Embed Size (px)
Citation preview

STEMI, Bleeding & Outcomes in Seniors: What Are the Issues?
Ron Waksman, MDJoshua P, Loh, MD
July 29, 2013
Trans –Radial Education and Therapeutics (TREAT IV

Overview
• Challenges of treating STEMI in elderly• PPCI in the elderly• Increased bleeding risk in STEMI• Increased bleeding risk in the elderly• Bleeding avoidance strategies

STEMI in the elderly: Challenges• Eligibility for reperfusion decreases in the elderly
(contraindications, cognition, comorbidities). Elderly STEMI patients less likely to receive reperfusion (PCI or fibrinolysis) even if eligible.
• Many elderly present with atypical symptoms, abnormal baseline ECGs, or comorbidities that contribute to clinical uncertainty, delayed diagnosis and delayed treatment.
• PCI success rates lower, with higher complication rates in the elderly.
• Higher mortality after STEMI.• Limited data from clinical trials
Alexander et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2570-89.
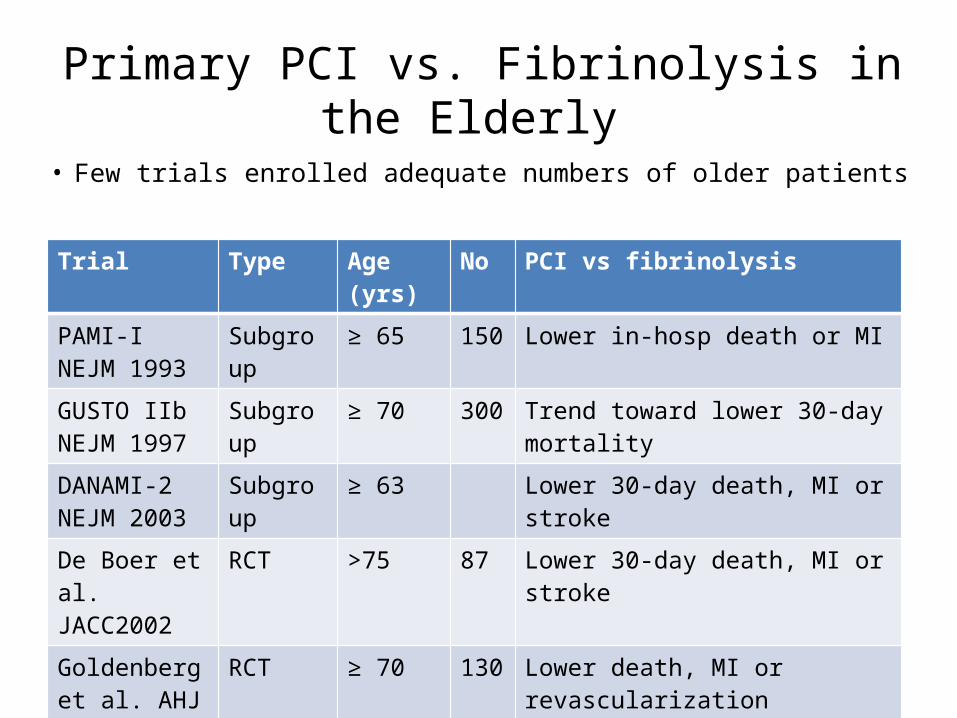
Primary PCI vs. Fibrinolysis in the Elderly
• Few trials enrolled adequate numbers of older patients
Trial Type Age (yrs) No PCI vs fibrinolysis
PAMI-INEJM 1993
Subgroup ≥ 65 150 Lower in-hosp death or MI
GUSTO IIbNEJM 1997
Subgroup ≥ 70 300 Trend toward lower 30-day mortality
DANAMI-2NEJM 2003
Subgroup ≥ 63 Lower 30-day death, MI or stroke
De Boer et al.JACC2002
RCT >75 87 Lower 30-day death, MI or stroke
Goldenberg et al. AHJ 2003
RCT ≥ 70 130 Lower death, MI or revascularization
Senior PAMITCT 2005
RCT ≥ 70 481 Lower death, stroke or reinfarction

Primary PCI vs. Fibrinolysis in the Elderly:Absolute mortality advantage of PCI increases
with age
Boersma E; Primary Coronary Angioplasty vs. Thrombolysis Group. Eur Heart J. 2006;27:779-788.

Challenges of Primary PCI in the Elderly:High-risk subset
ELDERLY ≥ 75 yrs
More comorbiditiesHTN, COPD, stroke, CHF, CKD, prior revasc, higher KILLIP class on presentation
Lower procedural success
More peri-procedural complicationsLess ST resolutionMechanicalElectricalBleeding (3% in <65 yrs, 9% in >75 yrs)

Challenges of Primary PCI in the Elderly:outcomes according to age
On multivariable adjustment, age was the strongest independent predictor of 90-day mortality (HR 2.07 per 10-year increase; 95% CI 1.84-2.33).
APEX-AMI
CADILLAC
Guagliumi G, et al. Outcome in elderly patients undergoing primary coronary intervention for acute myocardial infarction: CADILLAC. Circulation 2004;110:1598-604.

Primary PCI in the very elderlySalinas et al. (n=38)Eurointerv 2011
Koutouzis et al. (n=22)Clin cardiol 2010
Antoniucci et al. (n=55) AHJ 1999
Valente et al. (n=88)Circ J 2008
Median age/yrs 91.5 92 84 88
Procedural mortality
9%
In-hospital mortality
34.2% 27% 17%
30 day mortality 32% 16%
Factors associated with mortality
Killip class >I vs. I53.3% vs. 21.7%
TIMI flow <3 vs. 371.4% vs. 22.7%
Major bleeding vs. none100% vs. 31.4%
Killip class III/IV vs. I/II100% vs. 21%
Cardiogenic shock vs. none70% vs. 4%
Cardiogenic shock vs. none90% vs. 7%
Killip class III/IV vs. I/II40% vs. 12.3%
Major bleeding 5.4% 0 NA 11%

Bleeding after PCI
Elderly
STEMIComorbidities
e.g. renal failure
IncreasedRisk

Post PCI bleeding increases mortality: NCDR
Chhatriwalla et al; NCDR. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention. JAMA 2013;309:1022-9.
CathPCI registry: analyzed 3 million PCIs in the US between 2004 and 2011Bleeding events occurred in 1.7%In-hospital deaths occurred in 0.65%

Bleeding after Primary PCI: Sustained effect of bleeding on mortality and MACE up to 3 years
Suh JW, et al. Impact of in-hospital major bleeding on late clinical outcomes after primary percutaneous coronary intervention in acute myocardial infarction the HORIZONS-AMI trial. J Am Coll Cardiol. 2011;58:1750-6.
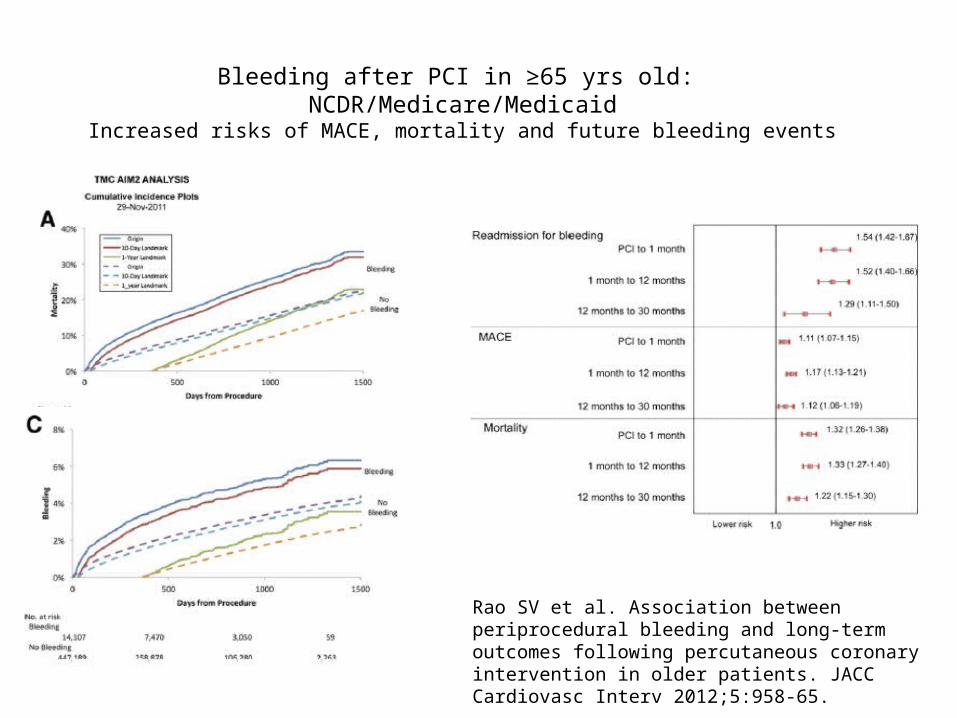
Bleeding after PCI in ≥65 yrs old: NCDR/Medicare/Medicaid
Increased risks of MACE, mortality and future bleeding events
Rao SV et al. Association between periprocedural bleeding and long-term outcomes following percutaneous coronary intervention in older patients. JACC Cardiovasc Interv 2012;5:958-65.

Bleeding increases mortality: proposed mechanisms
Doyle BJ, et al. Bleeding, blood transfusion, and increased mortality after percutaneous coronary intervention: implications for contemporary practice. J Am Coll Cardiol 2009;53:2019-2027.
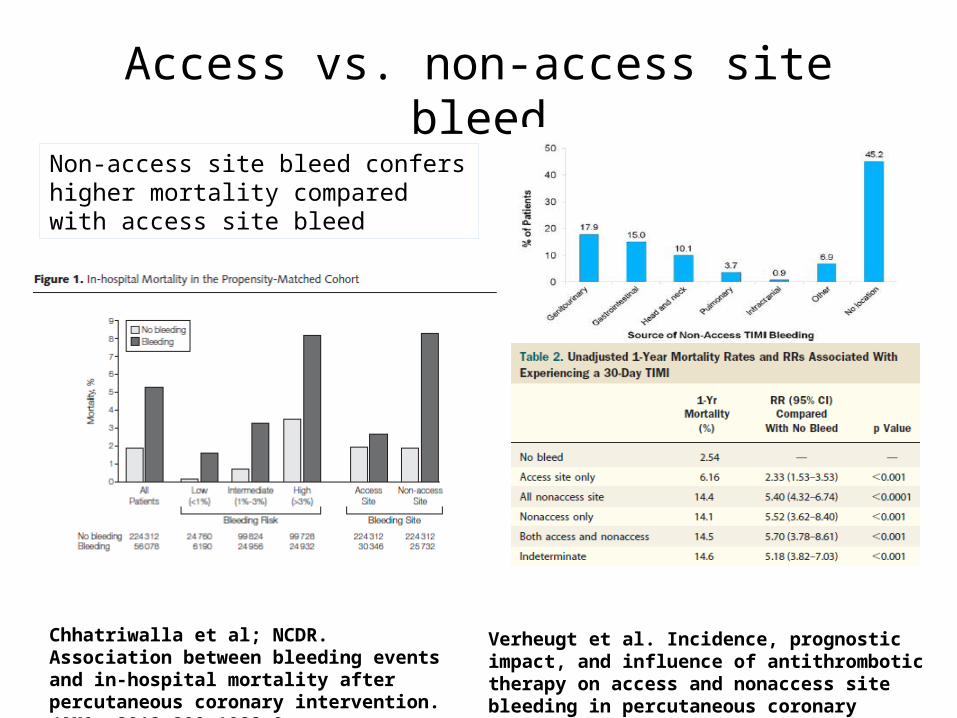
Access vs. non-access site bleed
Chhatriwalla et al; NCDR. Association between bleeding events and in-hospital mortality after percutaneous coronary intervention.JAMA. 2013;309:1022-9.
Verheugt et al. Incidence, prognostic impact, and influence of antithrombotic therapy on access and nonaccess site bleeding in percutaneous coronary intervention. JACC Cardiovasc Interv 2011;:191-7.
Non-access site bleed confers higher mortality compared with access site bleed

Bleeding across clinical presentations
SAP (n=6232) UAP (n=4705) NSTEMI (n=8335) STEMI (n=2562) CGS (n=852)0
5
10
15
20
25
30
0.700000000000001 1.1 2
4.3
15.4
2.1 2.84.3
7.8
27.4
Major bleeding (p<0.001)
Blood transfusion (p<0.001)
%
Loh, Waksman. Impact Of Clinical Presentation On In-Hospital Bleeding Outcomes In Percutaneous Coronary Intervention. TCT 2013

Patients at highest bleeding risk (NCDR): pre-procedural factors
Mehta SK, et al; NCDR. Bleeding in patients undergoing percutaneous coronary intervention: the development of a clinical risk algorithm from the NCDR. Circ Cardiovasc Interv. 2009;2:222-229.
Many risk factors co-exist in the elderly patient

Patients at highest bleeding risk: HORIZONS-AMI
Suh JW, et al. Impact of in-hospital major bleeding on late clinical outcomes after primary percutaneous coronary intervention in acute myocardial infarction the HORIZONS-AMI trial. J Am Coll Cardiol. 2011;58:1750-6.

Elderly patients at increased bleeding risk: NCDR/Medicare/Medicaid
Of patients who bled, access site bleed = 48.6%
Predominantly femoral access
PCI in 461311 patients≥ 65 yrs old
Post PCI bleeding in 3.1%
Rao SV et al. JACC Cardiovasc Interv 2012;5:958-65.

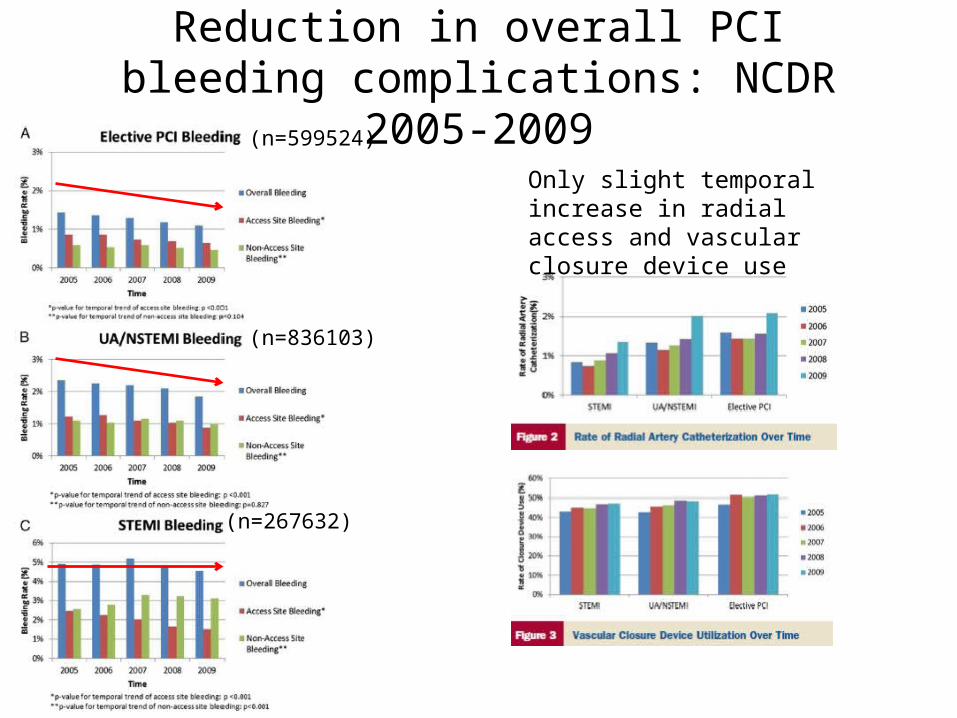
Reduction in overall PCI bleeding complications: NCDR 2005-2009
(n=599524)
(n=836103)
(n=267632)
Reduction in annual bleeding risk
Reduction in in annual bleeding risk
No change in annual bleeding risk
Subherwal S, et al. Temporal trends in and factors associated with bleeding complications among patients undergoing percutaneous coronary intervention: a report from the NCDR. J Am Coll Cardiol. 2012;59:1861-9.
Overall 20% reduction in post-PCI bleeding

Reduction in overall PCI bleeding complications: NCDR 2005-2009
(n=599524)
(n=836103)
(n=267632)
Temporal decrease in heparin + GPIIncrease in bivalirudin
No change in anticoagulation/ thrombolytic useIABP use 10%
Reduction in overall PCI bleeding complications: NCDR 2005-2009
(n=599524)
(n=836103)
(n=267632)
Only slight temporal increase in radial access and vascular closure device use

Bleeding avoidance strategies
Dauerman et al. Bleeding avoidance strategies. Consensus and controversy. J Am Coll Cardiol 2011;58:1-10.

Bleeding avoidance strategies:Consensus and Controversy
Dauerman et al. Bleeding avoidance strategies. Consensus and controversy. J Am Coll Cardiol 2011;58:1-10.

Pharmacology: Bivalirudin
Stone GW, et al; HORIZONS-AMI Trial Investigators. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med 2008;358:2218-30.

Pharmacology: BivalirudinReduction in both access and nonaccess site
bleeding compared to Hep + GPI
Verheugt FW, et al. Incidence, prognostic impact, and influence of antithrombotic therapy on access and nonaccess site bleeding in percutaneous coronary intervention. JACC Cardiovasc Interv 2011;4:191-7.

Pharmacology: BivalirudinDoes not reduce bleeding when used in conjunction with GPI
Time to event curve of major bleeding
Stone GW, et al. Bivalirudin in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a subgroup analysis from the ACUITY trial. Lancet 2007;369:907-19.

Bivalirudin vs. Heparin monotherapy
Bertrand OF, et al. Meta-analysis comparing bivalirudin versus heparin monotherapy on ischemic and bleeding outcomes after percutaneous coronary intervention. Am J Cardiol 2012;110:599-606.
Transfemoral
Decrease in major bleeding
Similar MACE
Bleeding outcomes

Effect of radial access on bleeding: Clinical trials
• Crossover rates 4-6%, age 60-65 yrs old• RIVAL (STEMI, n=1958): no difference in bleeding
(0.84% vs. 0.61%)• RIFLE-STEACS (n=1001): reduced bleeding (7.8% vs.
12.2%)• STEMI-RADIAL (n=707):

Growth of transradial access in the US: NCDR 2007-2012
Adoption of radial access and comparison of outcomes to femoral access in percutaneous coronary intervention: an updated report from the NCDR (2007-2012). Circulation 2013;127:2295-306.

Reduced bleeding and vascular complications in key subgroups with transradial access
Bleeding complications (unadjusted rates)
Vascular complications (unadjusted rates)

New generation antiplatelet therapy: efficacy
Newer generation antiplatelet agents significantly reduce adverse outcomes compared to clopidogrel up to 1-year in patients with ACS.
TRITON TIMI-38 PLATO
Wiviott et al. N Engl J Med 2007 15;357:2001-2015 Wallentin et al. N Engl J Med 2009;361(11):1045-57

Balance of efficacy and safety: Ticagrelor
Overall no difference in major bleeding as defined by the study criteria
More fatal intracranial bleed, non-CABG related bleed
Although no recommendation to dose-adjust in elderly, should take into consideration potential bleeding risks
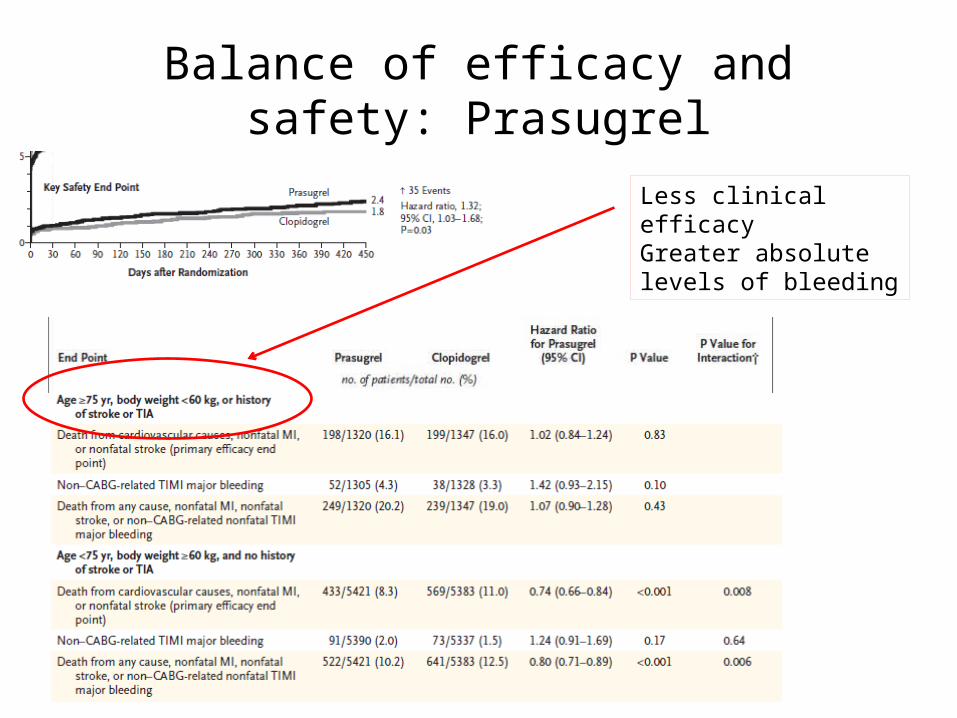
Balance of efficacy and safety: Prasugrel
Less clinical efficacyGreater absolute levels of bleeding

Dose adjust in the very elderly?
Prasugrel 5mg in very elderly met non-inferiority criterion by MPA vs. Prasugrel 10mg in non-elderly
Prasugrel 5mg resulted in fewer very elderly poor responders compared to clopidogrel 75mg
Erlinge D, et al. Prasugrel 5-mg in the very elderly attenuates platelet inhibition but maintains non-inferiority to prasugrel 10-mg in non-elderly patients: The GENERATIONS trial, a pharmacodynamic and pharmacokinetic study in stable CAD patients. J Am Coll Cardiol 2013 Jun 6. [Epub ahead of print]
Prasugrel 5mg suggested based on population pharmacokinetic substudy modeling in TRITON-TIMI 38.

Prasugrel: Summary of Boxed Warning
• Contraindications: Clinical hx of stroke/TIA
• Generally not recommended for age ≥ 75 yrs, except in high risk situations (prior MI, DM) where the ischemic benefit appears to be greater
• Greater risk of bleeding in patients weighing <60kg, can consider MD adjustment (5mg)

Summary• The elderly STEMI patient presents an extremely challenging
subset to treat due to presence of co-morbidities, high periprocedural mortality and significant morbidity.
• The elderly STEMI patients are at high risk of bleeding post PCI, and bleeding avoidance strategies should be employed as much as possible.
• There is still controversy towards certain strategies to reduce post-PCI bleed.
• The overall impact of transradial access on reduction of bleeding appears favorable,. However the greatest impact appears to be in the proper selection of antithrombotic therapy, especially in this high risk subpopulation.