-
Stayin’ Alive or Another One Bites
the Dust: The Science
Behind Good CPRSco$ Gilmore, MD,
EMT-‐P, FACEP
Medical Director St. Louis Fire
Department
-
A Li?le Background
• Incidence of cardiac arrest • 20
to 140 per 100,000 people
globally
• Survival • 2% to 11% globally
• Less then 15% in the United
States
• 3.0% to 16.3% according to the
ResuscitaPon Outcomes ConsorPum (ROC)
-
CPR is a lifesaving interven-on
and the cornerstone of resuscitaPon
from cardiac
arrest.
CPR quality has significant impact
on survival.
-
Current Knowledge
of CPR Quality
Optimal Implementation
Preventable Deaths
-
CPR is not a perfect
subsPtute for a beaPng heart But
it is the best
thing that we can do in the
out
of hospital seWng
-
Restore spontaneous circulaPon as
quickly as possible.
-
Five Main Components of
High-‐performance CPR
• Chest compression fracPon (CCF)
• Chest compression rate • Chest
compression depth • Chest recoil
(residual leaning) • VenPlaPon
-
Minimize InterrupKons
• Goal is a chest compression
fracPon greater than 80%
• This means less than 24 seconds
off the chest every 2 minutes
• Lower CCF is associated with
decreased ROSC and survival to
hospital discharge
-
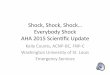
Chest Compression FracKon and Survival
In Ventricular FibrillaKon Arrest
Christenson J et al. Chest
compression fracPon determines survival
in paPents with out-‐of-‐hospital
ventricular fibrillaPon. CirculaPon.
2009;120:1241-‐1247
-
Chest Compression FracKon and Survival
In Non-‐Ventricular FibrillaKon Arrest
Vaillancourt C et al. The impact
of increased chest compression
fracPon on return of spontaneous
circulaPon for out-‐of-‐hospital cardiac
arrest paPents not in ventricular
fibrillaPon. ResuscitaPon. 2011;82:1501-‐1507
-
Manual versus AED mode
Cheskes S et al. Perishock pause:
an independent indicator of survival
from out-‐of-‐hospital cardiac arrest.
CirculaPon. 2011;124:58-‐66
-
Chest Compression Rates
• 2010 AHA Guidelines for CPR and
ECC recommend a chest compression
rate ≥ 100/minute
-
Chest Compression Rate
Idris AH et al. RelaPonship
between chest compressions rates and
outcomes from cardiac arrest.
CirculaPon. 2012; 125:3004-‐3012.
-
• As chest compression rates fall,
a significant drop-‐off in ROSC
occurs • Higher chest compression
rates
• May reduce coronary blood flow
• Decrease the percentage of
compressions that achieve target
depth
-
Chest Compression Depth
• 2010 AHA Guidelines for CPR and
ECC • ≥ 2 inches in adults
• At least one third of the
anterior-‐posterior dimension of the
chest in infants and children
• ≈1½ inches or 4 cm in
infants • ≈ 2 inches or 5
cm in children
-
Push Hard
SPell IG et al. What is the
role of chest compression depth
during out-‐of-‐hospital cardiac arrest
resuscitaPon? Crit Care Med.
2012;40:1192-‐1198
-
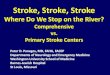
Compression Depth and Survival to
Discharge Rates
• < 38 mm compression depth •
Survival-‐to-‐discharge rates reduced by
30%
-
Perkins GD, Benny R, Giles S,
et al. Do different ma$resses
affect the quality of cardiopulmonary
resuscitaPon? Intensive Care Medicine.
29(12), 2330-‐5.
Comparison of chest compression depth
over Pme on 4 different
surfaces
Surfaces Do Ma?er
-
CPR Feedback Devices
• Accelerometer Device • Field InducPon
Device
-
Perkins GD, Kocierz L, Smith SCL,
McCulloch RA, Davies RP, Compression
feedback devices over esPmate chest
compression depth when performed on
a bed, ResuscitaPon, 80 (2009):
79–82
Get the PaKent to the Floor
-
Full Chest Recoil: No Residual
Leaning
• Decreases blood flow throughout the
heart • Can decrease venous return
and cardiac output
-
Oxygen Delivery and CPR
• EssenPal during CPR • Appropriate
Pmeframe to supplement exisPng oxygen
in the blood
• Varies with the type of arrest
• Arrhythmic • Asphyxial
• Metabolic demands for oxygen are
reduced in cardiac arrest
• Even during chest compressions
-
Sudden arrhythmic arrest
• Oxygen content iniPally sufficient
• High-‐quality chest compressions can
circulate oxygenated blood
• Studies suggest compressions without
venPlaPon may be adequate in
early nonasphyxial arrests
-
Asphyxial Cardiac Arrest
• CombinaPon of assisted venPlaPon and
high-‐quality chest compressions
• CriPcal to ensure adequate oxygen
delivery • Studies have found
improved outcomes when both assisted
venPlaPon and high-‐quality chest
compressions are delivered
-
Goal of Assisted VenKlaKon During
Cardiac Arrest• Providing sufficient oxygen
to the blood without impeding
perfusion • PosiPve pressure venPlaPon
reduces CPP during CPR • Synchronous
venPlaPon requires interrupPons
• Reduces chest compression fracPon
• Compression-‐only CPR versus standard
CPR
• Yielded similar survival outcomes •
Not enough evidence to define when
or if venPlaPon should be
withheld by experienced providers
• More data required
-
VenKlaKon Rate < 12 Breaths per
Minute
• No data showing higher rate of
venPlaPon is beneficial • InflaPon
Pme of 1 second for each
breath with a compression rate
of 100-‐120/min
• 6 to 12 breaths
-
Minimal Chest Rise
• VenPlaPon volume should produce no
more than visible chest rise
• PosiPve-‐pressure venPlaPon significantly
lowers cardiac output
• Spontaneous circulaPon • CPR
• Lower Pdal volumes during prolonged
cardiac arrest was not associated
with significant differences in Pao2
• PosiPve pressure venPlaPon in an
unprotected airway may gastric
insufflaPon
• AspiraPon of gastric contents • Lung
compliance is affected by
compressions during cardiac arrest
-
CPR in a Moving Ambulance
• The mean compression depth performed on the floor (39 ±
9mm)was greater than that on a moving stretcher (28±9mm) (p
-
DefibrillaKon Failure
• Longer pre-‐shock pauses • Shallow
chest compressions
-
Pre-‐Shock Pauses and DefibrillaKon
Success
Edelson DP et al. Effects of
compression depth and pre-‐shock
pauses predicts defibrillaPon failure
during cardiac arrest. ResuscitaPon.
2006;71:137-‐145.
-
Compression Depth and Shock Success
Rate
Edelson DP et al. Effects of
compression depth and pre-‐shock
pauses predicts defibrillaPon failure
during cardiac arrest. ResuscitaPon.
2006;71:137-‐145.























![Bee Gees - Stayin' Alive 'Evans]](https://img.pdfslide.us/doc/110x75/577cd7bd1a28ab9e789faaf4/bee-gees-stayin-alive-evans.jpg)


