Embed Size (px)
Citation preview

Stem Cell Transplantation for non-malignant pediatricnon-malignant pediatric
conditionsThe cost of cure
Leslie Lehmann M DLeslie Lehmann, M.D.Director, Pediatric Stem Cell Transplant Program,
Children’s Hospital/ Dana Farber, Boston

Indications in Non MalignantIndications in Non-Malignant Disorders
• Immunodeficiency Syndromes
Wiskott – AldrichHLH (H h ti L h hi ti t i )HLH (Hemophagocytic Lymphohistiocytosis)
aka Familial erythro/hemophagocytic lymphohistiocytosisChronic Granulomatous Disease

Indications in Non MalignantIndications in Non-Malignant Disorders
• Storage DiseasesStorage Diseases
• Osteopetrosis• Osteopetrosisaka: malignant infantile osteopetrosis

Indications in Non MalignantIndications in Non-Malignant Disorders
• Syndromes of Ineffective ErythropoiesisSyndromes of Ineffective Erythropoiesis
Th l i M jThalassemia Major
Sickle Cell DiseaseSickle Cell Disease

Unique considerations in non-li dimalignant diseases
• Rare, heterogeneous group of disorders withRare, heterogeneous group of disorders with variable outcomes
• Diagnosed at young age g y g g• Siblings may have disease or be carriers which
affects donor selection/future pregnancies/decisions regarding PGD
• Decision to undergo transplant very complicated in diseases not acutely life-threatening but impacting duration or quality of life

Unique considerations in non-li dimalignant diseases
• If acute SCT toxicities successfully navigated long term survival is very goodnavigated long-term survival is very good unlike in malignant disorders
• Successful SCT does not guarantee reversal of non-hematopoietic abnormalities

Immunodeficiency diseasesImmunodeficiency diseases
• SCT standard approach for infants withSCT standard approach for infants with significant immunodeficiency syndromes as early death likely without interventionas early death likely without intervention– Children are often very ill at
diagnosis/increased peri-SCT mortalitydiagnosis/increased peri SCT mortality – Role of reduced-intensity conditioning is being
elucidatedelucidated– Gene-therapy trials currently available for
SCID

WASWAS
• Rare X-linked disorderRare, X linked disorder• Microthrombocytopenia, eczema,
recurrent infectionsrecurrent infections• Cellular and humoral immune dysfunction• Increased risk of malignancy, mostly
lymphomas• SCT curative for immunodeficiency,
thrombocytopenia (Ozsahin, Blood,2008)y p ( , , )

Chronic Granulomatous DiseaseChronic Granulomatous Disease
• Failure of “oxygen burst” in phagocytesFailure of oxygen burst in phagocytes leads to impaired microbial killing
• Patients have recurrent infectionsPatients have recurrent infections• X-linked or autosomal recessive• Even with best supportive care only 50%• Even with best supportive care only 50%
of patients alive at 30 years• SCT from related or unrelated donor can• SCT from related or unrelated donor can
be curative with remission of colitis and catch-up growth ( Soncini, BJH, 2009)catch up growth ( Soncini, BJH, 2009)

HLHHLH
• Rare inherited disorderRare inherited disorder• Defective lymphocyte cytotoxic activity
results in uncontrolled proliferation ofresults in uncontrolled proliferation of macrophages and overproduction of inflammatory cytokinesinflammatory cytokines
• Children often very ill at presentation and t t d ith t t i dare treated with cytotoxic and
immunosuppresive therapy pre-SCT

HLHHLH
• SCT provides only curative optionSCT provides only curative option• Increased peri-SCT mortality
R d d i t it i b i• Reduced intensity regimens being investigated (Baker, BMT 2008) (Jordan, BMT 2008)

OsteopetrosisOsteopetrosis
• Congenital dysfunction of osteoclastsCongenital dysfunction of osteoclasts• Presents in infancy with extramedullary
hematopoiesis pancytopenia cranialhematopoiesis, pancytopenia, cranial nerve deficitsSCT i ti b t l t l t i• SCT is curative but early transplant is essential and neurological deficits may be
tpermanent (Driessen, BMT 2003)


Storage diseasesStorage diseases
• Heterogeneous group of congenitalHeterogeneous group of congenital disorders with deficiency in enzyme production that leads to accumulation ofproduction that leads to accumulation of substrate in multiple organs
• Marrow from unaffected donor corrects• Marrow from unaffected donor corrects hematopoietic compartment and may provide sufficient enzyme for other organsprovide sufficient enzyme for other organs

Storage diseasesStorage diseases
• Age and neurologic status are strongestAge and neurologic status are strongest predictors of outcome
• Successful SCT stops ongoing damage• Successful SCT stops ongoing damage and may reverse existing damageL t l i t t f i i• Long-term neurologic status of survivors is variable

Storage diseasesStorage diseases
• Best outcomes have been reported forBest outcomes have been reported for Hurlers Disease, Adrenoleukodystrophy and Globoid cell leukodystrophy (Peters Bloodand Globoid cell leukodystrophy (Peters, Blood, 2004)
• Use of umbilical cord blood as a stem cell source increases number of potential donors and can shorten time to SCT (Staba, ( ,nejm, 2004)

Thalassemia “ f h ”“of the sea”
• One of the most common geneticOne of the most common genetic disorders and the most common transfusion dependent anemia in the worldtransfusion dependent anemia in the world
• Inherited in an autosomal recessive mannermanner
• Affects almost 70,000 new infants per year

EpidemiologyEpidemiology
• Majority of cases occur in “ThalassemiaMajority of cases occur in Thalassemia Belt” - Mediterranean area, Africa, middle East Indian subcontinent Southeast AsiaEast, Indian subcontinent, Southeast Asia
• Disease concentrated in tropical areas due to protection against P falciparum malariato protection against P. falciparum malaria conferred by heterozygous state

Medical management of h l ithalassemia
• Chronic red cell transfusions every 4-6Chronic red cell transfusions every 4 6 weeks
Goals– Goals• Correct anemia• Suppress erythropoiesisSuppress erythropoiesis• Decrease GI iron absorption
– Complicationsp• Iron overload• Infectious exposures

Complications associated with iron l doverload
• Heart– Cardiac hypertrophy and dilatation
• Magnitude of iron loading in heart determines survivalLi• Liver– Portal fibrosis/cirrhosis– Result of hemosiderin deposits in parenchymal and– Result of hemosiderin deposits in parenchymal and
phagocytic cells• Endocrine glands
– Pituitary (gonadal failure), pancreas (DM), thyroid, adrenal

ChelationChelation
• Deferoxamine is the “gold standard”Deferoxamine is the gold standard– Only available by IV or SQ route
Usually need to use drug for 8 12 hours 5 6– Usually need to use drug for 8-12 hours 5-6 days a week beginning at age 3-5
• Oral chelators• Oral chelators– Not as well studied
M t b ff ti– May not be as effective

Outcome with medical management
• Life expectancy
Affected enormously by demographic and– Affected enormously by demographic and individual factors
Median survival exceeds 50 years in well• Median survival exceeds 50 years in well-chelated patients (Lawson, BrJHeme, 2003) but in UK 50% died before age 35 (Modell, BrMedJ, 1997)
• At age 25 99% survival if compliant withAt age 25, 99% survival if compliant with therapy but 70% in noncompliant (Piga, AnnNYAcadSci, 1998)

Psychological burdenPsychological burden
– Chronic illness that disrupts social relationships future plans (Atkin SocSciMed 2001)relationships, future plans (Atkin,SocSciMed, 2001)
– 60% of children < 18 reported anger/irritability, 50% reported a depressed mood and 21% had a suicide attempt or self-injury (Ghanizadeh, Iran JPedHO 2006)Iran, JPedHO, 2006)

Hemoglobin SS DiseaseHemoglobin SS Disease
• Affects 1/400 African-AmericansAffects 1/400 African Americans• Inherited disorder of hemoglobin
production leading to polymerization andproduction leading to polymerization and decreased deformability of the red cell in the deoxygenated stateyg
• Disease of endothelial damage – clinically most prominent in capillaries of lung, p p gcerebral-vascular system, spleen, skeleton, kidneys, eyes, penis

Medical management ofSi kl ll diSickle cell disease
• Severity of disease variable with few early predictors availablepredictors available
• Universal prophylaxis has dramatically d d hildh d f t litidecreased childhood fatalities
• Severely affected children may be treated with chronic transfusions or hydroxyrea

Medical management ofSi kl ll diSickle cell disease
• Life expectancy 40-60 yearsLife expectancy 40 60 years
P h l i l b d i bl th• Psychological burden as variable as the disease ranging from minimal symptoms t t k l d f ti d ito stroke, pulmonary dysfunction and pain crises causing constant hospitalizations
d ti d dand narcotic dependency

Transplant as a curative modalityTransplant as a curative modality
• Replacement of affected bone marrow by p yhealthy bone marrow restores normal hematopoiesis and cures diseaseFi l f h l i f d i• First transplant for thalassemia performed in 1982 and over 1500 transplants have now been done world-widedone world wide
• Usually restricted to patients having a matched family donor
• Usually restricted to sickle cell patients with significant disease manifestations

Cure =N l h l bi d iNormal hemoglobin production
In Sickle cell disease:• Resolution of VOC• Stable pulmonary disease• Possible correction of reticuloendothelial dysfunction (Ferster,
Blood 1993)
• Possible correction of osteonecrosis (Bernaudin, BMT 1997)
• Possible improvement in growth• Stable neurologic function/MRIg• Very good performance status

Cure =N l h l bi d iNormal hemoglobin production
In Thalassemia:• Freedom from transfusions• Improvement in growth• Resolution of liver fibrosis• Very good performance statuse y good pe o a ce status

The Cost of CureThe Cost of Cure
• Peri-SCT morbidity and mortalityPeri SCT morbidity and mortality• Risk of acute and chronic GVHD
Ri k f ft j ti• Risk of graft rejection• Restrictions• Long-term sequelae

Acute ComplicationsAcute Complications
• Nausea and vomitingNausea and vomiting• Mucositis
A i• Anorexia• Infections• 4-6 week hospital stay• 5-15% risk of mortality during acute5 15% risk of mortality during acute
transplant period

Graft versus host diseaseGraft versus host disease
• Acute GVHDAcute GVHD– Rash, diarrhea, hepatitis
Rarely significant in matched sibling setting in– Rarely significant in matched sibling setting in pediatric patients
– Usually responds to steroid therapy– Usually responds to steroid therapy

Graft versus Host DiseaseGraft versus Host Disease
• Chronic GVHDChronic GVHD– Scarring process that affects skin, liver, GI
tract, lung, eyes and mouth– Often steroid responsive but requires
prolonged immunosuppression– Risk factors include patient and donor age,
performance status pre-HSCT, multiple transfusions and prior infectionstransfusions and prior infections
– Occurs in ~10% of patients receiving matched sibling HSCT g

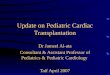
Chronic graft versus host disease

Restrictions or“ id li f f li i ”“guidelines for safe living”
• Patients are on immunosuppression for 6-9Patients are on immunosuppression for 6 9 months following SCT
• Neutropenia resolved but risk of life-threatening p gviral or fungal infection remains
• Patients can be inside only in their home/clinic yalthough outdoor activities are allowed
• Requires sophisticated economic and familial infrastructure

Graft rejectionGraft rejection
• Autologous reconstitution and return ofAutologous reconstitution and return of transfusion dependence
• Largest hurdle in transplant forLargest hurdle in transplant for hemoglobinopathies – hypercellular marrow due to ineffective erythropoiesis, y psensitization from transfusions, no prior immunosuppression
• Highest risk in older heavily-transfused patients

InfertilityInfertility
• The majority of patients undergoingThe majority of patients undergoing traditional ablative SCT have gonadal failure/infertilityfailure/infertility
• No definitive studies in this population where radiation is not used/no priorwhere radiation is not used/no prior chemotherapy/variable iron overload

Outcomes of matched sibling SCT i h l iin thalassemia
• Survival:Survival:– Class I – 95%– Class II – 84%Class II 84%– Class III – 79%
• Disease free survival = CUREDisease free survival CURE– Class I – 90%– Class II – 82%%– Class III – 57% (Galimberti, BMT, 1997)
• Extensive chronic GVHD in ~ 5%Extensive chronic GVHD in 5%

Outcomes of matched sibling SCT in Sickle Cell DiseaseS c e Ce sease
80-85% Disease Free Survival
5 10% Transplant related Mortality5-10% Transplant-related Mortality
10% Graft Rejection
10% cGVHD

Causes of death
% Alive
• Infection• Acute Chest Syndrome
85%
% Alive
• Acute Chest Syndrome• Organ Failure• CVA• Pulmonary Hypertension
(Gladwin,NEJM 2006)
50%
(Gladwin,NEJM 2006)
10 20 30 40 50 60
Yearsea s

Unrelated donor SCTUnrelated donor SCT
• In last decade marked improvement inIn last decade marked improvement in outcome following URD HSCT
High resolution molecular techniques for HLA– High resolution molecular techniques for HLA matching
– Improved GVHD prophylaxisImproved GVHD prophylaxis• First URD HSCT for thalassemia reported
in 1994 (Contu BMT 1994)in 1994 (Contu, BMT, 1994)

Nonmyeloablative SCTNonmyeloablative SCT
• Less intensive conditioning regimen withLess intensive conditioning regimen with goal of chimerism post transplant– Advantagesg
• Less upfront toxicity so attractive for older or high-risk patients
• Possible preservation of fertility• Possible preservation of fertility– Disadvantages
• Increased graft rejection – may be overcome with donor stem cell or l h t i f ilymphocyte infusions
• Increased incidence of chronic GVHD• Increased immunosuppression resulting in infectious complications

PBMTC protocolsPBMTC protocols
• Unrelated donor SCT for thalassemia orUnrelated donor SCT for thalassemia or severe sickle cell disease
• Bone marrow or cord blood as stem cell• Bone marrow or cord blood as stem cell sourceR d d i t it diti i i• Reduced-intensity conditioning regimen

Making the decisionMaking the decision
• Influenced byInfluenced by – Cultural norms– Donor availabilityy– Availability of well-matched, safe transfusions– Availability of chelation therapy– Patient compliance with transfusions, chelation– Patient and physician judgment re up-front risks,
fertility issues risk of chronic GVHDfertility issues, risk of chronic GVHD– Availability/accessibility of transplant center

RecommendationsRecommendations• HLA typing of parents and all siblings for any yp g p g y
child diagnosed with thalassemia or sickle cell disease
• Consultation with HSCT physician regardingConsultation with HSCT physician regarding risks and benefits of HSCT if matched family donor available/ discussion of PGDIf di l t f ili id f l• If medical management failing consider referral for consultation and URD search to determine if acceptable donor exists followed by HSCT
l i d SCT l if iconsultation and SCT on protocol if appropriate• Ideally both HSCT physician and hematologist
are present for all meetingsare present for all meetings

The goal of HSCTThe goal of HSCT


AcknowledgementsAcknowledgements
• Physician and nursing staff ofPhysician and nursing staff of DFCI/Children’s Hospital Boston who provide meticulous and compassionateprovide meticulous and compassionate care to our families
• Families whose children have a non• Families whose children have a non-malignant disease potentially cured by SCT who are struggling to determine theSCT who are struggling to determine the best therapy for their child