-
Stay Put or Move On:
To Age in Place or Move to a
Continuing Care Retirement
Community
Margaret Riley John DiMiceli
[email protected] [email protected]
spomo.weebly.com
Copyright © 2017
-
Class Four
First Topics of the Day:
Long Term Care Insurance
Recommendations for Legal Documents
North Carolina Department of Insurance
Special Entities Section Regulation of
Continuing Care Retirement
Communities
-
Long Term Care Insurance
The responses to our pre-course survey
indicated that:
17 of class members or about
71% of the class
are subscribed to a long term care
insurance policy. This is a higher-than-
average percentage.
-
Long Term Care
With thanks for content to:
Brad Fox
Medical Claims Rx Inc.
1201 Raleigh Rd, Suite 208,
Chapel Hill, NC 27517
Phone: 919-942-7211
-
Long-Term Care
The phrase “long term care“ refers to the help that people with
chronic illnesses, disabilities or other conditions need on a daily
basis over an extended period of time. The type of help needed can
range from assistance with simple activities (such as bathing,
dressing and eating) to skilled care that's provided by nurses,
therapists or other professionals.
AARP: Understanding Long Term Care Insurance, May, 2016
-
Odds of Needing LTC?
Age is the #1 risk factor
◦ 50% of people over 85 need some form of LTC
◦ 70%-75% of people over 65 will need some LTC in their
lifetime; Approximately 1/3 of those will need care for an average
of 2 1/2 years
50% of all LTC claims last about 90 days; the other 50% average
3 ½ yrs
48% of claims are for dementia; 13% for stroke; 3% for
cancer
Approximately 2/3 of people needing LTC are women
Approximately 78% of claims are for Home Care; 10.6% for
Assisted Living, 11.2% for Nursing Home*
Average # of days for claims*:
Home Care 523
Assisted Living 1079
Nursing Home 690
*Genworth Insurance
-
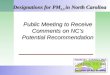
Needing Help As We Age
0
5
10
15
20
25
30
35
40
45
50P
erc
en
t
Activities of Daily Living
65 - 74
75 - 84
85 +
-
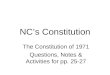
Years of Long Term Care
0
10
20
30
40
50
60
70
80
90
Need Care < 1 Yr 1 - 2 Yr 2 - 5 Yr > 5 Yr
Pe
rce
nt
Years of Care Needed
Men
Women
-
How Are LTC Needs Met?
Family or other non-paid caregivers (84%)
Paid Services (16%):
Self-insure
Other family member pay 22%
Life-care or Modified Life-care CCRCs
Long-term care insurance 12%
Medicare 4%
Medicaid 62% $180 Billion spent annually on LTC. 12% covered by
LTC insurance
60% of workers aged 55+ have < $100,000 savings; 43% <
$25,000
-
Eligible Providers of Care
Facility-Based Care
◦ Nursing Homes (Skilled and Intermediate)
◦ Assisted Living and Memory Care Facilities
Community-Based Care
◦ Licensed Home Care Agencies
◦ Adult Day Care Facility
◦ Informal Caregivers (?)
◦ Case Managers (?)
-
Tax Incentives for TQ LTC Policies
Premiums for Tax Qualified (TQ) plans are eligible as medical
expense for Federal deduction
Total medical expenses above 10% of AGI are deductible (7.5% if
you or your spouse are 65 or over).
Maximum eligible LTC premium amount based on age (per person).
2016 amount 2017 amount 51-60 $1460 $1530
61-70 $3900 $4090
>70 $4870 $5110
Benefits paid by Tax Qualified plans are not taxable as
income
-
Do You Qualify for Benefits?
Tax Qualified Plans (issued after 1/1/1997)
I. 2 of 6 Activities of Daily Living (ADL’s) for >90 days
Bathing
Dressing
Transferring
Toileting
Continence
Feeding
II. Cognitive Impairment
-
Filing the First Claim
Get all necessary forms completed by Doctor, Facility or
Agency
Get copies of LTC provider licenses
If possible have Providers return all forms to the person
assisting with filing the claim, and make copies before sending to
the LTC insurance company
Send a copy of POA with the first claim if appropriate
Ask Insurance company if they want first set of provider charges
with initial claim
Follow up with a phone call to Insurance Company two weeks after
submitting claim to confirm receipt and get claim status
-
The Next Step
Once Claim is Approved, file Provider Charges, and care notes if
necessary, going back to initial care start date, and monthly
thereafter. Keep copies.
Review Provider statements for accuracy. For home care claims,
check to be sure time sheets match provider invoice
Call Insurance Company two weeks after claim submitted to
confirm receipt and get claim status
Once claim is paid, review insurance Explanation of Benefits
(EOB) to be sure all eligible services have been reimbursed
correctly
Set up direct deposit of benefit checks if possible
-
Legal Documents
We are NOT ATTORNEYS!!
Others advise we include SOMETHING
about legal documents you should have
According to several sources, the
following are the minimum documents
you should have moving forward
Check SPOMO Resource Page for
relevant links
-
ESSENTIAL DOCUMENTS
A Will
◦ If you have significant assets, consider also a Revocable
Trust
to avoid the time and expense of probate (the
public legal process that examines your estate after
you die) and
helps ensure your estate’s privacy.
Durable Power of Attorney
Advanced Health Care Directive
-
National Academy of
Elder Law Attorneys (NAELA)Highlights five key items when
speaking with legal counsel about a living will, health care power
of attorney, and health care proxy:
1. Who will serve as your Agent for Health Care? Who will serve
as the alternate?
2. Are there certain medical treatments or pain control measures
you want or don’t want?
-
NAELA Recommendations (cont’d)
3. Do you wish to take or refuse any medication that may reduce
or eliminate the ability to communicate?
4. Do you have any particular directions regarding specific
health care facilities, religious preferences, disposition of your
body, donation of bodily parts for transplant or research,
etc.?
5. What directions will you provide related to end-of life
decisions?
-
NC Department of Insurance
Special Entities Section
-
With thanks for content to
Steve Johnson Manager Special Entities SectionNC Department of
Insurance
Michael McKinney Senior Financial Analyst Special Entities
SectionNC Department of Insurance
Phone: (919)807-6614
http://www.ncdoi.com/SE/Continuing_Care_Retirement_Communities.aspxNorth
Carolina Continuing Care Retirement Communities Reference Guide
(2017)
http://www.ncdoi.com/SE/Continuing_Care_Retirement_Communities.aspxhttp://spomo.weebly.com/uploads/5/0/6/9/50694751/ncdoi_ccrc_guide_2017.pdf
-
What is a CCRC
---or a---
Life Plan Community?
In general, CCRCs are communitiesthat provide a continuum of
care under a contract for the life of an individual, or a period
longer than one year, in exchange for an entrance fee and/or
periodic fees.
-
By state law CCRCs must meet two criteria to receive CCRC
classification:
They must offer independent living and health related services
(the health related services must be a licensed level of care,
either adult care, or nursing care, or both); and
The term of the contract offered to a resident must be for the
life of the individual or for a term in excess of one year
-
NC Growth
The seniorpopulation in North
Carolina isprojected to
increase from
1.5 Millionin 2014 to
2.5 Million in 2034 = +68%
Resident Population Jobs Generated Economic Impact
In 2014 there were
18,961 residents living in the 57CCRCs in North
Carolina. By 2034, the projected
number of residents
is 35,381 = +87%
CCRCs in North Carolina are supporting a
growing workforce.
By 2034, CCRCs areprojected to employ
29,752 workers compared to
14,906 in 2014 = +100%
total estimated economic impact on
NC’s economy in 2014 was
$1.7 BillionBy 2034,
the total estimated economic impact is
projected to be
$3.2 Billion = +88%
CCRCs in North Carolina (2014 to 2034)
Appold, Johnson, Parnell (November 2015)
"Market Needs and Economic Impact of Continuing Care Retirement
Communities in North Carolina.”
Frank Hawkins Kenan Institute of Private Enterprise, University
of North Carolina - Chapel Hill.
-
Types of Contracts
Extensive or Life Care - (Type A)
Modified Cost - (Type B)
Fee for Service - (Type C)
Equity - (Type D)
NEW
Rental Agreements - (Type E)
Continuing Care at Home - (Type F)
24
-
Continuing Care Without Lodging – July 2010
GS § 58-64-7 Continuing Care Services Without Lodging
Requires the provider to submit, among other things:
• Application
• Amended disclosure statement with project description and
market analysis
• Written service agreement
• Summary actuarial report
• Financial feasibility study by a CPA firm
Provider must enter into binding written service
agreements with subscribers
Financial statements must account for related revenue and
expenses separately from on-site operations
Presently only 3 in NC – Salemtowne, Carol Woods, and
Carolina Meadows
-
CCRC Regulation
CCRCs have been licensed and regulated by the DOI since January
1, 1990. Currently there are 59 CCRCs in NC.
“The DOI is here to protect residents and potential
residents!!”
Primary areas of regulation include:
Contract Disclosures
Financial Oversight
Health care is licensed and regulated by the NC Department of
Health and Human Services (“DHHS”). This includes
Adult Home Care (Assisted Living)
Skilled Nursing Care
-
CCRC Required Annual Filings
1) Filing Supplement CCRC-02
2) Current Disclosure Statement
3) Current Audited Financial Statements
4) Five Year Forecasted Financial Statements
5) Interim Unaudited Financial Statements
6) Material Differences Statements – Prior
Year Forecast vs CY Audited Financial
Statements
7) Current Resident Agreements
-
Operating Reserve Requirement
Based upon forecasted operating expenses
• “12 month period following the period covered by the most
recent disclosure statement”
• “forecasted statements serve as the basis for computing
future operating reserve requirements”
90% occupancy requirement
• 90% applies to Independent plus Assisted Living
occupancy – omits Skilled Nursing
Reporting
• Operating reserve is a restricted asset. The reserve can’t
be
released/used without the Commissioner’s written approval.
-
NC is one of the more regulated States as far as CCRCs. Other
states in the top tier are NY, CA, OH, FL, PA, AZ, and IL. Some
states have little or NO regulation.
NC’s operating reserve requirement that each CCRC maintain
restricted funds equal to 3 or 6 months of projected operating
expenses based upon occupancy rates. These funds can only be used
upon written approval of the Commissioner of Insurance.
DOI’s review and follow-up of annual, quarterly, and in some
instances, monthly filings.
NC’s ability to place troubled CCRCs under direct supervision of
the Regulatory Actions Section (“RAS”).
Why has NC NEVER had a CCRC fail?
-
CCRC Advisory Committee
Established by GS § 58-64-80
“…There shall be a 9 member Continuing
Care Advisory Committee appointed by the
Commissioner…” that:
Recommends changes in DOI's rules &
regulations
Provides advice regarding the
management/operation of NC CCRCs.
Holds semi-annual public meetings at
locations throughout the state.
-
CCRC Advisory Committee
The Committee consists of at least;
2 residents of CCRCs
2 representatives of LeadingAge NC
1 CPA licensed to practice in NC
1 individual skilled in architecture or
engineering,
1 health care professional,
2 at-large members
◦ One is currently a Carol Woods resident
http://www.leadingagenc.org/?
-
Trending in CCRC Development
Mergers
Two CCRCs
CCRC + Corporation
CCRC + Hospital
Expansions
Rental CCRCs
Continuing Care Without Lodging
New CCRCs by large companies or
organizations that own other facilities in single
and multiple states
-
What is in the DOI Pipeline? - $1,024B
4 Notifications of Intent (expansions) $366M
3 New CCRCs
1 CCRC that is expanding
5 Start-Up Certificates (new CCRC) $312M
1 New CCRC,
4 CCRCs that are expanding, and
4 Preliminary Certificates $251M
2 New CCRCs (1 on Hold) and
2 Expansions
2 Permanent Licenses (9/21/16) $95M