-
Gut 1995; 37: 309-313
Memory metal stents for palliation of malignantobstruction of
the oesophagus and cardia
A May, M Selmaier, J Hochberger, L Gossner, S Miihldorfer, E G
Hahn, C Ell
AbstractThirty patients with incurable malignantobstruction of
the oesophagus and cardiawere treated with self expanding
oeso-phageal memory metal stents (Ultraflex) ina prospective study.
The endoprostheseswere successfully placed in all patients.Within
one week after implantation dys-phagia had improved in 25 of 30
patients(830/o). Stent expansion was incompletewithin one week
after implantation in 12 of30 patients (40%). After an average of
twodilatation sessions eight of 12 stents hadexpanded completely.
Five patientscomplained of retrosternal pain and threeof them
suffered from heartburn overseveral days despite acid inhibition.
Majorproblems in the follow up period occurredin 10 of 30 patients
(30%) and included lateperforation (one) and tumour
ingrowth/overgrowth (nine). All of these complica-tions were
treated endoscopically.Improvement of the dysphagia of thepatients
with tumour ingrowthlover-growth lasted for about eight
weeks(median; range: 2-38 weeks). UntilNovember 1994 six of 30
patients were stillalive with a survival time of 309 days(median;
range: 103-368 days). It is con-cluded that oesophageal memory
metalstents are easy to implant, prove effectivein the palliation
of malignant oesophagealobstructions, and have a low risk of
severecomplications. The only disadvantagesare that incomplete
initial stent expansionas well as tumour
ingrowthlovergrowthoccurred in nearly one third ofthe patients.(Gut
1995; 37: 309-313)
Keywords: stents, malignant oesophageal stenoses.
Department ofMedicine I, UniversityofErlangen-Nuremberg,
GermanyA MayM SelmaierJ HochbergerL GossnerS MLihldorferE G HahnC
Ell
Correspondence to:Professor Dr med ChristianEll, Medizinische
Klinik Imit Poliklinik,
UniversitatErlangen-Niirnberg,Krankenhausstr 12, 91054Erlangen,
Germany.Accepted for publication10 January 1995
In the past few years the search for an effectivemethod of
palliative treatment with a low rateof complications and suitable
for the treatmentof incurable malignant oesophageal stenoseshad led
to the development and clinical appli-cation of various types of
self expanding metalendoprostheses.1-13 Most reports concernedthe
Wallstent endoprosthesis version.2 3 6 8 12But first clinical
experiences with stents madeof memory metal (nitinol) have also
beenreported.' 4 5 9 10 In most cases, only a smallnumber of
patients received treatment, how-ever, or the reports are available
only in theform of abstracts. Until now only one fullpaper from a
radiological centre with memorymetal stents (Ultraflex) in a larger
number ofpatients (40) has been published.1 Memorymetal
endoprostheses of the Ultraflex type,
which have recently been redesigned have beenavailable in
Germany in the improved versionsince August 1993. We report on our
pre-liminary clinical experiences in implementingthe new version of
this stent in 30 consecutivepatients.
Methods
PatientsFrom August 1993 to August 1994 a total of30 patients
with incurable tumours of theoesophagus and the cardia were treated
withself expanding metal endoprostheses of thememory metal stent
type (Ultraflex,Microvasive Boston Scientific, MA, USA) in
aprospective study. Twenty five patients weremen and five were
women. Their age rangedfrom 43 to 90 years with a mean (SD) of
65(12) years. Histologically, a squamous cellcarcinoma was found in
15 of 30 patients(50%), an adenocarcinoma in eight (27%),and an
anaplastic carcinoma in two (7%)patients. One patient had lung
cancer andanother patient a metastatic cancer of thethyroid gland,
both leading to an oesophagealobstruction. A histological
examination of thetumour was omitted in three patients, becausethe
malignancy had been conclusively con-firmed by imaging techniques
or by assessmentof the course of the disease. Most patients
(19)showed the obstructive lesion in the distal partof the
oesophagus and the gastro-oesophagealjunction. In five patients,
the tumour waslocated in the mid-section and in two patientsin the
proximal part of the oesophagus. Twoother patients had a tumour
recurrence at theanastomosis of an earlier gastrectomy
andoesophageal resection, respectively. The lengthof the tumour
stenosis ranged from 3 to 18 cm(mean (SEM) 7 (3) cm).
Seven of 30 patients suffered from dysphagiafor solid foods
alone (23%), 11 patients (37%)for semisolid foods, and 12 patients
(40%) forliquids. Most of the patients (24 of 30) hadreceived
previous treatment in the form ofbougienage (19), laser therapy
(eight), dilata-tion (one), and percutaneous
endoscopicallycontrolled gastrotomy (PEG) (three).
Stent materials and implantation techniqueThe self expanding
metal prostheses used werememory metal stents (Ultraflex), designed
foruse within the oesophagus. The stent mesh isknitted from a
single elastic wire, consisting ofa nickel-titanium alloy
(nitinol), also referredto as memory metal. When fully expanded,
thestent has a diameter of 18 mm. The upper end
309
on March 31, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.37.3.309 on 1 S
eptember 1995. D
ownloaded from
http://gut.bmj.com/
-
May, Selmaier, Hochberger, Gossner, Miihldorfer, Hahn, Ell
is shaped like a tulip and measures 20 mm indiameter to improve
the anchoring of the stentto the oesophageal wall. The prosthesis
is avail-able in three different lengths (7 cm, 10 cm,and 15
cm).The prosthesis is mounted in a compressed
state on the stent delivery system consisting of
A
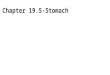
Figure 1: Tumour stenosis in the mid-section of the oesophagus
beforeimplantation (B, C).
a stabiliser and is encased in a soluble gelatin.The stabiliser
is fairly flexible and enclosed in atransparent plastic protective
sheath with anouter diameter of 8 mm. The tapered tip at thedistal
end of the stabiliser, which has a lumenfor a 0.038 guidewire,
favours the deliverysystem pass through tight strictures.
Fourradio-opaque markers are attached to thestabiliser. The two
outer ones mark the ends ofthe stent in the compressed state and
the innerones mark the ends of the expanded andtherefore shortened
stent. To release the stent,the proximal end of the stabiliser is
held steadywhile the outer plastic sheath is evenlyretracted. Upon
exposure to oesophagealfluids, the gelatin dissolves within three
to fiveminutes, resulting in expansion of the stent.Finally the
inner stabiliser is removed.
Before stent implantation, patients receiveda mild sedoanalgesia
with 5-10 mg diazepamand 50 mg meperidine intravenously. If
neces-sary, the stenosis was pretreated by laser coag-ulation or
bougienage, or both, until asatisfactory dilatation was achieved.
Generally,a diameter of 12 mm was considered to belarge enough to
permit an endoscope with aminimum diameter of 10 mm to pass the
stric-ture easily. After placement of a guidewire theentire length
of the tumour stenosis was pre-cisely measured while retracting the
endoscopeto calculate the correct stent length. Ideally,the stent
should extend beyond the margins ofthe tumour at both ends by at
least 3 cm. Incase of stenosis in the gastro-oesophageal junc-tion
the proximal extension of the stent endsbeyond the tumour margins
should be at least5 cm. With patients in a supine position,metallic
markers were attached to the patient'sskin at the distal and
proximal border of thestricture. Under fluoroscopic control the
stentswere inserted over the guidewire in the waydescribed.
Immediately after stent placementan endoscopy was performed to
verify the posi-tion, expansion, and anchoring of the proximalpart
of the stent. A complete passage throughthe stent was not forced
because of theincreased risk of stent displacement. The
stentopening was checked endoscopically andradiologically one or
two days after implanta-tion (Fig 1). If the endoprosthesis had
notexpanded sufficiently one day after implanta-tion, the stent
diameter was increased bymeans of balloon dilatation. The balloons
were15 and 18 mm in diameter and 8 cm in length(Rigiflex,
Microvasive Boston Scientific,Watertown, MA, USA). Until the stent
posi-tion was checked the patients were advised totake only
liquids. Thereafter they had semi-solid or solid foods, as
individually toleratedand were advised to avoid stringy meat,
greensalads, and cheese spread, even if they had nodysphagia after
stent implantation. Antirefluxmeasures (proton pump inhibitor and
aprokinetic agent) were given to patients whoseprosthesis extended
beyond the gastro-oeso-phageal junction. In accordance with the
studyprotocol an endoscopic follow up examinationand a short
medical history were carried outevery four weeks. Only four
patients refusedto undergo further endoscopies and were
310
on March 31, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.37.3.309 on 1 S
eptember 1995. D
ownloaded from
http://gut.bmj.com/
-
Memory metal stents for palliation of malignant obstruction of
the oesophagus and cardia
TABLE I Dysphagia before and after stent placement (- 7days
after implantation) (30 patients)
Before Afterimplantation implantation
No dysphagia 0 11Dysphagia for solid food alone 7 12*Dysphagia
for semisolid food 11 6Dysphagia for liquid food 12 it
*One patient was able to eat solid food with exception of
meatand another patient with the exception of both meat andbrown
bread, whereas before stent implantation neither patientcould
ingest solid food.tPsychogenic dysphagia, sufficient stent
expansion.
questioned as to their symptomatic conditionover the telephone
at regular intervals.
ResultsStent placement was successful in all 30patients. There
were no technical problemsduring stent placement, except for one
case ofa premature user induced expansion of anendoprosthesis. The
entire system wasremoved and a new stent was placed
withoutproblems. Every patient was treated with onlyone
endoprosthesis. Twenty three of 30patients were provided with a
stent 15 cm inlength. In five cases the stent had a length of 10cm
and in two cases 7 cm. One week after stentimplantation 25 of 30
patients (83%) showedan improvement of dysphagia, five patients(1
7%) reported unchanged difficulties inswallowing (Table I). In four
patients adysphagia for solid food and in one patient adysphagia
for liquids remained. In two of thesefour patients this occurred
despite a satisfac-tory stent passage after two dilatation
sessions(one of two patients), which had served toimprove an
initially insufficient stent expan-sion. In the third patient it
was not possible toachieve a complete expansion of the stentdespite
five dilatation sessions. Another patientcould only eat semisolid
foods because ofrecurrent chest pain and strong irritation of
thethroat. One patient suffered from a psy-chogenic dysphagia and
could not eat anyfood, although the stent was fully expanded.
Severe early complications (S7 days afterimplantation), for
example, stent migration,bleeding or perforation did not occur.
Minorproblems, which were seen in 21 of 30patients, included
insufficient opening of theprosthesis up to 48 hours after
implantation in17 patients. A complete expansion of the
stentwithout the need for further treatment withinone week after
placement was seen in five of
TABLE II Acute and intermediate problems afterimplantation of
the endoprosthesis (26 patients)
Patients (n) %
Acute problemsInsufficient stent expansion requiring
dilatation treatment 12 40Retrosternal pain 8 27Pyrosis despite
antireflux measures and
acid inhibition 3 11Intermediate problemsRecurrent dysphagia
caused by tumour
ingrowth/overgrowth* 9 30Perforation 1 4
*Endoscopically verified in six patients, three patients
refusedre-endoscopy.
these 17 patients, whereas the remaining 12patients (40°/)
required dilatation treatment(Table II). After an average of two
dilatationsessions using a balloon catheter (range 1-5)eight of 12
stents had expanded completely,that is to say, to a point where a
standard endo-scope could have been moved through thestent without
resistance. One of four patientswith an insufficient expansion
despite dilata-tion died three days after stent implantationand
before completion of the dilatation treat-ment in consequence of a
progressiveKorsakow syndrome and a blood sugar distur-bance. The
exact cause of death could not beestablished because the relatives
of thedeceased patient did not consent to a necropsy.In the second
patient a sufficient stent expan-sion could not be achieved,
because the lengthof the tumour - which had reached anadvanced
stage - was 17 cm. In the thirdpatient a pronounced compression of
thetumour from outside was ascertained, whichcould be treated only
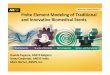
partially by dilatationtreatment. In another patient with a
remainingstenosis in the region of the cardia despite
fivedilatation sessions after stent placement aGianturco-Z-stent
was successfully implanted,which showed a sufficient expansion with
48hours (Fig 2). Eight patients complained ofchest pain, three of
them had acute pain sensa-tions over a period of several days, and
one ofthem also had a foreign body sensation. Threepatients
suffered from severe heartburn despiteantireflux measures and acid
inhibition overseveral days, which disappeared with increasedoral
intake of food. One patient reportedintermittent moderate pyrosis
(Table II).During the follow up period nine patientsagain developed
increasing dysphagia eightweeks (median; range: 2-38 weeks) after
stentplacement. Tumour ingrowth/overgrowth wasassumed and
endoscopically diagnosed in sixpatients. The other three patients
refusedfurther endoscopies and were fed by the PEGonly. Patients
with tumour ingrowth/over-growth were retreated by
electrocoagulation ofthe tumour tissue. In one patient
dilatationtreatment was carried out. Two patientsreceived a second
stent, one memory metalendoprosthesis and one Gianturco-Z-stent.
Inone patient with an oesophageal carcinoma aperforation occurred
about three weeks afterplacement of the endoprosthesis. The
patientwho complained of an increasing irritation ofthe throat was
examined and an oesophagotra-cheal fistula was diagnosed. An
elastic trachealprosthesis was subsequently inserted and thefistula
was sealed with a histoacrylic adhesiveby approaching the fistula
from the oesophagus(Table II). The final radiographic controlimages
showed no further signs of contrastmedium passing into the tracheal
system. Thepatient survived for another 18 weeks aftertreatment.
Table II lists the complications thatoccurred. In the remaining
group of 20patients no late complications have arisen todate. Until
14 November 1994, six of 30patients were still alive with a
survival time of309 days (median; range: 103-368 days).Twenty three
patients had died after a survival
311
on March 31, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.37.3.309 on 1 S
eptember 1995. D
ownloaded from
http://gut.bmj.com/
-
May, Selmaier, Hochberger, Gossner, Miihldorfer, Hahn, Ell
A
Figure 2: Tumour stenosis in the region of the
gastro-oesophageal junction with aninsufficient memory metal stent
expansion despite dilatation after placement (A) and goodpassage
after implantation ofa Gianturco-Z-stent (B).
time of 70 days (median; range: 3-21 1 days).One patient
returned to his native country(Croatia) and therefore was no longer
availablefor further follow up.
DiscussionGastroenterological experiences concerningthe
application of self expanding Ultraflexmemory metal (nitinol)
stents in the oeso-phagus have been reported to date only in
theform of abstracts or short communications5 9 10with the
exception of one full paper publishedin a radiological journal.'
Technical problemswith the stent release that we and other
users10also had with the previous stent version, didnot occur using
the redesigned and improvedstent, which has been commercially
availablein Germany since August 1993. Until nowthere have been no
prospective randomisedstudies comparing the different stent types,
butaccording to our experience the implantationprocedure is easier
to carry out with thememory metal stent (Ultraflex) than
theoesophageal endoprostheses of Wallstent typein its original
construction design.2 8 Obliquestent positions or stent migration
as seen byour group when using the Wallstent prosthesis2did not
occur with the Ultraflex stent versions.One reason for this could
be attributed to thestent length of up to 15 cm, which permits
abetter coaxial positioning of the prosthesis inthe oesophagus,
particularly in stenosis of the
gastro-oesophageal junction. Whereas themaximum length of a
fully expanded Wallstentprosthesis was only 11 cm. Furthermore,
thematerial properties and design specifications ofthe Ultraflex
stent give it a flexibility that canprove to be a particular
advantage in managingkinking stenoses in the region of the
gastro-oesophageal junction.On the other hand, the Ultraflex
memory
metal stent seems to offer a lower force ofexpansion. Cwikiel et
al1 reported on the needfor balloon dilatation after stent
placementbecause of insufficient expansion in 38% ofpatients. The
results of Raijman et al9 showedthat even in 71% of patients
dilatation treat-ment was performed, although some treatmentwas
immediately after placement. To our expe-rience about half of the
patients provided witha memory metal stent initially showed an
insuf-ficient degree of spontaneous expansion, thusrequiring 40% of
the patients to have one orseveral dilatation treatments. With the
excep-tion of three patients maximum stent expan-sion could be
achieved in all cases at the latestafter five dilatation sessions.
One of threepatients with an incompletely expanded stenthad a
particularly long tumour stenosis of 17cm and two had a strong
external compressionof the tumour. In contrast,
retreatmentsentailing dilatation because of incomplete
stentexpansion, which became necessary after theimplantation of
Wallstents or Gianturco-Z-Stents have either not been reported or
haveremained exceptions.2 3 6 7 13
In contrast with the Wallstent, the proximalend of the memory
metal Ultraflex stent isshaped like a tulip enhancing firm
anchoring ofthe stent of the oesophageal wall. This servesto avoid
the formation of pouches that wasseen in nearly every fifth patient
whenWallstent prostheses were implanted.2 7 Therisk of a bolus
obstruction at the upper rim ofthe stent is thus distinctly
reduced.To date, we have seen tumour ingrowth or
overgrowth in about a third of our patients.This is essentially
in agreement with clinicalexperiences in implementing
oesophagealWallstents,2 8 but somewhat in disagreementwith the
findings reported by Knyrim6 who sawthis problem in slightly less
than 24% of hispatients when vascular Wallstents wereapplied.
Nevertheless, it can be assumed thattumour ingrowth/overgrowth
closely correlateswith the patient survival times and that
suchforms of tumour growth generally develop inassociation with all
mesh type endoprostheseslacking a protective coating, especially
inpatients with long survival times. Retreatmentsbased on
thermocoagulation methods there-fore remain unavoidable, as long as
tumouringrowth cannot be prevented. Coated stentscan prevent this
from happening, but bear therisk of stent migration.2 3 8 13
In summary, it can be concluded that treat-ment of malignant
tumour stenoses in theupper gastrointestinal tract by
implementingself expanding wire mesh endoprotheses of thememory
metal Ultraflex stent type is simpleand effective. The implantation
procedureimposes little strain on the patient and can be
312
on March 31, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.37.3.309 on 1 S
eptember 1995. D
ownloaded from
http://gut.bmj.com/
-
Memory metal stents for palliation of malignant obstruction of
the oesophagus and cardia 313
performed on an outpatient basis. Dysphagiawas distinctly
improved in most patients.The rate of serious complications is low.
Theproblem in the early period after implantationis the
insufficient expansion of the stentparticularly in strong tumour
stenoses requir-ing further dilatation treatment. The mainproblem
occurring in the intermediate treat-ment stage is that of tumour
ingrowth andovergrowth.
In view of the degree of discomfort andthe system inherent rate
of complicationsassociated with plastic tube implantations,
thecurrently available generation of memorymetal Ultraflex stents
signifies, even today, avaluable improvement of palliative
treatmentconcepts applied to malignant stenosis in theupper
gastrointestinal tract.We wish to thank Professor M Grade for
translating and revis-ing the manuscript.
Addendum
During the follow up period until February 1995 two morepatients
developed increasing dysphagia due to tumour in-growth and were
retreated with electrocoagulation and KTPlasercoagulation,
respectively. Altogether the problem oftumour infiltration of the
wire mesh occurred in 11 of 30patients (36%) 18 weeks (median;
range: 2-49) after stentplacement.
Furthermore, two more patients died, so that until February1995
four of 30 patients were still alive with a survival time of416
days (median; range: 354-441) and 26 of 30 patients haddied after a
survival time of 108 days (median; range: 3-211).
1 Cwikiel W, Strindberg H, Tranberg K-G, Stael vonHolstein C,
Hambraeus G, Lillo-Gil R, et al. Malignant
esophageal strictures: treatment with a self-expandingmemory
metal stent. Radiology 1993; 187: 661-5.
2 Ell C, Hochberger J, May A, Fleig WE, Hahn EG. Coatedand
uncoated self-expanding metal stents for malignantstenosis in the
upper GI-tract. Am _7 Gastroenterol 1994;89: 1496-500.
3 Ell C, May A, Hahn EG. Gianturco-Z-stents in the pallia-tive
treatment of malignant esophageal obstruction andesophagotracheal
fistulas. Endoscopy (in press).
4 Goldin E, Beyar M, Safra T, Globerman 0, Craciun I,Wengrower
D, et al. A new self-expandable, nickel-titanium coil stent for
esophageal obstruction: a prelimi-nary report. Gastrointest Endosc
1994; 40: 64-8.
5 Grund KE, Storek D, Naruhn M. Flexible metal stentsin the
esophagus [Abstract]. Gastrointest Endosc 1993; 39:121.
6 Knyrim K, Wagner HJ, Bethge N, Keymling M, Vakil N.
Acontrolled trial of expansible metal stent for palliation
ofesophageal obstruction due to inoperable cancer. N Engl _tMed
1993; 18: 1302-7.
7 Kozarek RA, Ball TJ, Patterson DJ. Metallic
self-expandingstent application in the upper gastrointestinal
tract:caveats and concerns. Gastrointest Endosc 1992; 38: 1-6.
8 Neuhaus H, Hoffmann W, Dittler HJ, Niedermeyer HP,Classen M.
Implantation of self-expanding esophagealmetal stents for
palliation of malignant dysphagia.Endoscopy 1992; 24: 405-10.
9 Raijman I, Walden D, Kortan P, Haber GB, Fuchs E,Siemens M, et
al. Expandable esophageal stents: initialexperience with a new
nitinol stent. Gastrointest Endosc1994; 40: 614-21.
10 SaIB NL, Hagenmuller F. Nitinolstent beiOsophaguskarzinom
[Letter]. Dtsch Med Wochenschr1993; 118:45.
11 Schaer J, Katon RM, Ivancev K, Uchida B, Rosch J,Binmoeller
K. Treatment of malignant esophagealobstruction with
silicone-coated metallic self-expandingstents. Gastrointest Endosc
1992; 38: 7-11.
12 Wagner HJ, Knyrim K, Bethge N, Starck, E, Sommer N,Pausch J,
et al. Palliativtherapie der malignenOsophagusobstruktion mit
selbstexpandierendenMetallendoprothesen. Dtsch Med Wochenschr 1992;
117:248-55.
13 Wu WC, Katon RM, Uchida BT, Keller FS, Rosch
J.Silicone-covered self-expanding metallic stents for the
palli-ation ofmalignant esophageal obstruction and
esophagores-piratory fistulas: experience in 32 patients and a
review ofthe literature. Gastrointest Endosc 1994; 40: 22-33.
on March 31, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.37.3.309 on 1 S
eptember 1995. D
ownloaded from
http://gut.bmj.com/