Embed Size (px)
Citation preview

STEMI Network
EditorialBy Joseph Fredi, M.D., F.A.C.C. and Carol Scott, R.N., F.N.P., E.M.T.
Joseph L. Fredi, M.D., F.A.C.C.
Since the implementation of our program in 2007, the Vanderbilt STEMI Network continues to see steady improvement in reperfusion times for patients suffering an acute ST elevation myocardial infarction. We are pleased to report our door-to-balloon (D2B) results for patients presenting to the Vanderbilt Emergency Department and the Door 1-to Door 2-to balloon (DD2B) results for patients who were transferred from outlying facilities.
The median D2B time for patients presenting to the Vanderbilt ED for 2011 was 63 minutes.
The median DD2B time for patients transferred from an outlying facility within a 60-mile radius (zone 1) of Vanderbilt who participates in the Vanderbilt STEMI Network is 97 minutes. This is an improvement compared to 119 minutes in 2010 and 120 minutes in 2009.
The median DD2B time for patients transferred from an outlying facility within a 120-mile radius (zone 2) of Vanderbilt who participates in the Vanderbilt STEMI Network is 131 minutes. This remains stable when compared to 126.5 minutes in 2010 and 164 minutes in 2009.
Much of the credit for this success goes to the nurses and physicians of our partnering referring Emergency Departments and the crew of ground and air transport services. It is due to your dedication and commitment in providing the highest quality of care to your patients who suffer acute heart attacks that we have seen the tremendous improvement in DD2B times over the past five years.
We also feel that part of the success is due to the communication and feedback that Vanderbilt provides after every case, which includes a phone call from the interventional cardiologist to the referring physician notifying him of the cardiac catheterization results, and a detailed spread sheet that includes the time intervals, goals and cumulative times the following day. This information is sent to everyone involved in the care of the patient: EMS, referring hospital physician and nurses, air or ground transport service and personnel at Vanderbilt.
Each of our referring hospitals that participate in the Vanderbilt STEMI Network received an annual report card in February detailing its individual DD2B times for 2011 and a comparison of their DD2B times since 2008.
Since the STEMI Network has been so successful, we have implemented a Level 1 Cardiac Emergency System based on the same principles to include hypothermia after cardiac arrest, acute aortic dissections, pulmonary embolism and cardiogenic shock. Vanderbilt is one of only four medical centers in the United States that offers this type of program.
Vanderbilt Heart and Vascular Institute Publication
Spring 2012 | Volume 4 | Issue 5 | VanderbiltSTEMI.com
This bar graph reflects the median DD2B times for 2011 for both zone 1 and zone 2 referring facilities that participate in the Vanderbilt STEMI Network.
Median DD2B 2011200
180
160
140
120
100
80
60
40
20
10
0
A B C D G H I J K L O P R
Referring Facility
Hospitals A, B, C, D, G, J, K, L, O and P are in zone 1.Hospitals H, I, and R are in zone 2.
122
113 108
185
95
158
129
87
129
159
110
96
158
Min
utes
Carol Scott, R.N., F.N.P., E.M.T.

Case:An 80-year-old female with no significant past medical history presented to the local emergency room after being involved in a car accident. On arrival she reported right shoulder pain and mild substernal chest pain. A physical exam quickly identified a right clavicular fracture. She appeared very anxious and continuously inquired about the health of the other passengers in the car. Given substernal chest pain, a cardiac workup was completed. A chest X-ray was unremarkable except for a right non-displaced clavicular fracture. EKG showed anterior ST elevations; therefore, the diagnosis of an anterior STEMI was given. The nearest STEMI receiving center (SRC) for completion of primary percutaneous coronary intervention (PCI) was 45 miles away, so she was transported via a medical helicopter to the nearest STEMI receiving center. Acute treatments included dual anti-platelet therapy and a heparin bolus. She remained hemodynamically stable. Emergent coronary angiography was completed, which revealed no significant coronary artery stenosis. Left ventriculography showed severely depressed LV function, although the basal segments of the myocardium had normal contractility. The transferring hospital called to report an elevated troponin at 0.80mg/dl. The patient was diagnosed with Takotsubo cardiomyopathy.
Discussion:Takotsubo cardiomyopathy was first described in the early 1990s in Japan. The name comes from fishing pots used in Japan to catch octopuses. The affected myocardium’s shape resembles these fishing pots. Other names for this condition include stress-induced cardiomyopathy, apical ballooning syndrome and broken heart syndrome. Patients present with transient left ventricular apical ballooning (occurs during systole where the mid and apical areas of the LV have depressed contractility while the basal area compensates with hyperkinetic contractility producing a balloon-like appearance of the distal LV), no significant coronary artery stenosis and no prior history of cardiomyopathy. The majority of patients have an acute medical condition (i.e. CVA, asthma attack, seizures) or acute emotional stress (i.e. accident, family member death). Post-menopausal women are more commonly affected. Acute presentations of Takotsubo cardiomyopathy can mimic signs and symptoms of an acute myocardial infarction. Common presenting symptoms include chest pain, dyspnea and electrocardiographic abnormalities. Other complications include tachyarrhythmias, pulmonary edema, left ventricular outflow tract obstruction from basal myocardium hyperkinesis, mitral regurgitation and apical thrombus formation. EKG abnormalities include ST elevation (most commonly in the anterior leads), deep T wave inversion and development of Q waves. Lab studies specific for myocardial injury are commonly elevated, but are usually only mildly elevated. Echocardiogram or left ventriculogram during angiography demonstrates apical ballooning with dyskinesis in up to one-half of the LV– usually with sparing of the basal segments. Average LV ejection fractions are 30% to 50%. Echocardiogram can also document LVOT obstruction from basal segment hyperkinesis therefore having similar physiology and imaging findings of hypertrophic cardiomyopathy.
Management of these patients is usually conservative with typical CHF medications. These include beta blockers, ACE inhibitors, angiotensin receptor blockers and aldosterone antagonists. There are no specific therapies for Takotsubo cardiomyopathy. It is important to rule out other etiologies of chest pain and other acute symptoms. If ST elevations are present, emergent left heart catheterization is indicated. Takotsubo cardiomyopathy is usually a diagnosis of exclusion once coronary artery stenosis is ruled out as contributing to regional wall motion abnormalities. Prognosis of Takotsubo cardiomyopathy is excellent with the majority of patients regaining LV function in one to four weeks. Some case series report up to a 10% recurrence rate. In-hospital mortality rates range from zero to 8%. Mortality rates are confounded by other acute medical conditions and co-morbidities.
Our case demonstrates the appropriate transfer of this patient to a STEMI receiving center (SRC) based on her ST elevations and concurrent chest pain.
Takotsubo cardiomyopathy a diagnosis of exclusion By Eric Thomassee, M.D.
Eric Thomassee, M.D.
Takotsubo cardiomyopathy was first described in the early 1990s in Japan. The name comes from fishing pots used in Japan to catch octopuses. The affected myocardium’s shape resembles these fishing pots.
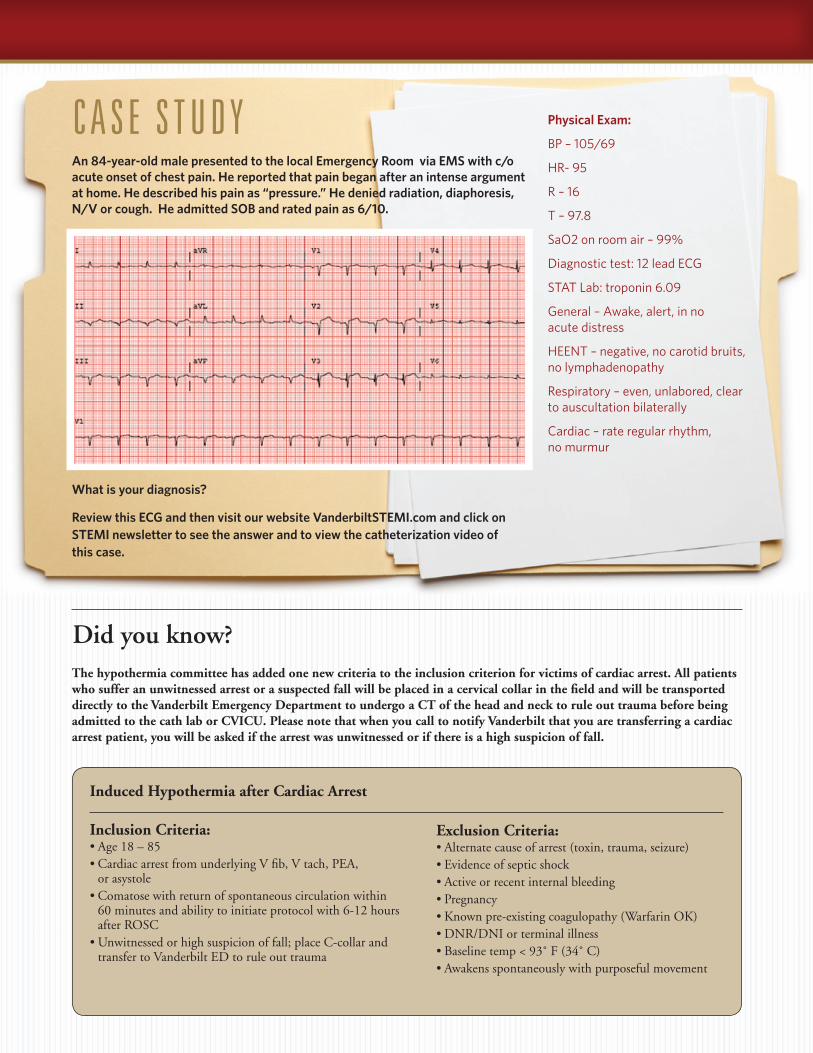
C A S E S T U D Y
The hypothermia committee has added one new criteria to the inclusion criterion for victims of cardiac arrest. All patients who suffer an unwitnessed arrest or a suspected fall will be placed in a cervical collar in the field and will be transported directly to the Vanderbilt Emergency Department to undergo a CT of the head and neck to rule out trauma before being admitted to the cath lab or CVICU. Please note that when you call to notify Vanderbilt that you are transferring a cardiac arrest patient, you will be asked if the arrest was unwitnessed or if there is a high suspicion of fall.
Induced Hypothermia after Cardiac Arrest
Inclusion Criteria: •Age18–85•CardiacarrestfromunderlyingVfib,Vtach,PEA, or asystole•Comatosewithreturnofspontaneouscirculationwithin 60 minutes and ability to initiate protocol with 6-12 hours after ROSC•Unwitnessedorhighsuspicionoffall;placeC-collarand transfer to Vanderbilt ED to rule out trauma
Exclusion Criteria:•Alternatecauseofarrest(toxin,trauma,seizure)•Evidenceofsepticshock•Activeorrecentinternalbleeding•Pregnancy•Knownpre-existingcoagulopathy(WarfarinOK)•DNR/DNIorterminalillness•Baselinetemp<93˚F(34˚C)•Awakensspontaneouslywithpurposefulmovement
Did you know?
An 84-year-old male presented to the local Emergency Room via EMS with c/o acute onset of chest pain. He reported that pain began after an intense argument at home. He described his pain as “pressure.” He denied radiation, diaphoresis, N/V or cough. He admitted SOB and rated pain as 6/10.
Physical Exam:
BP – 105/69
HR- 95
R – 16
T – 97.8
SaO2 on room air – 99%
Diagnostic test: 12 lead ECG
STAT Lab: troponin 6.09
General – Awake, alert, in no acute distress
HEENT – negative, no carotid bruits, no lymphadenopathy
Respiratory – even, unlabored, clear to auscultation bilaterally
Cardiac – rate regular rhythm, no murmur
What is your diagnosis?
Review this ECG and then visit our website VanderbiltSTEMI.com and click on STEMI newsletter to see the answer and to view the catheterization video of this case.
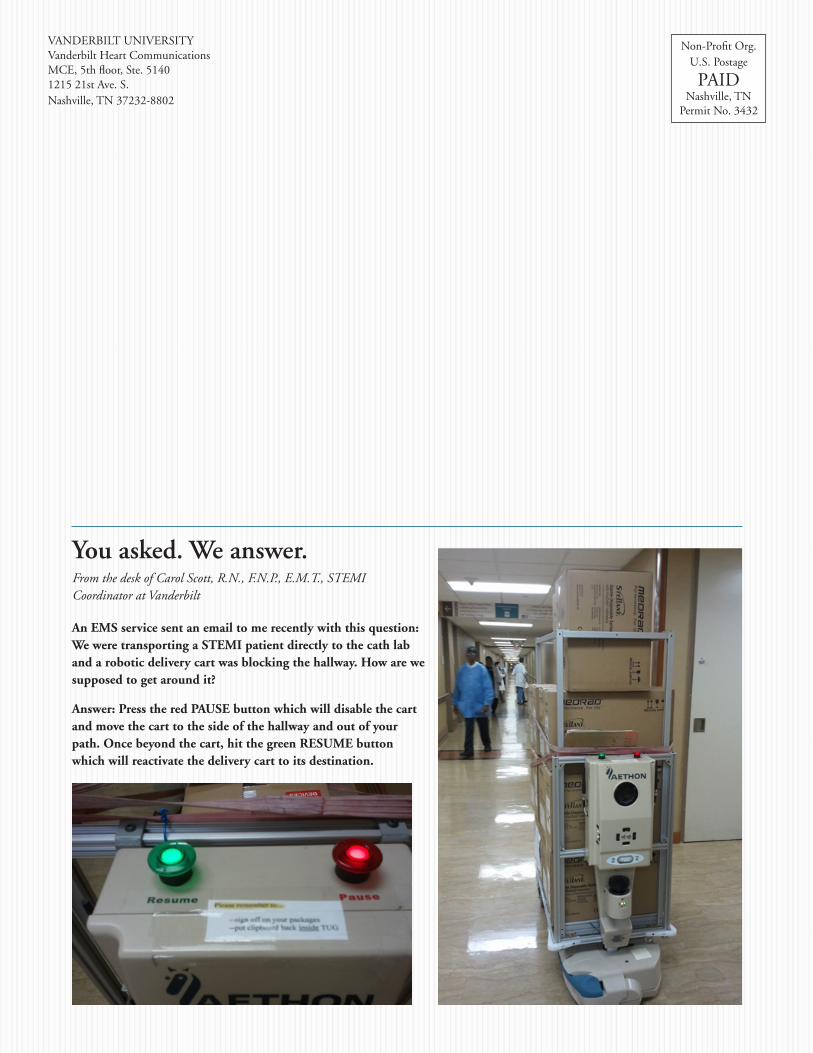
An EMS service sent an email to me recently with this question: We were transporting a STEMI patient directly to the cath lab and a robotic delivery cart was blocking the hallway. How are we supposed to get around it?
Answer: Press the red PAUSE button which will disable the cart and move the cart to the side of the hallway and out of your path. Once beyond the cart, hit the green RESUME button which will reactivate the delivery cart to its destination.
VANDERBILT UNIVERSITYVanderbilt Heart CommunicationsMCE, 5th floor, Ste. 51401215 21st Ave. S.Nashville, TN 37232-8802
Non-Profit Org.U.S. Postage
PAIDNashville, TN
Permit No. 3432
You asked. We answer.From the desk of Carol Scott, R.N., F.N.P., E.M.T., STEMI Coordinator at Vanderbilt