Embed Size (px)
Citation preview

Clinical Therapeutics/Volume 31, Number 10, 2009
October 2009 2215
Accepted for publication September 10, 2009.
Express Track online publication October 16, 2009.doi:10.1016/j.clinthera.2009.10.0070149-2918/$ - see front matter
© 2009 Excerpta Medica Inc. All rights reserved.
ABSTRACTBackground: Fampridine sustained release (SR) has
generally been well tolerated in clinical studies in pa-tients with multiple sclerosis (MS) at doses ≤20 mg/d. The pharmacokinetics of single escalating doses of fampridine SR (5, 10, 15, and 20 mg) were evaluated in a companion study.
Objectives: The primary objective of this study,which followed on from the single-dose pharmaco-kinetic study, was to assess the steady-state pharma-cokinetics of fampridine in patients with MS over2 weeks of oral administration of open-label fampri-dine SR 20 mg BID. Tolerability was also evaluated.
Methods: The dose of fampridine SR was titrated up-ward to twice-daily administration over days 1 and 2,with 20 mg given in the morning and 10 mg in theevening. From days 3 to 14, patients received fampri-dine SR 20 mg BID (total daily dose, 40 mg).Fampridine pharmacokinetic parameters were deter-mined on days 1, 8, and 15. The parameters of interestincluded Cmax, Tmax, Cmin, AUC, and apparent t1/2. These parameters were compared with those from the single-dose study. Tolerability was assessed based onadverse events, physical examinations, vital signs, laboratory tests, and ECGs.
Results: Twenty-one white patients who participated in the single-dose study were enrolled in the steady-state study (52.4% female; mean [SD] age, 45.1 [7.4] years; weight range, 54–87 kg). Fampridinepharmacokinetic parameters on day 1 were consistent with those obtained in the single-dose study. The Tmaxdid not differ significantly between day 1, day 8,day 15, and the single-dose study (range, 3.25–3.78 hours). Cmax values on days 8 and 15 (66.7 and62.6 ng/mL, respectively) were significantly higherthan those on day 1 (48.6 ng/mL) and in the single-dose study (50.5 ng/mL) (all, P < 0.001), reflecting
accumulation of fampridine with multiple dosing.Values for Cmax/Cmin did not differ significantly be-tween day 1 and the single-dose study (2.44 and 2.43,respectively) or between days 8 and 15 (2.90 and2.88, respectively); however, the single-dose and day-1 values differed significantly from the day-8 and day-15values (P ≤ 0.001). There were no significant differ-ences with respect to any other pharmacokinetic pa-rameters. One hundred adverse events were reported by 21 patients. With the exception of 1 case of severe nausea, all adverse events were of mild to moderate severity. Thirty-five events reported by 14 subjects were considered treatment related. Dizziness was the most common treatment-related adverse event, with 11 episodes reported by 8 patients. No clinically sig-nificant changes were found in clinical laboratoryvalues, vital signs, or physical examination findingsfrom baseline to the last visit, and there were no clini-cally significant changes in QTc intervals (Bazett’s correction).
Conclusions: In these patients with MS, thesteady-state pharmacokinetic profile of fampridine SR20 mg BID administered for 2 weeks appeared to support the use of twice-daily dosing in this popu-lation. This dosage was generally well tolerated. (Clin Ther. 2009;31:2215–2223) © 2009 ExcerptaMedica Inc.
Key words: 4-aminopyridine, fampridine SR,immediate-release fampridine, sustained release, mul-tiple sclerosis, pharmacokinetics.
Steady-State Pharmacokinetics and Tolerability of Orally Administered Fampridine Sustained-Release 10-mg Tablets in Patients With Multiple Sclerosis: A 2-Week, Open-Label, Follow-Up Study
Timothy Vollmer, MD1; Andrew R. Blight, PhD2; and Herbert R. Henney III, PharmD2
1University of Colorado, Denver, Colorado; and 2Acorda Therapeutics, Hawthorne, New York

2216 Volume 31 Number 10
Clinical Therapeutics
with spinal cord injury, with minor variability in ab-sorption characteristics noted in some subgroups of these patients.8,26,27 The differences included a 32%decrease in AUCtmax among tetraplegic patients rela-tive to paraplegic patients that was ascribed to a slower rate of initial absorption, although total bio-availability over the 12-hour assessment period did not differ between the 2 subgroups.8 Because pharmacoki-netic characteristics may predict variability in efficacy,the pharmacokinetics and safety profile of fampridineSR were evaluated in a study of single escalating dosesin patients with MS.28 That study found a prolongedt1/2 and lower Cmax values compared with those re-ported for fampridine IR.23,28,29
After acquisition of data on the pharmacokineticsof single escalating doses of fampridine SR,28 a follow-on study of repeated dosing was conducted in the same cohort of patients who had received fampridine SR at the maximum dose of 20 mg in the single-dose study. The entire study was conducted as part of a New Drug Application. The primary objective was to assess the steady-state pharmacokinetics of fampri-dine in patients with MS after twice-daily oral admin-istration of fampridine SR over a 2-week period. A secondary objective was to assess the tolerability of fampridine SR at steady state.
PATIENTS AND METHODSPatients
This follow-on study, conducted between Novem-ber 25, 1997, and February 10, 1998, enrolled patients who had successfully completed the study of single escalating doses of fampridine SR.28 Male and femalepatients with clinically definite MS (Poser criteria27) were eligible for participation. For inclusion, patientswere required to be between the ages of 18 and 65 years and be free of any clinically significant abnormality (other than MS) on the basis of medical history, physi-cal examination, and laboratory evaluation. Exclusioncriteria were participation in another trial (other than the single-dose pharmacokinetic study) within 30 days of fampridine dosing; history of alcohol or drug abuse; blood donation within the previous 30 days; known sensitivity to 4-aminopyridine or similar compounds; occurrence of a serious adverse event during the single-dose study; previous gastrointestinal surgery thatmight interfere with drug absorption; impaired liverfunction or receipt of known inducers or inhibitors of hepatic enzymes within 30 days before dosing; and
INTRODUCTIONRRThe demyelinated central nervous system axons thatare characteristic of multiple sclerosis (MS) exhibitconduction failure due in part to abnormal internodal potassium currents.1 Thus, pharmacologic modifica-tion of these potassium currents may have the poten-tial to improve nerve impulse conduction and mayoffer a useful therapeutic strategy for enhancing neu-romuscular function in individuals with MS. Fampri-dine (4-aminopyridine) is a potassium channel–blocking agent reported to restore conduction in focally demy-elinated axons.2,3 It may also enhance synaptic trans-mission in certain types of neurons and may potenti-ate neuromuscular transmission.4 There are several reports on the use of fampridine in various neurologicconditions,5–10 and clinical studies of a sustained-release (SR) formulation of fampridine have reportedsignificant improvements in walking compared withplacebo in patients with MS.11–14
Fampridine has been reported to have a relatively narrow therapeutic index, and several episodes of overdose have been reported, often in relation to usein an unregulated setting.15–19 Although fampridinehas not been approved for use by any national regula-tory body, some compounding pharmacies prepare immediate-release (IR) formulations, generally for usein patients with MS. Use of compounded IR formula-tions of fampridine occurs despite the fact that onethird of compounded drugs have failed standard quality tests.20 Furthermore, a recent report described4 cases of fampridine overdose due to a compounding error that resulted in a 10-fold increase in dosage strength.21 Exact dosing of fampridine is particularlyimportant, as IR formulations have a Tmax of ~1 hour and a short t1/2 of ~3.5 hours.22–24 In addition, the in-cidence of adverse events appears to be dependent on plasma concentrations, with a 4-fold higher incidence of adverse events reported at a mean (SE) plasma con-centration of 83 (6) ng/mL than at a concentration of 46 (4) ng/mL (36 vs 9 events, respectively).25
Fampridine SR was developed to reduce the phar-macokinetic limitations and some of the safety con-cerns associated with IR formulations. The safety andefficacy profiles of a twice-daily dosing regimen of fam-pridine SR have been reported in 2 clinical trials.13,14
Twice-daily dosing may be more convenient for pa-tients than the multiple daily doses required with IR formulations. The pharmacokinetic characteristics of fampridine SR also have been evaluated in patients

October 2009 2217
T. Vollmer et al.
tients were admitted to the study sites for the 24-hour period after drug intake on sampling days. Additionalsamples were obtained at 14, 18, and 20 hours onday 14, and at 30 and 36 hours on day 15. Sample preparation and analysis were performed as describedfor the single-dose pharmacokinetic study; validation methods were described in the same publication.28
Plasma samples were assayed by the Drug StudiesUnit, Analytical Division, University of California, San Francisco, using validated liquid-chromatographytechniques. Interday precision (%CV) ranged from 5.18% to 9.37%, and interday accuracy (relative er-ror [RE], calculated as [([mean-nominal concentration]/nominal concentration) × 100], ranged from –4.67%to +7.25%. Intraday precision (%CV) ranged from 2.49% to 8.28%, and the intraday RE ranged from –5.50% to –6.00%. The lower limit of quantification for the assay was equivalent to the low point of the standard curve, or nominally 1.00 ng/mL. The transday mean, %CV, and RE values were 1.83 ng/mL,11.7%, and –7.00%, respectively; the correspondinginterday values were 1.88 ng/mL, 10.6%, and –6.00%.
Pharmacokinetic parameters were estimated using nonparametric methods.30 Cmin represented observed concentrations at 12 hours after dosing, and the ratio of Cmax/Cmin was used to estimate fluctuations in con-centrations. The apparent terminal rate constant (ke) was estimated as the negative slope, calculated by least squares regression, of the last 3 observed natu-ral log concentration–time points. The AUC0–12h on days 8 and 15 was calculated using the linear trape-zoidal rule from the time of the morning dose to Cmax, and by the log-linear trapezoidal rule from Cmax toCmin. Apparent CL/F (clearance divided by bioavail-ability) on days 8 and 15 was estimated as the fampri-dine dose divided by AUC0–12h.
TolerabilityTolerability during the 2-week study period was de-
termined based on reported adverse events and regularphysical examinations, monitoring of vital signs, andlaboratory tests. Adverse-event data were obtainedby observation during admissions for drug adminis-tration and blood collection, and by interviews before, during, and after each drug-administration and blood-collection phase. All adverse events were reported, regardless of their causality, and the relationship between adverse events and study treatment wasdetermined.
history of epilepsy, psychiatric disorder, cardiac ar-rhythmias, or infection. Women who were lactating,pregnant, or of childbearing age and not using ap-proved birth control methods were also excluded,as were those who were significantly underweightor overweight in the opinion of the investigator, who tested positive for HIV, or who had evidence of malignancy.
Study DesignThis Phase I-II, open-label, single-period, multiple-
dose trial was conducted at 2 sites: University of Rochester Medical Center, Rochester, New York, andYale University School of Medicine, New Haven,Connecticut. It was carried out in compliance with national regulations for good clinical practice and inaccordance with the Declaration of Helsinki (3rd revi-sion). The protocol was approved by local ethics com-mittees (Western Institutional Review Board, Olym-pia, Washington, and Human Investigation Committee,Yale University School of Medicine), and written in-formed consent was obtained from all patients before study participation.
Enrollees who had successfully completed the dose-escalating study had received the maximum single dose of fampridine SR (20 mg). In the present study,the fampridine SR dose was titrated upward to twice-daily administration over days 1 and 2, with 20 mggiven in the morning and 10 mg in the evening. Fromdays 3 to 14, patients received fampridine SR 20 mg BID (total daily dose, 40 mg). Patients fasted from2 hours before dosing to 2 hours after dosing. Thedose was decreased by half in any patient with a plasma 4-aminopyridine concentration >90 ng/mL atany time during the trial. This was done to ensure subjects’ safety, for which purpose fampridine plasmaconcentrations were determined on days 2 and 8 of the study.
Pharmacokinetic AnalysisFampridine pharmacokinetic parameters were de-
termined on days 1, 8, and 15. Blood samples foranalysis of fampridine were collected after the initialdose on day 1, on day 8, and at study termination on day 15. These samples were collected immediatelybefore drug administration, hourly for the first 8 hoursafter administration, and subsequently at 10, 12, and 24 hours after administration. Because of the fre-quency of sampling for pharmacokinetic analysis, pa-

2218 Volume 31 Number 10
Clinical Therapeutics
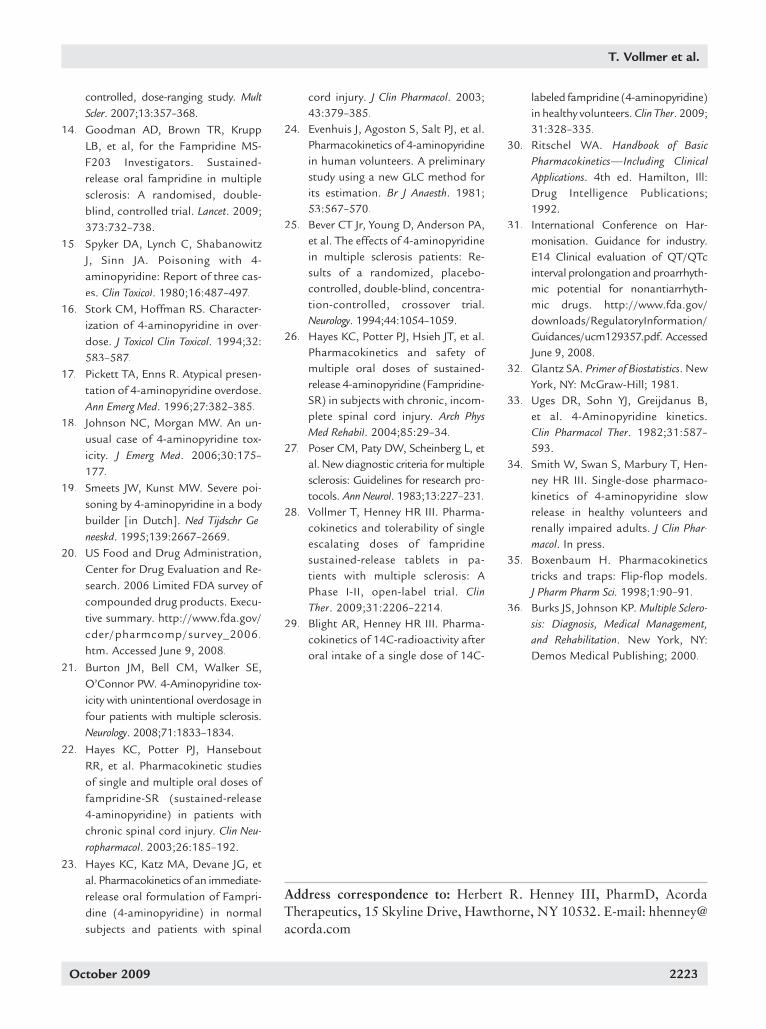
dose of 20 mg. Cmax and Cmax/Cmin were 66.7 ng/mLand 2.90, respectively, on day 8 and 62.6 ng/mL and2.88 on day 15. Cmax and Cmax/Cmin values on days 8and 15 were significantly greater than those duringsingle-dose treatment (50.5 ng/mL and 2.43) or onday 1 (48.6 ng/mL and 2.44) (all, P ≤ 0.001), reflecting accumulation of fampridine with multiple dosing. There were no significant differences in Cmax, Cmax/Cxx min, ap-parent CL/F, or AUC between days 8 and 15. Further-more, the AUC0–12h on days 8 and 15 (531 and 499 ng · h/mL, respectively) did not differ significantly fromthe dose-normalized AUC from the single-dose study(569 ng · h/mL). Similarly, there were no significant differences between estimates of apparent CL/F ondays 8 and 15 (700 and 703 mL/min) compared with the single-dose study (635 mL/min). There were no significant differences between the apparent ke and apparent t1/2 on day 15 (0.13 and 5.75 hours, respec-tively) compared with those in the single-dose study (0.14 and 5.13 hours). Normalization for dose andweight did not substantially affect the results (Table III). Weight-normalized doses ranged from 0.23 to0.36 mg/kg. The figure plots fampridine plasma con-centrations over time on days 1, 8, and 15, and in thesingle-dose study.
A 12-lead ECG was performed at baseline (0.5 hourbefore dosing) and at 1, 4, 12, and 24 hours after eachdose. ECGs were assessed for changes in the QT inter-rrval and QRS amplitude, as evaluation of pharmaco-logic therapies for potential cardiac effects, particularlyprolongation of the QT interval, is an important safety objective of the US Food and Drug Administration.31
As part of the interpretation of the ECGs, the QTinterval was corrected using the Bazett formula (QTc =QT/RR0.5), as recommended by International Confer-ence on Harmonisation guidance E14.31 All safety as-sessments, including examination of laboratory valuesand ECG results, were performed by the on-site physi-cian, including the assessment of clinical relevance.
Statistical AnalysisPrimary pharmacokinetic variables—Cmax, Tmax,
Cmin, AUC, and apparent t1/2—were analyzed using inferential statistics.32 The apparent t1/2 for each pa-tient was calculated based on the individual ke. Means and SDs were calculated for each parameter. Tolera-bility data were presented using descriptive statistics.
RESULTSPatient Disposition
Twenty-one of the 23 patients who successfullycompleted the single-dose study were enrolled in thepresent study. One patient discontinued on day 1 be-cause of a relapse of MS. Several minor protocol de-viations occurred, mainly omissions of data that wereconsidered to have no impact on the integrity of thestudy. One patient had an interruption of the dosingregimen because of a urinary tract infection that was considered unrelated to treatment.
The demographic characteristics of the 21 enrolledpatients are summarized in Table I. Ten were male and11 were female; all were white. The population had amean age of 45.1 years (range, 29–57 years). Their mean weight and height were 73.5 kg (162.1 lb) and171.7 cm (67.6 inches), respectively. The mean age of onset of MS was 29.8 years (range, 19–50 years).
Pharmacokinetic ProfileEstimates of fampridine pharmacokinetic parame-
ters for each evaluation day during the multiple-dosestudy, along with the corresponding values from thesingle-dose study,28 are summarized in Table II. Esti-mates on day 1 after the first dose were consistent with those obtained in the single-dose study, normalized to a
Table I. Demographic characteristics (N = 21).
Variable Value
Sex, no. (%)Female 11 (52.4)Male 10 (47.6)
White race, no. (%) 21 (100)
Age, yMean (SD) 45.1 (7.4)Range 29–57
Age at onset of MS, yMean (SD) 29.8 (8.3)Range 19–50
Weight, kgMean (SD) 73.5 (10.1)Range 54–87
Height, cmMean (SD) 171.7 (7.4)Range 158–183
MS = multiple sclerosis.

October 2009 2219
T. Vollmer et al.
tremor (2 events in 2 patients). Adverse events aresummarized by body system in Table IV.
All adverse events were mild to moderate in severi-ty, with the exception of 1 case of severe nausea.When the adverse-event data were evaluated based onmg/kg doses, 50 of 100 events occurred at the lowest dose, compared with 4 events (all of moderate severi-ty) occurring at the highest dose.
There were no clinically significant changes frombaseline to the last visit in terms of clinical laboratory values, vital signs, or physical examination findings. One patient had a clinically significant, nonserious
TolerabilityOne serious adverse event occurred during the
study—the relapse of MS in the patient who discon-tinued on day 1. This event was considered unrelated to the study drug. Overall, 100 adverse events werereported by 21 patients. Of these, 35 (in 14 subjects)were considered treatment related. Dizziness was themost common treatment-related adverse event, with11 episodes reported by 8 patients. Other treatment-related adverse events occurring in >1 patient includednausea (10 events in 7 patients), ataxia (2 events in2 patients), insomnia (2 events in 2 patients), and
Table II. Estimated mean (95% CI) fampridine pharmacokinetic parameters.
Pharmacokinetic Parameter Single-Dose Study* Day 1 Day 8 Day 15
TmaxT , h 3.76 (3.46–4.06) 3.78 (3.24–4.32) 3.33 (2.79–3.87) 3.25 (2.64–3.86)
Cmax, ng/mL 50.5 (45.2–55.7)† 48.6 (42.0–55.3) 66.7 (57.5–76.0)‡ 62.6 (55.7–69.4)‡
Cmin (at 12 h), ng/mL 21.4 (18.8–24.1)† 21.4 (18.2–24.6) 23.9 (19.6–28.3) 23.0 (19.5–26.5)
Cmax/Cmin 2.43 (2.23–2.63) 2.44 (2.00–2.88) 2.90 (2.69–3.11)‡ 2.88 (2.51–3.25)‡
AUC, ng · h/mL 569 (501–637)† NE 531 (452–610) 499 (446–552)
CL/F, mL/min 635 (567–703) NE 700 (557–844) 703 (621–786)
ke, h–1 0.14 (0.12–0.16) NE NE 0.13 (0.11–0.15)
t1/2, h§ 5.13 (4.53–5.73) NE NE 5.75 (4.95–6.55)
NE = not evaluable; ke = terminal rate constant; t1/2 = apparent elimination half-life.*Includes data for 21 of 23 patients who completed the single-dose study28 and were enrolled in the present study.† Normalized to a 20-mg dose.‡ P ≤ 0.001 versus single-dose study and day 1.§ Calculated based on individual subjects’ ke.
Table III. Mean (SE) estimates of fampridine pharmacokinetic parameters, normalized by dose and weight.
Pharmacokinetic Parameter Day 1 Day 8 Day 15
Cmax, ng/mL 177.90 (9.63) 240.43 (13.99) 229.26 (10.80)
Cmin, ng/mL 78.77 (5.42) 86.45 (7.28) 84.14 (5.97)
AUC, ng · h/mL NE 1910 (118) 1832 (87)
NE = not evaluable.

2220 Volume 31 Number 10
Clinical Therapeutics
evaluated its tolerability during steady-state dosing. After a 2-day titration period, multiple dosing of fampridine SR 40 mg/d was associated with signifi-cant increases in Cmax and Cmax/Cmin on days 8 and 15relative to day 1, as well as compared with single-doseadministration in the previous study (all, P ≤ 0.001).28
The lack of significant differences in Cmax, Cmin,AUC, and apparent CL/F between days 8 and 15 sug-gests that steady state was reached before day 8;by calculation, steady state would be achieved within39 hours. There was no evidence of significant al-terations in pharmacokinetics over the 2-week periodof multiple dosing with fampridine SR. Estimates of AUC and apparent CL/F on days 8 and 15, and of apparent ke and apparent t1/2 on day 15 did not dif-fer significantly from the corresponding estimates from the single-dose study. Although weight, age, and sex appeared to have an effect on apparent CL/F in the single-dose study, these effects were not evaluated with respect to steady-state pharmacoki-netics. Normalization for dose and weight did not substantially alter values for Cmax, Cmin, or AUC inthis study. The improved pharmacokinetic profile observed with fampridine SR in this study was simi-
elevation in glucose concentration (136 mg/dL) thatreturned to normal without intervention and was con-sidered unrelated to treatment. There were no clini-cally significant changes in QTc intervals (Table V) or QRS amplitudes after the administration of fampri-dine SR.
DISCUSSIONSeveral studies have characterized the pharmacokinet-ics of oral fampridine IR.23,24,33 Because the IR formu-lation is rapidly absorbed, with an apparent plasmat1/2 of ~3.5 hours, ≥4 daily doses of the IR formulationwould be needed to maintain therapeutic plasma con-centrations. Fampridine SR was developed to provide more sustained plasma concentrations relative to IR formulations. The SR formulation effectively prolongs absorption, with a Tmax of 3.75 hours and an appar-ent t1/2 of 5.47 hours.28 The effects of the altered re-lease characteristics of fampridine, as observed in this study and illustrated by the results of 2 clinical trials in patients with MS,13,14 support the use of twice-daily dosing.
This study further characterized the pharmacoki-netic profile of fampridine SR in patients with MS and
20
10
40
60
0
Plas
ma
Con
cent
ratio
n (n
g/m
L)
18151296 22 23213 17141185 202 16131074 1910 24
Time (h)
Day 1Day 8Day 15Single dose
70
30
50
Figure. Fampridine plasma concentrations over time.

October 2009 2221
T. Vollmer et al.
In this study, fampridine SR was completely ab-sorbed after oral administration. However, the appar-ent t1/2 at steady state in this study (5.75 hours) does not represent the true elimination t1/2 of fampridine, as it exceeded what is believed to be the true elimina-tion t1/2 of fampridine (3.14 hours), as determined by Blight and Henney.29 The formulation tested in the pres-ent study releases ~50% of drug in solution over 4 hoursin a sustained manner (data on file, Acorda Therapeu-tics, June 13, 2007). This longer apparent t1/2 supportsan effect on elimination as a result of the delay in ab-sorption of fampridine from the SR formulation, aneffect sometimes referred to as flip-flop pharmacokinet-ics.35 To evaluate the potential effect of flip-floppharmacokinetics, noncompartmental first-order phar-rrmacokinetics were used to determine the apparent phar-rrmacokinetic parameters of fampridine SR. To examine whether delayed absorption would affect estimation of the ke, the following equation was applied to the data:Tmax*Cmax = AUC*e–1.35 The results of the 2 sides of thecalculation revealed approximately equal values; thus, itwas assumed that delayed absorption had an effect on elimination, and the values for t1/2, ke, and CL/F werereported as apparent values throughout.
Two weeks of treatment with fampridine SR 40 mg/d was generally well tolerated in these patients with MS.The adverse-event profile was consistent with that re-ported in the single-dose study.28 Dizziness was the mostcommon treatment-related adverse event, and therewere no clinically significant changes in mean clinicallaboratory values, vital signs, or physical examinationfindings from baseline to the last visit. Also consistentwith the single-dose study, no clinically significantchanges in QTc intervals were observed. Furthermore,no relationship was observed between the QTc intervaland plasma concentrations of fampridine, although limited cardiac safety information was collected in thisstudy. There were no changes in QRS amplitudes after administration of fampridine SR.
The generalizability of the study results is limited by the relatively small sample size and the fact that all subjects were white. However, between 75% and 90%of people with MS are white and of European back-ground.36 Nonetheless, the impact of pharmacoge-nomic differences between ethnic groups cannot be ruled out.
The results of pharmacokinetic studies,28,29,34 along with evidence of the efficacy of fampridine SR in the treatment of impaired mobility in patients with MS,12,14
lar to that reported in studies in healthy volunteers34
and in patients with spinal cord injury.8,22,26 How-ever, because all patients in the present study werewhite, the results may not be generalizable to a moreheterogeneous population.
Table IV. Adverse events (no. [%] of patients), by body system (N = 21).
Treatment-All-Cause RelatedAdverse Adverse
Body System Events* Events†
Body as a wholeAsthenia 5 (23.8) –Headache 5 (23.8) 1 (4.8)
Infection 2 (9.5) –Injection-site pain 1 (4.8) 1 (4.8)Pain 2 (9.5) –
CardiovascularPalpitation 1 (4.8) 1 (4.8)
DigestiveAnorexia 1 (4.8) 1 (4.8)Nausea 8 (38.1) 7 (33.3)Mouth ulceration 2 (9.5) –Vomiting 1 (4.8) 1 (4.8)
Metabolic and nutrition
Edema 2 (9.5) –
MusculoskeletalArthralgia 2 (9.5) –
NervousAmnesia 2 (9.5) 1 (4.8)Ataxia 4 (19.0) 2 (9.5)Dizziness 10 (47.6) 8 (38.1)Abnormal gait 3 (14.3) –Hypertonia 3 (14.3) –Insomnia 3 (14.3) 2 (9.5)Nervousness 1 (4.8) 1 (4.8)Paresthesia 2 (9.5) 1 (4.8)Tremor 3 (14.3) 2 (9.5)
UrogenitalUrinary frequency 2 (9.5) –Urinary retention 2 (9.5) –
*Adverse events occurring in >1 patient, except for thepurposes of comparison with treatment-related ad-verse events.
† The patients listed in this column account for all 35 treatment-related adverse events.

2222 Volume 31 Number 10
Clinical Therapeutics
4. Lundh H, Thesleff S. The mode of action of 4-aminopyridineand guanidine on transmitter release from motor nerveterminals. Eur J Pharmacol. 1977;42:411–412.
5. Hansebout RR, Blight AR, Fawcett S, Reddy K. 4-Aminopyridine in chronic spinal cord injury: A controlled,double-blind, crossover study in eight patients. J Neuro-trauma. 1993;10:1–18.
6. Potter PJ, Hayes KC, Hsieh JT, et al. Sustained improve-ments in neurological function in spinal cord injured pa-tients treated with oral 4-aminopyridine: Three cases.Spinal Cord. 1998;36:147–155.
7. Segal JL, Pathak MS, Hernandez JP, et al. Safety and effi-cacy of 4-aminopyridine in humans with spinal cord in-jury: A long-term, controlled trial. Pharmacotherapy.1999;19:713–723.
8. Segal JL, Hayes KC, Brunnemann SR, et al. Absorptioncharacteristics of sustained-release 4-aminopyridine (fam-pridine SR) in patients with chronic spinal cord injury.J Clin Pharmacol. 2000;40:402–409.
9. van der Bruggen MA, Huisman HB, Beckerman H, et al. Ran-domized trial of 4-aminopyridine in patients with chronic in-complete spinal cord injury. J Neurol. 2001;248:665–671.
10. Cardenas DD, Ditunno J, Graziani V, et al. Phase 2 trial of sustained-release fampridine in chronic spinal cord injury.Spinal Cord. 2007;45:158–168.
11. Polman CH, Bertelsmann FW, van Loenen AC, Koetsier JC. 4-Aminopyridine in the treatment of patients withmultiple sclerosis. Long-term efficacy and safety. ArchNeurol. 1994;51:292–296.
12. Schwid SR, Petrie MD, McDermott MP, et al. Quantitativeassessment of sustained-release 4-aminopyridine for symptomatic treatment of multiple sclerosis. Neurology.1997;48:817–821.
13. Goodman AD, Cohen JA, Cross A, et al. Fampridine-SR inmultiple sclerosis: A randomized, double blind, placebo-
suggest that fampridine SR may have a role in the management of MS.
CONCLUSIONSFollowing on the study of single escalating doses, this steady-state study in patients with MS extends under-standing of the pharmacokinetic profile of fampridine SR. The results suggest that fampridine SR may have alower potential for peak concentration–related adverse events compared with the IR formulation, as well as the convenience of a twice-daily dosing regimen. Fampri-dine SR was generally well tolerated in this study.
ACKNOWLEDGMENTSThis study was supported by Acorda Therapeutics. Drs. Blight and Henney are employees of AcordaTherapeutics and hold stock in the company. The au-thors have indicated that they have no other conflictsof interest regarding the content of this article.
E. Jay Bienen, PhD, an independent scientific con-sultant based in New York City, provided editorialsupport, which was funded by Acorda Therapeutics.
REFERENCES1. Judge SI, Bever CT Jr. Potassium channel blockers in mul-
tiple sclerosis: Neuronal Kv channels and effects of symp-tomatic treatment. Pharmacol Ther. 2006;111:224–259.
2. Targ EF, Kocsis JD. 4-Aminopyridine leads to restoration of conduction in demyelinated rat sciatic nerve. Brain Res.1985;328:358–361.
3. Shi R, Blight AR. Differential effects of low and high concen-trations of 4-aminopyridine on axonal conduction in normal and injured spinal cord. Neuroscience. 1997;77:553–562.
Table V. Mean (SEM) QTc intervals (Bazett correction).
QTc Interval, msec
Study Day Baseline* 1 Hour 4 Hours 12 Hours 24 Hours
Day 1 n = 19 n = 19 n = 19 n = 19 n = 19408 (6.3) 401 (6.6) 404 (7.0) 393 (12.7) 408 (5.5)
Day 7 n = 18 n = 17 n = 16 n = 17 n = 17407 (7.5) 405 (6.2) 406 (6.8) 399 (5.8) 409 (6.7)
Day 14 n = 18 n = 18 n = 18 n = 17 n = 12413 (7.6) 402 (7.9) 411 (6.9) 402 (6.2) 409 (12.8)
*The baseline QTc interval was measured 0.5 hour before administration of fampridine sustained release.
October 2009 2223
T. Vollmer et al.
labeled fampridine (4-aminopyridine)in healthy volunteers. Clin Ther. 2009;31:328–335.
30. Ritschel WA. Handbook of Basic Pharmacokinetics—Including Clinical Applications. 4th ed. Hamilton, Ill:Drug Intelligence Publications;1992.
31. International Conference on Har-monisation. Guidance for industry.E14 Clinical evaluation of QT/QTcinterval prolongation and proarrhyth-mic potential for nonantiarrhyth-mic drugs. http://www.fda.gov/downloads/RegulatoryInformation/Guidances/ucm129357.pdf. AccessedJune 9, 2008.
32. Glantz SA. Primer of Biostatistics. New York, NY: McGraw-Hill; 1981.
33. Uges DR, Sohn YJ, Greijdanus B,et al. 4-Aminopyridine kinetics.Clin Pharmacol Ther. 1982;31:587–593.
34. Smith W, Swan S, Marbury T, Hen-ney HR III. Single-dose pharmaco-kinetics of 4-aminopyridine slow release in healthy volunteers andrenally impaired adults. J Clin Phar-rrmacol. In press.
35. Boxenbaum H. Pharmacokineticstricks and traps: Flip-flop models.J Pharm Pharm Sci. 1998;1:90–91.
36. Burks JS, Johnson KP. Multiple Sclero-sis: Diagnosis, Medical Management,and Rehabilitation. New York, NY:Demos Medical Publishing; 2000.
cord injury. J Clin Pharmacol. 2003;43:379–385.
24. Evenhuis J, Agoston S, Salt PJ, et al.Pharmacokinetics of 4-aminopyridinein human volunteers. A preliminary study using a new GLC method for its estimation. Br J Anaesth. 1981;53:567–570.
25. Bever CT Jr, Young D, Anderson PA,et al. The effects of 4-aminopyridinein multiple sclerosis patients: Re-sults of a randomized, placebo-controlled, double-blind, concentra-tion-controlled, crossover trial.Neurology. 1994;44:1054–1059.
26. Hayes KC, Potter PJ, Hsieh JT, et al.Pharmacokinetics and safety of multiple oral doses of sustained-release 4-aminopyridine (Fampridine-SR) in subjects with chronic, incom-plete spinal cord injury. Arch PhysMed Rehabil. 2004;85:29–34.
27. Poser CM, Paty DW, Scheinberg L, etal. New diagnostic criteria for multiplesclerosis: Guidelines for research pro-tocols. Ann Neurol. 1983;13:227–231.
28. Vollmer T, Henney HR III. Pharma-cokinetics and tolerability of singleescalating doses of fampridinesustained-release tablets in pa-tients with multiple sclerosis: APhase I-II, open-label trial. ClinTher. 2009;31:2206–2214.
29. Blight AR, Henney HR III. Pharma-cokinetics of 14C-radioactivity after oral intake of a single dose of 14C-
controlled, dose-ranging study. Mult Scler. 2007;13:357–368.
14. Goodman AD, Brown TR, KruppLB, et al, for the Fampridine MS-F203 Investigators. Sustained-release oral fampridine in multiplesclerosis: A randomised, double-blind, controlled trial. Lancet. 2009;373:732–738.
15. Spyker DA, Lynch C, ShabanowitzJ, Sinn JA. Poisoning with 4-aminopyridine: Report of three cas-es. Clin Toxicol. 1980;16:487–497.
16. Stork CM, Hoffman RS. Character-ization of 4-aminopyridine in over-dose. J Toxicol Clin Toxicol. 1994;32:583–587.
17. Pickett TA, Enns R. Atypical presen-tation of 4-aminopyridine overdose.Ann Emerg Med. 1996;27:382–385.
18. Johnson NC, Morgan MW. An un-usual case of 4-aminopyridine tox-icity. J Emerg Med. 2006;30:175–177.
19. Smeets JW, Kunst MW. Severe poi-soning by 4-aminopyridine in a body builder [in Dutch]. Ned Tijdschr Ge-neeskd. 1995;139:2667–2669.
20. US Food and Drug Administration,Center for Drug Evaluation and Re-search. 2006 Limited FDA survey of compounded drug products. Execu-tive summary. http://www.fda.gov/cder/pharmcomp/survey_2006.htm. Accessed June 9, 2008.
21. Burton JM, Bell CM, Walker SE,O’Connor PW. 4-Aminopyridine tox-icity with unintentional overdosage infour patients with multiple sclerosis.Neurology. 2008;71:1833–1834.
22. Hayes KC, Potter PJ, HanseboutRR, et al. Pharmacokinetic studiesof single and multiple oral doses of fampridine-SR (sustained-release4-aminopyridine) in patients withchronic spinal cord injury. Clin Neu-ropharmacol. 2003;26:185–192.
23. Hayes KC, Katz MA, Devane JG, etal. Pharmacokinetics of an immediate-release oral formulation of Fampri-dine (4-aminopyridine) in normalsubjects and patients with spinal
Address correspondence to: Herbert R. Henney III, PharmD, AcordaTherapeutics, 15 Skyline Drive, Hawthorne, NY 10532. E-mail: [email protected]