Embed Size (px)
Citation preview

Kidney international, Vol. 51(1997), pp. 277—280
Stenting of central venous stenoses in hemodialysis patients:Long-term results
VOLKER MlcIaEy, JOHANNES GORICH, NORBERT RILINGER, MARTIN STORCK, and DIETMAR ABENDROTH
Department of Thoracic and Vascular Surgery, Department of Diagnostic Radiolo, University of U/rn, U/rn, Germany
Stenting of central venous stenoses in hemodialysis patients: Long-term results. From November 1992 through July 1996, 15 Wallstentswere implanted for the treatment of symptomatic central arm veinobstructions in 14 hemodialysis patients (10 subclavian, 2 brachiocephalicvein stenoses, 2 subclavian vein occlusions). There were no acute compli-cations. Al! patients were investigated by clinical examination and color-duplex sonography at regular three month intervals. When recurrentswelling predicted restenosis, phlebography was also performed. Duringthe follow-up, high grade stenoses at the central or peripheral ends of fourstents were successfully treated with five overlapping stents, giving a totalof 20 Wallstent' implantations. Complete occlusion of another subclavianvein distally to the stent at 16 months required ligation of the patient'sarteriovenous fistula. Life table analysis including all 20 stents revealed acumulative primary one year (two year) stent patency of 70% (50%). Thecumulative secondary one year (two year) stent patency was 100% (85%).We believe that in hemodialysis patients, PTA plus Walistent" implanta-tion is a safe and effective procedure in the treatment of central venousstenoses and even short occlusions. Consequent follow-up allows fortimely diagnosis and treatment of restenoses, thus guaranteeing long-termpatency rates comparable to those of veno-venous bypass surgery.
Stenoses and occlusions of central arm veins frequently occurafter repeated or prolonged catheterization for hemodialysisaccess [1, 2], especially, if the subclavian vein was used for access[3], and following catheter-associated infection [4]. If the drainingvein of a functioning shunt is obstructed, extreme venous hyper-tension with pain, incapacitating swelling, and ulceration mayoccur [5, 6]. Surgical treatment (patch angioplasty or bypassprocedures) may be hazardous in these often multimorbid pa-tients [7, 8]. Percutaneous dilation (PTA) is less invasive, however,the long-term results are disappointing [9—12]. We thereforecombined PTA with implantation of flexible, self-expanding stents(PTA+S).
Methods
From November 1992 through July 1996, 15 Wallstents"' wereimplanted for treatment of symptomatic central arm vein obstruc-tions in 14 hemodialysis patients (10 suhclavian, 2 brachiocephalievein stenoses, 2 subclavian vein occlusions). All patients had ahistory of repeated or prolonged subclavian vein catheterizationfor hemodialysis access. All obstructions were central to a func-
Received for publication April 30, 1996and in revised form August 16, 1996Accepted for publication August 18, 1996
© 1997 by the International Society of Nephrology
277
tioning access fistula which had been created two months to sevenyears prior to onset of symptoms. Eleven patients presented withmassive arm swelling, two suffered from additional unilateral faceswelling, and the last had arm swelling and localized graftinfection. All patients had chronic obstructions. Symptoms hadlasted for two months to two years before treatment. In onepatient, an unsuccessful PTA at another institution had precededstenting by four weeks.
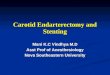
Venous pathology was visualized by transhrachial fine needle-arteriovenography in DSA technique (Fig. 1A) immediately be-fore intervention. Then all patients received 5000 IU heparin i.v.All stents were placed via a transfemoral route to avoid unneces-sary trauma to peripheral arm veins. Guide wire passing of tight,kinking stenoses, however, sometimes had to be facilitated byrendezvous maneuvers with additional upper arm access. Twoshort occlusions were reopened with rotating devices (Rotacs'catheter, Fig. 1B) [13]. Only extremely tight stenoses were pre-dilated to allow for passage of the stent equipment. After place-ment all stents had to be dilated with high-pressure balloons toachieve complete opening within the fibrotic venous strictures(Fig. 1C). Over-dilation of adjacent vein segments was strictlyavoided. After stenting a PYT of 60 seconds to 90 seconds wasmaintained for three days by a continuous heparin infusion.Patients were advised to take 100 mg acetylsalicylic acid a daythroughout the study period.
All patients were investigated by clinical examination andcolor-duplex sonography at regular three month intervals. Whenrecurrent swelling predicted symptomatic restenosis, phlebogra-phy was also done. Whenever indicated interventional redoprocedures were performed giving a total of 20 Wallstent''implantations. Cumulative primary and secondary patency ratesincluding all 20 stents were estimated by life table analysis [14]according to the recommendations of the International ConsensusCommittee on Chronic Venous Disease [15].
Results
Stent placement with complete opening was achieved in allcases. Besides local pain during dilation and minor hematomas atpuncture sites, there were no procedure-related complications,not even during the Rotacs"' maneuvers. All patients werecompletely free of symptoms within 24 to 48 hours after treat-ment. Arteriovenous (av) fistulae and grafts were used for hemo-dialysis after the procedure when indicated. There were no signsor symptoms of shunt dysfunction or recirculation. The localized

•1; •
recurred in five patients (with 6 stents) after 3, 6, 7, 10, and 16months, respectively.
Complete visualization by color-duplex sonography was possi-ble in only 10 of 20 stents. In these patients, repeat investigationsduring the study period revealed only a smooth neo-intima withno areas of stenosis within the stents. In three patients out of fivewith recurrent swelling, however, venous obstructions (2 highgrade stenoses, I complete occlusion) were detected in peripheralvein segments adjacent to the widely patent stents. Phlebographywas done in all five patients with recurring complaints. Ultrasoundfindings were confirmed in the three cases with complete sono-graphic visualization of the stents. In two additional patients theirvery central stents could not completely be examined by sonogra-phy for anatomical reasons. These stents were also widely patent.Stenoses were located in vein segments close to the central endsof the stents.
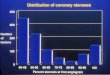
High grade stenoses at the central or peripheral ends of fourstents were successfully treated with five overlapping stents.Complete occlusion of a subclavian vein distally to the stent at 16months required ligation of the patient's av-fistula after unsuc-cessful interventional treatment. Life table analysis of all 20Wallstents implanted so far (Fig. 2) gave a cumulative primaryone year (two year) stcnt patency of 70% (50%). Cumulativesecondary one year (two year) patency was 100% (85%).
Comment
C
Fig. 1. A. Complete occlusion of left subclavian vein 18 months aftercreation of proximal cimino-fistula. Extensive collaterals around left shoul-der and left upper thoracic aperture owing to functioning av-fistula.Guidewire already passed the occlussion. B. Transbracial RotacsTM ma-neuver necessary to allow for introduction of balloon catheter. C. Collat-erals vanish immediatley after successful PTA and WallstentTM implanta-tion.
graft infection healed after excision of the infected prostheticsegment.
Four patients died (3 from complications of their coronaryartery disease, 1 from unexplained scpticemia) after 7, 8, 15 and24 months, respectively, with patent stents. All other patientscould be followed up during the whole study period (from 1month to 3 years, median 9 months). Arm or face swelling
Typical clinical findings in subclavian vein obstruction are armswelling and development of widespread subcutaneous venouscollaterals around the shoulder and the upper thoracic aperture.Especially when the draining vein of a functioning av-fistula isstenosed, massive venous hypertension with pain and peripheralulceration may develop [1, 2, 5]. Strictures of the central subcla-vian or inriominate vein may cause additional unilateral swellingof breast, face, and neck [16].
Before treatment exact delineation of venous pathology isindispensable. For this indication, color-duplex ultrasound is oflimited value, because neither the innominate vein nor theproximal third of the subclavian vein can be visualized with thistechnique [17]. Phlebography is still felt to be the gold standardfor diagnosis of upper extremity venous stenoses and occlusions[15]. In our study, sonographic pre-treatment localization ofcentral venous strictures was not attempted. Color-coded ultra-sound was used for follow-up examinations of stented veinsegments. Only half of the stents could be completely visualized,and only three out of five restenoses were seen. In these few cases,sonographic findings were completely confirmed by arteriovenog-raphy. The other stents and restenoses were at least in partlocated deep in the mediastinal part of the subclavian andinnominate veins beyond ultrasound accessibility. In these pa-tients clinical diagnosis of restenosis was based solely on recurrentarm (and face) swelling, and was also confirmed by arteriovenog-raphy. Transbrachial fine needle-arteriovenography in DSA tech-nique always allowed an exact delineation of the site and exten-sion of all obstructions as well as of important collaterals.Therefore, interventional therapy could immediately follow aradiological diagnosis.
There are several options for the treatment of venous hyper-tension due to outflow obstruction of functioning hemodialysisaccess. Fistula ligation [5, 6] is the least invasive as well as themost frustrating operation, as the vascular pathology causing the
278 Mickley et al: Stenting and stenoses in hemodialysis
A
B

Mickley et al: Stenting and stenoses in hemodialysis 279
I I IFig. 2. Cumulative primaly (LI) and sccondaiy
___________________________________________________________________________________ • patency of central venous stents in
0 3 6 9 12 15 18 21 24 hemodialysis patients. Symbol I representsstandard deviations.
Table 1. Primary one and two year patency rates of PTA, PTA +Wallstent rS, implantation, and surgery for central venous stenoses in
hemodialysis patients
Author Patient 12 24
________ [Referencel # Months Months
PTA Glanz, 1987 [9] 30 35% 10%Wisselink, 1993 [12] 15 36% 0%Quinn, 1995 [281 10 12%Money, 1995 [281 26 7%
PTA + Wallstent" Shoenfeld, 1994 [30] 19 68%Money, 1995 [281 13 71%Vorwerk, 1995 [29] 27 60% 60%Mickley, 1996 14 70% 50%
Surgery Wisselink, 1993 [12] 13 86% 66%
______ Money, 1995 [28] 13 80%
Some of the stenoses in this study were treated with Palmaz stents
patients problem is not corrected. The respective extremity is thusrendered unsuitable for further shunt operations. Patch angio-plasty of a subclavian or innominate vein as well as orthotopicbypass surgery [7, 8] makes clavicular or sternal osteotomy (andgeneral anesthesia) necessary and is therefore burdened withsignificant morbidity and even mortality in these chronically illand often rnultimorbid patients. Extra-anatomical bypass (such assubclavian-to-jugular [18, 19]) is less distressing to the patient;however, another central vein is lost for further access. Inconsequence, non-operative, interveritional procedures that areappropriate to obtain and maintain central venous patency inhemodialysis patients have been investigated.
Most of the patients present with long lasting symptoms sub-stantiating the chronic nature of their stenoses and occlusions.Therefore, thrombectomy, thrombaspiration, or thrombolysisalone are not likely to sufficiently restore venous patency. Inselected cases with evidence of fresh thrombi causing totalobstruction of a former fihiforme venous stricture, however,thrombolysis may help to re-establish the stenosed lumen to allowfor additional PTA [201. PTA of central venous stenoses inhemodialysis patients has been reported since the early 1980s [9,11, 21—23]. Because of frequent restenoses arid occlusions, how-ever, one year primary patency of PTA alone is less than 40%(Table 1). To reduce the number of reintervcntions, stent implan-tation was added to PTA by different investigators [24—271.L.ong-term results after implantation of Gianturco stents intocentral veins of hemodialysis patients are not better than PTA[10]. The self-expandable Wallsten(' [28, 29] and the balloon-
expandable Palmaz stent [30], however, have recently been re-ported to allow for primary one year (two year) patency rates of60% to 71% (60%) thus almost resembling the results aftersurgical correction [12, 28] of central venous stenoses (Table 1).
After demonstrating the favorable results of PTA+S whencompared to PTA alone for postoperative central venous stric-tures [24], we started this prospective study in hemodialysispatients. Ten subclavian and two innominate vein stenoses andtwo subclavian vein occlusions were treated by immediate Wall-stent implantation. Only in one patient, stenting was performedfour weeks after unsuccessful PTA at another institution. Duringthe study period, another four patients with central venousocclusions were operated on. Three of them presented with longsubclavian vein occlusions that could not be recanalized percuta-neously. In these cases an extra-anatomical axillary-to-internaljugular vein bypass graft was implanted. In the fourth patient,bilateral subclavian vein and superior vena caval occlusion re-quired construction of a subclavian artery-to-right atrial accessgraft [31].
Our results confirm the earlier communications quoted above.The Wallstent has some mechanical advantages over alternativestent models that should be mentioned. It is flexible even whenconstrained on the delivery catheter, so that it can safely be usedin a tortuous stenosis once a guide wire has been properlypositioned. During placement the stent will attach closely to thevessel wall by its own elasticity thus preventing later dislocation.The large but unpredictable extent of stent shortening duringdelivery, however, may cause some difficulty with respect to theexact positioning of the proximal end of the Wallstent'. Innom-mate vein stenoses close to the confluence therefore should bestented via an upper extremity venous approach. If cannulation ofan arm vein has to be avoided in order not to further compromisethe outflow tract of a functioning hemodialysis access, transfemo-ral implantation of a Palmaz stent should he considered [30].
During stent implantation patients were anticoagulated withheparin. From the first post-interventional day on, they wereadvised to take 100 mg acetylsalicylic acid a day. The samemedication has been recommended by others [29]. However,there are no reliable data on the possible value of acetylsalicylicacid or of vitamin K-antagonists to maintain long-term patency ofcentral venous stents, as comparative studies are lacking.
In hemodialysis patients, PTA plus Wallstenr implantation isa safe and effective procedure in the treatment of central venousstenoses and even short occlusions. Consequent follow-up allows
N=20100%
N=9 N=5
80%
60%
40%
20%
0%

280 Mickley et at: Stenting and stenoses in hemodiaiysis
for timely diagnosis and treatment of restenoses thus guarantee-ing long-term patency rates comparable to those of surgery.Veno-venous bypass implantation should therefore be restrictedto long venous occlusions.
Reprint requests to Volker Mickley, M.D., Department of Thoracic andVascular Surgety, University of Ulm, Steinhoeveistr. 9, D-89075 Vim, Ger-many.
References
1. BARRETt N, SPENCER S, MCIv0R J, BROWN EA: Suhclavian stenosis:a major complication of subelavian dialysis catheters. Nephroi DialTransplant 3:423—425, 1988
2. SPINOWITZ BS, GALLER M, GOLDEN RA, PASCOFF JH, SCHECIITER L,HELD B, CHARYTON C: Subelavian vein stenosis as a complication ofsubclavian catheterization for hemodialysis. Arch mt Med 157:305—307, 1987
3. BAMBAUER R, INNIGER R, PIRRUNG KJ, SCHIEL R, DAHI,EM R:Complications and side effects associated with large-bore catheters inthe subclavian and internal jugular veins. Artif Org 18:318—321, 1994
4. HERNANDEZ D, DIAZ F, SURIA 5, MACHADO M, LORENZO V, LOSADAM, GONZALEZ-POSADA JM, DE BONI5 E, DOMINGUEZ ML,RODRIGUEZ AP, TORRI::S A: Subclavian catheter-related infection is amajor risk factor for the late development of subclavian vein stenosis.Nephrol Dial Transplant 8:227—230, 1993
5. MCNALLY PG, BROWN CB, MOORHFAD PJ, RAFTERY AT: Unmaskingof subclavian vein obstruction following creation of arteriovenousfistulae for haemodialysis. A problem following subclavian line dialy-sis? Nephrol Dial Transplant 1:258—260, 1987
6. STONE Wi, WALL MN, POWERS, TA: Massive upper extremity edemawith arteriovenous fistula for hemodialysis. Nephron 31:184—186, 1982
7. DUNCAN JM, BALDWIN RT, CARAI.IS JP, COOLEY DA: Suhelavian veinto right atrial bypass for symptomatic venous hypertension. AnnThorac Surg 52:1342—1343, 1991
8. MOoRE WM, HOLLIER LH, PICKET1 TK: Superior vena cava andcentral venous reconstruction. Surgery 110:35—41, 1991
9. GLANZ S, GORDON DH, BUTt KMH, HONG J, LIPKOWITZ GS: Therole of percutaneous angioplasty in the management of chronichcmodialysis fistulas. Ann Surg 206:777—781, 1987
10. QUINN SF, SCHUMAN ES, DEMLOW TA, STANDAGE BA, RAG5DALEJW, GREEN GS, SHELEY RC: Percutaneous transluminal angioplastyversus endovascular stent placement in the treatment of venousstenoses in patients undergoing hemodialysis: Intermediate results. JVase Intervent Radioi 6:851—855, 1995
11. SCHWAB SJ, QUARLES D, MIDDLETON JP, COnAN RH, SAEED M,DENNIS VW: Hemodialysis-associated subelavian vein stenosis. Kidneymt 33:1156—1159, 1988
12. WISSELINK W, MONEY SR, BECKER MO, RICE KL, RAMEE SR, WHITECJ, KAZMIER FJ, HOLLIER LH: Comparison of operative reconstruc-tion and percutaneous balloon dilatation for central venous obstruc-tion. Am J Surg 166:200—205, 1993
13. SCHOLZ A, SCHUBEUS P, LANGER R, LANGER M, FELIX R: Primaerefemorale Rekanalisation mit einem langsam rotierenden Kathetersys-tent Akt Radio! 3:295—297, 1993
14. RUTHERFORD RB, FLANIGAN DP, GUI'rA SK, JoIINRIIN KW, KAIS-MODY A, WHITTEMORE AD, BAKER iD ERNST CB, JAMIUSON C,MImIA S: Suggested standard for reports dealing with lower extremityischemia. J Vasc Surg 4:80—94, 1986
15. PORTER JM, MONETA GL: Reporting standards in venous disease: Anupdate. J Vase Surg 21:635—645, 1995
16. GADALLAI-J MF, EL-SHAHAWY MA, CAMPESE VM: Unilateral breastenlargement secondary to hemodialysis arteriovenous fistula andsubelavian vein occlusion. Nephron 63:351—353, 1993
17. HAIKU WD, LYNCH TG, LIEBERMAN RP, LUND GB, EDNEY JA: Utilityof duplex ultrasound in the diagnosis of asymptomatic catheter-induced subelavian vein thrombosis. J Ultrasound Med 10:493—496,1991
18. CURRIER CB, WIDDER 5, AI,I A, KuusIsTo E, SIDAWY A: Surgicalmanagement of suhclavian and axillary vein thrombosis in patientswith a functioning arteriovenous fistula. Surgery 100:25—28, 1986
19. HANSEN B, FEINS RS, DETMER DE: Simple extra-anatomic jugularvein bypass for subclavian vein thrombosis. J Vase Surg 2:921—923,1985
20. NEWMAN GE, SAEED M, HIMMELSTEIN 5, COHAN RH, SCHWAB SJ:Total central vein obstruction: Resolution with angioplasty and fibri-nolysis. Kidney mt 39:761—764, 1991
21. GLANZ S, GORDON D, BUTr KMH, HONG J, ADAMSON R, SCI,AFANISJA: Dialysis access fistulas: Treatment of stenoses by transluminalangioplasty. Radiology 152:637—642, 1984
22. INGRAM TL, REID SH, TISNADO J, CHO SR, POSNER MP: Percutane-ous transluminal angioplasty of brachiocephalic vein stenoses inpatients with dialysis shunts. Radiology 166:45—47, 1988
23. STALTER KA, STEVENS GF, STERLING WA: Late stenosis of thesubelavian vein after hemodialysis catheter injury. Surgery 100:924—927, 1986
24. MICKI.EY V, FRIEDRICH JM, RILINGER N, STORCK M, ABENDROTH D:PTA plus stent implantation versus PTA alone for central venousstenoses. Vase Surg 28:505—511, 1994
25. EL5ON JD, BECKER GJ, WHOLEY MH, EURMAN KO: Vena caval andcentral venous stenoses: Management with Palmaz balloon-expand-able intraluminal stents. J Vase Intereent Radio! 2:215—223, 1991
26. ROUSSEAU H, MORFAUX V, JOFFRE F, THAT HT, GOUDABLE C,BARTOLI P, YONG MY: Treatment of hemodialysis arterio-venousfistula stenosis by percutaneous implantation of new intravascularstent. J intervent Radio! 4:161—167, 1989
27. VORWERK D, GUENTHER RW, BOHNDORF K, KISrI.ER D, HANDT 5,MANN H, SIEHERTH HG: Perkutane vaskulaere Endoprothesen beiVerschluessen oder Stenosen von Haemodialysc-Shunts. Dtsch MedWschr 115:43—47, 1990
28. MONEY 5, BHATIA D, DAHARAMSY 5, MULINGTAPANG R, SHAW D,RAIIEE 5: Comparison of surgical by-pass, percutaneous balloondilatation (PTA), and PTA with stent placement in the treatment ofcentral venous occlusion in the dialysis patient. One year follow-up.(abstract) IntAngiol 14:176, 1995
29. VORWERK D, GUENTHER RW, MANN H, BOHNDORF K, KEULERS P,AI.ZEN G, SOHN M, KI5TLER D: Venous stenoses and occlusion inhemodialysis shunts: Follow-up results of stent placement in 65patients. Radiology 195:140—146, 1995
30. SIIOENFELD R, HERMANS H, NOvICK A, BRENER B, CORDERO P,EIsLNHUD D, MODY 5, GOLDENKRANZ R, PARSONNET V: Stenting ofproximal venous obstructions to maintain hemodialysis access. J VaseSurg 19:532—539, 1994
31. MICKIFY V: Suhclavian artery4o-right atrial haemodialysis bridgegraft for superior vena eaval occlusion. Nephrol Dial Transplant10:1361—1362, 1996