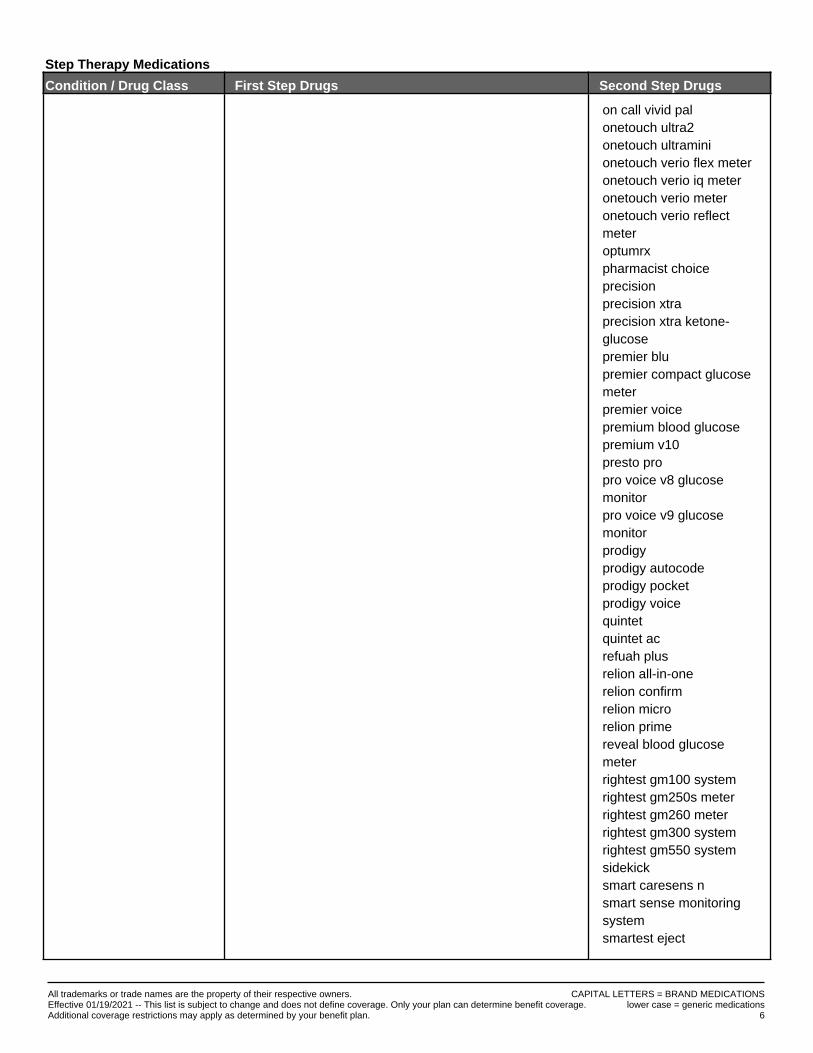
Condition / Drug Class First Step Drugs Second Step Drugs
on call vivid palonetouch ultra2onetouch ultraminionetouch verio flex meteronetouch verio iq meteronetouch verio meteronetouch verio reflectmeteroptumrxpharmacist choiceprecisionprecision xtraprecision xtra ketone-glucosepremier blupremier compact glucosemeterpremier voicepremium blood glucosepremium v10presto propro voice v8 glucosemonitorpro voice v9 glucosemonitorprodigyprodigy autocodeprodigy pocketprodigy voicequintetquintet acrefuah plusrelion all-in-onerelion confirmrelion microrelion primereveal blood glucosemeterrightest gm100 systemrightest gm250s meterrightest gm260 meterrightest gm300 systemrightest gm550 systemsidekicksmart caresens nsmart sense monitoringsystemsmartest eject
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 6
Step Therapy Medications
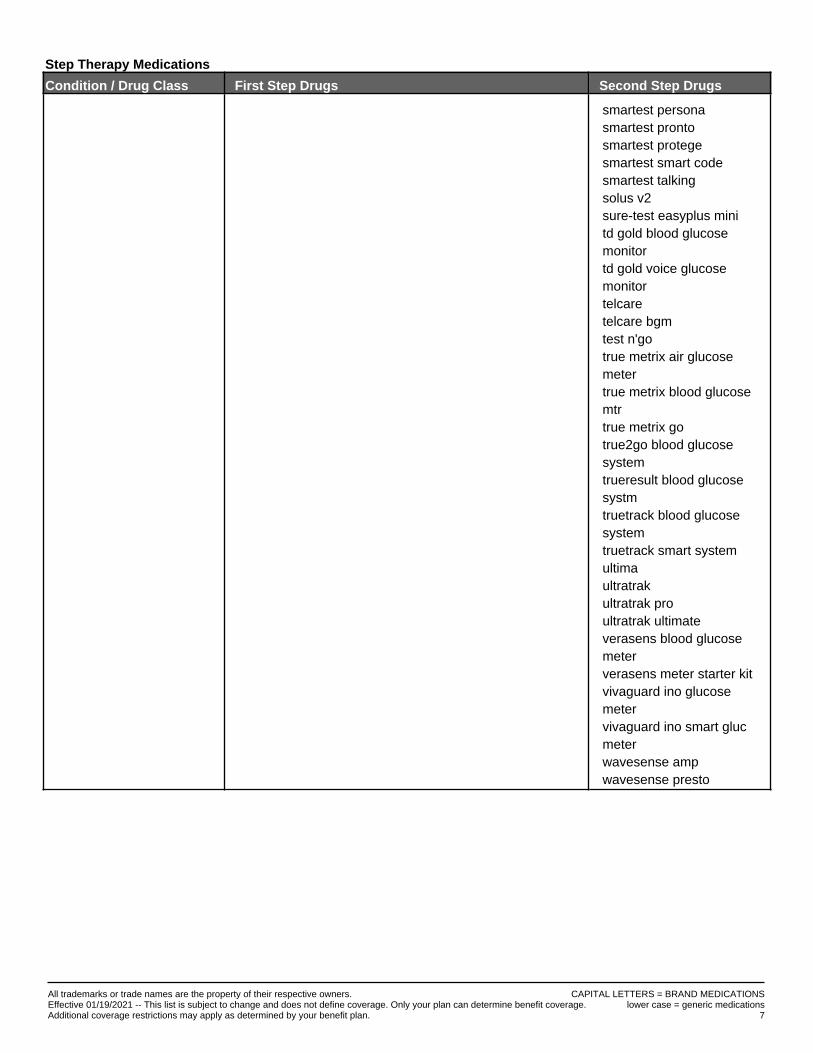
Condition / Drug Class First Step Drugs Second Step Drugs
smartest personasmartest prontosmartest protegesmartest smart codesmartest talkingsolus v2sure-test easyplus minitd gold blood glucosemonitortd gold voice glucosemonitortelcaretelcare bgmtest n'gotrue metrix air glucosemetertrue metrix blood glucosemtrtrue metrix gotrue2go blood glucosesystemtrueresult blood glucosesystmtruetrack blood glucosesystemtruetrack smart systemultimaultratrakultratrak proultratrak ultimateverasens blood glucosemeterverasens meter starter kitvivaguard ino glucosemetervivaguard ino smart glucmeterwavesense ampwavesense presto
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 7
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
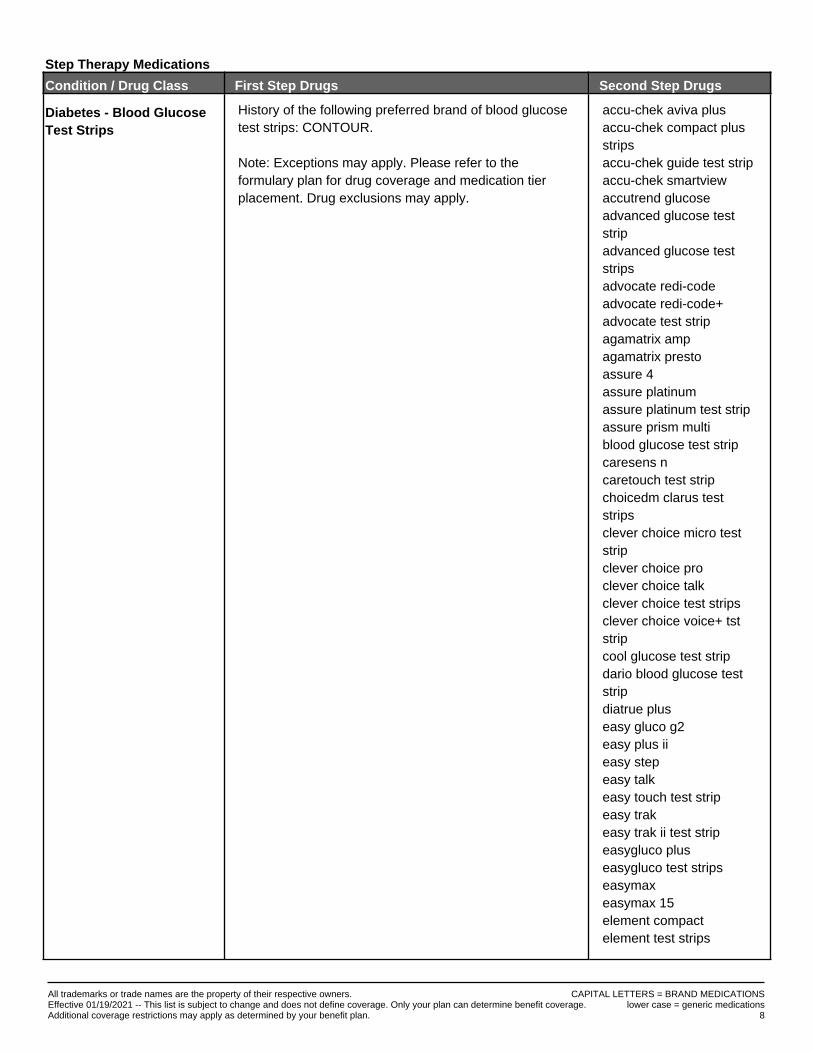
Diabetes - Blood GlucoseTest Strips
History of the following preferred brand of blood glucosetest strips: CONTOUR.
Note: Exceptions may apply. Please refer to theformulary plan for drug coverage and medication tierplacement. Drug exclusions may apply.
accu-chek aviva plusaccu-chek compact plusstripsaccu-chek guide test stripaccu-chek smartviewaccutrend glucoseadvanced glucose teststripadvanced glucose teststripsadvocate redi-codeadvocate redi-code+advocate test stripagamatrix ampagamatrix prestoassure 4assure platinumassure platinum test stripassure prism multiblood glucose test stripcaresens ncaretouch test stripchoicedm clarus teststripsclever choice micro teststripclever choice proclever choice talkclever choice test stripsclever choice voice+ tststripcool glucose test stripdario blood glucose teststripdiatrue pluseasy gluco g2easy plus iieasy stepeasy talkeasy touch test stripeasy trakeasy trak ii test stripeasygluco pluseasygluco test stripseasymaxeasymax 15element compactelement test strips
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 8
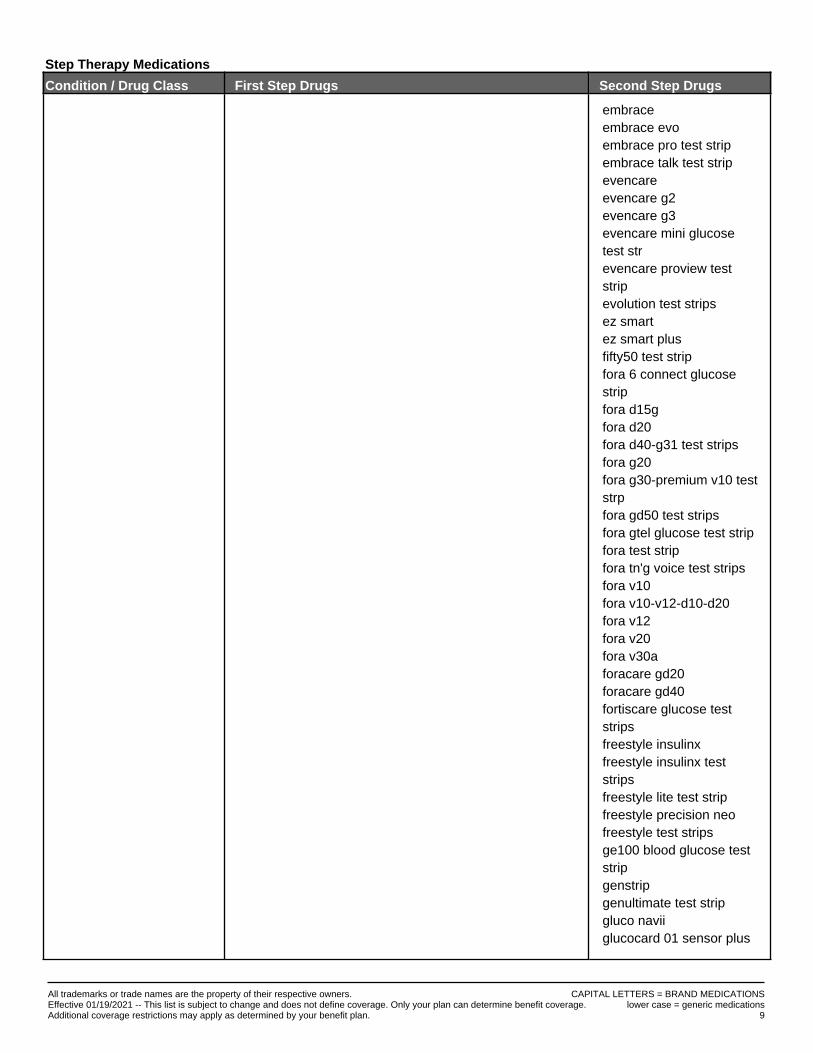
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
embraceembrace evoembrace pro test stripembrace talk test stripevencareevencare g2evencare g3evencare mini glucosetest strevencare proview teststripevolution test stripsez smartez smart plusfifty50 test stripfora 6 connect glucosestripfora d15gfora d20fora d40-g31 test stripsfora g20fora g30-premium v10 teststrpfora gd50 test stripsfora gtel glucose test stripfora test stripfora tn'g voice test stripsfora v10fora v10-v12-d10-d20fora v12fora v20fora v30aforacare gd20foracare gd40fortiscare glucose teststripsfreestyle insulinxfreestyle insulinx teststripsfreestyle lite test stripfreestyle precision neofreestyle test stripsge100 blood glucose teststripgenstripgenultimate test stripgluco naviiglucocard 01 sensor plus
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 9
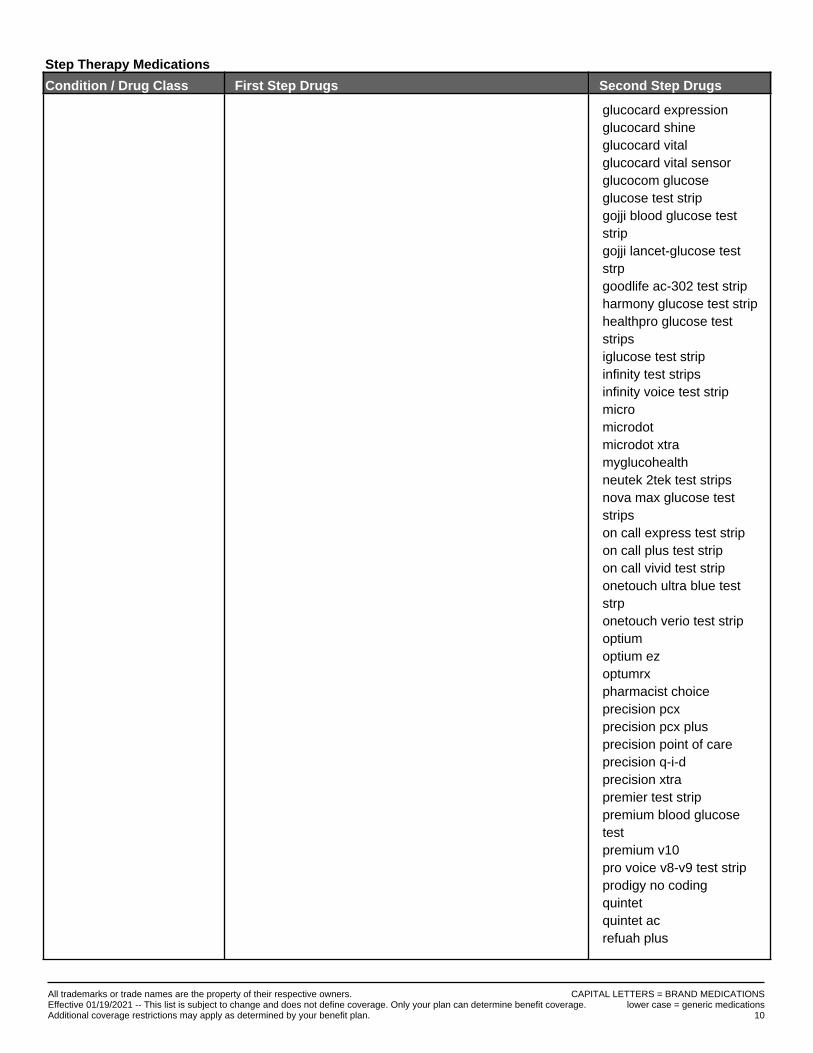
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
glucocard expressionglucocard shineglucocard vitalglucocard vital sensorglucocom glucoseglucose test stripgojji blood glucose teststripgojji lancet-glucose teststrpgoodlife ac-302 test stripharmony glucose test striphealthpro glucose teststripsiglucose test stripinfinity test stripsinfinity voice test stripmicromicrodotmicrodot xtramyglucohealthneutek 2tek test stripsnova max glucose teststripson call express test stripon call plus test stripon call vivid test striponetouch ultra blue teststrponetouch verio test stripoptiumoptium ezoptumrxpharmacist choiceprecision pcxprecision pcx plusprecision point of careprecision q-i-dprecision xtrapremier test strippremium blood glucosetestpremium v10pro voice v8-v9 test stripprodigy no codingquintetquintet acrefuah plus
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 10
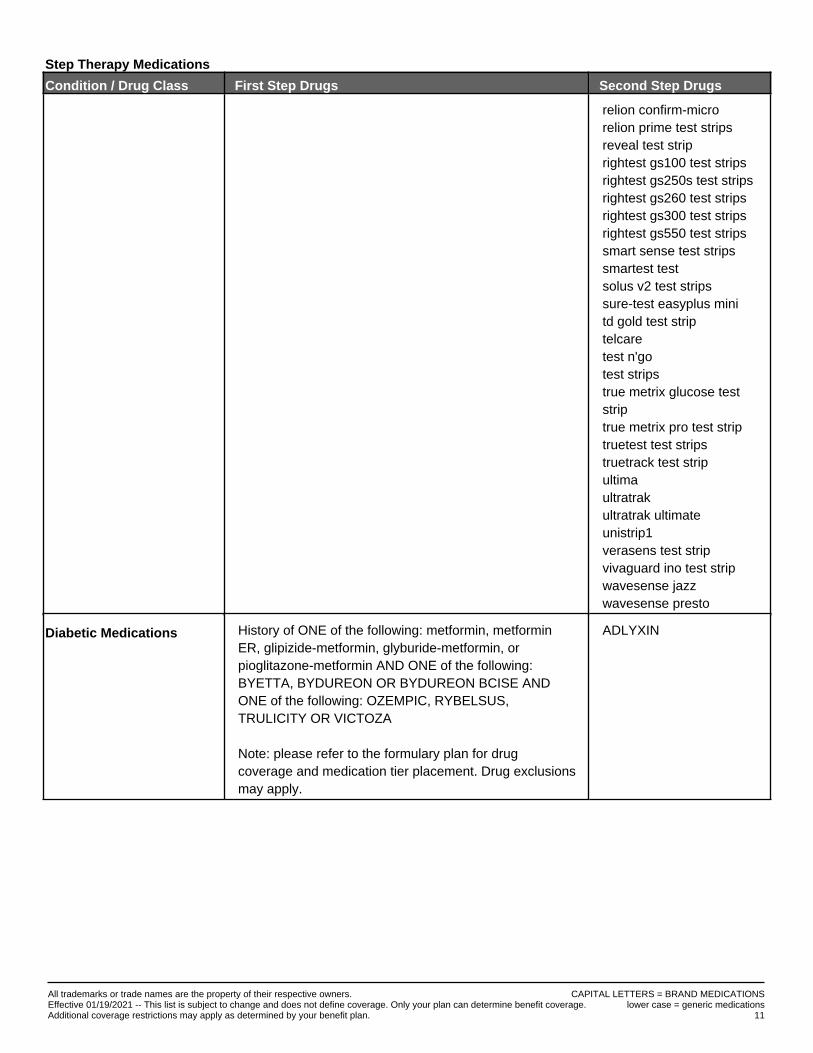
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
relion confirm-microrelion prime test stripsreveal test striprightest gs100 test stripsrightest gs250s test stripsrightest gs260 test stripsrightest gs300 test stripsrightest gs550 test stripssmart sense test stripssmartest testsolus v2 test stripssure-test easyplus minitd gold test striptelcaretest n'gotest stripstrue metrix glucose teststriptrue metrix pro test striptruetest test stripstruetrack test stripultimaultratrakultratrak ultimateunistrip1verasens test stripvivaguard ino test stripwavesense jazzwavesense presto
Diabetic Medications History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin, orpioglitazone-metformin AND ONE of the following:BYETTA, BYDUREON OR BYDUREON BCISE ANDONE of the following: OZEMPIC, RYBELSUS,TRULICITY OR VICTOZA
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
ADLYXIN
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 11
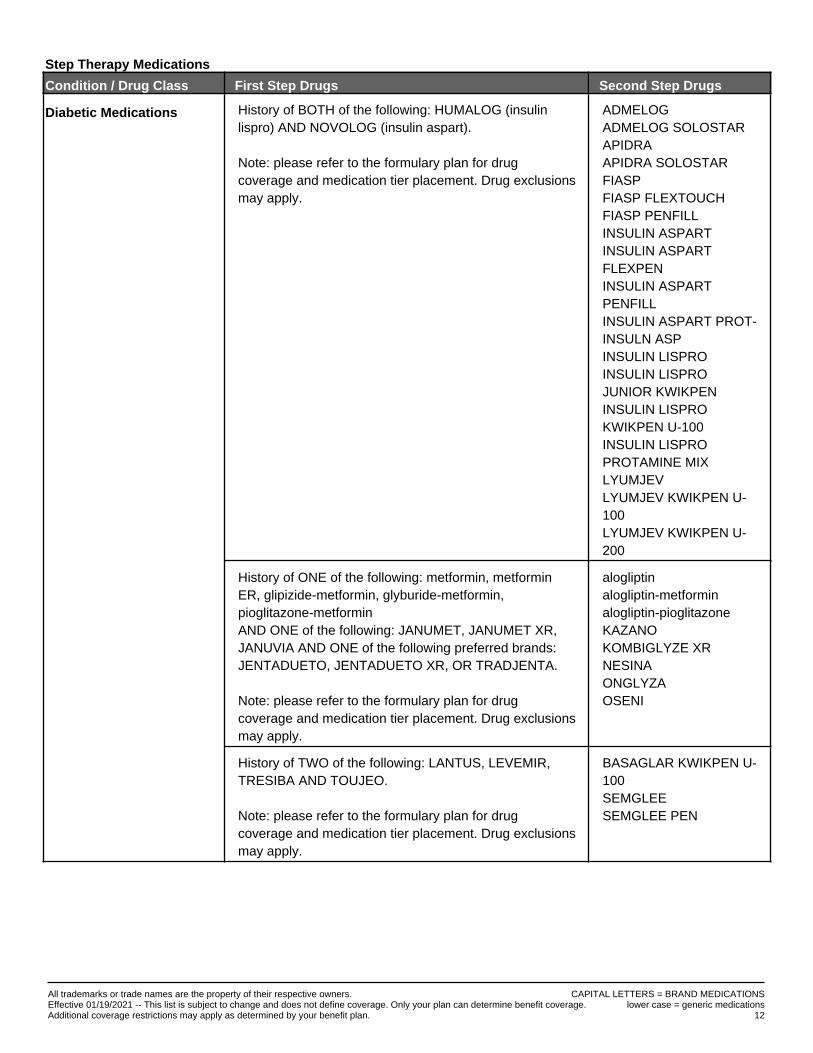
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
Diabetic Medications History of BOTH of the following: HUMALOG (insulinlispro) AND NOVOLOG (insulin aspart).
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
ADMELOGADMELOG SOLOSTARAPIDRAAPIDRA SOLOSTARFIASPFIASP FLEXTOUCHFIASP PENFILLINSULIN ASPARTINSULIN ASPARTFLEXPENINSULIN ASPARTPENFILLINSULIN ASPART PROT-INSULN ASPINSULIN LISPROINSULIN LISPROJUNIOR KWIKPENINSULIN LISPROKWIKPEN U-100INSULIN LISPROPROTAMINE MIXLYUMJEVLYUMJEV KWIKPEN U-100LYUMJEV KWIKPEN U-200
History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin,pioglitazone-metforminAND ONE of the following: JANUMET, JANUMET XR,JANUVIA AND ONE of the following preferred brands:JENTADUETO, JENTADUETO XR, OR TRADJENTA.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
alogliptinalogliptin-metforminalogliptin-pioglitazoneKAZANOKOMBIGLYZE XRNESINAONGLYZAOSENI
History of TWO of the following: LANTUS, LEVEMIR,TRESIBA AND TOUJEO.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
BASAGLAR KWIKPEN U-100SEMGLEESEMGLEE PEN
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 12
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
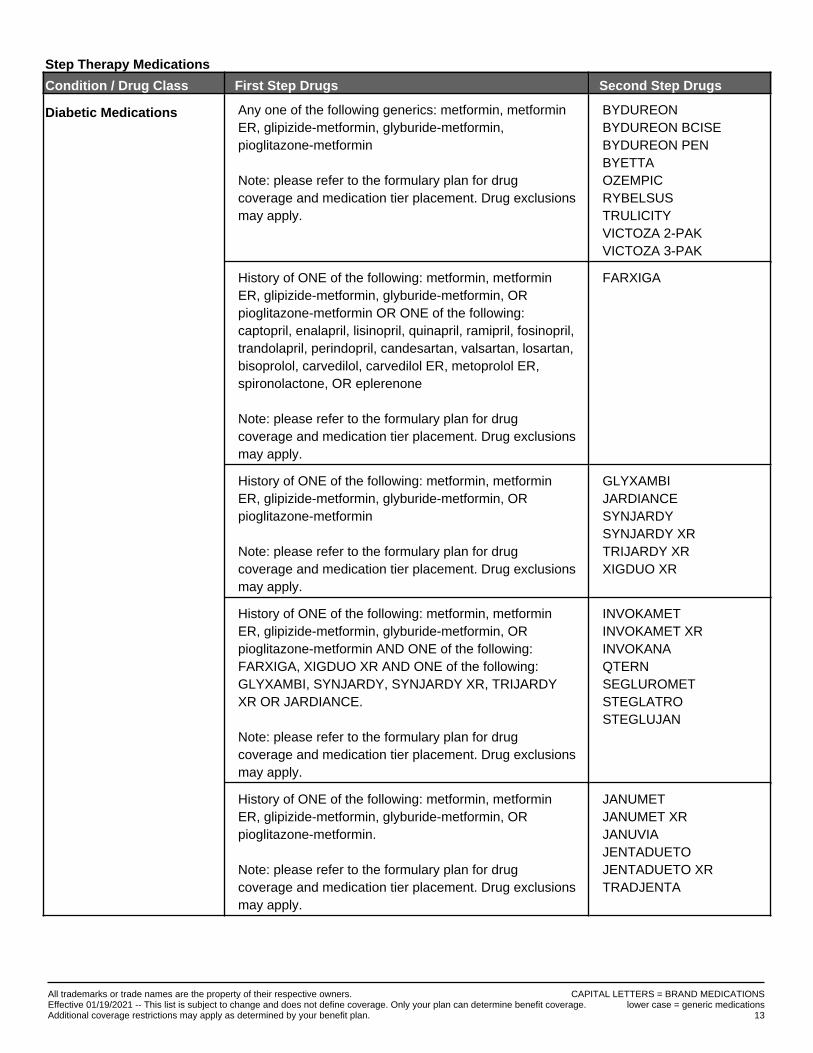
Diabetic Medications Any one of the following generics: metformin, metforminER, glipizide-metformin, glyburide-metformin,pioglitazone-metformin
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
BYDUREONBYDUREON BCISEBYDUREON PENBYETTAOZEMPICRYBELSUSTRULICITYVICTOZA 2-PAKVICTOZA 3-PAK
History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin, ORpioglitazone-metformin OR ONE of the following:captopril, enalapril, lisinopril, quinapril, ramipril, fosinopril,trandolapril, perindopril, candesartan, valsartan, losartan,bisoprolol, carvedilol, carvedilol ER, metoprolol ER,spironolactone, OR eplerenone
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
FARXIGA
History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin, ORpioglitazone-metformin
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
GLYXAMBIJARDIANCESYNJARDYSYNJARDY XRTRIJARDY XRXIGDUO XR
History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin, ORpioglitazone-metformin AND ONE of the following:FARXIGA, XIGDUO XR AND ONE of the following:GLYXAMBI, SYNJARDY, SYNJARDY XR, TRIJARDYXR OR JARDIANCE.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
INVOKAMETINVOKAMET XRINVOKANAQTERNSEGLUROMETSTEGLATROSTEGLUJAN
History of ONE of the following: metformin, metforminER, glipizide-metformin, glyburide-metformin, ORpioglitazone-metformin.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
JANUMETJANUMET XRJANUVIAJENTADUETOJENTADUETO XRTRADJENTA
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 13
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
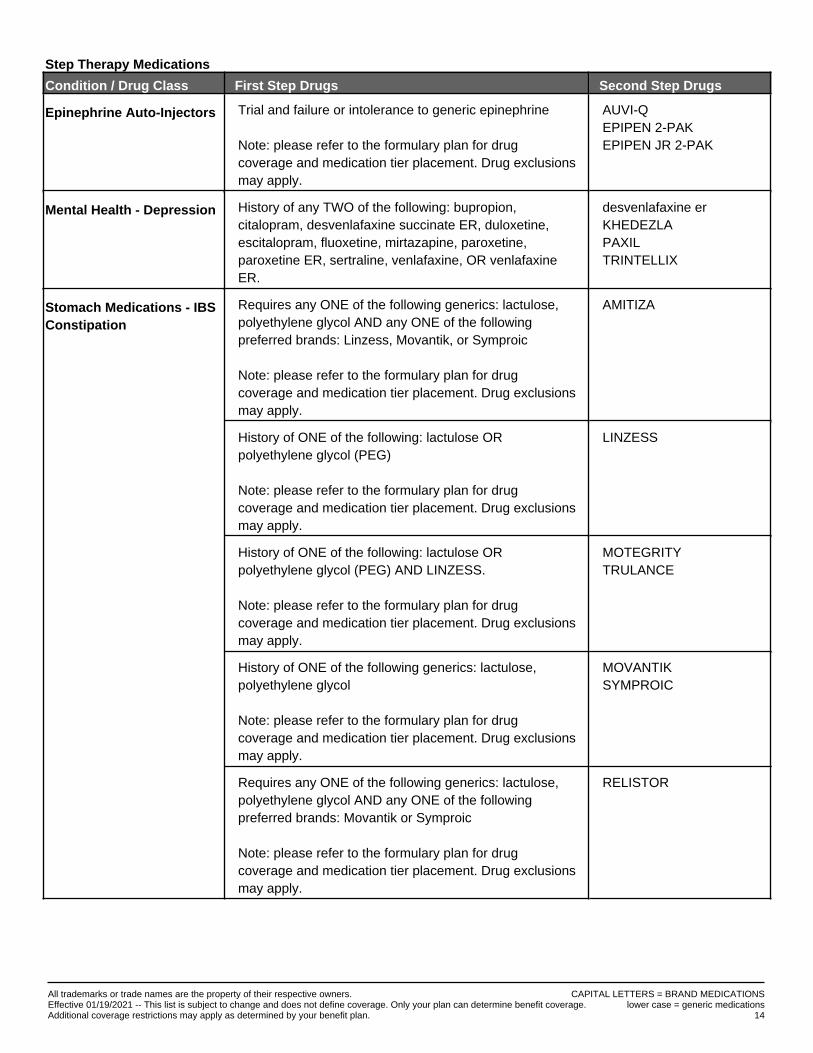
Epinephrine Auto-Injectors Trial and failure or intolerance to generic epinephrine
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
AUVI-QEPIPEN 2-PAKEPIPEN JR 2-PAK
Mental Health - Depression History of any TWO of the following: bupropion,citalopram, desvenlafaxine succinate ER, duloxetine,escitalopram, fluoxetine, mirtazapine, paroxetine,paroxetine ER, sertraline, venlafaxine, OR venlafaxineER.
desvenlafaxine erKHEDEZLAPAXILTRINTELLIX
Stomach Medications - IBSConstipation
Requires any ONE of the following generics: lactulose,polyethylene glycol AND any ONE of the followingpreferred brands: Linzess, Movantik, or Symproic
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
AMITIZA
History of ONE of the following: lactulose ORpolyethylene glycol (PEG)
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
LINZESS
History of ONE of the following: lactulose ORpolyethylene glycol (PEG) AND LINZESS.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
MOTEGRITYTRULANCE
History of ONE of the following generics: lactulose,polyethylene glycol
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
MOVANTIKSYMPROIC
Requires any ONE of the following generics: lactulose,polyethylene glycol AND any ONE of the followingpreferred brands: Movantik or Symproic
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
RELISTOR
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 14
Step Therapy Medications
Condition / Drug Class First Step Drugs Second Step Drugs
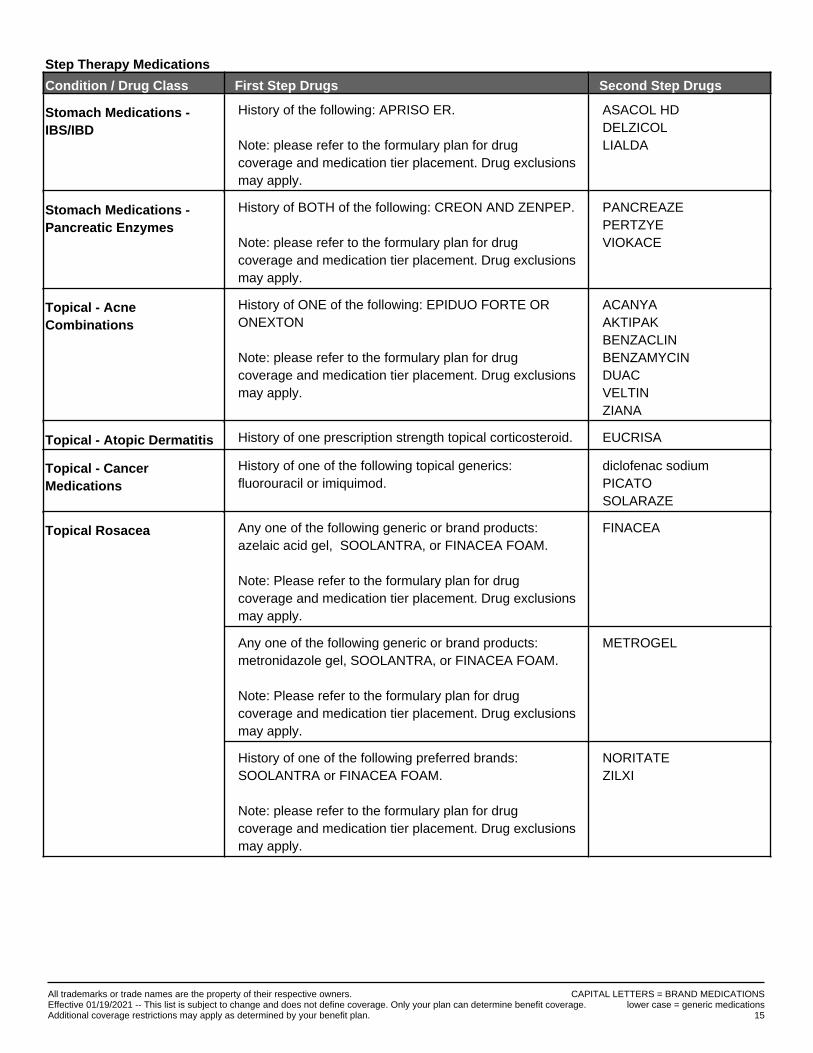
Stomach Medications -IBS/IBD
History of the following: APRISO ER.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
ASACOL HDDELZICOLLIALDA
Stomach Medications -Pancreatic Enzymes
History of BOTH of the following: CREON AND ZENPEP.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
PANCREAZEPERTZYEVIOKACE
Topical - AcneCombinations
History of ONE of the following: EPIDUO FORTE ORONEXTON
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
ACANYAAKTIPAKBENZACLINBENZAMYCINDUACVELTINZIANA
Topical - Atopic Dermatitis History of one prescription strength topical corticosteroid. EUCRISA
Topical - CancerMedications
History of one of the following topical generics:fluorouracil or imiquimod.
diclofenac sodiumPICATOSOLARAZE
Topical Rosacea Any one of the following generic or brand products:azelaic acid gel, SOOLANTRA, or FINACEA FOAM.
Note: Please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
FINACEA
Any one of the following generic or brand products:metronidazole gel, SOOLANTRA, or FINACEA FOAM.
Note: Please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
METROGEL
History of one of the following preferred brands:SOOLANTRA or FINACEA FOAM.
Note: please refer to the formulary plan for drugcoverage and medication tier placement. Drug exclusionsmay apply.
NORITATEZILXI
CAPITAL LETTERS = BRAND MEDICATIONSlower case = generic medications
All trademarks or trade names are the property of their respective owners.Effective 01/19/2021 -- This list is subject to change and does not define coverage. Only your plan can determine benefit coverage.Additional coverage restrictions may apply as determined by your benefit plan. 15
DISCRIMINATION IS AGAINST THE LAW Final Rule Under Section 1557 for Nondiscrimination
and Accessibility RequirementsWe comply with applicable Federal civil rights laws and the Minnesota Human Rights Act. We do not discriminate against, exclude, or treat people differently
or deny any person the full and equal enjoyment of the goods, services, facilities, privileges, advantages, and accommodations of a place of public
accommodation because of race, color, creed, religion, national origin, marital status, age, disability, sexual orientation or sex.
We provide free aids and services to help people communicate effectively with us, such as:
• Qualified sign language interpreters, call 612-273-3780.
• TTY for hearing and language impaired, dial 711.
• Qualified spoken language interpreters, for people whose preferred language is not English, call 1-844-278-9798
• Written information in other languages and formats (such as large print, audio and accessible electronic formats), call 612-273-3780.
If you believe that we have failed to provide these services or discriminated in another way on the basis of race, color, creed, religion, national origin, marital
status, age, disability, sexual orientation or sex, you can file a grievance with your facility in person or by mail, fax or email. The contacts listed below will help
you. For a copy of our grievance procedure, go to: http://www.fvfiles.com/524620.pdf.
ClearScriptSM Fairview Pharmacy ServicesCorporate Office, 711 Kasota Ave. S.E., Minneapolis, MN 55414Phone: 612-617-3513 Fax: 612-672-5201 Email: [email protected]
You can also file a non-discrimination complaint with the U.S. Department of Health and Human Services and/or Minnesota Department of Human Rights:
U.S. Department of Health and Human Services, Office for Civil Rights:
• Electronically through the Office for Civil Rights Complaint Portal, available at: https://ocrportal.hhs.gov/ocr/portal/lobby.jsf.
• By mail at: U.S. Department of Health and Human Services, 200 Independence Avenue SW, Room 509F, HHH Building, Washington, D.C. 20201.
• By phone:1-800-368-1019, 800-537-7697 (TDD).
• Complaint forms are available at: http://www.hhs.gov/ocr/office/file/index.html.
Minnesota Department of Human Rights:
• Electronically through the MDHR complaint inquiry form, available at https://b5.caspio.com/dp.asp?AppKey=18a340001049f4ae67b24974b4ec.
• By mail at: Minnesota Department of Human Rights, 625 Robert Street North, Saint Paul, MN 55155.
• By phone: 651.539.1100 (TTY 651.296.1283) or Toll Free at 800.657.3704.
LANGUAGE SERVICES 1-844-278-9798 (TTY: 711) – Available 24 Hours
ATTENTION: Language assistance services, free of charge, are available to you. Call 1-844-278-9798.
SomaliFIIRO GAAR AH: Hadii aad ku hadasho Soomaali,
waaxda luqadaha,qaybta kaalmada adeegyada, waxay idiin hayaan adeeg kharash la’aan ah.
So wac 1-844-278-9798.
SpanishATENCIÓN: si habla español, tiene a su disposición
servicios gratuitos de asistencia lingüística. Llame al 1-844-278-9798.
page 1 of 2
VietnameseCHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn.
Gọi số 1-844-278-9798.
Arabic ملحوظة: إذا كنت تتحدث اللغة العربية، فإن خدمات
المساعدة اللغوية تتوافر لك بالمجان. اتصل برقم 1-844-278-9798.
RussianВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода. Звоните
1-844-278-9798.
OromoXIYYEEFFANNAA: Afaan dubbattu Oroomiffa, tajaajila gargaarsa afaanii, kanfaltiidhaan ala,
ni argama. Bilbilaa 1-844-278-9798.
HmongLUS CEEV: Yog tias koj hais lus Hmoob,
cov kev pab txog lus, muaj kev pab dawb rau koj. Hu rau 1-844-278-9798.
Chinese注意:如果您使用繁體中文,您可以免費獲得語言援助服
務。請致電 1-844-278-9798。
Amharicማስታወሻ: የሚናገሩት ቋንቋ ኣማርኛ ከሆነ የትርጉም እርዳታ
ድርጅቶች፣ በነጻ ሊያግዝዎት ተዘጋጀተዋል፡ ወደ ሚከተለው ቁጥር ይደውሉ 1-844-278-9798.
Cambodian
Laoໂປດຊາບ: ຖ າ້ວ່າ ທ່ານເວົ າ້ພາສາ ລາວ,
ການບໍລິການຊ່ວຍເຫຼື ອດ າ້ນພາສາ, ໂດຍບໍ່ເສັຽຄ່າ, ແມ່ນມີພ ອ້ມໃຫ ທ້່ານ. ໂທຣ 1-844-278-9798.
Korean주의: 한국어를 사용하시는 경우, 언어 지원 서비스를
무료로 이용하실 수 있습니다. 1-844-278-9798 번으로 전화해 주십시오.
FrenchATTENTION: Si vous parlez français, des services d’aide linguistique vous sont proposés gratuitement.
Appelez le 1-844-278-9798.
Farsi
Karen
1-844-278-9798
TagalogPAUNAWA: Kung nagsasalita ka ng Tagalog, maaari
kang gumamit ng mga serbisyo ng tulong sa wika nang walang bayad. Tumawag sa 1-844-278-9798.
French CreoleATANSYON: Si w pale Kreyòl Ayisyen, gen sèvis èd pou
lang ki disponib gratis pou ou. Rele 1-844-278-9798.
PolishUWAGA: Jeżeli mówisz po polsku, możesz skorzystać z
bezpłatnej pomocy językowej. Zadzwoń pod numer 1-844-278-9798.
PortugueseATENÇÃO: Se fala português, encontram-se disponíveis
serviços linguísticos, grátis. Ligue para 1-844-278-9798.
Italian ATTENZIONE: In caso la lingua parlata sia l’italiano,
sono disponibili servizi di assistenza linguistica gratuiti. Chiamare il numero 1-844-278-9798.
Japanese 注意事項:日本語を話される場合、無料の言語支援をご利用いただけます。1-844-278-9798 まで、お電話にてご連絡
ください。
German ACHTUNG: Wenn Sie Deutsch sprechen, stehen
Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer 1-844-278-9798.
1-844-278-9798
SW 545531 . Rev. 03.18
1-844-278-9798
page 2 of 2





























